Timing of Ureteric Stent Removal and Occurrence of Urological Complications after Kidney Transplantation: A Systematic Review and Meta-Analysis

 and
and
Abstract
:1. Introduction
2. Methods
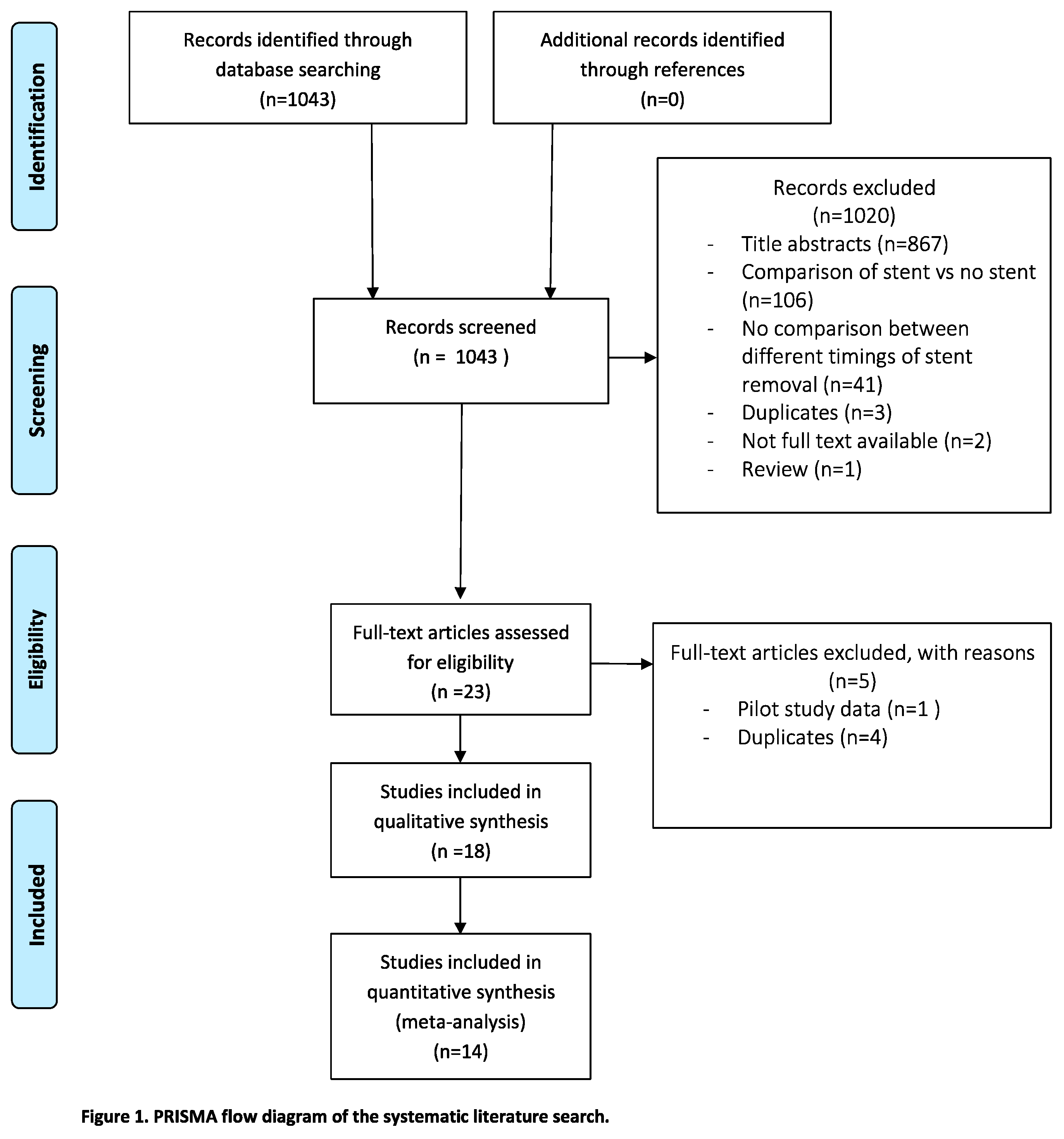
2.1. Literature Search Strategy
2.2. Literature Screening
2.3. Data Extraction
2.4. Critical Appraisal
2.5. Statistical Analysis
3. Results
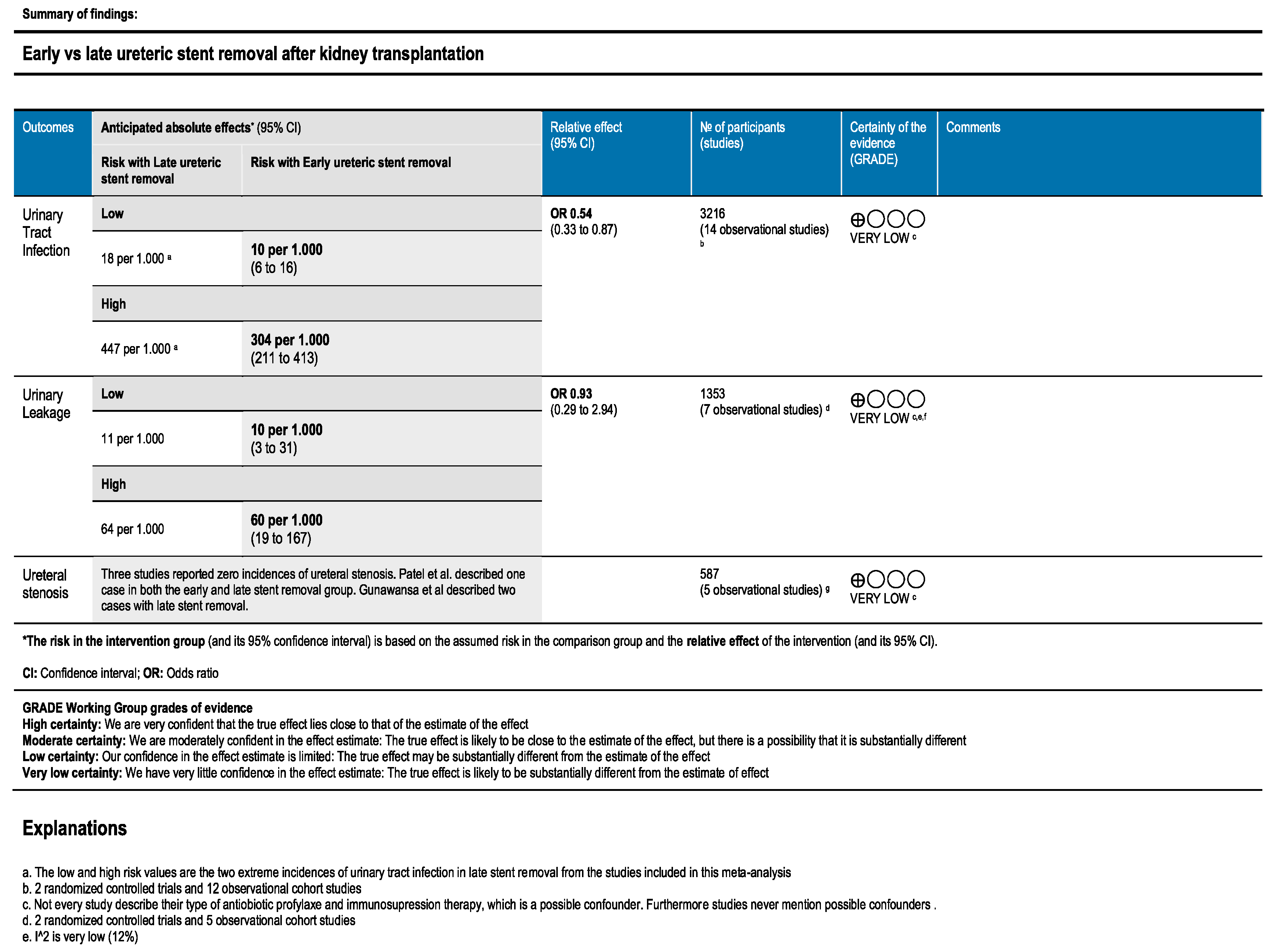
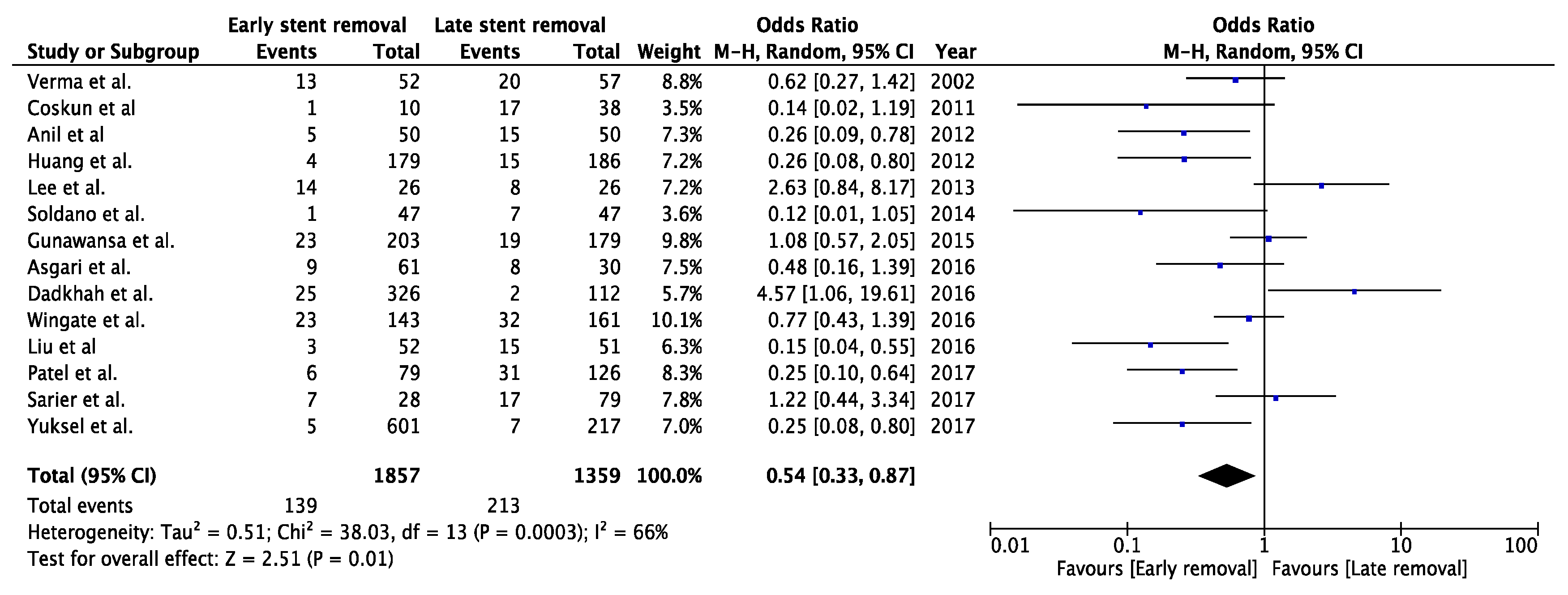
3.1. Urinary Tract Infection
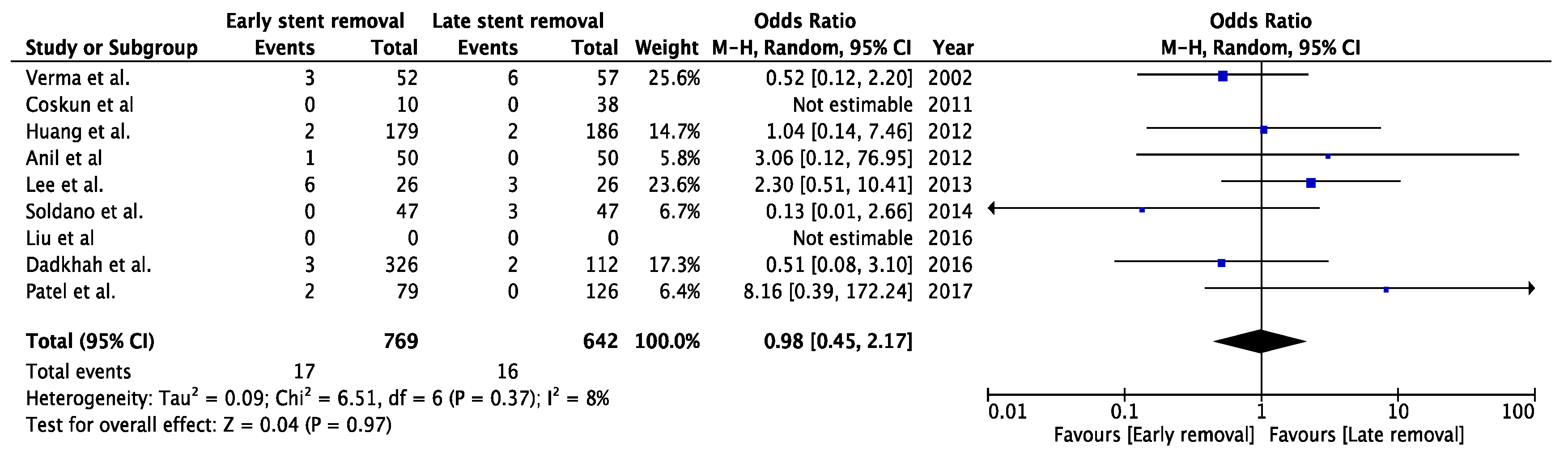
3.2. Urinary Leakage
3.3. Ureteral Stenosis
3.4. Reintervention
4. Discussion
4.1. Difficulty in Anastomosis
4.2. Urinary Tract Infection
4.3. Ureteral Leakage and Ureteral Stenosis
4.4. Additional Advantages
4.5. Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | Date of Patient Results | Timing of Stent Removal | Type of Stent | Living/Deceased Donor | Mean Age of Patients | Technique UNC | Technique of Stent Removal | Immunsupression Threapy | Prophylactic Antibiotics | Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|
| Yuksel et al. [23] | jan2014–jan2016 | 5–7 days | Double J-stent | 100%/0% | 40.7 y * | Lich-Gregoir | Cystoscopy | CNI + MMF + Cor | Yes * | NR |
| 8–14 days | ″ | 43.5 y * | Cystoscopy | Until stent removal | ||||||
| 15–21 days | ″ | 41.5 y * | Cystoscopy | |||||||
| >22 days | ″ | 41.9 y * | Cystoscopy | |||||||
| Patel et al. [21] | may2010–nov2013 | 5 days | Double J stent | 60.5%/39.5% | 47.5 y * | Lich-Gregoir | Attached to UC | NR | Yes * | UTI: 3 months |
| 6 weeks | 65.6%/34.4% | 41.7 y * | Cystoscopy | 6 months | MUC: 6 months | |||||
