Strengthening the Brain—Is Resistance Training with Blood Flow Restriction an Effective Strategy for Cognitive Improvement?

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Effects and Mechanisms of Resistance Training on Cognition
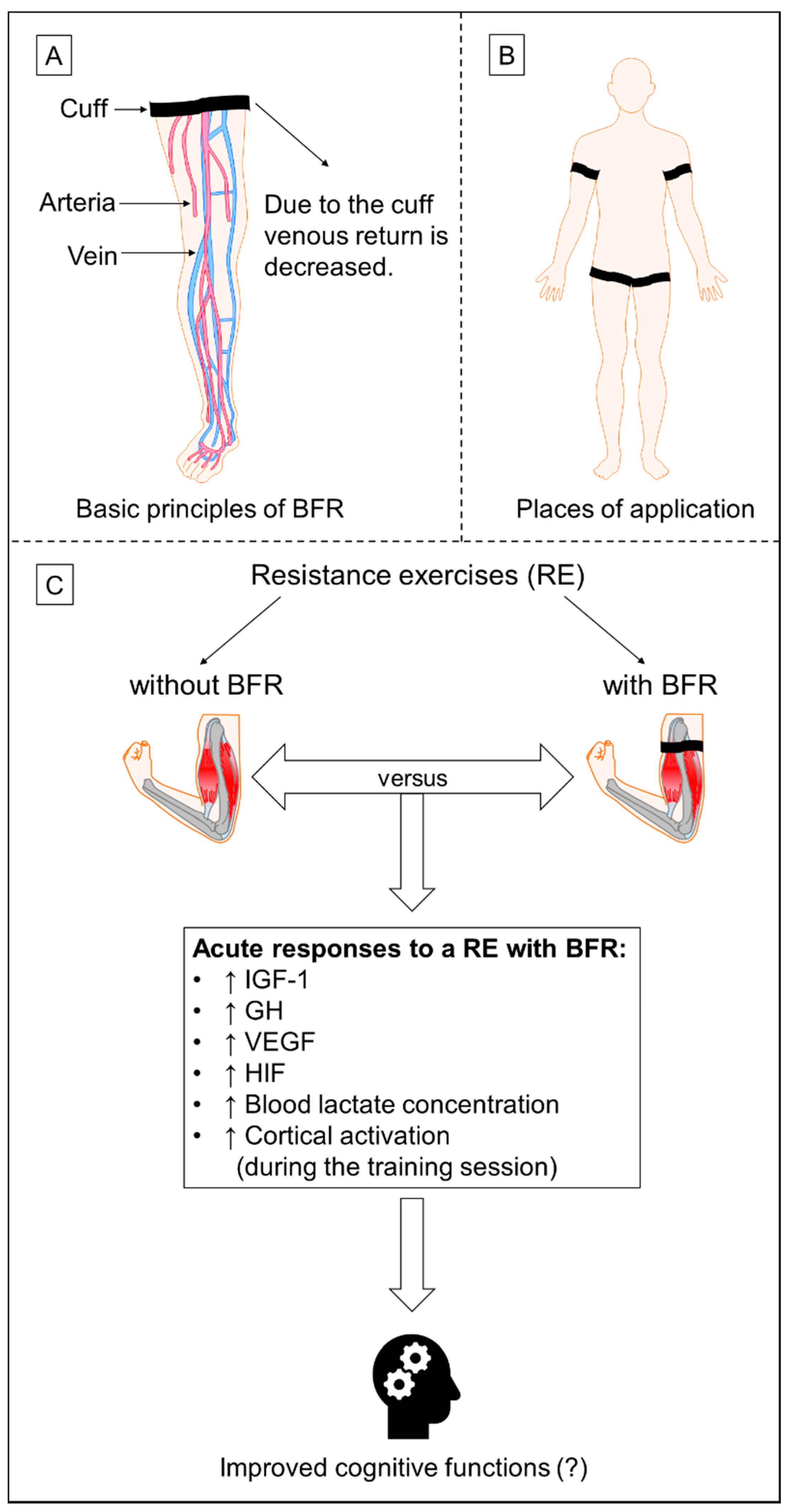
3. Resistance Training with Blood Flow Restriction—An Added Value for Cognition?
3.1. Hypothesis
3.2. Considerations to Evaluate the Hypothesis
- (1)
- load (amount of weight that is used for an exercise; usually given as a percentage of the one repetition maximum [1RM]);
- (2)
- number of repetitions;
- (3)
- number of sets;
- (4)
- inter-set rest periods;
- (5)
- inter-exercise rest periods;
- (6)
- number of exercises (for the whole training session or for a muscle or a muscle group with the same function);
- (7)
- repetition velocity (temporal details should be given for: concentric phase–inter-repetition rest periods–eccentric phase rest period up to the start of the next repetition, e.g., 2–0–2–1 s);
- (8)
- muscle action (concentric, eccentric, isometric);
- (9)
- exercise selection (e.g., multi-joint or single joint exercises);
- (10)
- exercise order (e.g., squat, leg extension, biceps curl and concentration curl or squat, biceps curl, leg extension and concentration curl);
- (11)
- volitional muscle failure
- (12)
- range of motion.
- (13)
- frequency (number of training sessions per week);
- (14)
- density (distribution of training sessions across a week with regard to recovery time in-between training sessions) and
- (15)
- duration (duration over which a training program is carried out before exercise variables are changed).
- (1)
- (2)
- Cuff material: it might be that the cuff material has an impact on the arterial blood flow restriction [211]. However, current investigations comparing different cuff materials (5 cm nylon vs. 3 cm elastic cuffs) do not consider the cuff width [223]. In contrast, Loenneke et al. [224] compared nylon and elastic cuffs with the same width (5 cm) and observed no differences in the arterial occlusion pressure [224].
- (3)
- Restricted extremity (upper or lower limbs): cuff pressures should be determined individually for the upper and lower limbs [225].
- (4)
- (5)
- (6)
- (7)
- (8)
- Blood flow restriction system: different blood flow restriction systems (automatic pressure control vs. manual handheld pressure control) lead to diverging pressure on the limbs at rest and during exercise. However, one first investigation by Hughes et al. [239] compared several blood flow restriction systems with different cuff widths. Therefore, the influence of blood flow restriction systems for inducing effective BFR-stimuli needs further investigations [239].
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Adams, K.J.; O’Shea, P.; O’Shea, K.L. Aging: Its effects on strength, power, flexibility, and bone density. Strength Cond. J. 1999, 21, 65–77. [Google Scholar] [CrossRef]
- Goldspink, G. Age-related loss of muscle mass and strength. J. Aging Res. 2012, 2012, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Keller, K.; Engelhardt, M. Strength and muscle mass loss with aging process. Age and strength loss. MLTJ 2013, 3, 346–350. [Google Scholar] [PubMed]
- Davis, J.W.; Ross, P.D.; Preston, S.D.; Nevitt, M.C.; Wasnich, R.D. Strength, physical activity, and body mass index: Relationship to performance-based measures and activities of daily living among older Japanese women in Hawaii. J. Am. Geriatr. Soc. 1998, 46, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Rantanen, T.; Avlund, K.; Suominen, H.; Schroll, M.; Frändin, K.; Pertti, E. Muscle strength as a predictor of onset of ADL dependence in people aged 75 years. Aging Clin. Exp. Res. 2002, 14, 10–15. [Google Scholar] [PubMed]
- Wolfson, L.; JUDGE, J.; Whipple, R.; King, M. Strength is a major factor in balance, gait, and the occurrence of falls. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, 64–67. [Google Scholar] [PubMed]
- Horlings, C.G.C.; van Engelen, B.G.M.; Allum, J.H.J.; Bloem, B.R. A weak balance: The contribution of muscle weakness to postural instability and falls. Nat. Clin. Pract. Neurol. 2008, 4, 504–515. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Stuart, A.L.; Kay, D.; Ebeling, P.R.; Nicholson, G.; Sanders, K.M. Investigating the predictive ability of gait speed and quadriceps strength for incident falls in community-dwelling older women at high risk of fracture. Arch. Gerontol. Geriatr. 2014, 58, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Kilgour, A.H.M.; Todd, O.M.; Starr, J.M. A systematic review of the evidence that brain structure is related to muscle structure and their relationship to brain and muscle function in humans over the lifecourse. BMC Geriatr. 2014, 14, 85. [Google Scholar] [CrossRef] [PubMed]
- Tolea, M.I.; Galvin, J.E. Sarcopenia and impairment in cognitive and physical performance. Clin. Interv. Aging 2015, 10, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.M.; Johnson, D.K.; Watts, A.; Swerdlow, R.H.; Brooks, W.M. Reduced lean mass in early Alzheimer disease and its association with brain atrophy. Arch. Neurol. 2010, 67, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Nourhashémi, F.; Andrieu, S.; Gillette-Guyonnet, S.; Reynish, E.; Albarede, J.-L.; Grandjean, H.; Vellas, B. Is there a relationship between fat-free soft tissue mass and low cognitive function? Results from a study of 7,105 women. J. Am. Geriatr. Soc. 2002, 50, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Hedden, T.; Gabrieli, J.D.E. Insights into the ageing mind: A view from cognitive neuroscience. Nat. Rev. Neurosci. 2004, 5, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Park, D.C.; Lautenschlager, G.; Hedden, T.; Davidson, N.S.; Smith, A.D.; Smith, P.K. Models of visuospatial and verbal memory across the adult life span. Psychol. Aging 2002, 17, 299–320. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.S. The ageing brain: Normal and abnormal memory. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1997, 352, 1703–1709. [Google Scholar] [CrossRef] [PubMed]
- Buckner, R.L. Memory and executive function in aging and AD: Multiple factors that cause decline and reserve factors that compensate. Neuron 2004, 44, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Fjell, A.M.; Walhovd, K.B. Structural brain changes in aging: Courses, causes and cognitive consequences. Rev. Neurosci. 2010, 21, 187–221. [Google Scholar] [CrossRef] [PubMed]
- Fiest, K.M.; Jette, N.; Roberts, J.I.; Maxwell, C.J.; Smith, E.E.; Black, S.E.; Blaikie, L.; Cohen, A.; Day, L.; Holroyd-Leduc, J.; et al. The prevalence and incidence of dementia: A systematic review and meta-analysis. Can. J. Neurol. Sci. 2016, 43, 35. [Google Scholar] [CrossRef] [PubMed]
- Berr, C.; Wancata, J.; Ritchie, K. Prevalence of dementia in the elderly in Europe. Eur. Neuropsychopharmacol. 2005, 15, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Scherder, E.; Eggermont, L.; Visscher, C.; Scheltens, P.; Swaab, D. Understanding higher level gait disturbances in mild dementia in order to improve rehabilitation: ‘Last in–first out’. Neurosci. Biobehav. Rev. 2011, 35, 699–714. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Jonsson, L.; Bond, J.; Prince, M.; Winblad, B. The worldwide economic impact of dementia 2010. Alzheimers. Dement. 2013, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Prina, A.M.; Winblad, B.; Jönsson, L.; Liu, Z.; Prince, M. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers. Dement. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, L.; Wimo, A. The cost of dementia in Europe: A review of the evidence, and methodological considerations. Pharmacoeconomics 2009, 27, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Hurd, M.D.; Martorell, P.; Delavande, A.; Mullen, K.J.; Langa, K.M. Monetary costs of dementia in the United States. N. Engl. J. Med. 2013, 368, 1326–1334. [Google Scholar] [CrossRef] [PubMed]
- Tariot, P.N. Pharmacological treatment of neuropsychiatric symptoms of dementia. JAMA 2005, 293, 2212. [Google Scholar] [CrossRef] [PubMed]
- Ringman, J.M.; Cummings, J.L. Current and emerging pharmacological treatment options for dementia. Behav. Neurol. 2006, 17, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. Pharmacologic options for the treatment of Sarcopenia. Calcif. Tissue Int. 2016, 98, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, S.; Froelich, L.; Burns, A. Pharmacological treatment of dementia. Curr. Opin. Psychiatry 2012, 25, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Van de Glind, E.M.M.; van Enst, W.A.; van Munster, B.C.; Olde Rikkert, M.G.M.; Scheltens, P.; Scholten, R.J.P.M.; Hooft, L. Pharmacological treatment of dementia: A scoping review of systematic reviews. Dement. Geriatr. Cogn. Disord. 2013, 36, 211–228. [Google Scholar] [CrossRef] [PubMed]
