

Gossypiboma, the Hidden Enemy of an Emergency Cesarean Hysterectomy—Case Report and Review of the Literature
 , ,
, ,
Abstract
:1. Introduction
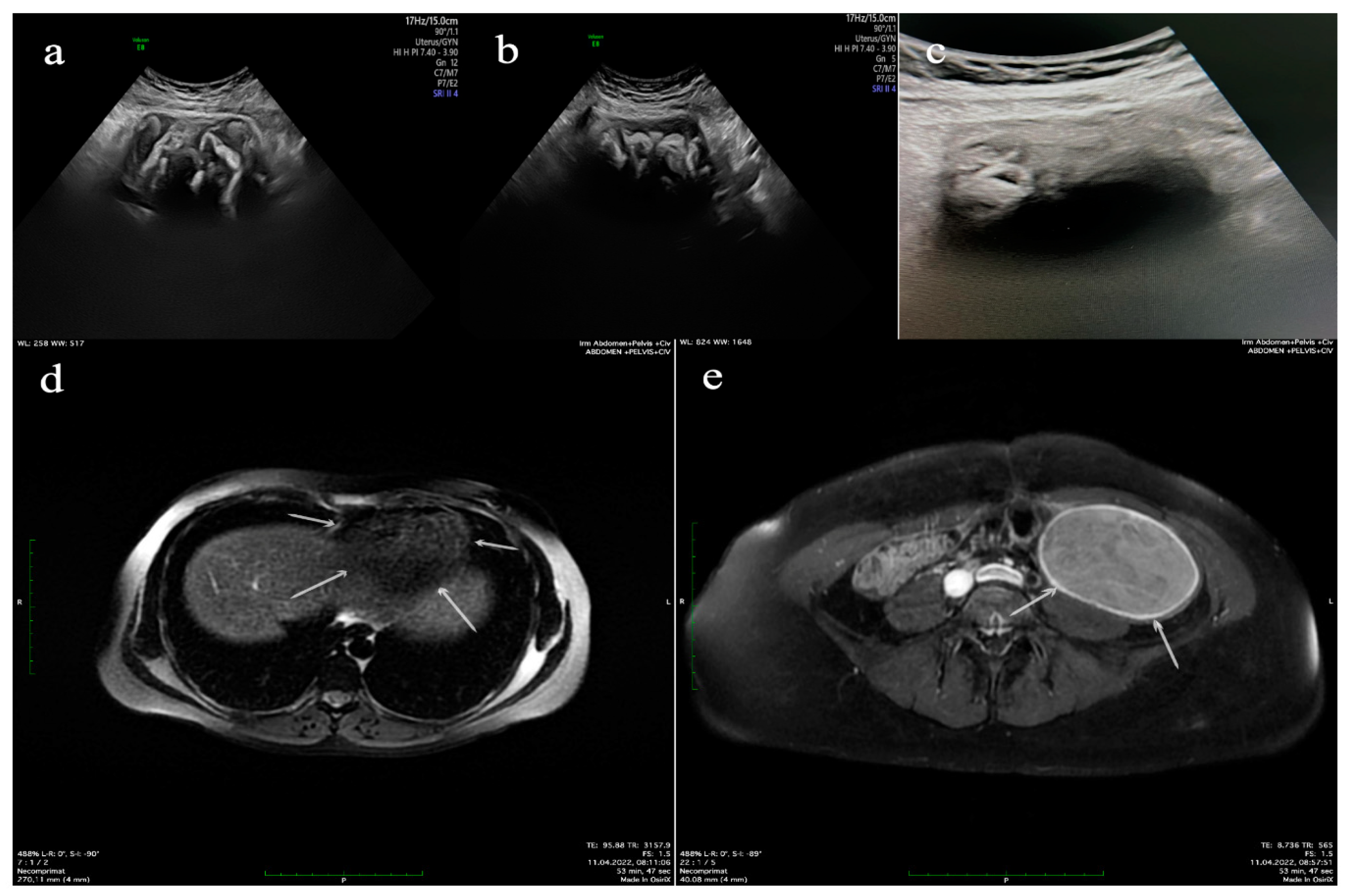
2. Case Report
- -
- Left adnexal tumor mass measuring 9.5 × 9.5 × 6.5 cm3; when sectioning, textile material with dimensions of 9 × 8 × 5 cm3 is evacuated; after the extraction of the textile material, the internal surface of the pseudocyst wall is intensely congestive, with greyish-yellow deposits; and isolated intramural nodular mass with dimensions of 4.5 × 4.5 × 1 cm3 of firm elastic consistency;
- -
- Subhepatic tumor mass with dimensions of 10 × 8 × 5.5 cm3 with a grayish-pink external surface with areas of fatty tissue; when sectioning, textile material with dimensions of 7 × 6 × 4 cm3 is extracted.
