


Ozone Therapy as an Adjuvant in the Treatment of Periodontitis
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
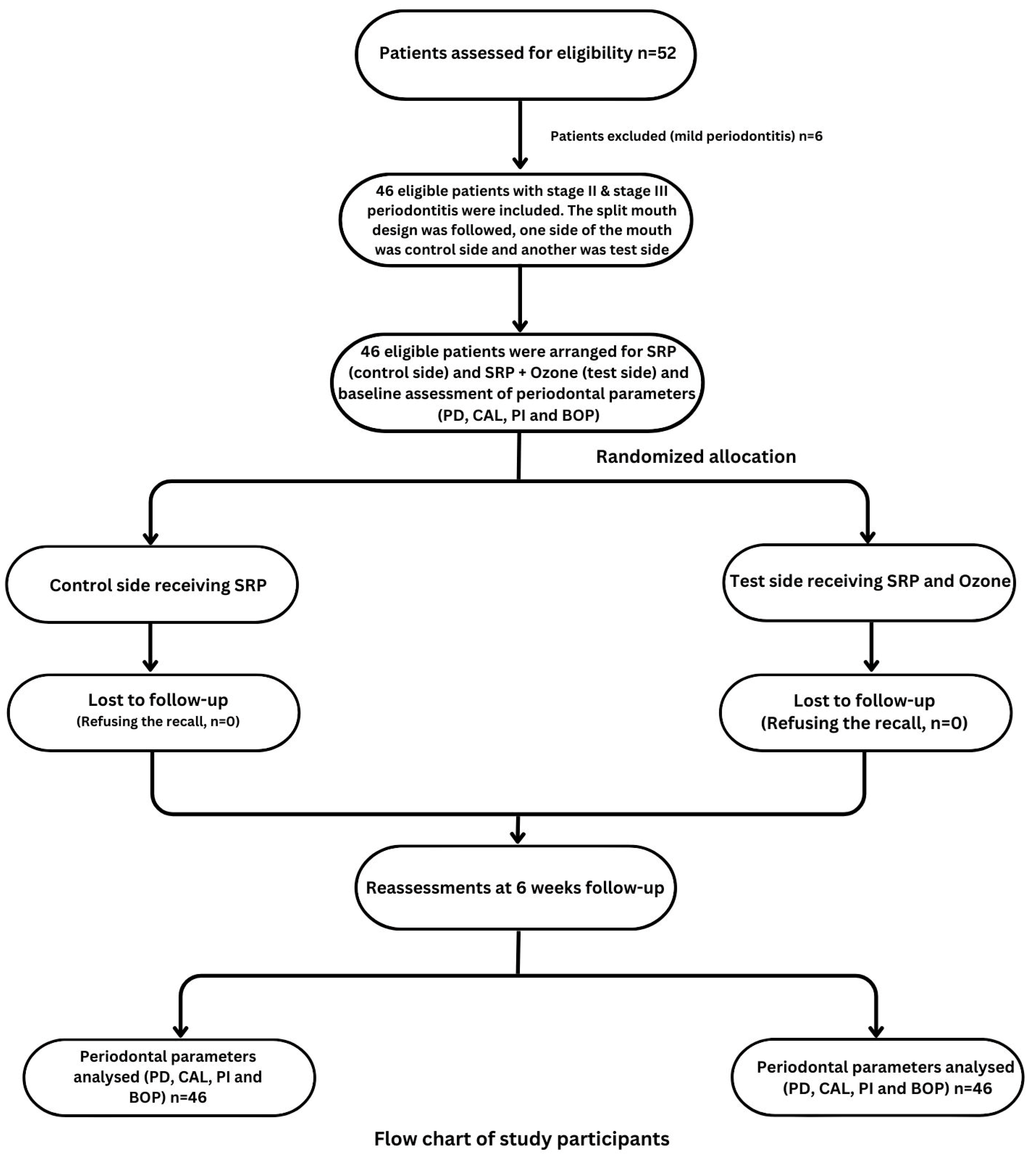
2. Materials and Methods
Statistical Analyses and Sample Size Calculation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45, S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.; Tay, J.R.H.; Ong, M.M.A. Minimally invasive periodontology: A treatment philosophy and suggested approach. Int. J. Dent. 2021, 2021, 2810264. [Google Scholar] [CrossRef] [PubMed]
- Haffajee, A.D.; Socransky, S.S. Microbial etiological agents of destructive periodontal diseases. Periodontology 2000 1994, 5, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L. Disease progression: Identification of high-risk groups and individuals for periodontitis. J. Clin. Periodontol. 2005, 32, 196–209. [Google Scholar] [CrossRef] [PubMed]
- Detert, J.; Pischon, N.; Burmester, G.R.; Buttgereit, F. The association between rheumatoid arthritis and periodontal disease. Arthritis Res. Ther. 2010, 12, 218. [Google Scholar] [CrossRef]
- Lee, J.M.; Kim, J.H.; Kwon, E.Y.; Kim, Y.K.; Lee, J.Y.; Kim, S.J.; Choi, J.I. Comparative study on the results of non-surgical periodontal treatment according to the location of the affected site. J. Periodontal Implant Sci. 2011, 41, 92–97. [Google Scholar] [CrossRef]
- Quaglia, E.; Moscufo, L.; Corsalini, M.; Coscia, D.; Sportelli, P.; Cantatore, F.; De Rinaldis, C.; Rapone, B.; Carossa, M.; Carossa, S. Polyamide vs silk sutures in the healing of postextraction sockets: A split mouth study. Oral Implantol. 2018, 11, 115–120. [Google Scholar]
- Cobb, C.M.; Sottosanti, J.S. A re-evaluation of scaling and root planing. J. Periodontol. 2021, 92, 1370–1378. [Google Scholar] [CrossRef]
- Van der Weijden, G.; Timmerman, M. A systematic review on the clinical efficacy of subgingival debridement in the treatment of chronic periodontitis. J. Clin. Periodontol. 2002, 29, 55–71. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.; Trombelli, L.; Heitz, F.; Needleman, I.; Moles, D. A systematic review of the effect of surgical debridement vs. non-surgical debridement for the treatment of chronic periodontitis. J. Clin. Periodontol. 2002, 29, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Nagarakanti, S.; Gunupati, S.; Chava, V.K.; Reddy, B.V.R. Effectiveness of subgingival irrigation as an adjunct to scaling and root planing in the treatment of chronic periodontitis: A systematic review. J. Clin. Diagn. Res. 2015, 9, 06–09. [Google Scholar] [CrossRef] [PubMed]
