
Significantly Elevated CA 19-9 after COVID-19 Vaccination and Literature Review of Non-Cancerous Cases with CA 19-9 > 1000 U/mL
 , ,
, ,
Abstract
:1. Introduction
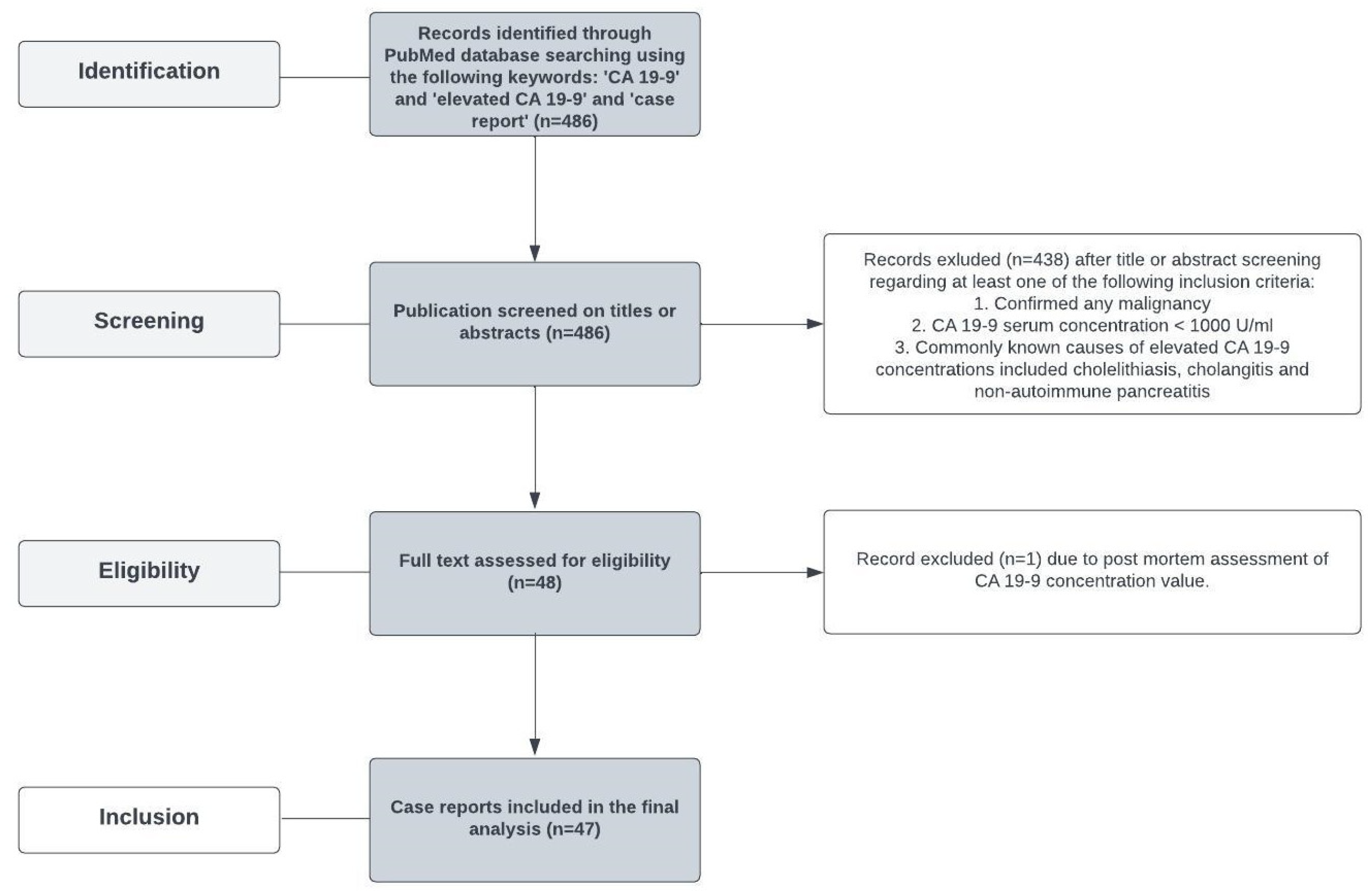
2. Materials and Methods
2.1. Data Extraction
2.2. Statistical Analysis
3. Case Report
4. Results
5. Discussion
6. Conclusions
7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scarà, S.; Bottoni, P.; Scatena, R. CA 19-9: Biochemical and Clinical Aspects. Adv. Exp. Med. Biol. 2015, 867, 247–260. [Google Scholar]
- Zhao, B.; Cheng, Q.; Cao, H.; Zhou, X.; Li, T.; Dong, L. Dynamic change of serum CA19–9 levels in benign and malignant patients with obstructive jaundice after biliary drainage and new correction formulas. BMC Cancer 2021, 21, 517. [Google Scholar] [CrossRef] [PubMed]
- Omyła-Staszewska, J. Opis przypadku pacjentki z zaawansowanym nowotworem neuroendokrynnym trzustki z przerzutami do wątroby leczonej oktreotydem LAR. Onkol. Prakt. Klin. Edu. 2015, 11, G24–G28. [Google Scholar]
- Ventrucci, M.; Pozzato, P.; Cipolla, A.; Uomo, G. Persistent elevation of serum CA 19-9 with no evidence of malignant disease. Dig. Liver Dis. 2009, 41, 357–363. [Google Scholar] [CrossRef]
- Okabayashi, K.; Motohiro, A.; Ueda, H.; Ondo, K.; Kawahara, K.; Shirakusa, T. Subcarinal Bronchogenic Cyst with High Carbohydrate Antigen 19-9 Production. Jpn. J. Thorac. Cardiovasc. Surg. 2002, 50, 46–48. [Google Scholar] [CrossRef]
- Wang, M.X.; Qiu, X.; Tian, C.; Li, J.; Lv, M. Retroperitoneal bronchogenic cyst resembling an adrenal tumor with high levels of serum carbohydrate antigen 19-9. Medicine 2017, 96, e7678. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Cai, Y.; Chen, R.; Du, S.; Chen, Y.; Shi, K. A case report and a short literature review of pulmonary sequestration showing elevated serum levels of carbohydrate antigen 19-9. J. Nippon. Med. Sch. 2015, 82, 211–215. [Google Scholar] [CrossRef]
- Liu, K.L.; Chen, J.S.; Cheng, T.Y. Pulmonary sequestration: An unusual cause of Elevated CA 19-9. Am. J. Gastroenterol. 2016, 111, 289. [Google Scholar] [CrossRef]
- Yango, J.; Pieters, T.; Coche, E.; Lambert, M. Élévation du CA 19.9 sérique et bronchectasies. Rev. Mal. Respir. 2008, 25, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Inokuma, T.; Minami, S.; Suga, K.; Kusano, Y.; Chiba, K.; Furukawa, M. Spontaneously ruptured giant splenic cyst with elevated serum levels of CA 19-9, CA 125 and carcinoembryonic antigen. Case Rep. Gastroenterol. 2010, 4, 191–197. [Google Scholar] [CrossRef]
- Imoto, Y.; Einama, T.; Fukumura, M.; Kouzu, K.; Nagata, H.; Matsunaga, A.; Hoshikawa, M.; Nishikawa, M.; Kimura, A.; Noro, T.; et al. Laparoscopic fenestration for a large ruptured splenic cyst combined with an elevated serum carbohydrate antigen 19-9 level: A case report. BMC Surg. 2019, 19, 58. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, A.; Nakamura, Y.; Suzuki, H.; Mizutani, S.; Chihara, N.; Matsunobu, T.; Maejima, K.; Miura, K.; Hanawa, H.; Nomura, S.; et al. Giant epidermoid cyst of the spleen with elevated CA 19-9 production managed laparoscopically: Report of a case. J. Nippon. Med. Sch. 2013, 80, 470–474. [Google Scholar] [CrossRef]