| Sarier et al. [22] | jan2016–may2016 | 15–21 days | Double J-stent | 100%/0% | 45.14 y | Extravesical = Lich-Gregoir | Cystoscopy | CNI + Ster | Yes * | NR |
| 21–28 days | ″ | 41.18 y | Cystoscopy | |||||||
| 28–35 days | ″ | 47.52 y | Cystoscopy | |||||||
| Wingate et al. [8] | jan2010–jan2015 | <3 weeks | Double J-stent | 32/68% (5) | 55.5 y (5) | NR | Attached to external string = suture | Tac+ MMF+ Pred + (Atg/Bas/Dac(6)) | NR | 9 months |
| >3 weeks | ″ | ″ | Cystoscopy | |||||||
| Liu et al. [20] | oct2010–march2015 | 7 days | Double J-stent | 100%/0% | 34.9 y | Lich-Gregoir | Attached to external sutures | CNI + MMF + Cor + Bas | Yes | 3 months |
| 28 days | ″ | 35.4 y | Cystoscopy | 3 days post operative | ||||||
| Dadkhah et al. [37] | may2011–march2012 | 10 days | Unspecified | 100%/0% | 40.5 y * | NR | NR | NR | NR | 1 month |
| 20 days | ″ | 40.4 y * | ||||||||
| 30 days | ″ | 41.9 y * | ||||||||
| Asgari et al. [38] | may2011–march2012 | 10 days | Unspecified | 100%/0% | 41.4 y * | NR | NR | NR | NR | 1 month |
| 20 days | ″ | 38.0 y * | ||||||||
| 30 days | ″ | 43.7 y * | ||||||||
| Gunawansa et al. [36] (1) | Jan2009–August2013 | 6 days | Unspecified | 100%/0% | NR | NR | Attached to UC | NR | NR | 16 (12–36) months |
| 28 days | ″ | Cystoscopy | ||||||||
| Soldano et al. [35] (2) | NR | 5 days | Unspecified | NR | NR | NR | Attached to UC | NR | Yes | NR |
| 6 weeks | Cystoscopy | |||||||||
| Lee et al. [34] (3) | jan2011–aug2011 | 5 days | Unspecified | NR | NR | NR | Attached to UC | NR | Yes * | 12 months |
| 6 weeks | Cystoscopy | |||||||||
| Huang et al. [33] | jan2009–dec2010 | 3 weeks | Double J-stent | 0%/100% | 42.8 y | NR | Cystoscopy | CNI + MMF + Pred | Yes | 3 months |
