Syncope in a Working-Age Population: Recurrence Risk and Related Risk Factors

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Exclusion Criteria
2.3. Study End Points
- The 6-month, 1-year, and 5-year risk of syncope recurrence after the index event.
- The risk factors potentially related to syncope relapse at 6 months and 1 year.
- The 6-month, 1-year, and 5-year prognosis after the index syncope.
2.4. Definitions
2.5. Data Collection and Follow-Up
2.6. Statistical Analysis
3. Results
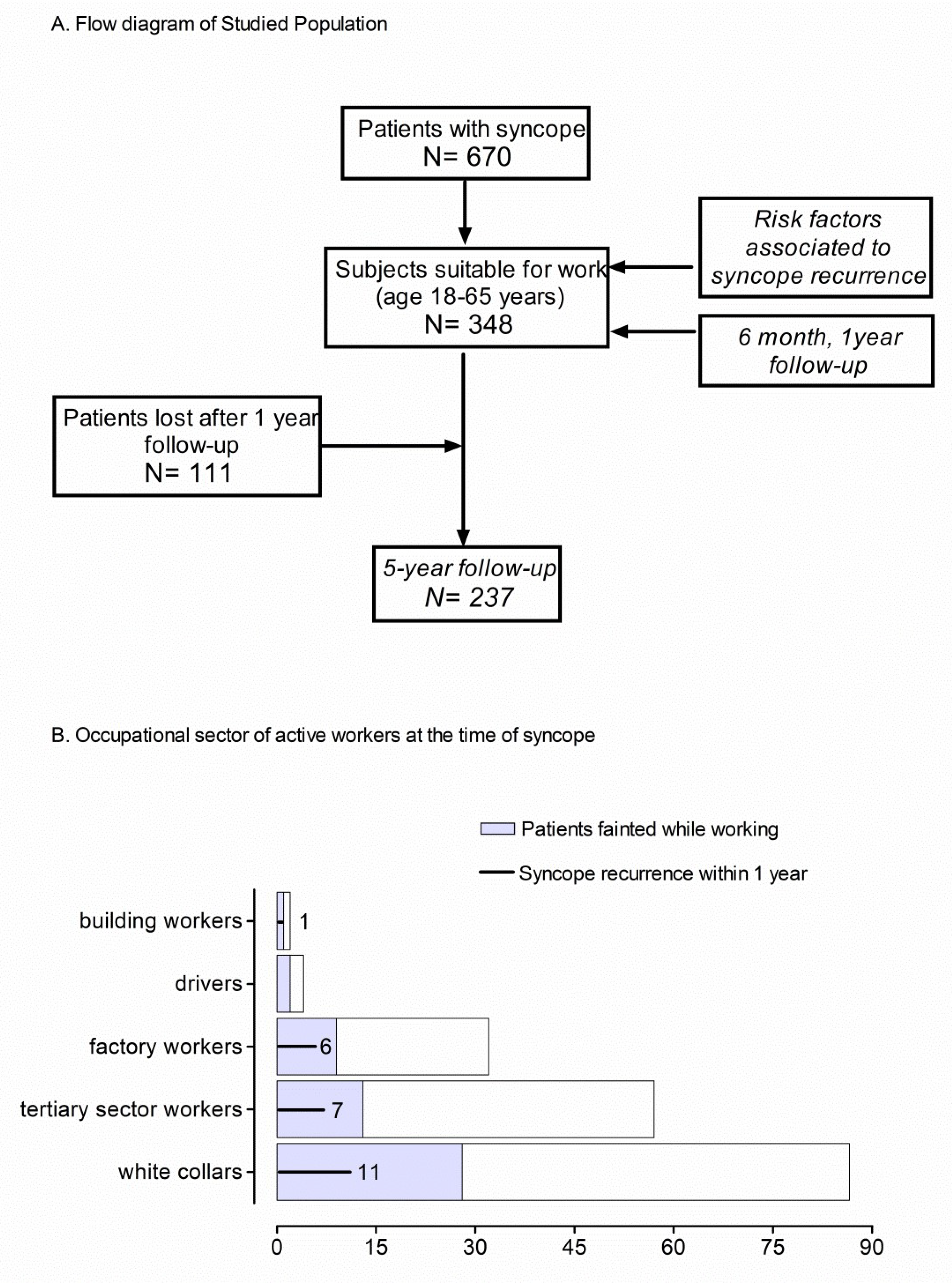
3.1. Population Occupational Profile
3.2. Syncope Recurrences Time Course within 5-Years
3.3. Predictors of Syncope Recurrence at 6-Month and 1-Year Follow-Up
3.4. Six-Month, 1-Year, and 5-Year Prognosis
4. Discussion
- In total, 51.9% of patients presenting to the ED because of syncope were of working-age (18–65 years) and proved to be healthier compared to unselected syncope patients of previous studies (19–22).