- Waerhaug, J. Healing of the Dento-Epithelial Junction Following Subgingival Plaque Control: II: As Observed on Extracted Teeth. J. Periodontol. 1978, 49, 119–134. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, G.M.; Ash, M.M.; Caffesse, R.G. The effectiveness of subgingival scaling and root planing in calculus removal. J. Periodontol. 1981, 52, 119–123. [Google Scholar] [CrossRef]
- Uraz, A.; Karaduman, B.; Isler, S.Ç.; Gönen, S.; Çetiner, D. Ozone application as adjunctive therapy in chronic periodontitis: Clinical, microbiological and biochemical aspects. J. Dent. Sci. 2019, 14, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Teughels, W.; De Soete, M.; Van Steenberghe, D. Topical antiseptics and antibiotics in the initial therapy of chronic adult periodontitis: Microbiological aspects. Periodontology 2000 2002, 28, 72–90. [Google Scholar] [CrossRef]
- Issac, A.V.; Mathew, J.J.; Ambooken, M.; Kachappilly, A.J.; Ajithkumar, P.; Johny, T.; Linith, V.; Samuel, A. Management of chronic periodontitis using subgingival irrigation of ozonized water: A clinical and microbiological study. J. Clin. Diagn. Res. 2015, 9, 29–33. [Google Scholar] [CrossRef]
- Edmondo, F. Apparatus for the Production and Use of Ozone in Therapeutics. U.S. Patent No 2,054,367, 15 September 1936. [Google Scholar]
- Gupta, G.; Mansi, B. Ozone therapy in periodontics. J. Med. Life 2012, 5, 59–67. [Google Scholar]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Topi, S.; Gnoni, A.; Dipalma, G.; Mancini, A.; Di Domenico, M.; Tartaglia, G.M.; Scarano, A. The Gaseous Ozone Therapy as a Promising Antiseptic Adjuvant of Periodontal Treatment: A Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 985. [Google Scholar] [CrossRef]
- Ramirez-Peña, A.M.; Sánchez-Pérez, A.; Campos-Aranda, M.; Hidalgo-Tallón, F.J. Ozone in patients with periodontitis: A clinical and microbiological study. J. Clin. Med. 2022, 11, 2946. [Google Scholar] [CrossRef]
- Carinci, F.; Palmieri, A.; Girardi, A.; Cura, F.; Lauritano, D. Aquolab® ozone-therapy is an efficient adjuvant in the treatment of chronic periodontitis: A case-control study. J. Orofac. Sci. 2015, 7, 27–32. [Google Scholar]
- Tasdemir, Z.; Oskaybas, M.N.; Alkan, A.B.; Cakmak, O. The effects of ozone therapy on periodontal therapy: A randomized placebo-controlled clinical trial. Oral Dis. 2019, 25, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Das, S. Application of ozone therapy in dentistry. Indian J. Dent. Adv. 2011, 3, 538–542. [Google Scholar]
- Srikanth, A.; Sathish, M.; Harsha, A.V.S. Application of ozone in the treatment of periodontal disease. J. Pharm. Bioallied Sci. 2013, 5, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Di Paolo, N.; Bocci, V.; Gaggiotti, E. Ozone therapy. Int. J. Artif. Organs 2004, 27, 168–175. [Google Scholar] [CrossRef]