| 6 weeks | ″ | 43.5 y | Cystoscopy | First week post operative | ||||||
| Indu et al. [31] | Jan 2007–Dec 2009 | 7 days | Double J stent | 100%/0% | 34.4y | Lich-Gregoir | NR | Cycl + Aza/ MMF + Pred + (Dac(6)) | Yes* | 6 months |
| 28 days | ″ | 33.8 y) | 6 months | |||||||
| Coskun et al. [13] | nov2005–may2010 | 13–14 days | Double J stent | 70%/30% | 21–41 y | Lich-Gregoir | NR | NR | Yes* | 14–49 months |
| >20 days (4) | 58%/42% | 19–56 y | 3 months | 4–55 months | ||||||
| Verma et al. [32] | Jan 1996–June 1996 | 2 weeks | Double J stent | 100%/0% | 31.2 y | Lich-Gregoir | Cystoscopy | Cycl+ Aza + Pred | Yes* | NR |
| 4 weeks | ″ | 33.8 y | Cystoscopy | 3 months |
| Embase.com | 944 | 936 |
| Medline Ovid | 443 | 55 |
| Web of Science | 268 | 25 |
| Cochrane CENTRAL | 43 | 3 |
| Google Scholar | 100 | 24 |
| Total | 1798 | 1043 |
References
- Abecassis, M.; Bartlett, S.T.; Collins, A.J.; Davis, C.L.; Delmonico, F.L.; Friedewald, J.J.; Hays, R.; Howard, A.; Jones, E.; Leichtman, A.B.; et al. Kidney transplantation as primary therapy for end-stage renal disease: A National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQITM) conference. Clin. J. Am. Soc. Nephrol. 2008, 3, 471–480. [Google Scholar] [CrossRef]
- Lafranca, J.A.; Hesselink, D.A.; Dor, F.J.M.F. Oxford Textbook of Urological Surgery; Ploeg, R., Ed.; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed]
- Rigg, K.M.; Proud, G.; Taylor, R.M. Urological complications following renal transplantation. A study of 1016 consecutive transplants from a single centre. Transplant. Int. 1994, 7, 120–126. [Google Scholar]