- In total, 60.6% of the working age patients were active workers at that time and 25% of them fainted while working.
- The risk of syncope relapse was higher within the first 6 months, i.e., 9.2%, after the index event compared to the remaining follow-up periods (3.5% per year).
- Diabetes, anaemia, and ≥3 lifetime syncope episodes were risk factors independently associated with syncope recurrence at 1-year.
4.1. Syncope in A Working-Age Population
4.2. Risk of Syncope Recurrence in A Working-Age Population
4.3. Predictors of Syncope Recurrence
4.4. Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Soteriades, E.S.; Evans, J.C.; Larson, M.G.; Chen, M.H.; Chen, L.; Benjamin, E.J.; Levy, D. Incidence and prognosis of syncope. N. Engl. J. Med. 2002, 347, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Alboni, P.; Coppola, P.; Stucci, N.; Tsakiridu, V. Differential diagnosis between ‘unexplained’ fall and syncopal fall: A difficult or impossible task. J. Cardiovasc. Med. (Hagerstown) 2015, 16, 82–89. [Google Scholar] [CrossRef]
- Linzer, M.; Pontinen, M.; Gold, D.T.; Divine, G.W.; Felder, A.; Brooks, W.B. Impairment of physical and psychosocial function in recurrent syncope. J. Clin. Epidemiol. 1991, 44, 1037–1043. [Google Scholar] [CrossRef]
- Mosqueda-Garcia, R.; Furlan, R.; Tank, J.; Fernandez-Violante, R. The elusive pathophysiology of neurally mediated syncope. Circulation 2000, 102, 2898–2906. [Google Scholar] [CrossRef] [PubMed]
- Alboni, P.; Alboni, M. Origin and Evolution of the Vasovagal Reflex. In Vasovagal Syncope; Alboni, P., Furlan, R., Eds.; Springer: Cham, Switzerland, 2015; pp. 3–17. [Google Scholar]
- Toarta, C.; Mukarram, M.; Arcot, K.; Kim, S.M.; Gaudet, S.; Sivilotti, M.L.A.; Rowe, B.H.; Thiruganasambandamoorthy, V. Syncope Prognosis Based on Emergency Department Diagnosis: A Prospective Cohort Study. Acad. Emerg. Med. 2018, 25, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Nume, A.K.; Kragholm, K.; Carlson, N.; Kristensen, S.L.; Boggild, H.; Hlatky, M.A.; Torp-Pedersen, C.; Gislason, G.; Ruwald, M.H. Syncope and Its Impact on Occupational Accidents and Employment: A Danish Nationwide Retrospective Cohort Study. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003202. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.C.; Costantino, G.; Barbic, F.; Bossi, I.; Casazza, G.; Dipaola, F.; McDermott, D.; Quinn, J.; Reed, M.; Sheldon, R.S.; et al. Priorities for emergency department syncope research. Ann. Emerg. Med. 2014, 64, 649–655 e642. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.K.; Sheldon, R.S.; Benditt, D.G.; Cohen, M.I.; Forman, D.E.; Goldberger, Z.D.; Grubb, B.P.; Hamdan, M.H.; Krahn, A.D.; Link, M.S.; et al. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2017, 136, e25–e59. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martin, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef] [PubMed]
- Barbic, F.; Borella, M.; Perego, F.; Dipaola, F.; Costantino, G.; Galli, A.; Mantovani, C.; Seghizzi, P.; Malliani, A.; Furlan, R. Syncope and work. STePS study (Short Term Prognosis of Syncope). G. Ital. Med. Lav. Ergon. 2005, 27, 272–274. [Google Scholar]