- Buda, N.; Wszołek, A.; Śledziński, M.; Żawrocki, A.; Sworczak, K. Epidermoid splenic cyst with elevated serum level of CA19-9. Korean J. Intern. Med. 2018, 33, 1032–1033. [Google Scholar] [CrossRef] [PubMed]
- Matsui, T.; Matsubayashi, H.; Sugiura, T.; Sasaki, K.; Ito, H.; Hotta, K.; Imai, K.; Tanaka, M.; Kakushima, N.; Ono, H. A Splenic Epithelial Cyst: Increased Size, Exacerbation of Symptoms, and Elevated Levels of Serum Carcinogenic Antigen 19-9 after 6-year Follow-up. Intern. Med. 2016, 55, 2629–2634. [Google Scholar] [CrossRef] [PubMed]
- Soudack, M.; Ben-Nun, A.; Toledano, C. Elevated carbohydrate antigen 19-9 in patients with true (epithelial) splenic cysts-Rare or undiscovered? Can. J. Gastroenterol. 2001, 15, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Sardi, A.; Ojeda, H.F.; King, D. Laparoscopic resection of a benign true cyst of the spleen with the harmonic scalpel producing high levels of CA 19-9 and carcinoembryonic antigen. Am. Surg. 1998, 64, 1149–1154. [Google Scholar] [PubMed]
- Filipovic, B.; Milinić, N.; Gacic, J.; Markovic, O.; Djokovic, A.; Filipovic, B. Benign hydronephrosis and elevated of serum levels of carbohydrate antigen CA 19-9: A case report. Am. J. Case Rep. 2016, 17, 395–397. [Google Scholar] [CrossRef]
- Meyer, A.; Kausch, I.; Krüger, S.; Fetscher, S.; Böhle, A.; Jocham, D. Elevation of CA 19-9 in giant hydronephrosis induced by a renal calculus. Urology 2004, 63, 381–382. [Google Scholar] [CrossRef]
- Shudo, R.; Saito, T.; Takahashi, K.; Horita, K.; Waku, K.; Honma, I.; Sato, T. Giant hydronephrosis due to a ureteral stone, and elevated serum levels of CA 19-9. Intern. Med. 1999, 38, 887–891. [Google Scholar] [CrossRef]
- Ito, S.; Nishikawa, K.; Goto, T.; Tsujita, M.; Takegaki, Y.; Kishimoto, T. A case of hydronephrosis caused by renal stones with elevated serum levels of CA-19-9 and CA-125. Hinyokika Kiyo 1994, 40, 885–888. [Google Scholar]
- Atabekoǧlu, C.; Bozaci, E.A.; Tezcan, S. Elevated carbohydrate antigen 19-9 in a dermoid cyst. Int. J. Gynaecol. Obstet. 2005, 91, 262–263. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, J.; Sarmento-Gonçalves, I.; Barros, J.M.; Felix, J.; Tiago-Silva, P. Mature cystic teratoma of ovary with abnormally high levels of Ca19-9: A case report. Rev. Bras. Ginecol. Obs. 2016, 38, 365–367. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.C.; Yen, R.F.; Chen, Y.K. Dermoid cyst with secretion of CA 19-9 detected by 18F-FDG PET/CT: A case report. Medicine 2020, 99, e18988. [Google Scholar] [CrossRef] [PubMed]
- Cho, A.; Kim, B.R.; Lim, S.H.; Park, C.M. Extreme elevation of CA 19-9 levels in mature cystic teratoma without any complications: A case report. Ann. Med. Surg. 2022, 78, 103803. [Google Scholar] [CrossRef] [PubMed]
- Pyeon, S.Y.; Park, J.Y.; Ki, K.D.; Lee, J.M. Abnormally high level of CA-19-9 in a benign ovarian cyst. Obstet. Gynecol. Sci. 2015, 58, 530–532. [Google Scholar] [CrossRef] [PubMed]
- Pandey, D.; Sharma, R.; Sharma, S.; Salhan, S. Unusually high serum levels of CA 19-9 in an ovarian tumour: Malignant or benign? J. Clin. Diagn. Res. 2017, 11, JC01–JC03. [Google Scholar] [CrossRef]