- Burton, L.A.; Sumukadas, D. Optimal management of sarcopenia. CIA 2010, 5, 217. [Google Scholar] [CrossRef] [Green Version]
- Paillard-Borg, S.; Fratiglioni, L.; Winblad, B.; Wang, H.-X. Leisure activities in late life in relation to dementia risk: Principal component analysis. Dement. Geriatr. Cogn. Disord. 2009, 28, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Rovio, S.; Kåreholt, I.; Helkala, E.-L.; Viitanen, M.; Winblad, B.; Tuomilehto, J.; Soininen, H.; Nissinen, A.; Kivipelto, M. Leisure-time physical activity at midlife and the risk of dementia and Alzheimer’s disease. Lancet Neurol. 2005, 4, 705–711. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Herod, S.M.; Cardinal, B.J.; Noakes, T.D. Physical activity and the brain: A review of this dynamic, bi-directional relationship. Brain Res. 2013, 1539, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Ponce, P.; Loprinzi, P.D. A bi-directional model of exercise and episodic memory function. Med. Hypotheses 2018, 117, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Pentikäinen, H.; Savonen, K.; Komulainen, P.; Kiviniemi, V.; Paajanen, T.; Kivipelto, M.; Soininen, H.; Rauramaa, R. Muscle strength and cognition in ageing men and women: The DR’s EXTRA study. Eur. Geriatr. Med. 2017, 8, 275–277. [Google Scholar] [CrossRef]
- Chen, W.-L.; Peng, T.-C.; Sun, Y.-S.; Yang, H.-F.; Liaw, F.-Y.; Wu, L.-W.; Chang, Y.-W.; Kao, T.-W. Examining the association between quadriceps strength and cognitive performance in the elderly. Medicine 2015, 94, e1335. [Google Scholar] [CrossRef] [PubMed]
- Alfaro-Acha, A.; Al Snih, S.; Raji, M.A.; Kuo, Y.-F.; Markides, K.S.; Ottenbacher, K.J. Handgrip strength and cognitive decline in older Mexican Americans. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Lustig, C.; Shah, P.; Seidler, R.; Reuter-Lorenz, P.A. Aging, training, and the brain: A review and future directions. Neuropsychol. Rev. 2009, 19, 504–522. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; van Abellan Kan, G.; Vellas, B. Healthy brain aging: Role of exercise and physical activity. Clin. Geriatr. Med. 2010, 26, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. J. Aging Res. 2013. [Google Scholar] [CrossRef] [PubMed]
- Voelcker-Rehage, C.; Niemann, C. Structural and functional brain changes related to different types of physical activity across the life span. Neurosci. Biobehav. Rev. 2013, 37, 2268–2295. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Abrahamson, K. Does exercise impact cognitive performance research article op in community-dwelling older adults with mild cognitive impairment? A systematic review. Qual. Prim. Care 2015, 23, 214–222. [Google Scholar]
- Esteban-Cornejo, I.; Tejero-Gonzalez, C.M.; SALLIS, J.F.; Veiga, O.L. Physical activity and cognition in adolescents: A systematic review. J. Sci. Med. Sport 2015, 18, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Lautenschlager, N.T. Twelve months of resistance training can improve the cognitive functioning of older women living in the community. J. Physiother. 2010, 56, 200. [Google Scholar] [CrossRef]
- Powell, K.E.; Paluch, A.E.; Blair, S.N. Physical activity for health: What kind? How much? How intense? On top of what? Annu. Rev. Public Health 2011, 32, 349–365. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Schmicker, M.; Müller, N.G. Präventionsstrategien gegen Demenz. Z. Gerontol. Geriatr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Herold, F.; Hamacher, D.; Schega, L.; Müller, N.G. Thinking while Moving or Moving while Thinking—Concepts of motor-cognitive training for cognitive performance enhancement. Front. Aging Neurosci. 2018, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Bryan, S.; Marra, C.A.; Hsiung, G.-Y.R.; Liu-Ambrose, T. Challenges with cost-utility analyses of behavioural interventions among older adults at risk for dementia. Br. J. Sports Med. 2015, 49, 1343–1347. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Marra, C.A.; Robertson, M.C.; Najafzadeh, M.; Liu-Ambrose, T. Sustained economic benefits of resistance training in community-dwelling senior women. J. Am. Geriatr. Soc. 2011, 59, 1232–1237. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Bryan, S.; Marra, C.A.; Sharma, D.; Chan, A.; Beattie, B.L.; Graf, P.; Liu-Ambrose, T. An economic evaluation of resistance training and aerobic training versus balance and toning exercises in older adults with mild cognitive impairment. PLoS ONE 2013, 8, e63031. [Google Scholar] [CrossRef] [PubMed]
- Ashton, R.E.; Tew, G.A.; Aning, J.J.; Gilbert, S.E.; Lewis, L.; Saxton, J.M. Effects of short-term, medium-term and long-term resistance exercise training on cardiometabolic health outcomes in adults: Systematic review with meta-analysis. Br. J. Sports Med. 2018. [Google Scholar] [CrossRef]
- Hunter, G.R.; McCarthy, J.P.; Bamman, M.M. Effects of resistance training on older adults. Sports Med. 2004, 34, 329–348. [Google Scholar] [CrossRef] [PubMed]
- Hurley, B.F.; Hanson, E.D.; Sheaff, A.K. Strength training as a countermeasure to aging muscle and chronic disease. Sports Med. 2011, 41, 289–306. [Google Scholar] [CrossRef] [PubMed]
- Hurley, B.F.; Roth, S.M. Strength Training in the Elderly. Sports Med. 2000, 30, 249–268. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, W.J.; Ratamess, N.A.; French, D.N. Resistance Training for Health and Performance. Curr. Sports Med. Rep. 2002, 1, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Shaw, B.S.; Shaw, I.; Brown, G.A. Resistance exercise is medicine: Strength training in health promotion and rehabilitation. Int. J. Ther. Rehabilit. 2015, 22, 385–389. [Google Scholar] [CrossRef]
- Winett, R.A.; Carpinelli, R.N. Potential health-related benefits of resistance training. Prev. Med. 2001, 33, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Westcott, W.L. Resistance training is medicine: Effects of strength training on health. Curr. Sports Med. Rep. 2012, 11, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-K.; Pan, C.-Y.; Chen, F.-T.; Tsai, C.-L.; Huang, C.-C. Effect of resistance-exercise training on cognitive function in healthy older adults: A review. J. Aging Phys. Act. 2012, 20, 497–517. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Donaldson, M.G. Exercise and cognition in older adults: Is there a role for resistance training programmes? Br. J. Sports Med. 2009, 43, 25–27. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J.; Herring, M.P.; Caravalho, A. Mental health benefits of strength training in adults. Am. J. Lifestyle Med. 2010, 4, 377–396. [Google Scholar] [CrossRef]
- Soga, K.; Masaki, H.; Gerber, M.; Ludyga, S. Acute and long-term effects of resistance training on executive function. J. Cogn. Enhanc. 2018, 56, 729. [Google Scholar] [CrossRef]
- Altug, Z. Resistance exercise to improve cognitive function. J. Strength Cond. 2014, 36, 46–50. [Google Scholar] [CrossRef]
- Voss, M.W.; Nagamatsu, L.S.; Liu-Ambrose, T.; Kramer, A.F. Exercise, brain, and cognition across the life span. J. Appl. Physiol. 2011, 111, 1505–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stillman, C.M.; Cohen, J.; Lehman, M.E.; Erickson, K.I. Mediators of physical activity on neurocognitive function: A review at multiple levels of analysis. Front. Hum. Neurosci. 2016, 10, 626. [Google Scholar] [CrossRef] [PubMed]
- Barha, C.K.; Galea, L.A.; Nagamatsu, L.S.; Erickson, K.I.; Liu-Ambrose, T. Personalising exercise recommendations for brain health: Considerations and future directions. Br. J. Sports Med. 2017, 51, 636–639. [Google Scholar] [CrossRef] [PubMed]
- Cassilhas, R.C.; Lee, K.S.; Venâncio, D.P.; Oliveira, M.G.M.; Tufik, S.; Mello, M.T. de. Resistance exercise improves hippocampus-dependent memory. Braz. J. Med. Biol. Res. 2012, 45, 1215–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassilhas, R.C.; Lee, K.S.; Fernandes, J.; Oliveira, M.G.M.; Tufik, S.; Meeusen, R.; Mello de, M.T. Spatial memory is improved by aerobic and resistance exercise through divergent molecular mechanisms. Neurosci. 2012, 202, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Ohlsson, C.; Mohan, S.; Sjögren, K.; Tivesten, A.; Isgaard, J.; Isaksson, O.; Jansson, J.-O.; Svensson, J. The role of liver-derived insulin-like growth factor-I. Endocr. Rev. 2009, 30, 494–535. [Google Scholar] [CrossRef] [PubMed]