- Kumar, A.; Verma, B.S.; Srivastava, A.; Bhandari, M.; Gupta, A.; Sharma, R. Evaluation of the urological complications of living related renal transplantation at a single center during the last 10 years: Impact of the Double-J* stent. J. Urol. 2000, 164, 657–660. [Google Scholar] [CrossRef]
- Wilson, C.H.; Bhatti, A.A.; Rix, D.A.; Manas, D.M. Routine intraoperative ureteric stenting for kidney transplant recipients. Cochrane Database Syst. Rev. 2005, 4, CD004925. [Google Scholar]
- Sansalone, C.V.; Maione, G.; Aseni, P.; Mangoni, I.; Soldano, S.; Minetti, E.; Radaelli, L.; Civati, G. Advantages of short-time ureteric stenting for prevention of urological complications in kidney transplantation: An 18-year experience. Transplant. Proc. 2005, 37, 2511–2515. [Google Scholar] [CrossRef] [PubMed]
- Wingate, J.T.; Brandenberger, J.; Weiss, A.; Scovel, L.G.; Kuhr, C.S. Ureteral stent duration and the risk of BK polyomavirus viremia or bacteriuria after kidney transplantation. Transplant. Infect. Dis. 2017, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Mangus, R.S.; Haag, B.W. Stented versus nonstented extravesical ureteroneocystostomy in renal transplantation: A metaanalysis. Am. J. Transplant. 2004, 4, 1889–1896. [Google Scholar] [CrossRef]
- Dominguez, J.; Clase, C.M.; Mahalati, K.; MacDonald, A.S.; McAlister, V.C.; Belitsky, P.; Kiberd, B.; Lawen, J.G. Is routine ureteric stenting needed in kidney transplantation? A randomized trial. Transplantation 2000, 70, 597–601. [Google Scholar] [CrossRef]