- Chew, K.T.; Zakaria, I.A.; Abu, M.A.; Ahmad, M.F.; Hing, E.Y.; Ghani, N.A.A. Elevated serum CA 19-9 with adnexal mass: Is it always an ovarian malignancy? Horm. Mol. Biol. Clin. Investig. 2018, 34, 20180011. [Google Scholar] [CrossRef]
- Park, B.J.; Kim, T.E.; Kim, Y.W. Massive peritoneal fluid and markedly elevated serum CA125 and CA19-9 levels associated with an ovarian endometrioma. J. Obstet. Gynaecol. Res. 2009, 35, 935–939. [Google Scholar] [CrossRef]
- Sato, H.; Borsari, R.; Yajima, E.K.; Ninomiya, T.; Saito, C.S.; Kumagai, C.A.K. Adenomyoma associated with high level of CA 125 and CA 19-9: Case report. Eur. J. Gynaecol. Oncol. 2011, 32, 455–456. [Google Scholar]
- Buyukbayrak, E.E.; OzyapI, A.G.; Karsidag, Y.K.; Pirimoglu, Z.M.; Unal, O.; Turan, C. Imperforate hymen: A new benign reason for highly elevated serum CA 19.9 and CA 125 levels. Arch. Gynecol. Obstet. 2008, 277, 475–477. [Google Scholar] [CrossRef]
- Moshref, L.H.; Mandili, R.A.; Almaghrabi, M.; Abdulwahab, R.A.; Alosaimy, R.A.; Miro, J. Elevation of CA 19-9 in mirizzi syndrome in the absence of malignancy: A case report. Am. J. Case Rep. 2021, 22, e931819-1. [Google Scholar] [CrossRef]
- Robertson, A.G.N.; Davidson, B.R. Mirizzi syndrome complicating an anomalous biliary tract: A novel cause of a hugely elevated CA19-9. Eur. J. Gastroenterol. Hepatol. 2007, 19, 167–169. [Google Scholar] [CrossRef]
- Shirai, Y.; Shiba, H.; Fujiwara, Y.; Eto, K.; Misawa, T.; Yanaga, K. Hepatic inflammatory pseudotumor with elevated serum CA19-9 level mimicking liver metastasis from rectal cancer: Report of a case. Int. Surg. 2013, 98, 324–329. [Google Scholar] [CrossRef]
- Ogawa, T.; Yokoi, H.; Kawarada, Y. A case of inflammatory pseudotumor of the liver causing elevated serum CA19-9 levels. Am. J. Gastroenterol. 1998, 93, 2551–2555. [Google Scholar] [CrossRef] [PubMed]
- Giannaris, M.; Dourakis, S.P.; Alexopoulou, A.; Archimandritis, A.J. Markedly elevated CA 19-9 in the pus and the serum of a patient with pyogenic liver abscess. J. Clin. Gastroenterol. 2006, 40, 657. [Google Scholar] [CrossRef] [PubMed]
- Vandemergel, X.; Vandergheynst, F.; Decaux, G. Very high elevation of CA19-9 level in a patient with steatosis. Acta Gastroenterol. Belg. 2005, 68, 380–381. [Google Scholar]
- Schoonbroodt, D.; Horsmans, Y.; Gigot, J.F.; Rahier, J.; Geubel, A.P. Biliary cystadenoma of the liver with elevated CA 19-9. Liver 1994, 14, 320–322. [Google Scholar] [CrossRef] [PubMed]
- De Marchi, G.; Paiella, S.; Luchini, C.; Capelli, P.; Bassi, C.; Frulloni, L. Very high serum levels of CA 19-9 in autoimmune pancreatitis: Report of four cases and brief review of literature. J. Dig. Dis. 2016, 17, 697–702. [Google Scholar] [CrossRef]
- Ong, S.L.; Garcea, G.; Puls, F.; Richards, C.; Mulcahy, K.; Grant, A.; Dennison, A.R.; Berry, D.P. IgG4-positive sclerosing cholangitis following autoimmune pancreatitis with deranged CA19.9. Int. J. Surg. Pathol. 2011, 19, 697–702. [Google Scholar] [CrossRef]