- Gubbi, S.; Quipildor, G.F.; Barzilai, N.; Huffman, D.M.; Milman, S. 40 years of IGF1: IGF1: The Jekyll and Hyde of the aging brain. J. Mol. Endocrinol. 2018, 61, T171–T185. [Google Scholar] [CrossRef] [PubMed]
- Bassil, F.; Fernagut, P.-O.; Bezard, E.; Meissner, W.G. Insulin, IGF-1 and GLP-1 signaling in neurodegenerative disorders: Targets for disease modification? Prog. Neurobiol. 2014, 118, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Dyer, A.H.; Vahdatpour, C.; Sanfeliu, A.; Tropea, D. The role of insulin-like growth factor 1 (IGF-1) in brain development, maturation and neuroplasticity. Neuroscience 2016, 325, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Deak, F.; Sonntag, W.E. Aging, synaptic dysfunction, and insulin-like growth factor (IGF)-1. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67A, 611–625. [Google Scholar] [CrossRef] [PubMed]
- Aberg, N.D.; Brywe, K.G.; Isgaard, J. Aspects of growth hormone and insulin-like growth factor-I related to neuroprotection, regeneration, and functional plasticity in the adult brain. Sci. World J. 2006, 6, 53–80. [Google Scholar] [CrossRef] [PubMed]
- Toth, P.; Tarantini, S.; Ashpole, N.M.; Tucsek, Z.; Milne, G.L.; Valcarcel-Ares, N.M.; Menyhart, A.; Farkas, E.; Sonntag, W.E.; Csiszar, A.; et al. IGF-1 deficiency impairs neurovascular coupling in mice: Implications for cerebromicrovascular aging. Aging Cell 2015, 14, 1034–1044. [Google Scholar] [CrossRef] [PubMed]
- Saber, H.; Himali, J.J.; Beiser, A.S.; Shoamanesh, A.; Pikula, A.; Roubenoff, R.; Romero, J.R.; Kase, C.S.; Vasan, R.S.; Seshadri, S. Serum insulin-like growth factor 1 and the risk of ischemic stroke: The framingham study. Stroke 2017, 48, 1760–1765. [Google Scholar] [CrossRef] [PubMed]
- Arwert, L.I.; Deijen, J.B.; Drent, M.L. The relation between insulin-like growth factor I levels and cognition in healthy elderly: A meta-analysis. Growth Horm. IGF Res. 2005, 15, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Calvo, D.; Gunstad, J.; Miller, L.A.; Glickman, E.; Spitznagel, M.B. Higher serum insulin-like growth factor-1 is associated with better cognitive performance in persons with mild cognitive impairment. Psychogeriatrics 2013, 13, 170–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westwood, A.J.; Beiser, A.; DeCarli, C.; Harris, T.B.; Chen, T.C.; He, X.-M.; Roubenoff, R.; Pikula, A.; Au, R.; Braverman, L.E.; et al. Insulin-like growth factor-1 and risk of Alzheimer dementia and brain atrophy. Neurology 2014, 82, 1613–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas Vega, S.; Knicker, A.; Hollmann, W.; Bloch, W.; Strüder, H.K. Effect of resistance exercise on serum levels of growth factors in humans. Horm. Metab. Res. 2010, 42, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.-L.; Wang, C.-H.; Pan, C.-Y.; Chen, F.-C. The effects of long-term resistance exercise on the relationship between neurocognitive performance and GH, IGF-1, and homocysteine levels in the elderly. Front. Behav. Neurosci. 2015, 9, 471. [Google Scholar] [CrossRef] [PubMed]
- Borst, S.E.; Hoyos de, D.V.; Garzarella, L.; Vincent, K.; Pollock, B.H.; Lowenthal, D.T.; Pollock, M.L. Effects of resistance training on insulin-like growth factor-I and IGF binding proteins. Med. Sci. Sports Exerc. 2001, 33, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.M.; Silva, T.M.V.; Coelho, F.G.D.M.; Arantes, F.J.; Costa, J.L.R.; Teodoro, E.; Santos-Galduróz, R.F. Physical exercise, IGF-1 and cognition A systematic review of experimental studies in the elderly. Dement. Neuropsychol. 2018, 12, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Fontes, E.B.; Libardi, C.A.; Castellano, G.; Okano, A.H.; Fernandes, P.T.; Chacon-Mikahil, M.P.; Ugrinowitsch, C.; Cavaglieri, C.R.; Li, L.M. Effects of resistance training in gray matter density of elderly. Sport Sci. Health 2017, 13, 233–238. [Google Scholar] [CrossRef]
- Suo, C.; Singh, M.F.; Gates, N.; Wen, W.; Sachdev, P.; Brodaty, H.; Saigal, N.; Wilson, G.C.; Meiklejohn, J.; Singh, N.; et al. Therapeutically relevant structural and functional mechanisms triggered by physical and cognitive exercise. Mol. Psychiatry 2016, 21, 1633–1642. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Nagamatsu, L.S.; Graf, P.; Beattie, B.L.; Ashe, M.C.; Handy, T.C. Resistance training and executive functions: A 12-month randomized controlled trial. Arch. Intern. Med. 2010, 170, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Fox, N.C.; Black, R.S.; Gilman, S.; Rossor, M.N.; Griffith, S.G.; Jenkins, L.; Koller, M. Effects of Abeta immunization (AN1792) on MRI measures of cerebral volume in Alzheimer disease. Neurology 2005, 64, 1563–1572. [Google Scholar] [CrossRef] [PubMed]
- Ströhlein, J.K.; van den Bongard, F.; Barthel, T.; Reinsberger, C. Dose-response-relationship between physical activity and cognition in elderly. Dtsch. Z. Sportmed. 2017, 2017, 234–242. [Google Scholar] [CrossRef]
- Voss, M.W.; Vivar, C.; Kramer, A.F.; van Praag, H. Bridging animal and human models of exercise-induced brain plasticity. Trends Cogn. Sci. 2013, 17, 525–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stimpson, N.J.; Davison, G.; Javadi, A.-H. Joggin’ the noggin: Towards a physiological understanding of exercise-induced cognitive benefits. Neurosci. Biobehav. Rev. 2018, 88, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Osman, J.; Cabral, D.F.; Morris, T.P.; McInerney, K.; Cahalin, L.P.; Rundek, T.; Oliveira, A.; Pascual-Leone, A. Exercise for cognitive brain health in aging. Neurol. Clin. Pract. 2018, 8, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Best, J.R.; Chiu, B.K.; Liang Hsu, C.; Nagamatsu, L.S.; Liu-Ambrose, T. Long-term effects of resistance exercise training on cognition and brain volume in older women: Results from a randomized controlled trial. J. Int. Neuropsychol. Soc. 2015, 21, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Bolandzadeh, N.; Tam, R.; Handy, T.C.; Nagamatsu, L.S.; Hsu, C.L.; Davis, J.C.; Dao, E.; Beattie, B.L.; Liu-Ambrose, T. Resistance training and white matter lesion progression in older women: Exploratory analysis of a 12-month randomized controlled trial. J. Am. Geriatr. Soc. 2015, 63, 2052–2060. [Google Scholar] [CrossRef] [PubMed]
- de Groot, J.C.; de Leeuw, F.E.; Oudkerk, M.; van Gijn, J.; Hofman, A.; Jolles, J.; Breteler, M.M. Cerebral white matter lesions and cognitive function: The rotterdam scan study. Ann. Neurol. 2000, 47, 145–151. [Google Scholar] [CrossRef]
- Gunning-Dixon, F.M.; Raz, N. The cognitive correlates of white matter abnormalities in normal aging: A quantitative review. Neuropsychology 2000, 14, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Vernooij, M.W.; Ikram, M.A.; Vrooman, H.A.; Wielopolski, P.A.; Krestin, G.P.; Hofman, A.; Niessen, W.J.; van der Lugt, A.; Breteler, M.M.B. White matter microstructural integrity and cognitive function in a general elderly population. Arch. Gen. Psychiatry 2009, 66, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Gunning-Dixon, F.M.; Brickman, A.M.; Cheng, J.C.; Alexopoulos, G.S. Aging of cerebral white matter: A review of MRI findings. Int. J. Geriatr. Psychiatry 2009, 24, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Alves, C.R.R.; Tessaro, V.H.; Teixeira, L.A.C.; Murakava, K.; Roschel, H.; Gualano, B.; Takito, M.Y. Influence of acute high-intensity aerobic interval exercise bout on selective attention and short-term memory tasks. Percept. Mot. Skills 2014, 118, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Kim, K.; Jung, Y.-J.; Kato, M. Effects of acute high-intensity resistance exercise on cognitive function and oxygenation in prefrontal cortex. J. Exerc. Nutrition Biochem. 2017, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Nagamatsu, L.S.; Voss, M.W.; Khan, K.M.; Handy, T.C. Resistance training and functional plasticity of the aging brain: A 12-month randomized controlled trial. Neurobiol. Aging 2012, 33, 1690–1698. [Google Scholar] [CrossRef] [PubMed]
- Nagamatsu, L.S.; Handy, T.C.; Hsu, C.L.; Voss, M.; Liu-Ambrose, T. Resistance training promotes cognitive and functional brain plasticity in seniors with probable mild cognitive impairment. Arch. Intern. Med. 2012, 172, 666–668. [Google Scholar] [CrossRef] [PubMed]