- Osman, Y.; Ali-El-Dein, B.; Shokeir, A.A.; Kamal, M.; El-Din, A.B. Routine insertion of ureteral stent in live-donor renal transplantation: Is it worthwhile? Urology 2005, 65, 867–871. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, A.; Surange, R.S.; Pearson, R.C.; Parrott, N.R.; Augustine, T.; Riad, H.N. Impact of Stents on Urological Complications and Health Care Expenditure in Renal Transplant Recipients: Results of a Prospective, Randomized Clinical Trial. J. Urol. 2007, 177, 2260–2264. [Google Scholar] [CrossRef] [PubMed]
- Coskun, A.K.; Harlak, A.; Ozer, T.; Eyitilen, T.; Yigit, T.; Demirbaş, S.; Uzar, A.İ.; Kozak, O.; Cetiner, S. Is removal of the stent at the end of 2 weeks helpful to reduce infectous or urologic complications after renal transplantation? Transplant. Proc. 2011, 43, 813–815. [Google Scholar] [CrossRef]
- Guvence, N.; Oskay, K.; Karabulut, I.; Ayli, D. Effects of ureteral stent on urologic complications in renal transplant recipients: A retrospective study. Renal Fail. 2009, 31, 899–903. [Google Scholar] [CrossRef]
- Ranganathan, M.; Akbar, M.; Ilham, M.A.; Chavez, R.; Kumar, N.; Asderakis, A. Infective Complications Associated with Ureteral Stents in Renal Transplant Recipients. Transplant. Proc. 2009, 41, 162–164. [Google Scholar] [CrossRef]
- Glazier, D.B.; Jacobs, M.G.; Lyman, N.W.; Whang, M.I.; Manor, E.; Mulgaonkar, S.P. Urinary tract infection associated with ureteral stents in renal transplantation. Can. J. Urol. 1998, 5, 462–466. [Google Scholar] [PubMed]
- Breda, A.; Olsburgh, J.; Budde, K.; Figueiredo, A.; LledóGarcía, E.; Regele, H. EAU Guidelines on Renal Transplantation 2014. Available online: https://www.uroweb.org/guideline/renal-transplantation/ (accessed on 1 June 2018).