- Efeovbokhan, N.; Makol, A.; Cuison, R.V.; Minter, R.M.; Kotaru, V.P.; Conley, B.A.; Chandana, S.R. An unusual case of autoimmune pancreatitis presenting as pancreatic mass and obstructive jaundice: A case report and review of the literature. J. Med. Case Rep. 2011, 5, 253. [Google Scholar] [CrossRef]
- Kaur, M.; Dalal, V.; Bhatnagar, A.; Siraj, F. Pancreatic tuberculosis with markedly elevated CA 19-9 levels: A diagnostic pitfall. Oman Med. J. 2016, 31, 446–449. [Google Scholar] [CrossRef]
- Chou, J.W.; Chang, K.P.; Wu, Y.H. A Rare Cause of Elevated Serum CA19-9. Gastroenterology 2021, 160, 31–32. [Google Scholar] [CrossRef]
- El-Khoury, M.; Bohlok, A.; Sleiman, Y.A.; Loi, P.; Coppens, E.; Demetter, P.; El Nakadi, I. A rare presentation of small diaphragmatic epidermoid cyst with extremely elevated serum CA19-9 level. Ann. R. Coll. Surg. Engl. 2020, 102, e23–e25. [Google Scholar] [CrossRef]
- Ergül, B.; Doǧan, Z.; Sarikaya, M.; Filik, L. Rapid decline to normal levels of extraordinarily elevated CA 19-9 after Giardiasis. Clin. Res. Hepatol. Gastroenterol. 2013, 37, e97. [Google Scholar] [CrossRef]
- Hyman, J.; Wilczynski, S.P.; Schwarz, R.E. Extrahepatic bile duct stricture and elevated CA 19-9: Malignant or benign? South Med. J. 2003, 96, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Lemaire, V.; Jeannou, J.; Goupille, P.; Valat, J. La fibrose pulmonaire, une cause d’élévation du CA 19-9. Rev. Med. Intern. 1998, 19, 942–944. [Google Scholar] [CrossRef] [PubMed]
- de Meira-Júnior, J.D.; Costa, T.N.; Montagnini, A.L.; Nahas, S.C.; Jukemura, J. Elevated CA 19-9 in an asymptomatic patient: What does it mean? Arq. Bras. Cir. Dig. 2022, 35, e1687. [Google Scholar] [CrossRef]
- Noda, Y.; Tomita, H.; Ishihara, T.; Tsuboi, Y.; Kawai, N.; Kawaguchi, M.; Kaga, T.; Hyodo, F.; Hara, A.; Kambadakone, A.R.; et al. Prediction of overall survival in patients with pancreatic ductal adenocarcinoma: Histogram analysis of ADC value and correlation with pathological intratumoral necrosis. BMC Med. Imaging 2022, 22, 23. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Lee, K.T.; Lee, J.K.; Paik, S.W.; Rhee, J.C.; Choi, K.W. Clinical usefulness of carbohydrate antigen 19-9 as a screening test for pancreatic cancer in an asymptomatic population. Gastroenterol. Hepatol. 2004, 19, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Ferrone, C.R.; Finkelstein, D.M.; Thayer, S.P.; Muzikansky, A.; Fernandez-Del Castillo, C.; Warshaw, A.L. Perioperative CA19-9 levels can predict stage and survival in patients with resectable pancreatic adenocarcinoma. J. Clin. Oncol. 2006, 24, 2897–2902. [Google Scholar] [CrossRef] [PubMed]
- Parra-Robert, M.; Santos, V.M.; Canis, S.M.; Pla, X.; Fradera, J.M.A.; Porto, R.M. Relationship between CA 19.9 and the lewis phenotype: Options to improve diagnostic efficiency. Anticancer Res. 2018, 38, 5883–5888. [Google Scholar] [CrossRef]
- Lee, T.; Teng, T.Z.J.; Shelat, V.G. Carbohydrate antigen 19-9—Tumor marker: Past, present, and future. World J. Gastrointest. Surg. 2020, 12, 468–490. [Google Scholar] [CrossRef]
- Duffy, M.J.; Sturgeon, C.; Lamerz, R.; Haglund, C.; Holubec, V.L.; Klapdor, R.; Nicolini, A.; Topolcan, O.; Heinemann, V. Tumor markers in pancreatic cancer: A European Group on Tumor Markers (EGTM) status report. Ann. Oncol. 2009, 21, 441–447. [Google Scholar] [CrossRef]