- Cosola, S.; Giammarinaro, E.; Genovesi, A.; Pisante, R.; Poli, G.; Covani, U.; Marconcini, S. A short-term study of the effects of ozone irrigation in an orthodontic population with fixed appliances. Eur. J. Paediatr. Dent. 2019, 20, 15–18. [Google Scholar]
- Saini, R. Ozone therapy in dentistry: A strategic review. J. Nat. Sci. Biol. Med. 2011, 2, 151–153. [Google Scholar] [CrossRef]
- Hodson, N.; Dunne, S.M.; Swift, E.J., Jr. Using ozone to treat dental caries. J. Esthet. Restor. Dent. 2007, 19, 303–305. [Google Scholar] [CrossRef]
- Scarano, A.; Inchingolo, F.; Rapone, B.; Festa, F.; RexhepTari, S.; Lorusso, F. Protective face masks: Effect on the oxygenation and heart rate status of oral surgeons during surgery. Int. J. Environ. Res. Public Health 2021, 18, 2363. [Google Scholar] [CrossRef]
- Suvan, J.; Leira, Y.; Moreno Sancho, F.M.; Graziani, F.; Derks, J.; Tomasi, C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J. Clin. Periodontol. 2020, 47, 155–175. [Google Scholar] [CrossRef]
- Hoffman, R. Toxic gases. Inhib. Destr. Microb. Cell 1971, 4, 225–258. [Google Scholar]
- Krammer, F. Ozone in the dental practice. In Medical Applications of Ozone; International Ozone Association, Pan American Committee: Norwalk, CT, USA, 1983; Volume 1, pp. 258–265. [Google Scholar]
- O’leary, T.J. The plaque control record. J. Periodontol. 1972, 43, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Scorzetti, L.; Marcattili, D.; Pasini, M.; Mattei, A.; Marchetti, E.; Marzo, G. Association between obesity and periodontal disease in children. Eur. J. Paediatr. Dent. 2013, 14, 181–184. [Google Scholar]
- Akdeniz, S.S.; Beyler, E.; Korkmaz, Y.; Yurtcu, E.; Ates, U.; Araz, K.; Sahin, F.; Torun, O. The effects of ozone application on genotoxic damage and wound healing in bisphosphonate-applied human gingival fibroblast cells. Clin. Oral Investig. 2018, 22, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Alpan, A.L.; Toker, H.; Ozer, H. Ozone therapy enhances osseous healing in rats with diabetes with calvarial defects: A morphometric and immunohistochemical study. J. Periodontol. 2016, 87, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, H.; Toker, H.; Balcı, H.; Ozer, H. Effect of ozone therapy on autogenous bone graft healing in calvarial defects: A histologic and histometric study in rats. J. Periodont. Res. 2013, 48, 722–726. [Google Scholar] [CrossRef]
- Taşdemir, Z.; Taşdemir, F.Ö.; Koçyiğit, İ.; Gürgan, C.A. The clinical and systemic effects of periodontal treatment in diabetic and non-diabetic obese patients. J. Oral Sci. 2016, 58, 523–531. [Google Scholar] [CrossRef]