- Parapiboon, W.; Ingsathit, A.; Disthabanchong, S.; Nongnuch, A.; Jearanaipreprem, A.; Charoenthanakit, C.; Jirasiritham, S.; Sumethkul, V. Impact of early ureteric stent removal and cost-benefit analysis in kidney transplant recipients: Results of a randomized controlled study. Transplant. Proc. 2012, 44, 737–739. [Google Scholar] [CrossRef]
- Ali Asgari, M.; Dadkhah, F.; Tara, S.A.; Argani, H.; Tavoosian, A.; Ghadian, A. Early Stent Removal After Kidney Transplantation: Is it Possible? Nephrourol. Mon. 2016, 8, e30598. [Google Scholar] [CrossRef]
- Liu, S.; Luo, G.; Sun, B.; Lu, J.; Zu, Q.; Yang, S.; Zhang, X.; Dong, J. Early Removal of Double-J Stents Decreases Urinary Tract Infections in Living Donor Renal Transplantation: A Prospective, Randomized Clinical Trial. Transplant. Proc. 2017, 49, 297–302. [Google Scholar] [CrossRef]
- Patel, P.; Rebollo-Mesa, I.; Ryan, E.; Sinha, M.D.; Marks, S.D.; Banga, N.; Macdougall, I.C.; Webb, M.C.; Koffman, G.; Olsburgh, J. Prophylactic Ureteric Stents in Renal Transplant Recipients: A Multicenter Randomized Controlled Trial of Early Versus Late Removal. Am. J. Transplant. 2017, 17, 2129–2138. [Google Scholar] [CrossRef] [PubMed]
- Sarier, M.; Demir, M.; Duman, I.; Yuksel, Y.; Demirbas, A. Evaluation of Ureteral Stent Colonization in Live-Donor Renal Transplant Recipients. Transplant. Proc. 2017, 49, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, Y.; Tekin, S.; Yuksel, D.; Duman, I.; Sarier, M.; Yucetin, L.; Kiraz, K.; Demirbas, M.; Kaya Furkan, A.; Aslan Sezer, M.; et al. Optimal Timing for Removal of the Double-J Stent After Kidney Transplantation. Transplant. Proc. 2017, 49, 523–527. [Google Scholar] [CrossRef]
- Thompson, E.R.; Hosgood, S.A.; Nicholson, M.L.; Wilson, C.H. Early versus late ureteric stent removal after kidney transplantation. Cochrane Database Syst. Rev. 2018, 1, CD011455. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration. 2011. Available online: http://handbook.cochrane.org.
- Visser, I.J.; Van der Staaij, J.P.T.; Willicombe, M.; Muthusamy, A.; Lafranca, J.A.; Dor, F.J.M.F. Timing of Double-J stent Removal and Occurrence of Urological Complications: A Systematic Review and Meta-Analysis. PROSPERO 2018 CRD42018079867. Available online: http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018079867 (accessed on 23 April 2019).
- Bonkat, G.; Groschl, I.; Rieken, M.; Rentsch, C.A.; Wyler, S.; Gasser, T.C.; Widmer, A.F.; Bachmann, A. Microbial biofilm formation on ureteral stents in renal transplant recipients: Frequency and influence on short time functional outcome. Eur. Urol. Suppl. 2010, 9, 164. [Google Scholar] [CrossRef]
- GRADEpro GDT; McMaster University: Hamilton, ON, Canada, 2015.
- Review Manager; The Nordic Cochrane Centre: Copenhagen, Denmark, 2014.
- Indu, K.N.; Lakshminarayana, G.; Anil, M.; Rajesh, R.; George, K.; Ginil, K.; Georgy, M.; Nair, B.; Sudhindran, S.; Appu, T.; et al. Is early removal of prophylactic ureteric stents beneficial in live donor renal transplantation. Indian J. Nephrol. 2012, 22, 275–279. [Google Scholar]
- Verma, B.S.; Bhandari, M.; Srivastava, A.; Kapoor, R.; Kumar, A. Optimum duration of J.J. Stenting in live related renal transplantation. Indian J. Urol. 2002, 19, 54–57. [Google Scholar]
- Huang, L.; Wang, X.; Ma, Y.; Wang, J.; Tao, X.; Liao, L.; Tan, J. A comparative study of 3-week and 6-week duration of double-j stent placement in renal transplant recipients. Urol. Int. 2012, 89, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.; Herzig, J.; Crotty, C.; Shah, K.; Nicholson, M.L.; Hosgood, S.A. Comparison of early versus late ureteric stent removal after kidney transplantation. Transplant. Int. 2013, 26, 271. [Google Scholar]
- Soldano, S.; Ali, A.; Pawelec, K.; Sammartino, C.; Sivaprakasam, R.; Puliatti, C.; Cacciola, R. Safety and potential benefits of early ureteric stent removal tied with urinary catheter after renal transplant. Transplantation 2014, 98, 638–639. [Google Scholar] [CrossRef]