- Coetsee, C.; Terblanche, E. Cerebral oxygenation during cortical activation: The differential influence of three exercise training modalities. A randomized controlled trial. Eur. J. Appl. Physiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Firth, J.A.; Stubbs, B.; Vancampfort, D.; Schuch, F.B.; Hallgren, M.; Veronese, N.; Yung, A.R.; Sarris, J. Association Between Muscular Strength and Cognition in People With Major Depression or Bipolar Disorder and Healthy Controls. JAMA Psychiatry 2018. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Stubbs, B.; Vancampfort, D.; Firth, J.A.; Large, M.; Rosenbaum, S.; Hallgren, M.; Ward, P.B.; Sarris, J.; Yung, A.R. Grip Strength Is Associated With Cognitive Performance in Schizophrenia and the General Population: A UK Biobank Study of 476559 Participants. Schizophrenia Bull. 2018, 44, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Steves, C.J.; Mehta, M.M.; Jackson, S.H.D.; Spector, T.D. Kicking Back Cognitive Ageing: Leg Power Predicts Cognitive Ageing after Ten Years in Older Female Twins. Gerontology 2016, 62, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Buckner, S.L.; Dankel, S.J.; Mouser, J.G.; Mattocks, K.T.; Jessee, M.B.; Loenneke, J.P. Chasing the top quartile of cross-sectional data: Is it possible with resistance training? Med. Hypotheses 2017, 108, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Decker, L.M.; Cignetti, F.; Stergiou, N. Executive function orchestrates regulation of task-relevant gait fluctuations. Gait Posture 2013, 38, 537–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IJmker, T.; Lamoth, C.J.C. Gait and cognition: The relationship between gait stability and variability with executive function in persons with and without dementia. Gait Posture 2012, 35, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Kearney, F.C.; Harwood, R.H.; Gladman, J.R.F.; Lincoln, N.; Masud, T. The relationship between executive function and falls and gait abnormalities in older adults: A systematic review. Dement. Geriatr. Cogn. Disord. 2013, 36, 20–35. [Google Scholar] [CrossRef] [PubMed]
- Herold, F.; Wiegel, P.; Scholkmann, F.; Thiers, A.; Hamacher, D.; Schega, L. Functional near-infrared spectroscopy in movement science: A systematic review on cortical activity in postural and walking tasks. Neurophoton 2017, 4, 41403. [Google Scholar] [CrossRef] [PubMed]
- Hamacher, D.; Herold, F.; Wiegel, P.; Hamacher, D.; Schega, L. Brain activity during walking: A systematic review. Neurosci. Biobehav. Rev. 2015, 57, 310–327. [Google Scholar] [CrossRef] [PubMed]
- Saraçlı, Ö.; Akca, A.S.D.; Atasoy, N.; Önder, Ö.; Şenormancı, Ö.; Kaygisız, I.; Atik, L. The relationship between quality of life and cognitive functions, anxiety and depression among hospitalized elderly patients. Clin. Psychopharmacol. Neurosci. 2015, 13, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Kekäläinen, T.; Kokko, K.; Sipilä, S.; Walker, S. Effects of a 9-month resistance training intervention on quality of life, sense of coherence, and depressive symptoms in older adults: Randomized controlled trial. Qual. Life Res. 2018, 27, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Barha, C.K.; Davis, J.C.; Falck, R.S.; Nagamatsu, L.S.; Liu-Ambrose, T. Sex differences in exercise efficacy to improve cognition: A systematic review and meta-analysis of randomized controlled trials in older humans. Front. Neuroendocrinol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Jessee, M.B.; Mattocks, K.T.; Buckner, S.L.; Dankel, S.J.; Mouser, J.G.; Abe, T.; Loenneke, J.P. Mechanisms of blood flow restriction: The New Testament. Tech. Orthop. 2018, 33, 72–79. [Google Scholar] [CrossRef]
- Slysz, J.; Stultz, J.; Burr, J.F. The efficacy of blood flow restricted exercise: A systematic review & meta-analysis. J. Sci. Med. Sport 2016, 19, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Pearson, S.J.; Hussain, S.R. A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy. Sports Med. 2015, 45, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Bird, S.P.; Tarpenning, K.M.; Marino, F.E. Designing resistance training programmes to enhance muscular fitness: A review of the acute programme variables. Sports Med. 2005, 35, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-K.; Chu, I.-H.; Chen, F.-T.; Wang, C.-C. Dose-response effect of acute resistance exercise on tower of London in middle-aged adults. J. Sport Exerc. Psychol. 2011, 33, 866–883. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-K.; Etnier, J.L. Exploring the dose-response relationship between resistance exercise intensity and cognitive function. J. Sport Exerc. Psychol. 2009, 31, 640–656. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Blood flow restricted exercise for athletes: A review of available evidence. J. Sci. Med. Sport 2015. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Exercise with blood flow restriction: An updated evidence-based approach for enhanced muscular development. Sports Med. 2015, 45, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.R.; Slattery, K.M.; Sculley, D.V.; Dascombe, B.J. Hypoxia and resistance exercise: A comparison of localized and systemic methods. Sports Med. 2014, 44, 1037–1054. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Campo, D.J.; Scott, B.R.; Alcaraz, P.E.; Rubio-Arias, J.A. The efficacy of resistance training in hypoxia to enhance strength and muscle growth: A systematic review and meta-analysis. Euro. J. Sport Sci 2018, 18, 92–103. [Google Scholar] [CrossRef] [PubMed]
- de Castro, F.M.P.; Aquino, R.; Berti, J.A.; Gonçalves, L.G.C.; Puggina, E.F. Strength training with vascular occlusion: A review of possible adaptive mechanisms. Hum. Mov. 2017, 18, 1974. [Google Scholar] [CrossRef]
- Kawada, S. What phenomena do occur in blood flow-restricted muscle? Int. J. KAATSU Train. Res. 2005, 1, 37–44. [Google Scholar] [CrossRef]
- Manini, T.M.; Clark, B.C. Blood flow restricted exercise and skeletal muscle health. Exerc. Sport Sci. Rev. 2009, 37, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, K.; Hamed, I. Moderate Blood Flow Restriction Training. MOJSM 2017, 1. [Google Scholar] [CrossRef]
- Sato, Y. The history and future of KAATSU Training. Int. J. KAATSU Train. Res. 2005, 1, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Lopata, V.A.; Serebrovskaya, T.V. Hypoxicators: Review of the operating principles and constructions. In Intermittent Hypoxia and Human Diseases; Springer: London, UK, 2012; pp. 291–302. [Google Scholar]
- Nakajima, T.; Kurano, M.; Iida, H.; Takano, H.; Oounuma, H.; Morita, T.; Meguro, K.; Sato, Y.; Nagata, T. Use and safety of KAATSU training: Results of a national survey. Int. J. KAATSU Train. Res. 2006, 2, 5–13. [Google Scholar] [CrossRef]
- Nakajima, T.; Morita, T.; Sato, Y. Key considerations when conducting KAATSU training. Int. J. KAATSU Train. Res. 2011, 7, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Navarrete-Opazo, A.; Mitchell, G.S. Therapeutic potential of intermittent hypoxia: A matter of dose. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2014, 307, R1181–R1197. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Meguro, M.; Sato, Y.; Nakajima, T. Use and safety of KAATSU training: Results of a national survey in 2016. Int. J. KAATSU Train. Res. 2017, 13, 1–9. [Google Scholar] [CrossRef]
- Abe, T.; Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Thiebaud, R.S.; Bemben, M.G. Exercise intensity and muscle hypertrophy in blood flow-restricted limbs and non-restricted muscles: A brief review. Clin. Physiol. Funct. Imaging 2012, 32, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Madarame, H.; Neya, M.; Ochi, E.; Nakazato, K.; Sato, Y.; Ishii, N. Cross-transfer effects of resistance training with blood flow restriction. Med. Sci. Sports Exerc. 2008, 40, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Manukhina, E.B.; Downey, H.F.; Shi, X.; Mallet, R.T. Intermittent hypoxia training protects cerebrovascular function in Alzheimer’s disease. Exp. Biol. Med. 2016, 241, 1351–1363. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.; Hogan, A.M.; Bucks, R.S.; Baya, A.; Virues-Ortega, J.; Holloway, J.W.; Rose-Zerilli, M.; Palmer, L.J.; Webster, R.J.; Kirkham, F.J.; et al. Neurophysiological evidence for cognitive and brain functional adaptation in adolescents living at high altitude. Clin. Neurophysiol. 2011, 122, 1726–1734. [Google Scholar] [CrossRef] [PubMed]