- Gaggioli, G.; Laffi, M.; Montemanni, M.; Mocini, A.; Rubartelli, P.; Brignole, M. Risk of syncope during work. Europace 2014, 16, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Barbic, F.; Dipaola, F.; Solbiati, M.; Furlan, R. Do work accidents play any role in the increased risk of death observed in 25- to 44-year-old patients after syncope? J. Am. Coll. Cardiol. 2013, 61, 2488–2489. [Google Scholar] [CrossRef]
- Barbic, F.; Casazza, G.; Zamuner, A.R.; Costantino, G.; Orlandi, M.; Dipaola, F.; Capitanio, C.; Achenza, S.; Sheldon, R.; Furlan, R. Driving and working with syncope. Auton. Neurosci. 2014, 184, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Barbic, F.; Sheldon, R.; Furlan, R. Vasovagal Syncope during Driving, Working and Exercise. In Vasovagal Syncope; Alboni, P., Furlan, R., Eds.; Springer: Cham, Switzerland, 2015; pp. 297–307. [Google Scholar]
- Kapoor, W.N. Evaluation and outcome of patients with syncope. Medicine (Baltimore) 1990, 69, 160–175. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, W.N.; Peterson, J.; Wieand, H.S.; Karpf, M. Diagnostic and prognostic implications of recurrences in patients with syncope. Am. J. Med. 1987, 83, 700–708. [Google Scholar] [CrossRef]
- Solbiati, M.; Casazza, G.; Dipaola, F.; Rusconi, A.M.; Cernuschi, G.; Barbic, F.; Montano, N.; Sheldon, R.S.; Furlan, R.; Costantino, G. Syncope recurrence and mortality: A systematic review. Europace 2015, 17, 300–308. [Google Scholar] [CrossRef]
- Costantino, G.; Perego, F.; Dipaola, F.; Borella, M.; Galli, A.; Cantoni, G.; Dell’Orto, S.; Dassi, S.; Filardo, N.; Duca, P.G.; et al. Short- and long-term prognosis of syncope, risk factors, and role of hospital admission: Results from the STePS (Short-Term Prognosis of Syncope) study. J. Am. Coll. Cardiol. 2008, 51, 276–283. [Google Scholar] [CrossRef]
- Sheldon, R.; Raj, S.R.; Rose, M.S.; Morillo, C.A.; Krahn, A.D.; Medina, E.; Talajic, M.; Kus, T.; Seifer, C.M.; Lelonek, M.; et al. Fludrocortisone for the Prevention of Vasovagal Syncope: A Randomized, Placebo-Controlled Trial. J. Am. Coll. Cardiol. 2016, 68, 1–9. [Google Scholar] [CrossRef]
- Sheldon, R.S.; Raj, S.R. Pacing and vasovagal syncope: Back to our physiologic roots. Clin. Auton. Res. 2017, 27, 213–214. [Google Scholar] [CrossRef]
- Brignole, M.; Ungar, A.; Bartoletti, A.; Ponassi, I.; Lagi, A.; Mussi, C.; Ribani, M.A.; Tava, G.; Disertori, M.; Quartieri, F.; et al. Standardized-care pathway vs. usual management of syncope patients presenting as emergencies at general hospitals. Europace 2006, 8, 644–650. [Google Scholar] [CrossRef] [Green Version]
- Sun, B.C.; Emond, J.A.; Camargo, C.A., Jr. Characteristics and admission patterns of patients presenting with syncope to U.S. emergency departments, 1992–2000. Acad. Emerg. Med. 2004, 11, 1029–1034. [Google Scholar] [PubMed]
- Ungar, A.; Tesi, F.; Chisciotti, V.M.; Pepe, G.; Vanni, S.; Grifoni, S.; Balzi, D.; Rafanelli, M.; Marchionni, N.; Brignole, M. Assessment of a structured management pathway for patients referred to the Emergency Department for syncope: Results in a tertiary hospital. Europace 2016, 18, 457–462. [Google Scholar] [CrossRef]