- Gunawansa, N.; Wijeyaratne, M.; Cassim, R.; Sahabandu, C. Early bedside removal versus delayed cystoscopic removal of ureteric stents following live donor renal transplantation: A randomized prospective study. Transplant. Int. 2015, 28, 118. [Google Scholar]
- Dadkhah, F.; Yari, H.; Asgari, M.A.; Fallahnezhad, M.H.; Tavoosian, A.; Ghadian, A. Benefits and complications of removing ureteral stent based on the elapsed time after renal transplantation surgery. Nephro-Urol. Mon. 2016, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Asgari, M.A.; Dadkhah, F.; Tara, S.A.; Argani, H.; Tavoosian, A.; Ghadian, A. Early stent removal after kidney transplantation: Is it possible? Nephro-Urol. Mon. 2016, 8, 2. [Google Scholar]
- Thiel, K.; Wichmann, D.; Nadalin, S.; Ladurner, R.; Königsrainer, A. Urinary tract infection in renal transplant patients-what to do? Transplant. Int. 2013, 26, 284. [Google Scholar]
- Mannu, G.S.; Bettencourt-Silva, J.H.; Gilbert, J. The ideal timing of ureteric stent removal in transplantation patients. Transplant. Int. 2014, 27, e96–e97. [Google Scholar] [CrossRef]
- Raza, S.; Ghazanfar, A.; Alahmadi, I.; Alahdal, H.; Brockmann, J.; Broring, D.; Abassi, A.; Aleid, H. Impacts of ureteric stent removal timing on post renal transplant major urological complication. A single centre experience. Transplantation 2016, 100, S318. [Google Scholar]
- Pleass, H.C.C.; Clark, K.R.; Rigg, K.M.; Reddy, K.S.; Forsythe, J.L.R.; Proud, G.; Taylor, R.M. Urologic complications after renal transplantation: A prospective randomized trial comparing different techniques of ureteric anastomosis and the use of prophylactic ureteric stents. Transplant. Proc. 1995, 27, 1091–1092. [Google Scholar]
- Eschwege, P.; Blancher, P.; Bellamy, J.; Charpentier, B.; Jardin, A.; Benoit, G. Does the use of double J ureteral stents reduce stenosis and fistulas in renal transplantation. Transplant. Proc. 1995, 27, 2436. [Google Scholar] [PubMed]
- Kumar, A.; Kumar, R.; Bhandari, M. Significance of routine JJ stenting in living related renal transplantation: A prospective randomised study. Transplant. Proc. 1998, 30, 2995–2997. [Google Scholar] [CrossRef]
- Gedroyc, W.M.W.; Koffman, G.; Saunders, A.J.S. Ureteric obstruction in stented renal transplants. Brit. J. Urol. 1988, 62, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Mangus, R.S.; Haag, B.W.; Carter, C.B. Stented Lich-Gregoir ureteroneocystostomy: Case series report and cost-effectiveness analysis. Transplant. Proc. 2004, 36, 2959–2961. [Google Scholar] [CrossRef] [PubMed]
- Thomalla, J.V.; Leapman, S.B.; Filo, R.S. The use of internalised ureteric stens in renal transplant recipients. Brit. J. Urol. 1990, 66, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Ooms, L.; Ijzermans, J.; Voor, I.; Holt, A.; Betjes, M.; Vos, M.; Terkivatan, T. Urinary Tract Infections After Kidney Transplantation: A Risk Factor Analysis of 417 Patients. Ann. Transplant. 2017, 22, 402–408. [Google Scholar] [CrossRef] [PubMed]




| Studies | Year | Sort Study | Timing of Stent Removal | Number of Patients | Urinary Tract Infection | Major Urological Complication | Urinary Leakage | Ureteral Stenosis |
|---|---|---|---|---|---|---|---|---|
| Yuksel et al. [23] | 2017 | Retrospective | 5–7 days | 153 | x | x | ||
| 8–14 days | 165 | |||||||
| 15–21 days | 283 | |||||||
| >22 days | 217 | |||||||
| Patel et al. [21] | 2017 | RCT | 5 days | 79 | x | x | x | x |
| 6 weeks | 126 | |||||||
| Sarier et al. [22] | 2017 | Retrospective | 15–21 days | 28 | x | |||
| 21–28 days | 54 | |||||||
| 28–35 days | 25 | |||||||
| Wingate et al. [8] | 2017 | Retrospective | <3 weeks | 143 | x | |||
| >3 weeks | 161 | |||||||
| Liu et al. [20] | 2016 | RCT | 7 days | 52 | x | x | x | x |
| 28 days | 51 | |||||||