- Schega, L.; Peter, B.; Törpel, A.; Mutschler, H.; Isermann, B.; Hamacher, D. Effects of intermittent hypoxia on cognitive performance and quality of life in elderly adults: A pilot study. Gerontology 2013, 59, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Schega, L.; Peter, B.; Brigadski, T.; Lessmann, V.; Isermann, B.; Hamacher, D.; Torpel, A. Effect of intermittent normobaric hypoxia on aerobic capacity and cognitive function in older people. J. Sci. Med. Sport 2016. [Google Scholar] [CrossRef] [PubMed]
- Sardeli, A.V.; Ferreira, M.L.V.; Santos, L.d.C.; Rodrigues, M.d.S.; Damasceno, A.; Cavaglieri, C.R.; Chacon-Mikahil, M.P.T. Low-load resistance exercise improves cognitive function in older adults. Rev. Bras. Med. Esporte. 2018, 24, 125–129. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Pujol, T.J. The use of occlusion training to produce muscle hypertrophy. Strength Cond. J. 2009, 31, 77–84. [Google Scholar] [CrossRef]
- Takano, H.; Morita, T.; Iida, H.; Asada, K.-I.; Kato, M.; Uno, K.; Hirose, K.; Matsumoto, A.; Takenaka, K.; Hirata, Y.; et al. Hemodynamic and hormonal responses to a short-term low-intensity resistance exercise with the reduction of muscle blood flow. Eur. J. Appl. Physiol. 2005, 95, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Manini, T.M.; Yarrow, J.F.; Buford, T.W.; Clark, B.C.; Conover, C.F.; Borst, S.E. Growth hormone responses to acute resistance exercise with vascular restriction in young and old men. Growth Horm. IGF Res. 2012, 22, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, S.D.; Leggate, M.; Nimmo, M.A.; Ferguson, R.A. Circulating hormone and cytokine response to low-load resistance training with blood flow restriction in older men. Eur. J. Appl. Physiol. 2013, 113, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Takarada, Y.; Nakamura, Y.; Aruga, S.; Onda, T.; Miyazaki, S.; Ishii, N. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. Eur. J. Appl. Physiol. 2000, 88, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Takano, H.; Morita, T.; Iida, H.; Kato, M.; Uno, K.; Hirose, K.; Matsumoto, A.; Takenaka, K.; Hirata, Y.; Furuichi, T.; et al. Effects of low-intensity “KAATSU” resistance exercise on hemodynamic and growth hormone responses. Int. J. KAATSU Train. Res. 2005, 1, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, R.A.; Hunt, J.E.A.; Lewis, M.P.; Martin, N.R.W.; Player, D.J.; Stangier, C.; Taylor, C.W.; Turner, M.C. The acute angiogenic signalling response to low-load resistance exercise with blood flow restriction. Eur. J. Sport Sci. 2018, 18, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Larkin, K.A.; Macneil, R.G.; Dirain, M.; Sandesara, B.; Manini, T.M.; Buford, T.W. Blood flow restriction enhances post-resistance exercise angiogenic gene expression. Med. Sci. Sports Exerc. 2012, 44, 2077–2083. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Yasuda, T.; Midorikawa, T.; Sato, Y.; Kearns, C.F.; Inoue, K.; Koizumi, K.; Ishii, N. Skeletal muscle size and circulating IGF-1 are increased after two weeks of twice daily “KAATSU” resistance training. Int. J. KAATSU Train. Res. 2005, 1, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Nyberg, F.; Hallberg, M. Growth hormone and cognitive function. Nat. Rev. Endocrinol. 2013, 9, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, P.S.; Aleman, A.; de Vries, W.R.; Deijen, J.B.; van der Veen, E.A.; de Haan, E.H.; Koppeschaar, H.P. Growth hormone, insulin-like growth factor I and cognitive function in adults. Growth Horm. IGF Res. 2000, 10, S69–S73. [Google Scholar] [CrossRef]
- Ari, Z.; Kutlu, N.; Uyanik, B.S.; Taneli, F.; Buyukyazi, G.; Tavli, T. Serum testosterone, growth hormone, and insulin-like growth factor-1 levels, mental reaction time, and maximal aerobic exercise in sedentary and long-term physically trained elderly males. Int. J. Neurosci. 2004, 114, 623–637. [Google Scholar] [CrossRef] [PubMed]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.-A. Exercise builds brain health: Key roles of growth factor cascades and inflammation. Trends Neurosci. 2007, 30, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Lucas, S.J.E.; Cotter, J.D.; Brassard, P.; Bailey, D.M. High-intensity interval exercise and cerebrovascular health: Curiosity, cause, and consequence. J. Cereb. Blood Flow Metab. 2015, 35, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Hogan, D.B.; Eskes, G.A.; Longman, R.S.; Poulin, M.J. Cerebrovascular reserve: The link between fitness and cognitive function? Exerc. Sport Sci. Rev. 2012, 40, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Basso, J.C.; Suzuki, W.A. The effects of acute exercise on mood, cognition, neurophysiology, and neurochemical pathways: A review. BPL 2017, 2, 127–152. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.H.; Alitalo, K. Molecular regulation of angiogenesis and lymphangiogenesis. Nat. Rev. Mol. Cell Biol. 2007, 8, 464–478. [Google Scholar] [CrossRef] [PubMed]
- Eichmann, A.; Simons, M. VEGF signaling inside vascular endothelial cells and beyond. Curr. Opin. Cell Biol. 2012, 24, 188–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, L.; Jia, J.; Liu, R. Decreased serum levels of the angiogenic factors VEGF and TGF-β1 in Alzheimer’s disease and amnestic mild cognitive impairment. Neurosci. Lett. 2013, 550, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Hohman, T.J.; Bell, S.P.; Jefferson, A.L. The role of vascular endothelial growth factor in neurodegeneration and cognitive decline: Exploring interactions with biomarkers of Alzheimer disease. JAMA Neurol. 2015, 72, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Gentil, P.; Oliveira, E.; Bottaro, M. Time under Tension and Blood Lactate Response during Four Different Resistance Training Methods. J. Physiol. Anthropol. 2006, 25, 339–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, S.; Abe, T.; Drummond, M.J.; Cadenas, J.G.; Dreyer, H.C.; Sato, Y.; Volpi, E.; Rasmussen, B.B. Blood flow restriction during low-intensity resistance exercise increases S6K1 phosphorylation and muscle protein synthesis. J. Appl. Physiol. 2007, 103, 903–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reeves, G.V.; Kraemer, R.R.; Hollander, D.B.; Clavier, J.; Thomas, C.; Francois, M.; Castracane, V.D. Comparison of hormone responses following light resistance exercise with partial vascular occlusion and moderately difficult resistance exercise without occlusion. J. Appl. Physiol. 2006, 101, 1616–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuda, T.; Abe, T.; Brechue, W.F.; Iida, H.; Takano, H.; Meguro, K.; Kurano, M.; Fujita, S.; Nakajima, T. Venous blood gas and metabolite response to low-intensity muscle contractions with external limb compression. Metabolism 2010, 59, 1510–1519. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.M.; Lowery, R.P.; Joy, J.M.; Loenneke, J.P.; Naimo, M.A. Practical blood flow restriction training increases acute determinants of hypertrophy without increasing indices of muscle damage. J. Strength Cond. Res. 2013, 27, 3068–3075. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Balapur, A.; Thrower, A.D.; Barnes, J.; Pujol, T.J. Blood flow restriction reduces time to muscular failure. Eur. J. Sport Sci. 2012, 12, 238–243. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Wilson, J.M.; Balapur, A.; Thrower, A.D.; Barnes, J.T.; Pujol, T.J. Time under tension decreased with blood flow-restricted exercise. Clin. Physiol. Funct. Imaging 2012, 32, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.W.; Koh, A.C.H.; Koh, S.X.T.; Liu, G.J.X.; Nio, A.Q.X.; Fan, P.W.P. Neck cooling and cognitive performance following exercise-induced hyperthermia. Eur. J. Appl. Physiol. 2014, 114, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, H.; Suga, T.; Takenaka, S.; Tanaka, D.; Takeuchi, T.; Hamaoka, T.; Isaka, T.; Ogoh, S.; Hashimoto, T. Repeated high-intensity interval exercise shortens the positive effect on executive function during post-exercise recovery in healthy young males. Physiol. Behav. 2016, 160, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Tsukamoto, H.; Takenaka, S.; Olesen, N.D.; Petersen, L.G.; Sørensen, H.; Nielsen, H.B.; Secher, N.H.; Ogoh, S. Maintained exercise-enhanced brain executive function related to cerebral lactate metabolism in men. FASEB J. 2017. [Google Scholar] [CrossRef] [PubMed]