- Sandhu, R.K.; Sheldon, R.S.; Savu, A.; Kaul, P. Nationwide Trends in Syncope Hospitalizations and Outcomes from 2004 to 2014. Can. J. Cardiol. 2017, 33, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Ungar, A.; Del Rosso, A.; Giada, F.; Bartoletti, A.; Furlan, R.; Quartieri, F.; Lagi, A.; Morrione, A.; Mussi, C.; Lunati, M.; et al. Early and late outcome of treated patients referred for syncope to emergency department: The EGSYS 2 follow-up study. Eur. Heart J. 2010, 31, 2021–2026. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Menozzi, C.; Bartoletti, A.; Giada, F.; Lagi, A.; Ungar, A.; Ponassi, I.; Mussi, C.; Maggi, R.; Re, G.; et al. A new management of syncope: Prospective systematic guideline-based evaluation of patients referred urgently to general hospitals. Eur. Heart J. 2006, 27, 76–82. [Google Scholar] [CrossRef]
- Kapoor, W.N.; Karpf, M.; Wieand, S.; Peterson, J.R.; Levey, G.S. A prospective evaluation and follow-up of patients with syncope. N. Engl. J. Med. 1983, 309, 197–204. [Google Scholar] [CrossRef]
- Van Dijk, N.; Sprangers, M.A.; Colman, N.; Boer, K.R.; Wieling, W.; Linzer, M. Clinical factors associated with quality of life in patients with transient loss of consciousness. J. Cardiovasc. Electrophysiol. 2006, 17, 998–1003. [Google Scholar] [CrossRef]
- Santhouse, J.; Carrier, C.; Arya, S.; Fowler, H.; Duncan, S. A comparison of self-reported quality of life between patients with epilepsy and neurocardiogenic syncope. Epilepsia 2007, 48, 1019–1022. [Google Scholar] [CrossRef]
- Canadian Cardiovascular Society. Assessment of the cardiac patient for fitness to drive. Can. J. Cardiol. 1992, 8, 406–411. Available online: https://ccs.ca/images/Guidelines/...POS.../DF_CC_2003_ES.pdf (accessed on 28 January 2019).
- Canadian Cardiovascular Society. Assessment of the cardiac patient for fitness to drive: 1996 update. Can. J. Cardiol. 1996, 12, 1164–1170, 1175–1182. Available online: https://www.ncbi.nlm.nih.gov/pubmed/9191510 (accessed on 28 January 2019).
- Sumner, G.L.; Rose, M.S.; Koshman, M.L.; Ritchie, D.; Sheldon, R.S. Recent history of vasovagal syncope in a young, referral-based population is a stronger predictor of recurrent syncope than lifetime syncope burden. J. Cardiovasc. Electrophysiol. 2010, 21, 1375–1380. [Google Scholar] [CrossRef] [PubMed]
- Malik, P.; Koshman, M.L.; Sheldon, R. Timing of first recurrence of syncope predicts syncopal frequency after a positive tilt table test result. J. Am. Coll. Cardiol. 1997, 29, 1284–1289. [Google Scholar] [CrossRef]
- Sheldon, R.; Rose, S.; Flanagan, P.; Koshman, M.L.; Killam, S. Risk factors for syncope recurrence after a positive tilt-table test in patients with syncope. Circulation 1996, 93, 973–981. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Active Workers | Non-Active Workers | ||
|---|---|---|---|
| Patients Enrolled | n = 348 | n = 211 | n = 137 |
| Age, median “years” (IQR) | 42 (29–54) | 38 (28–48) * | 52 (33–60) |
| Women, n (%) | 199 (57.2) | 126 (59.7) | 73 (53.3) |
| Admitted, n (%) | 52 (14.9) | 26 (12.3) | 26 (19) |
| Discharged n, (%) | 296 (85.1) | 185 (87.7) | 111 (81) |
| Syncope recurrences, 6 m | 32 (9.2) | 20 (9.5) | 12 (8.8) |
| Syncope recurrences, 1 year | 41 (11.8) | 24 (11.4) | 17 (12.4) |
| Past medical history, n (%) | |||
| ≥3 lifetime syncope | 91 (26.1) | 63 (29.8) | 28 (20.4) |
| No comorbidities | 224 (64.4) | 152 (72.0) | 72 (52.6) |
| One or more comorbidities | 124 (35.6) | 59 (28.0) | 65 (47.4) |
| Hypertension | 66 (19.0) | 23 (10.9)* | 43 (31.4) |