- Yılmaz, S.; Algan, S.; Gursoy, H.; Noyan, U.; Kuru, B.E.; Kadir, T. Evaluation of the clinical and antimicrobial effects of the Er: YAG laser or topical gaseous ozone as adjuncts to initial periodontal therapy. Photomed. Laser Surg. 2013, 31, 293–298. [Google Scholar] [CrossRef]
- Al Habashneh, R.; Alsalman, W.; Khader, Y. Ozone as an adjunct to conventional nonsurgical therapy in chronic periodontitis: A randomized controlled clinical trial. J. Periodont. Res. 2015, 50, 37–43. [Google Scholar] [CrossRef]
- Nagayoshi, M.; Kitamura, C.; Fukuizumi, T.; Nishihara, T.; Terashita, M. Antimicrobial effect of ozonated water on bacteria invading dentinal tubules. J. Endod. 2004, 30, 778–781. [Google Scholar] [CrossRef]
- Ramzy, M.I.; Gomaa, H.E.; Mostafa, M.I.; Zaki, B.M. Management of aggressive periodontitis using ozonized water. Egypt. Med. J. NRC 2005, 6, 229–245. [Google Scholar]
- Huth, K.C.; Quirling, M.; Lenzke, S.; Paschos, E.; Kamereck, K.; Brand, K.; Hickel, R.; Ilie, N. Effectiveness of ozone against periodontal pathogenic microorganisms. Eur. J. Oral Sci. 2011, 119, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Azarpazhooh, A.; Limeback, H. The application of ozone in dentistry: A systematic review of literature. J. Dent. 2008, 36, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Nogales, C.G.; Ferrari, P.H.; Kantorovich, E.O.; Lage-Marques, J.L. Ozone therapy in medicine and dentistry. J. Contemp. Dent. Pract. 2008, 9, 75–84. [Google Scholar] [CrossRef]
- Morrison, E.C.; Ramfjord, S.P.; Hill, R. Short-term effects of initial, nonsurgical periodontal treatment (hygienic phase). J. Clin. Periodontol. 1980, 7, 199–211. [Google Scholar] [CrossRef]
- Proye, M.; Caton, J.; Polson, A. Initial healing of periodontal pockets after a single episode of root planing monitored by controlled probing forces. J. Periodontol. 1982, 53, 296–301. [Google Scholar] [CrossRef]
- Holmes, J.; Holmes, J. Zastosowanie ozonu do leczenia pierwotnych zmian próchnicowych bruzd. Por. Stomat. 2004, 39, 1–12. [Google Scholar]
- Sechi, L.A.; Lezcano, I.; Nunez, N.; Espim, M.; Duprè, I.; Pinna, A.; Molicotti, P.; Fadda, G.; Zanetti, S. Antibacterial activity of ozonized sunflower oil (Oleozon). J. Appl. Microb. 2001, 90, 279–284. [Google Scholar] [CrossRef]
- Albandar, J.M.; Rams, T.E. Global epidemiology of periodontal diseases: An overview. Periodontology 2000 2002, 29, 7–10. [Google Scholar] [CrossRef]
- Petersen, P.E.; Ogawa, H. Strengthening the prevention of periodontal disease: The WHO approach. J. Periodontol. 2005, 76, 2187–2193. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Mean | SD | |