- Riske, L.; Thomas, R.K.; Baker, G.B.; Dursun, S.M. Lactate in the brain: An update on its relevance to brain energy, neurons, glia and panic disorder. Ther. Adv. Psychopharmacol. 2017, 7, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Taher, M.; Leen, W.G.; Wevers, R.A.; Willemsen, M.A. Lactate and its many faces. Eur. J. Paediatr. Neurol. 2016, 20, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Van Hall, G.; Stromstad, M.; Rasmussen, P.; Jans, O.; Zaar, M.; Gam, C.; Quistorff, B.; Secher, N.H.; Nielsen, H.B. Blood lactate is an important energy source for the human brain. J. Cereb. Blood Flow Metab. 2009, 29, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Brooks, G.A. The Science and Translation of Lactate Shuttle Theory. Cell Metab. 2018, 27, 757–785. [Google Scholar] [CrossRef] [PubMed]
- Quistorff, B.; Secher, N.H.; van Lieshout, J.J. Lactate fuels the human brain during exercise. FASEB J. 2008, 22, 3443–3449. [Google Scholar] [CrossRef] [PubMed]
- Ferris, L.T.; Williams, J.S.; Shen, C.-L. The effect of acute exercise on serum brain-derived neurotrophic factor levels and cognitive function. Med. Sci. Sports Exerc. 2007, 39, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Schiffer, T.; Schulte, S.; Sperlich, B.; Achtzehn, S.; Fricke, H.; Struder, H.K. Lactate infusion at rest increases BDNF blood concentration in humans. Neurosci. Lett. 2011, 488, 234–237. [Google Scholar] [CrossRef] [PubMed]
- Borror, A. Brain-derived neurotrophic factor mediates cognitive improvements following acute exercise. Med. Hypotheses 2017, 106, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Brothers, R.M.; Castelli, D.M.; Glowacki, E.M.; Chen, Y.T.; Salinas, M.M.; Kim, J.; Jung, Y.; Calvert, H. Acute high-intensity exercise-induced cognitive enhancement and brain-derived neurotrophic factor in young, healthy adults. Neurosci. Lett. 2016, 630, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. Hypoxia-inducible factor 1: Master regulator of O2 homeostasis. Curr. Opin. Genet. Dev. 1998, 8, 588–594. [Google Scholar] [CrossRef]
- Schofield, C.J.; Ratcliffe, P.J. Oxygen sensing by HIF hydroxylases. Nat. Rev. Mol. Cell Biol. 2004, 5, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Laurentino, G.; Aoki, M.; Fernandes, R.; Soares, A.; Ugrinowitsch, C.; Hoschel, H.; Tricoli, V. Low-load resistance exercise with blood flow restriction changes hypoxia-induced genes expression. FASEB J. 2018, 32. [Google Scholar] [CrossRef]
- Correia, S.C.; Moreira, P.I. Hypoxia-inducible factor 1: A new hope to counteract neurodegeneration? J. Neurochem. 2010, 112, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, N.; Gerber, H.-P.; LeCouter, J. The biology of VEGF and its receptors. Nat. Med. 2003, 9, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Slomiany, M.G.; Rosenzweig, S.A. Hypoxia-inducible factor-1-dependent and -independent regulation of insulin-like growth factor-1-stimulated vascular endothelial growth factor secretion. J. Pharmacol. Exp. Ther. 2006, 318, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Brandner, C.R.; Warmington, S.A.; Kidgell, D.J. Corticomotor Excitability is Increased Following an Acute Bout of Blood Flow Restriction Resistance Exercise. Front. Hum. Neurosci. 2015, 9, 652. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Fukuda, T.; Kikuchi, H.; Ikeda, K.; Yumoto, M.; Sato, Y. Effects of blood flow restriction on cerebral blood flow during a single arm-curl resistance exercise. Int. J. KAATSU Train. Res. 2010, 6, 9–12. [Google Scholar] [CrossRef] [Green Version]
- Ganesan, G.; Cotter, J.A.; Reuland, W.; Cerussi, A.E.; Tromberg, B.J.; Galassetti, P. Effect of blood flow restriction on tissue oxygenation during knee extension. Med. Sci. Sports Exerc. 2015, 47, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Obrig, H.; Villringer, A. Beyond the visible—Imaging the human brain with light. J. Cereb. Blood Flow Metab. 2003, 23, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Lindauer, U.; Dirnagl, U.; Fuchtemeier, M.; Bottiger, C.; Offenhauser, N.; Leithner, C.; Royl, G. Pathophysiological interference with neurovascular coupling—When imaging based on hemoglobin might go blind. Front. Neuroenergetics 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Scholkmann, F.; Wolf, M. Measuring brain activity using functional near infrared spectroscopy: A short review. Spectrosc. Eur. 2012, 24, 6–10. [Google Scholar]
- Aslin, R.N.; Shukla, M.; Emberson, L.L. Hemodynamic correlates of cognition in human infants. Annu. Rev. Psychol. 2015, 66, 349–379. [Google Scholar] [CrossRef] [PubMed]
- Kirilina, E.; Jelzow, A.; Heine, A.; Niessing, M.; Wabnitz, H.; Brühl, R.; Ittermann, B.; Jacobs, A.M.; Tachtsidis, I. The physiological origin of task-evoked systemic artefacts in functional near infrared spectroscopy. NeuroImage 2012, 61, 70–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dravida, S.; Noah, J.A.; Zhang, X.; Hirsch, J. Comparison of oxyhemoglobin and deoxyhemoglobin signal reliability with and without global mean removal for digit manipulation motor tasks. Neurophotonics 2018, 5, 11006. [Google Scholar] [CrossRef] [PubMed]
- Obrig, H.; Neufang, M.; Wenzel, R.; Kohl, M.; Steinbrink, J.; Einhäupl, K.; Villringer, A. Spontaneous low frequency oscillations of cerebral hemodynamics and metabolism in human adults. NeuroImage 2000, 12, 623–639. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Shivakumar, V.; Chhabra, H.; Bose, A.; Venkatasubramanian, G.; Gangadhar, B.N. Functional near infra-red spectroscopy (fNIRS) in schizophrenia: A review. Asian J. Psychiatr. 2017, 27, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Haeussinger, F.B.; Dresler, T.; Heinzel, S.; Schecklmann, M.; Fallgatter, A.J.; Ehlis, A.-C. Reconstructing functional near-infrared spectroscopy (fNIRS) signals impaired by extra-cranial confounds: An easy-to-use filter method. NeuroImage 2014, 95, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Heinzel, S.; Haeussinger, F.B.; Hahn, T.; Ehlis, A.-C.; Plichta, M.M.; Fallgatter, A.J. Variability of (functional) hemodynamics as measured with simultaneous fNIRS and fMRI during intertemporal choice. NeuroImage 2013, 71, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Byun, K.; Hyodo, K.; Suwabe, K.; Ochi, G.; Sakairi, Y.; Kato, M.; Dan, I.; Soya, H. Positive effect of acute mild exercise on executive function via arousal-related prefrontal activations: An fNIRS study. NeuroImage 2014, 98, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Hyodo, K.; Dan, I.; Suwabe, K.; Kyutoku, Y.; Yamada, Y.; Akahori, M.; Byun, K.; Kato, M.; Soya, H. Acute moderate exercise enhances compensatory brain activation in older adults. Neurobiol. Aging 2012, 33, 2621–2632. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, Y.; Sato, D.; Yamashiro, K.; Tsubaki, A.; Yamaguchi, Y.; Takehara, N.; Maruyama, A. Inter-individual differences in exercise-induced spatial working memory improvement: A near-infrared spectroscopy study. Adv. Exp. Med. Biol. 2017, 977, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Barha, C.K.; Liu-Ambrose, T. Exercise and the aging brain: Considerations for sex differences. BPL 2018, 3, 1–11. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Frith, E. The role of sex in memory function: Considerations and recommendations in the context of exercise. J. Clin. Med. 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.; Kiely, J.; Suraci, B.; Collins, D.; de Lorenzo, D.; Pickering, C.; Grimaldi, K. A genetic-based algorithm for personalized resistance-training. Biol. Sport 2016, 33, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Ratamess, N.; Alvar, B.A.; Evetoch, T.K.; Housh, T.J.; Kibler, W.B.; Kraemer, W.J.; Triplett, N.T. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- Toigo, M.; Boutellier, U. New fundamental resistance exercise determinants of molecular and cellular muscle adaptations. Eur. J. Appl. Physiol. 2006, 97, 643–663. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Jeffries, O.; Waldron, M.; Rosenblatt, B.; Gissane, C.; Paton, B.; Patterson, S.D. Influence and reliability of lower-limb arterial occlusion pressure at different body positions. PeerJ 2018, 6, e4697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Thiebaud, R.S.; Mattocks, K.T.; Abe, T.; Bemben, M.G. Blood flow restriction pressure recommendations: A tale of two cuffs. Front. Physiol. 2013, 4, 249. [Google Scholar] [CrossRef] [PubMed]
- Sieljacks, P.; Knudsen, L.; Wernbom, M.; Vissing, K. Body position influences arterial occlusion pressure: Implications for the standardization of pressure during blood flow restricted exercise. Eur. J. Appl. Physiol. 2018, 118, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Brown, H.; Binnie, M.J.; Dawson, B.; Bullock, N.; Scott, B.R.; Peeling, P. Factors affecting occlusion pressure and ischemic preconditioning. Eur. J. Sport Sci. 2018, 18, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Sherk, V.D.; Thiebaud, R.S.; Abe, T.; Bemben, D.A.; Bemben, M.G. Effects of cuff width on arterial occlusion: Implications for blood flow restricted exercise. Eur. J. Appl. Physiol. 2012, 112, 2903–2912. [Google Scholar] [CrossRef] [PubMed]