| Dadkhah et al. [37] | 2016 | Prospective | 10 days | 164 | x | x | x | |
| 20 days | 162 | |||||||
| 30 days | 112 | |||||||
| Asgari et al. [38] | 2016 | Retrospective | 10 days | 30 | x | x | x | |
| 20 days | 31 | |||||||
| 30 days | 30 | |||||||
| Gunawansa et al. [36] | 2014(1) | Prospective | 6 days | 203 | x | x | x | |
| randomised | 28 days | 179 | ||||||
| Soldano et al. [35] | 2014(2) | Retrospective | 5 days | 47 | x | x | x | |
| 6 weeks | 47 | |||||||
| Lee et al. [34] | 2013(3) | Retrospective | 5 days | 26 | x | x | ||
| 6 weeks | 26 | |||||||
| Huang et al. [33] | 2012 | Retrospective | 3 weeks | 179 | x | x | x | x |
| 6 weeks | 186 | |||||||
| Indu et al. [31] | 2012 | Prospective RCT | 7 days | 50 | x | x | x | |
| 28 days | 50 | |||||||
| Coskun et al. [13] | 2011 | Retrospective | 13–14 days | 10 | x | x | ||
| >20 days | 38 | |||||||
| Verma et al. [32] | 2002 | Retrospective | 2 weeks | 52 | x | x | x | x |
| 4 weeks | 57 |
| Studies | Stent Removal | Number of Patients | Urinary Tract Infection (%) | Major Urological Complication | Ureteral Stenosis (%) | Urinary Leakage (%) | Surgical Reintervention (%) |
|---|---|---|---|---|---|---|---|
| Yuksel et al. [23] | 5–7 days | 153 | 0% * | 11.0% | 11.0% | ||
| 8–14 days | 165 | 1.2% * | 9.6% | 9.6% | |||
| 15–21 days | 283 | 1.1% * | 1.7% | 1.7% | |||
| >22 days | 217 | 3.2% * | 1.3% | 1.3% | |||
| Patel et al. [21] | 5 days | 79 | 7.6% * | 3.7% | 1.2% | 2.5% | 3.7% |
| 6 weeks | 126 | 24.6% * | 0.8% | 0.8% | 0% | 0.8% | |
| Sarier et al. [22] | 15–21 days | 28 | 7.1% * | x | |||
| 21–28 days | 54 | 5.6% * | x | ||||
| 28–35 days | 25 | 12.0% * | x | ||||
| Wingate et al. [8] | <3 weeks | 143 | 31.7% * | x | |||
| >3 weeks | 161 | 51.6% * | x | ||||
| Liu et al. [20] | 7 days | 52 | 5.8% * | 0% | 0% | 0% | 0% |
| 28 days | 51 | 29.4% * | 0% | 0% | 0% | 0% | |
| Dadkhah et al. [37] | 10 days | 164 | 18.1% | 1.0% | 1.0% | ||
| 20 days | 162 | 5.7% | 1.0% | 1.0% | |||
| 30 days | 112 | 9.1% | 2.8% | 2.8% | |||
| Asgari et al. [38] | 10 days | 30 | 20.0% | 6.6% | 6.6% | ||
| 20 days | 31 | 9.7% | 6.4% | 6.4% | |||
| 30 days | 30 | 26.7% | 13.3% | 13.3% | |||
| Gunawansa et al. [36] | 6 days | 203 | 11.3% | 0% | 0% | ||
| 28 days | 179 | 10.6% | 1.1% | 1.1% | |||
| Soldano et al. [35] | 5 days | 47 | 10.6% * | 0% | 0% | 0% | |
| 6 weeks | 47 | 25.5% * | 6.3% | 6.3% | 2.1% | ||
| Lee et al. [34] | 5 days | 26 | 53.0% | 23.0% | |||
| 6 weeks | 26 | 30.0% | 12.0% | ||||
| Huang et al. [33] | 3 weeks | 179 | 2.2% * | 1.1% | 0% | 1.1% | 1.1% |
| 6 weeks | 186 | 8.1% * | 1.1% | 0% | 1.1% | 1.1% | |
| Indu et al. [31] | 7 days | 50 | 14.0% * | 2.0% | 2.0% | 0% | |
| 28 days | 50 | 38.0% * | 0% | 0% | 0% | ||
| Coskun et al. [13] | 13–14 days | 10 | 10.0% * | 0% | |||
| >20 days | 38 | 45.0% * | 0% | ||||
| Verma et al. [32] | 2 weeks | 52 | 25.0% * | 5.8% | 0% | 5.8% | 0% |
| 4 weeks | 57 | 35.1% * | 10.0% | 0% | 10.0% | 0% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Visser, I.J.; van der Staaij, J.P.T.; Muthusamy, A.; Willicombe, M.; Lafranca, J.A.; Dor, F.J.M.F. Timing of Ureteric Stent Removal and Occurrence of Urological Complications after Kidney Transplantation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 689. https://doi.org/10.3390/jcm8050689
Visser IJ, van der Staaij JPT, Muthusamy A, Willicombe M, Lafranca JA, Dor FJMF. Timing of Ureteric Stent Removal and Occurrence of Urological Complications after Kidney Transplantation: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(5):689. https://doi.org/10.3390/jcm8050689
Chicago/Turabian StyleVisser, Isis J., Jasper P. T. van der Staaij, Anand Muthusamy, Michelle Willicombe, Jeffrey A. Lafranca, and Frank J. M. F. Dor. 2019. "Timing of Ureteric Stent Removal and Occurrence of Urological Complications after Kidney Transplantation: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 5: 689. https://doi.org/10.3390/jcm8050689