- Goonetilleke, K.S.; Siriwardena, A.K. Systematic review of carbohydrate antigen (CA 19-9) as a biochemical marker in the diagnosis of pancreatic cancer. Eur. J. Surg. Oncol. 2007, 33, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Ermiah, E.; Eddfair, M.; Abdulrahman, O.; Elfagieh, M.; Jebriel, A.; Al-Sharif, M.; Assidi, M.; Buhmeida, A. Prognostic value of serum CEA and CA19-9 levels in pancreatic ductal adenocarcinoma. Mol. Clin. Oncol. 2022, 17, 126. [Google Scholar] [CrossRef]
- Steinberg, W. The clinical utility of the CA 19-9 tumor-associated antigen. Am. J. Gastroenterol. 1990, 85, 350–355. [Google Scholar]
- Tessler, D.A.; Catanzaro, A.; Velanovich, V.; Havstad, S.; Goel, S. Predictors of cancer in patients with suspected pancreatic malignancy without a tissue diagnosis. Am. J. Surg. 2006, 191, 191–197. [Google Scholar] [CrossRef]
- Patel, A.H.; Amin, R.; Lalos, A.T. Acute liver injury and IgG4-related autoimmune pancreatitis following mRNA-based COVID-19 vaccination. Hepatol. Forum 2022, 3, 97–99. [Google Scholar] [CrossRef]
- Chahed, F.; Ben Fadhel, N.; Maamri, K.; Abdelali, M.; Ben Romdhane, H.; Chadli, Z.; Ben Fredj, N.; Zrig, A.; Aouam, K.; Chaabane, A. An unusual occurrence of autoimmune pancreatitis after gam-COVID-Vac (Sputnik V): A case report and literature review. Br. J. Clin. Pharmacol. 2023, 89, 2915–2919. [Google Scholar] [CrossRef] [PubMed]
- Becker, E.C.; Siddique, O.; Kapur, D.; Patel, K.; Mehendiratta, V. Type 1 Autoimmune Pancreatitis Unmasked by COVID-19 Vaccine. ACG Case Rep. J. 2023, 10, 950. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, T.; Komanduri, S. Seronegative type i autoimmune pancreatitis with immunoglobulin g4-related disease triggered by the pfizer-biontech COVID-19 vaccine. Gastrointest. Endosc. 2022, 95, 36. [Google Scholar] [CrossRef]
- Aochi, S.; Uehara, M.; Yamamoto, M. IgG4-related Disease Emerging after COVID-19 mRNA Vaccination. Intern. Med. 2023, 62, 1547–1551. [Google Scholar] [CrossRef] [PubMed]
- Zafar, M.; Gordon, K.; Macken, L.; Parvin, J.; Heath, S.; Whibley, M.; Tibble, J. COVID-19 Vaccination-Induced Cholangiopathy and Autoimmune Hepatitis: A Series of Two Cases. Cureus 2022, 14, e30304. [Google Scholar] [CrossRef] [PubMed]
- Bril, F.; Al Diffalha, S.; Dean, M.; Fettig, D.M. Autoimmune hepatitis developing after coronavirus disease 2019 (COVID-19) vaccine: Causality or casualty? J. Hepatol. 2021, 75, 222–224. [Google Scholar] [CrossRef] [PubMed]
- McShane, C.; Kiat, C.; Rigby, J.; Crosbie, Ó. The mRNA COVID-19 vaccine–A rare trigger of autoimmune hepatitis? J. Hepatol. 2021, 75, 1252–1254. [Google Scholar] [CrossRef] [PubMed]
- Correia de Sá, T.; Soares, C.; Rocha, M. Acute pancreatitis and COVID-19: A literature review. World J. Gastrointest. Surg. 2021, 13, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Kanduc, D.; Shoenfeld, Y. Molecular mimicry between SARS-CoV-2 spike glycoprotein and mammalian proteomes: Implications for the vaccine. Immunol. Res. 2020, 68, 310–313. [Google Scholar] [CrossRef]