- Mouser, J.G.; Dankel, S.J.; Jessee, M.B.; Mattocks, K.T.; Buckner, S.L.; Counts, B.R.; Loenneke, J.P. A tale of three cuffs: The hemodynamics of blood flow restriction. Eur. J. Appl. Physiol. 2017, 117, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Vanwye, W.R.; Weatherholt, A.M.; Mikesky, A.E. Blood flow restriction training: Implementation into clinical practice. Int. J. Exerc. Sci. 2017, 10, 649–654. [Google Scholar] [PubMed]
- Thurston, B.; Burr, J.F. Blood flow restricted training: Applications, mechanisms, and future directions. Health Fitness J. Can. 2017, 10, 13–16. [Google Scholar]
- Jessee, M.B.; Buckner, S.L.; Dankel, S.J.; Counts, B.R.; Abe, T.; Loenneke, J.P. The influence of cuff width, sex, and race on arterial occlusion: Implications for blood flow restriction research. Sports Med. 2016, 46, 913–921. [Google Scholar] [CrossRef] [PubMed]
- Laurentino, G.C.; Loenneke, J.P.; Teixeira, E.L.; Nakajima, E.; Iared, W.; Tricoli, V. The effect of cuff width on muscle adaptations after blood flow restriction training. Med. Sci. Sports Exerc. 2016, 48, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Mittal, P.; Shenoy, S.; Sandhu, J.S. Effect of different cuff widths on the motor nerve conduction of the median nerve: An experimental study. J. Orthop. Surg. Res. 2008, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Mouser, J.G.; Dankel, S.J.; Mattocks, K.T.; Jessee, M.B.; Buckner, S.L.; Abe, T.; Loenneke, J.P. Blood flow restriction and cuff width: Effect on blood flow in the legs. Clin. Physiol. Funct. Imaging 2018. [Google Scholar] [CrossRef] [PubMed]
- Mattocks, K.T.; Jessee, M.B.; Mouser, J.G.; Dankel, S.J.; Buckner, S.L.; Bell, Z.W.; Owens, J.G.; Abe, T.; Loenneke, J.P. The application of blood flow restriction: Lessons from the laboratory. Curr. Sports Med. Rep. 2018, 17, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Buckner, S.L.; Dankel, S.J.; Counts, B.R.; Jessee, M.B.; Mouser, J.G.; Mattocks, K.T.; Laurentino, G.C.; Abe, T.; Loenneke, J.P. Influence of cuff material on blood flow restriction stimulus in the upper body. J. Physiol. Sci. 2017, 67, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Thiebaud, R.S.; Fahs, C.A.; Rossow, L.M.; Abe, T.; Bemben, M.G. Effect of cuff type on arterial occlusion. Clin. Physiol. Funct. Imaging 2013, 33, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Allen, K.M.; Mouser, J.G.; Thiebaud, R.S.; Kim, D.; Abe, T.; Bemben, M.G. Blood flow restriction in the upper and lower limbs is predicted by limb circumference and systolic blood pressure. Eur. J. Appl. Physiol. 2015, 115, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Brandner, C.R.; Kidgell, D.J.; Warmington, S.A. Unilateral bicep curl hemodynamics: Low-pressure continuous vs high-pressure intermittent blood flow restriction. Scand. J. Med. Sci. Sports 2015, 25, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Counts, B.R.; Dankel, S.J.; Barnett, B.E.; Kim, D.; Mouser, J.G.; Allen, K.M.; Thiebaud, R.S.; Abe, T.; Bemben, M.G.; Loenneke, J.P. Influence of relative blood flow restriction pressure on muscle activation and muscle adaptation. Muscle Nerve 2016, 53, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Dankel, S.J.; Jessee, M.B.; Buckner, S.L.; Mouser, J.G.; Mattocks, K.T.; Loenneke, J.P. Are higher blood flow restriction pressures more beneficial when lower loads are used? Psychophysiol. Int. 2017, 104, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Fatela, P.; Reis, J.F.; Mendonca, G.V.; Avela, J.; Mil-Homens, P. Acute effects of exercise under different levels of blood-flow restriction on muscle activation and fatigue. Eur. J. Appl. Physiol. 2016, 116, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Jessee, M.B.; Buckner, S.L.; Mouser, J.G.; Mattocks, K.T.; Loenneke, J.P. Letter to the editor: Applying the blood flow restriction pressure: The elephant in the room. Am. J. Physiol. 2016, 310, H132–H133. [Google Scholar] [CrossRef] [PubMed]
- Karabulut, M.; Leal, J.A., Jr.; Garcia, S.D.; Cavazos, C.; Bemben, M. Tissue oxygenation, strength and lactate response to different blood flow restrictive pressures. Clin. Physiol. Funct. Imaging 2014, 34, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Kim, D.; Mouser, J.G.; Allen, K.M.; Thiebaud, R.S.; Abe, T.; Bemben, M.G. Are there perceptual differences to varying levels of blood flow restriction? Physiol. Behav. 2016, 157, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Barnett, B.E.; Dankel, S.J.; Counts, B.R.; Nooe, A.L.; Abe, T.; Loenneke, J.P. Blood flow occlusion pressure at rest and immediately after a bout of low load exercise. Clin. Physiol. Funct. Imaging 2016, 36, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Kim, D.; Fahs, C.A.; Thiebaud, R.S.; Abe, T.; Larson, R.D.; Bemben, D.A.; Bemben, M.G. Effects of exercise with and without different degrees of blood flow restriction on torque and muscle activation. Muscle Nerve 2015, 51, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Kim, D.; Fahs, C.A.; Thiebaud, R.S.; Abe, T.; Larson, R.D.; Bemben, D.A.; Bemben, M.G. The effects of resistance exercise with and without different degrees of blood-flow restriction on perceptual responses. J. Sports Sci. 2015, 33, 1472–1479. [Google Scholar] [CrossRef] [PubMed]
- Fitschen, P.J.; Kistler, B.M.; Jeong, J.H.; Chung, H.R.; Wu, P.T.; Walsh, M.J.; Wilund, K.R. Perceptual effects and efficacy of intermittent or continuous blood flow restriction resistance training. Clin. Physiol. Funct. Imaging 2014, 34, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Neto, G.R.; Novaes, J.S.; Salerno, V.P.; Gonçalves, M.M.; Piazera, B.K.L.; Rodrigues-Rodrigues, T.; Cirilo-Sousa, M.S. Acute effects of resistance exercise with continuous and intermittent blood flow restriction on hemodynamic measurements and perceived exertion. Percept. Mot. Skills 2016. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Loenneke, J.P.; Ogasawara, R.; Abe, T. Influence of continuous or intermittent blood flow restriction on muscle activation during low-intensity multiple sets of resistance exercise. Acta Physiol. Hung. 2013, 100, 419–426. [Google Scholar] [CrossRef]
- Hughes, L.; Rosenblatt, B.; Gissane, C.; Paton, B.; Patterson, S.D. Interface pressure, perceptual, and mean arterial pressure responses to different blood flow restriction systems. Scand. J. Med. Sci. Sports 2018, 28, 1757–1765. [Google Scholar] [CrossRef] [PubMed]
- McEwen, J.A.; Owens, J.G.; Jeyasurya, J. Why is it crucial to use personalized occlusion pressures in blood flow restriction (BFR) rehabilitation? J. Med. Biol. Eng. 2018, 99, 235. [Google Scholar] [CrossRef]
- Day, B. Personalized Blood Flow Restriction Therapy: How, When and Where Can It Accelerate Rehabilitation After Surgery? Arthroscopy 2018, 34, 2511–2513. [Google Scholar] [CrossRef] [PubMed]
- Lixandrão, M.E.; Ugrinowitsch, C.; Laurentino, G.; Libardi, C.A.; Aihara, A.Y.; Cardoso, F.N.; Tricoli, V.; Roschel, H. Effects of exercise intensity and occlusion pressure after 12 weeks of resistance training with blood-flow restriction. Eur. J. Appl. Physiol. 2015, 115, 2471–2480. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Thiebaud, R.S.; Abe, T.; Bemben, M.G. Blood flow restriction pressure recommendations: The hormesis hypothesis. Medical Hypotheses 2014, 82, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.D.; Hughes, L.; Head, P.; Warmington, S.; Brandner, C. Blood flow restriction training: A novel approach to augment clinical rehabilitation: How to do it. Br. J. Sports Med. 2017, 51, 1648–1649. [Google Scholar] [CrossRef] [PubMed]
- Pope, Z.K.; Willardson, J.M.; Schoenfeld, B.J. Exercise and blood flow restriction. J. Strength Cond. Res. 2013, 27, 2914–2926. [Google Scholar] [CrossRef] [PubMed]
- Fahs, C.A.; Loenneke, J.P.; Rossow, L.M.; Tiebaud, R.S.; Bemben, M.G. Methodological considerations for blood flow restricted resistance exercise. J. Trainol. 2012, 1, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Loenneke, J.P.; Wilson, J.M.; Marin, P.J.; Zourdos, M.C.; Bemben, M.G. Low intensity blood flow restriction training: A meta-analysis. Eur. J. Appl. Physiol. 2012, 112, 1849–1859. [Google Scholar] [CrossRef] [PubMed]