|---|---|---|---|
| Age | 44.41 years | 9.10 | |
| Gender [N (%)] | Male | 31 (67.39) | |
| Female | 15 (32.61) | ||
| Control group | BOP | 62.46% | 20.49 |
| PI | 64.22% | 22.72 | |
| CAL | 5.54 mm | 1.06 | |
| PD | 5.02 mm | 1.10 | |
| Test group | BOP | 63.13% | 20.65 |
| PI | 63.78% | 21.61 | |
| CAL | 6.22 mm | 1.00 | |
| PD | 5.24 mm | 1.49 | |
| Variables (N = 46) | Z | p | |
|---|---|---|---|
| Baseline | BOP | −1.634 | 0.102 |
| PI | −0.049 | 0.961 | |
| CAL | −4.318 | 0.0001 * | |
| PD | −1.815 | 0.070 | |
| After 6 weeks | BOP | −4.715 | 0.0001 * |
| PI | −3.082 | 0.002 * | |
| CAL | −3.075 | 0.002 * | |
| PD | −5.256 | 0.001 * | |
| Variables (N = 46) | Baseline [Median (IQR)] | After 6th Week [Median (IQR)] | Z | p | |
|---|---|---|---|---|---|
| Control side | BOP | 57.50 (32.50) | 21.50 (20.00) | −5.907 | 0.0001 * |
| PI | 60.00 (39.25) | 20.00 (19.25) | −5.906 | 0.0001 * | |
| CAL | 5.00 (1.00) | 4.00 (1.00) | −5.562 | 0.0001 * | |
| PD | 5.00 (1.00) | 4.00 (2.00) | −5.599 | 0.0001 * | |
| Test side | BOP | 57.00 (30.25) | 10.00 (17.00) | −5.907 | 0.0001 * |
| PI | 62.50 (31.25) | 15.00 (21.25) | −5.907 | 0.0001 * | |
| CAL | 6.00 (2.00) | 4.00 (2.00) | −5.833 | 0.0001 * | |
| PD | 5.00 (1.00) | 3.00 (1.25) | −5.749 | 0.0001 * | |
| Variables (N = 46) | Control Side [Median (IQR)] | Test Side [Median (IQR)] | Z | p |
|---|---|---|---|---|
| BOP | 43.50 (26.25) | 50.00 (30.75) | −4.615 | 0.0001 * |
| PI | 44.50 (32.25) | 48 (30.75) | −2.038 | 0.042 * |
| CAL | 1.00 (0.00) | 2.00 (1.00) | −5.287 | 0.0001 * |
| PD | 1.00 (0.00) | 2.00 (1.00) | −5.488 | 0.0001 * |
| Variables (N = 46) | Z | p | |
|---|---|---|---|
| Control side | BOP | −0.434 | 0.664 |
| PI | −0.106 | 0.916 | |
| CAL | −1.183 | 0.237 | |
| PD | −1.557 | 0.119 | |
| Test side | BOP | −0.446 | 0.656 |
| PI | −0.305 | 0.760 | |
| CAL | −1.933 | 0.053 | |
| PD | −2.164 | 0.030 * | |
| Variables (N = 46) | Z | p | |
|---|---|---|---|
| Control side | BOP | −0.033 | 0.973 |
| PI | −0.536 | 0.592 | |
| CAL | −0.589 | 0.370 | |
| PD | −0.897 | 0.370 | |
| Test side | BOP | −1.239 | 0.215 |
| PI | −0.045 | 0.964 | |
| CAL | −1.010 | 0.312 | |
| PD | −1.611 | 0.107 | |
| Variables (N = 46) | Mean | SD | df | p | |
|---|---|---|---|---|---|
| Control side | BOP | 42.95 | 18.13 | 2 | 0.072 |
| PI | 43.96 | 18.13 | 0.238 | ||
| CAL | 0.96 | 0.63 | 0.676 | ||
| PD | 0.93 | 0.61 | 0.567 | ||
| Test side | BOP | 50.48 | 18.79 | 0.098 | |
| PI | 46.95 | 19.81 | 0.601 | ||
| CAL | 2.09 | 0.89 | 0.234 | ||
| PD | 2.09 | 0.98 | 0.113 | ||