- Rasappan, K.; Shaw, L.K.R.M.Y.; Chan, L.W.M.; Chuah, K.L.; Cheng, M.H.W. A case of raised CA 19–9 in a patient with desmoplastic fibroblastoma of the upper limb. Int. Cancer Conf. J. 2021, 10, 222–227. [Google Scholar] [CrossRef]
- Howaizi, M.; Abboura, M.; Krespine, C.; Sbai-Idrissi, M.S.; Marty, O.; Djabbari-Sobhani, M. A new cause for CA19.9 elevation: Heavy tea consumption. Gut 2003, 52, 913–914. [Google Scholar] [CrossRef]
- Khandelwal, A.; Inoue, D.; Takahashi, N. Autoimmune pancreatitis: An update. Abdom. Radiol. 2020, 45, 1359–1370. [Google Scholar] [CrossRef]
- Shimosegawa, T.; Chari, S.T.; Frulloni, L.; Kamisawa, T.; Kawa, S.; Mino-Kenudson, M.; Kim, M.H.; Klöppel, G.; Lerch, M.M.; Löhr, M.; et al. International consensus diagnostic criteria for autoimmune pancreatitis: Guidelines of the International Association of Pancreatology. Pancreas 2011, 26, 352–358. [Google Scholar] [CrossRef]
- Kim, K.P.; Kim, M.H.; Kim, J.C.; Lee, S.S.; Seo, D.W.; Lee, S.K. Diagnostic criteria for autoimmune chronic pancreatitis revisited. World J. Gastroenterol. 2006, 12, 2487–2496. [Google Scholar] [CrossRef] [PubMed]
- Jani, N. Autoimmune pancreatitis and cholangitis. World J. Gastrointest. Pharmacol. Ther. 2015, 6, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Nakamura, T.; Fujimori, N.; Niina, Y.; Igarashi, H.; Oono, T.; Uchida, M.; Kawabe, K.; Takayanagi, R.; Nishimori, I.; et al. Characteristics of pancreatic diabetes in patients with autoimmune pancreatitis. J. Dig. Dis. 2011, 12, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Nishimori, I.; Tamakoshi, A.; Kawa, S.; Tanaka, S.; Takeuchi, K.; Kamisawa, T.; Saisho, H.; Hirano, K.; Okamura, K.; Yanagawa, N.; et al. Influence of steroid therapy on the course of diabetes mellitus in patients with autoimmune pancreatitis: Findings from a nationwide survey in Japan. Pancreas 2006, 32, 244–248. [Google Scholar] [CrossRef]
- Ogawa, H.; Takehara, Y.; Naganawa, S. Imaging diagnosis of autoimmune pancreatitis: Computed tomography and magnetic resonance imaging. J. Med. Ultrason. 2021, 48, 565–571. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sex | Age | Symptoms Prior to Diagnosis (Yes, No) | CA 19-9 Serum Concentration [U/mL] | Final Diagnosis | Any CA 19-9 Decrease after Treatment (Yes, No) | CA 19-9 Normalization after Treatment (<37 U/mL) (Yes, No) | Time to Normalization of CA 19-9 after Therapy (Days) | Reference |
|---|---|---|---|---|---|---|---|---|
| Lungs, bronchi, and mediastinum diseases | ||||||||
| Female | 80 | Yes | 1118 | Interstitial pulmonary disease | NA | NA | NA | [4] |
| Male | 57 | Yes | 1300 | Bronchogenic cyst | Yes | Yes | 0.5 month | [5] |
| Female | 48 | Yes | >1200 | Bronchogenic cyst | Yes | Yes | 2 months | [6] |
| Male | 39 | Yes | 3051.1 | Pulmonary sequestration | Yes | Yes | 6 months | [7] |
| Female | 46 | Yes | 2810.3 | Pulmonary sequestration | Yes | Yes | 3 months | [8] |
| Female | 67 | Yes | >1500 | Bronchiectasis | Yes | No | No | [9] |
| Spleen diseases | ||||||||
| Female | 20 | Yes | 43,000 | Epidermoid splenic cyst | Yes | NA | NA | [10] |
| Female | 23 | Yes | 17,580 | Epidermoid splenic cyst | Yes | Yes | 4 months | [11] |