- Radaelli, R.; Fleck, S.J.; Leite, T.; Leite, R.D.; Pinto, R.S.; Fernandes, L.; Simão, R. Dose-response of 1, 3, and 5 sets of resistance exercise on strength, local muscular endurance, and hypertrophy. J. Strength Cond. Res. 2015, 29, 1349–1358. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Wilson, J.M.; Wilson, G.J.; Pujol, T.J.; Bemben, M.G. Potential safety issues with blood flow restriction training. Scand. J. Med. Sci. Sports 2011, 21, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.D.; Brandner, C.R. The role of blood flow restriction training for applied practitioners: A questionnaire-based survey. J. Sports Sci. 2018, 36, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Fahs, C.A.; Abe, T.; Rossow, L.M.; Ozaki, H.; Pujol, T.J.; Bemben, M.G. Hypertension risk: Exercise is medicine for most but not all. Clin. Physiol. Funct. Imaging 2014, 34, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Kacin, A.; Rosenblatt, B.; Grapar Zagri, T.; Biswas, A. Safety considerations with blood flow restricted resistance training. Ann. Kinesiol. 2015, 6, 3–26. [Google Scholar]
- Lövdén, M.; Wenger, E.; Mårtensson, J.; Lindenberger, U.; Bäckman, L. Structural brain plasticity in adult learning and development. Neurosci. Biobehav. Rev. 2013, 37, 2296–2310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooks, C.R.; Thom, N.J.; McCully, K.K.; Dishman, R.K. Effects of incremental exercise on cerebral oxygenation measured by near-infrared spectroscopy: A systematic review. Prog. Neurobiol. 2010, 92, 134–150. [Google Scholar] [CrossRef] [PubMed]
- Kenville, R.; Maudrich, T.; Carius, D.; Ragert, P. Hemodynamic Response Alterations in Sensorimotor Areas as a Function of Barbell Load Levels during Squatting: An fNIRS Study. Front. Hum. Neurosci. 2017, 11, 268. [Google Scholar] [CrossRef] [PubMed]
- Park, J.L.; Fairweather, M.M.; Donaldson, D.I. Making the case for mobile cognition: EEG and sports performance. Neurosci. Biobehav. Rev. 2015, 52, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Tsujii, T.; Komatsu, K.; Sakatani, K. Acute effects of physical exercise on prefrontal cortex activity in older adults: A functional near-infrared spectroscopy study. Adv. Exp. Med. Boil. 2013, 765, 293–298. [Google Scholar] [CrossRef]
- Moriya, M.; Aoki, C.; Sakatani, K. Effects of Physical Exercise on Working Memory and Prefrontal Cortex Function in Post-Stroke Patients. Adv. Exp. Med. Biol. 2016, 923, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.-S.; Chang, Y.-K.; Hung, T.-M.; Fang, C.-L. The effects of acute resistance exercise on young and older males’ working memory. Psychol. Sport Exerc. 2016, 22, 286–293. [Google Scholar] [CrossRef]
- McMorris, T. Exercise–Cognition Interaction: State of the Art and Future Research; Elsevier: Amsterdam, The Netherlands, 2016; pp. 459–481. [Google Scholar]
- Svebak, S.; Murgatroyd, S. Metamotivational dominance: A multimethod validation of reversal theory constructs. J. Pers. Soc. Psychol. 1985, 48, 107–116. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, H.; Suga, T.; Takenaka, S.; Takeuchi, T.; Tanaka, D.; Hamaoka, T.; Hashimoto, T.; Isaka, T. An acute bout of localized resistance exercise can rapidly improve inhibitory control. PLoS ONE 2017, 12, e0184075. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, H.; Takenaka, S.; Suga, T.; Tanaka, D.; Takeuchi, T.; Hamaoka, T.; Isaka, T.; Hashimoto, T. Impact of exercise intensity and duration on post exercise executive function. Med. Sci. Sports Exerc. 2016. [Google Scholar] [CrossRef]
- Tsukamoto, H.; Suga, T.; Takenaka, S.; Tanaka, D.; Takeuchi, T.; Hamaoka, T.; Isaka, T.; Hashimoto, T. Greater impact of acute high-intensity interval exercise on post-exercise executive function compared to moderate-intensity continuous exercise. Physiol. Behav. 2016, 155, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Kovacevic, A.; Mavros, Y.; Heisz, J.J.; Fiatarone Singh, M.A. The effect of resistance exercise on sleep: A systematic review of randomized controlled trials. Sleep Med. Rev. 2018, 39, 52–68. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Iwamoto, K.; Kawano, N.; Noda, Y.; Ozaki, N.; Noda, A. Differential effects of physical activity and sleep duration on cognitive function in young adults. J. Sport Health Sci. 2017. [Google Scholar] [CrossRef]
- Hughes, L.; Paton, B.; Rosenblatt, B.; Gissane, C.; Patterson, S.D. Blood flow restriction training in clinical musculoskeletal rehabilitation: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- Dankel, S.J.; Jessee, M.B.; Abe, T.; Loenneke, J.P. The Effects of Blood Flow Restriction on Upper-Body Musculature Located Distal and Proximal to Applied Pressure. Sports Med. 2016, 46, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Lixandrão, M.E.; Ugrinowitsch, C.; Berton, R.; Vechin, F.C.; Conceição, M.S.; Damas, F.; Libardi, C.A.; Roschel, H. Magnitude of muscle strength and mass adaptations between high-load resistance training versus low-load resistance training associated with blood-flow restriction: A systematic review and meta-analysis. Sports Med. 2018, 48, 361–378. [Google Scholar] [CrossRef] [PubMed]
- Karabulut, M.; Abe, T.; Sato, Y.; Bemben, M.G. The effects of low-intensity resistance training with vascular restriction on leg muscle strength in older men. Eur. J. Appl. Physiol. 2010, 108, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Mavros, Y.; Gates, N.; Wilson, G.C.; Jain, N.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. Mediation of Cognitive Function Improvements by Strength Gains After Resistance Training in Older Adults with Mild Cognitive Impairment: Outcomes of the Study of Mental and Resistance Training. J. Am. Geriatr. Soc. 2017, 65, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Tumati, S.; Burger, H.; Martens, S.; van der Schouw, Y.T.; Aleman, A. Association between Cognition and Serum Insulin-Like Growth Factor-1 in Middle-Aged & Older Men: An 8 Year Follow-Up Study. PLoS ONE 2016, 11, e0154450. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Thiebaud, R.S.; Abe, T. Does blood flow restriction result in skeletal muscle damage? A critical review of available evidence. Scand. J. Med. Sci. Sports 2014, 24, e415–e422. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Beekley, M.D.; Hinata, S.; Koizumi, K.; Sato, Y. Day-to-day change in muscle strength and MRI-measured skeletal muscle size during 7 days KAATSU resistance training: A case study. Int. J. KAATSU Train. Res. 2005, 1, 71–76. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Exercise Variables | Recommendations for Resistance Training with BFR |
|---|---|
| (1.) load | 20 to 50% of 1RM |
| (2.) number of repetitions | 15 to 30 per set, 50 to 80 repetitions per exercise (e.g., 30–15–15–15 reps) |
| (3.) number of sets | 3 to 5 sets per exercise |
| (4.) inter-set rest periods | 30 to 60 s |
| (5.) inter-exercise rest periods | 5 min (without BFR) |
| (6.) number of exercises | n.a. |
| (7.) repetition velocity | 1 (to 2)–0–1 (to 2)–1 s |
| (8.) muscle action | dynamic muscle action, eccentric is more effective than concentric |
| (9.) exercise selection | single- and multi-joint exercise |
| (10.) exercise order | n.a., depending on the training goal |
| (11.) volitional muscle failure | until volitional fatigue/repetition failure/technical failure |
| (12.) range of motion | full range of motion |
| (13.) frequency | 2 to 3 sessions per week |
| (14.) density | n.a., depending on the performance level |
| (15.) duration | n.a., but according to the general physiological view, exercise variables or exercises should be changed after a mesocycle of 8 to 12 weeks |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Törpel, A.; Herold, F.; Hamacher, D.; Müller, N.G.; Schega, L. Strengthening the Brain—Is Resistance Training with Blood Flow Restriction an Effective Strategy for Cognitive Improvement? J. Clin. Med. 2018, 7, 337. https://doi.org/10.3390/jcm7100337
Törpel A, Herold F, Hamacher D, Müller NG, Schega L. Strengthening the Brain—Is Resistance Training with Blood Flow Restriction an Effective Strategy for Cognitive Improvement? Journal of Clinical Medicine. 2018; 7(10):337. https://doi.org/10.3390/jcm7100337
Chicago/Turabian StyleTörpel, Alexander, Fabian Herold, Dennis Hamacher, Notger G. Müller, and Lutz Schega. 2018. "Strengthening the Brain—Is Resistance Training with Blood Flow Restriction an Effective Strategy for Cognitive Improvement?" Journal of Clinical Medicine 7, no. 10: 337. https://doi.org/10.3390/jcm7100337