| Variables (N = 46) | Standardized Coefficient (B) | CI | p | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| BOP | Gender | 0.034 | −12.01 | 14.65 | 0.843 |
| Age | 0.161 | −0.39 | 1.03 | 0.367 | |
| Stages | −0.071 | −16.42 | 11.25 | 0.708 | |
| Grades | 0.254 | −3.92 | 15.09 | 0.242 | |
| PI | Gender | 0.001 | −14.04 | 14.02 | 0.999 |
| Age | −0.092 | −0.94 | 0.56 | 0.608 | |
| Stages | 0.07 | −12.09 | 17.02 | 0.734 | |
| Grades | 0.026 | −9.41 | 10.58 | 0.906 | |
| CAL | Gender | −0.230 | −0.77 | 0.16 | 0.189 |
| Age | −0.101 | −0.03 | 0.02 | 0.571 | |
| Stages | 0.136 | −0.31 | 0.65 | 0.471 | |
| Grades | −0.102 | −0.41 | 0.25 | 0.637 | |
| PD | Gender | −0.300 | −0.82 | 0.05 | 0.079 |
| Age | −0.196 | −0.04 | 0.01 | 0.258 | |
| Stages | 0.159 | −0.25 | 0.65 | 0.386 | |
| Grades | −0.09 | −0.37 | 0.24 | 0.669 | |
| Variables (N = 46) | Standardized Coefficient (B) | CI | p | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| BOP | Gender | −0.050 | −15.59 | 11.66 | 0.772 |
| Age | 0.124 | −0.47 | 0.98 | 0.481 | |
| Stages | 0.151 | −8.44 | 19.85 | 0.420 | |
| Grades | 0.159 | −6.09 | 13.34 | 0.456 | |
| PI | Gender | −0.004 | −14.92 | 14.56 | 0.980 |
| Age | −0.056 | −0.91 | 0.66 | 0.758 | |
| Stages | −0.057 | −17.55 | 13.05 | 0.768 | |
| Grades | 0.125 | −7.49 | 13.52 | 0.566 | |
| CAL | Gender | −0.314 | −1.20 | 0.04 | 0.067 |
| Age | −0.143 | −0.05 | 0.02 | 0.407 | |
| Stages | 0.089 | −0.49 | 0.81 | 0.627 | |
| Grades | −0.014 | −0.46 | 0.43 | 0.948 | |
| PD | Gender | −0.474 | −1.59 | −0.37 | 0.002 * |
| Age | −0.413 | −0.08 | −0.01 | 0.009 * | |
| Stages | 0.240 | −0.16 | 1.11 | 0.139 | |
| Grades | −0.156 | −0.62 | 0.25 | 0.395 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsakr, A.; Gufran, K.; Alqahtani, A.S.; Alasqah, M.; Alnufaiy, B.; Alzahrani, H.G.; Alahmari, A.A.; Alhumaidani, F.K.; Alhumaidani, R.K.; Althobiti, M.J. Ozone Therapy as an Adjuvant in the Treatment of Periodontitis. J. Clin. Med. 2023, 12, 7078. https://doi.org/10.3390/jcm12227078
Alsakr A, Gufran K, Alqahtani AS, Alasqah M, Alnufaiy B, Alzahrani HG, Alahmari AA, Alhumaidani FK, Alhumaidani RK, Althobiti MJ. Ozone Therapy as an Adjuvant in the Treatment of Periodontitis. Journal of Clinical Medicine. 2023; 12(22):7078. https://doi.org/10.3390/jcm12227078
Chicago/Turabian StyleAlsakr, Abdulaziz, Khalid Gufran, Abdullah Saad Alqahtani, Mohammed Alasqah, Banna Alnufaiy, Hanadi Ghurmallah Alzahrani, Ali Ayidh Alahmari, Faisal Khaled Alhumaidani, Rakan Khaled Alhumaidani, and Mishari Jameel Althobiti. 2023. "Ozone Therapy as an Adjuvant in the Treatment of Periodontitis" Journal of Clinical Medicine 12, no. 22: 7078. https://doi.org/10.3390/jcm12227078