| Female | 33 | Yes | 3347 | Epidermoid splenic cyst | Yes | Yes | 0.5 month | [12] |
| Male | 25 | Yes | 2878 | Epidermoid splenic cyst | Yes | Yes | 0.68 month | [13] |
| Male | 52 | Yes | 1918 | Epidermoid splenic cyst | Yes | Yes | 2 months | [14] |
| Female | 24 | Yes | 1200 | Epidermoid splenic cyst | NA | NA | NA | [15] |
| Male | 16 | Yes | 1264 | Epidermoid splenic cyst | Yes | Yes | 0.23 month | [16] |
| Kidney diseases | ||||||||
| Male | 58 | Yes | 3500 | Hydronephrosis | Yes | Yes | 2 months | [17] |
| Female | 56 | No | 3049 | Hydronephrosis | Yes | Yes | 6 months | [18] |
| Female | 42 | Yes | 2500 | Hydronephrosis | Yes | Yes | NA | [19] |
| Female | 74 | Yes | >1000 | Hydronephrosis | Yes | Yes | NA | [20] |
| Ovary and uterine diseases | ||||||||
| Female | 25 | No | 1430 | Epidermoid cyst | Yes | Yes | NA | [21] |
| Female | 50 | Yes | 8922.76 | Teratoma | Yes | Yes | NA | [22] |
| Female | 27 | No | 3498 | Teratoma | Yes | Yes | 6 months | [23] |
| Female | 26 | No | 1633.68 | Teratoma | Yes | No | No | [24] |
| Female | 37 | Yes | 2753 | Mucinous cystadenoma | Yes | Yes | NA | [25] |
| Female | 55 | Yes | 1999 | Mucinous cystadenoma | Yes | Yes | 2 months | [26] |
| Female | 27 | Yes | 7946 | Ovarian endometrioma | Yes | Yes | NA | [27] |
| Female | 34 | Yes | 7604 | Ovarian endometrioma | Yes | Yes | 1.5 months | [28] |
| Female | 39 | No | 1796 | Denomyoma | Yes | Yes | NA | [29] |
| Female | 13 | Yes | >1000 | Hydrometrocolpos | Yes | Yes | 0.5 month | [30] |
| Liver and biliary tract diseases | ||||||||
| Male | 71 | Yes | 21,068 | Mirizzi syndrome | Yes | No | NA | [31] |
| Male | 71 | Yes | >16,000 | Mirizzi syndrome | Yes | Yes | 0.16 month | [32] |
| Female | 72 | Yes | 14,632 | Liver inflammatory pseudotumor | Yes | Yes | 1 month | [33] |
| Male | 50 | Yes | 1167.9 | Liver inflammatory pseudotumor | Yes | Yes | 1 month | [34] |
| Female | 66 | Yes | 6000 | Pyogenic liver abscess | Yes | Yes | 2 months | [35] |
| Female | 45 | Yes | 1930 | Hepatic steatosis | Yes | No | NA | [36] |
| Female | 70 | Yes | 2700 | Biliary cystadenoma | Yes | Yes | 2 months | [37] |
| Pancreas diseases | ||||||||
| Male | 38 | Yes | >12,000 | Autoimmune pancreatitis | Yes | No | NA | [38] |
| Male | 72 | Yes | >12,000 | Autoimmune pancreatitis | Yes | No | 1 month | [38] |
| Male | 72 | Yes | >10,000 | Autoimmune pancreatitis | Yes | NA | NA | [39] |
| Male | 70 | Yes | 8000 | Autoimmune pancreatitis | NA | NA | NA | [38] |
| Male | 31 | Yes | 3282 | Autoimmune pancreatitis | NA | NA | NA | [40] |
| Male | 69 | Yes | 1950 | Autoimmune pancreatitis | NA | NA | NA | [38] |
| Male | 25 | Yes | 18,860 | Pancreatic tuberculosis | NA | NA | NA | [41] |
| Female | 26 | No | 1036 | Heterotopic pancreas | Yes | NA | NA | [42] |
| Others | ||||||||
| Female | 61 | Yes | 12,000 | Diaphragmatic epidermoid cyst | Yes | Yes | 3 months | [43] |
| Female | 42 | No | 2410 | Giardiasis | Yes | Yes | 0.32 month | [44] |
| Female | 36 | No | 1880 | H. Pylori infection | Yes | Yes | NA | [45] |
| Female | 70 | Yes | 1000 | Rheumatoid polyarthritis with pulmonary fibrosis | NA | NA | NA | [46] |