| Structural heart disease | 38 (10.9) | 13 (6.2)* | 25 (18.2) |
| Diabetes mellitus | 23 (6.6) | 7 (3.3)* | 16 (11.7) |
| Chronic anaemia | 17 (4.9) | 12 (5.7) | 5 (3.6) |
| Neurological disease | 20 (5.7) | 10 (4.7) | 10 (7.3) |
| COPD | 9 (2.6) | 4 (1.9) | 5 (3.6) |
| Cancer | 7 (2.0) | 4 (1.9) | 3 (2.2) |
| Cerebrovascular disease | 6 (1.7) | 2 (0.9) | 4 (2.9) |
| Ventricular Arrhythmias | 4 (1.1) | 1 (0.5) | 3 (2.2) |
| Heart failure | 3 (0.9) | 0 | 3 (2.2) |
| Index syncope history, n (%) | |||
| Supine/Sitting | 73 (21.0) | 45 (21.3) | 28 (20.4) |
| Upright posture | 266 (76.4) | 161 (76.3) | 105 (76.6) |
| During exercise | 9 (2.6) | 5 (2.4) | 4 (2.9) |
| Trauma, n (%) | 70 (20.1) | 49 (23.2) | 21 (15.3) |
| Abnormal ECG, n (%) | 56 (16.1) | 27 (12.8) | 29 (21.2) |
| Absence of prodromes n (%) | 71 (20.4) | 40 (19.0) | 31 (22.6) |
| First syncope, n (%) | 141 (40.5) | 93 (44.1) | 48 (35.0) |
| 6-Months | 1-Year | |||||
|---|---|---|---|---|---|---|
| Univariable Analysis | Univariable Analysis | Multivariable Analysis | ||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Age > 40 “years” | 1.84 (0.86–3.94) | 0.12 | 1.49 (0.77–2.91) | 0.24 | - | |
| Gender | 1.10 (0.53–2.31) | 0.79 | 1.19 (0.61–2.33) | 0.60 | - | |
| No Hospital admission | 2.82 (0.65–12.17) | 0.17 | 1.71 (0.58–5.03) | 0.33 | - | |
| Abnormal ECG | 1.53 (0.63–3.72) | 0.35 | 2.14 (1.00–4.56) | 0.05 | - | |
| First syncopal episode | 1.33 (0.62–2.86) | 0.46 | 1.36 (0.69–2.7) | 0.38 | - | |
| Syncopal episodes ≥ 3 | 2.10 (0.99–4.42) | 0.05 | 2.23 (1.14–4.38) | 0.02 | 2.06 (1.03–4.10) | 0.04 |
| Trauma | 1.85 (0.63–5.45) | 0.27 | 1.54 (0.62–3.81) | 0.35 | - | |
| Absence of prodromal symptoms | 1.43 (0.53–3.84) | 0.48 | 1.28 (0.54–3.02) | 0.57 | - | |
| Cardiovascular Disease | 1.74 (0.67–4.51) | 0.25 | 1.25 (0.49–3.18) | 0.64 | - | |
| Neoplasm | 1.67 (0.19–14.29) | 0.64 | 1.25 (0.15–10.69) | 0.84 | - | |
| Neurological Disease | 2.68 (0.84–8.57) | 0.10 | 1.97 (0.62–6.20) | 0.25 | - | |
| COPD | 2.95 (0.59–14.81) | 0.19 | 2.2 (0.44–10.96) | 0.34 | - | |
| Diabetes | 1.53 (0.43–5.46) | 0.51 | 2.93 (1.08–7.91) | 0.03 | 2.85 (1.04–7.83) | 0.04 |
| Hypertension | 1.22 (0.50–2.95) | 0.66 | 1.23 (0.56–2.73) | 0.60 | - | |
| Anemia | 2.68 (0.84–8.57) | 0.10 | 3.59 (1.30–9.94) | 0.01 | 3.51 (1.25–9.83) | 0.02 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbic, F.; Dipaola, F.; Casazza, G.; Borella, M.; Minonzio, M.; Solbiati, M.; Raj, S.R.; Sheldon, R.; Quinn, J.; Costantino, G.; et al. Syncope in a Working-Age Population: Recurrence Risk and Related Risk Factors. J. Clin. Med. 2019, 8, 150. https://doi.org/10.3390/jcm8020150
Barbic F, Dipaola F, Casazza G, Borella M, Minonzio M, Solbiati M, Raj SR, Sheldon R, Quinn J, Costantino G, et al. Syncope in a Working-Age Population: Recurrence Risk and Related Risk Factors. Journal of Clinical Medicine. 2019; 8(2):150. https://doi.org/10.3390/jcm8020150
Chicago/Turabian StyleBarbic, Franca, Franca Dipaola, Giovanni Casazza, Marta Borella, Maura Minonzio, Monica Solbiati, Satish R. Raj, Robert Sheldon, James Quinn, Giorgio Costantino, and et al. 2019. "Syncope in a Working-Age Population: Recurrence Risk and Related Risk Factors" Journal of Clinical Medicine 8, no. 2: 150. https://doi.org/10.3390/jcm8020150