| Male | 52 | No | 96,544.3 | No etiological factor was found | Yes | No | NA | [47] |
| Disease Category | Female; n (%) | Male; n (%) | Median Age | Median CA 19-9 Values |
|---|---|---|---|---|
| Lungs, bronchi, and mediastinum | 4 (66.7) | 2 (33.3) | 52.5 (IQR, 46.5–52.5) | 1400 (IQR, 1225–2483) |
| Spleen | 4 (57.1) | 3 (42.9) | 24 (IQR, 21.5–29) | 2878 (IQR, 1591–10,464) |
| Kidney | 3 (75) | 1 (25) | 57 (IQR, 52.5–62) | 2775 (IQR, 2125–3162) |
| Ovary and uterus | 10 (100) | 0 (0) | 30.5 (IQR, 26.3–38.5) | 2376 (IQR, 1674–6578) |
| Liver and biliary tract | 4 (57.1) | 3 (42.9) | 70 (IQR 58–71) | 6000 (IQR, 2315–15,316) |
| Pancreas | 1 (12.5) | 7 (87.5) | 53.5 (IQR, 29.8–70.5) | 9000 (IQR, 2949–12,000) |
| Others | 4 (80) | 1 (20) | 52 (IQR, 42–61) | 2410 (IQR, 1880–12,000) |
| Sex | Age | Vaccine | The Onset of Symptoms after the Primary (P) or Secondary (S) Dose; Time Interval from Vaccination | Confirmed Other Autoimmune Diseases | Confirmed Elevation of CA 19-9 | Ref. |
|---|---|---|---|---|---|---|
| M | 63 | COVID-19-mRNA | S; 60 days | no | no | [58] |
| M | 39 | Gam-COVID-Vac (Sputnik V) | S; 4 days | no | no | [59] |
| M | 54 | Pfizer/BioNTech COVID-19 mRNA | S; 30 days | yes | no | [60] |
| M | 65 | Pfizer/BioNTech COVID-19 mRNA | P; 14 days | no | no | [61] |
| F | 78 | Pfizer/BioNTech COVID-19 mRNA | S; 14 days | no | no | [62] |
| Autoimmune Chronic Pancreatitis (AIP) Diagnostic Criteria | Presented Case | |
|---|---|---|
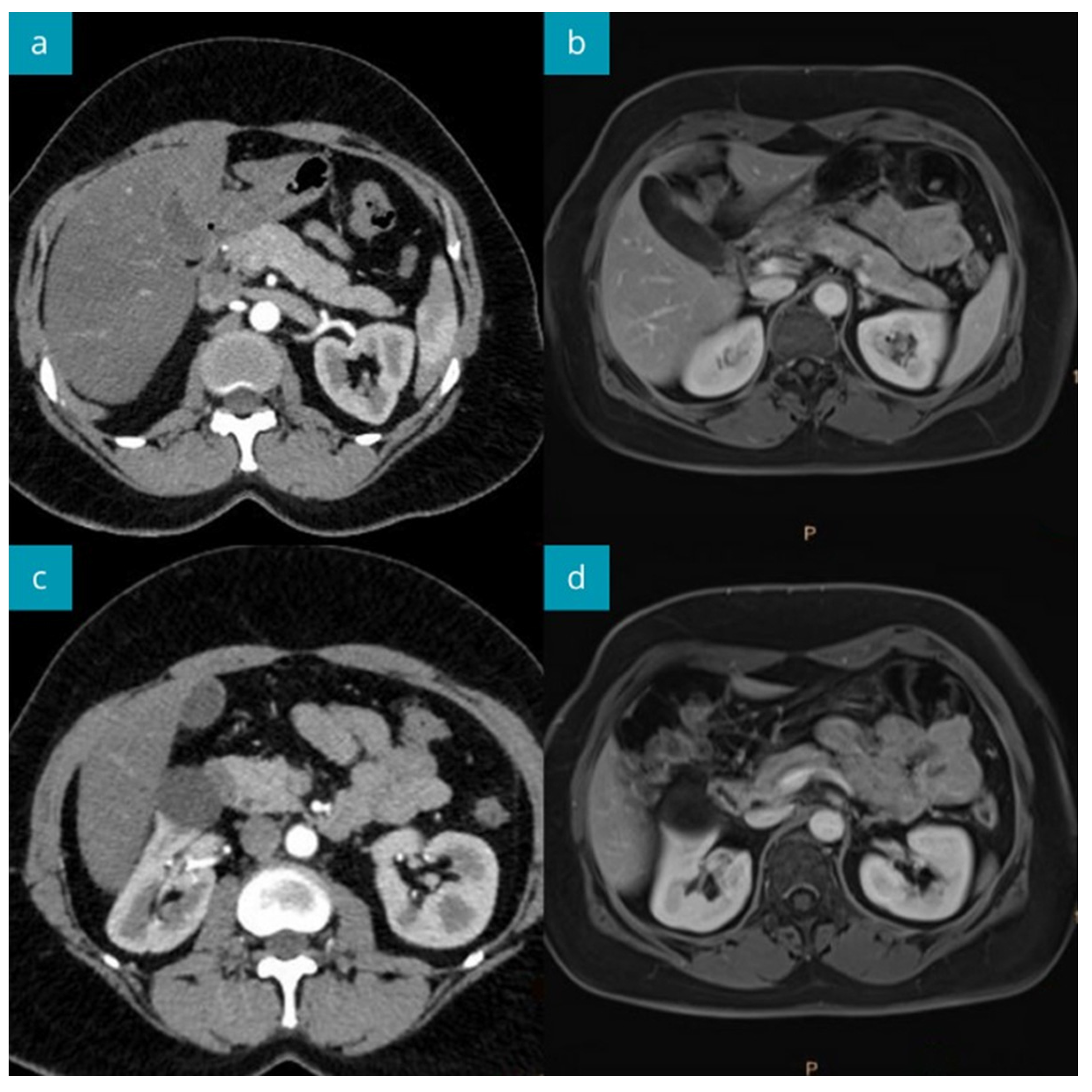
| Criterion I: Pancreatic Imagining | CT: Diffuse enlargement (swelling) of the pancreas | Yes |
| ERCP: Diffuse or segmental irregular narrowing of the main pancreatic duct | No | |
| Criterion II: Laboratory Findings | Elevated levels of IgG and/or IgG4 | No data |
| Detected autoantibodies | No data | |
| Criterion III: Histopathologic findings | Fibrosis and lymphoplasmacytic infiltration | No data |
| Criterion IV: Association of other postulated autoimmune disease | No | |
| Definite: I + II + III + I or I + II + III or I + II/I + III Probable: I + IV (Rediagnosed as ‘’definite” if respond to steroid is present) Possible: Only I | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciesielka, J.; Jakimów, K.; Tekiela, N.; Peisert, L.; Kwaśniewska, A.; Kata, D.; Chudek, J. Significantly Elevated CA 19-9 after COVID-19 Vaccination and Literature Review of Non-Cancerous Cases with CA 19-9 > 1000 U/mL. J. Clin. Med. 2024, 13, 1263. https://doi.org/10.3390/jcm13051263
Ciesielka J, Jakimów K, Tekiela N, Peisert L, Kwaśniewska A, Kata D, Chudek J. Significantly Elevated CA 19-9 after COVID-19 Vaccination and Literature Review of Non-Cancerous Cases with CA 19-9 > 1000 U/mL. Journal of Clinical Medicine. 2024; 13(5):1263. https://doi.org/10.3390/jcm13051263
Chicago/Turabian StyleCiesielka, Jakub, Krzysztof Jakimów, Natalia Tekiela, Laura Peisert, Anna Kwaśniewska, Dariusz Kata, and Jerzy Chudek. 2024. "Significantly Elevated CA 19-9 after COVID-19 Vaccination and Literature Review of Non-Cancerous Cases with CA 19-9 > 1000 U/mL" Journal of Clinical Medicine 13, no. 5: 1263. https://doi.org/10.3390/jcm13051263