- -
- Left adnexal tumor mass: tissue fragment with a histopathological aspect of conjunctive-adipose and vascular–nervous tissue presenting multiple foci of chronic granulomatous inflammation with multinucleated foreign body giant cells arranged around exogenous, acellular, translucent materials; diffuse areas of fibroblast–fibrocystic proliferation; numerous groups of foamy histiocytes, some with a multinucleolate appearance; and marked capillary hyperemia, interstitial edema, and diffuse regions of hematic extravasation. The ovarian histological structure is identified at a certain level, with multiple foci of chronic granulomatous inflammation with foreign body multinucleated giant cells, in addition to tubal wall with lesions of chronic xanthogranulomatous salpingitis, discrete tubular epithelial hyperplasia, moderate capillary hyperemia, and intramural interstitial edema;
- -
- Right subhepatic tumor mass: tissue fragment with a histopathological aspect of conjunctive-adipose and vascular–nervous tissue presenting multiple foci of chronic granulomatous inflammation with multinucleated foreign body giant cells arranged around exogenous, acellular, translucent materials; diffuse areas of fibroblast–fibrocystic proliferation; numerous groups of foamy histiocytes, some with a multinucleolate appearance; and moderate capillary hyperemia, interstitial edema (Figure 3).
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chopra, S.; Suri, V.; Sikka, P.; Aggarwal, N. A Case Series on Gossypiboma—Varied Clinical Presentations and Their Management. J. Clin. Diagn. Res. JCDR 2015, 9, QR01–QR03. [Google Scholar] [CrossRef] [PubMed]
- Wan, W.; Le, T.; Riskin, L.; Macario, A. Improving Safety in the Operating Room: A Systematic Literature Review of Retained Surgical Sponges. Curr. Opin. Anaesthesiol. 2009, 22, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Hyslop, J.W.; Maull, K.I. Natural History of the Retained Surgical Sponge. South. Med. J. 1982, 75, 657–660. [Google Scholar] [CrossRef] [PubMed]
- Cima, R.R.; Kollengode, A.; Garnatz, J.; Storsveen, A.; Weisbrod, C.; Deschamps, C. Incidence and Characteristics of Potential and Actual Retained Foreign Object Events in Surgical Patients. J. Am. Coll. Surg. 2008, 207, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Fukatsu, T.; Oki, S.; Iizuka, Y.; Otsuka, Y.; Sanui, M.; Lefor, A.K. Characteristics of Retained Foreign Bodies and Near-Miss Events in the Operating Room: A Ten-Year Experience at One Institution. J. Anesth. 2023, 37, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Birolini, D.V.; Rasslan, S.; Utiyama, E.M. Unintentionally Retained Foreign Bodies after Surgical Procedures. Analysis of 4547 Cases. Rev. Colégio Bras. Cir. 2016, 43, 12–17. [Google Scholar] [CrossRef]
- Gavrić Lovrec, V.; Cokan, A.; Lukman, L.; Arko, D.; Takač, I. Retained Surgical Needle and Gauze after Cesarean Section and Adnexectomy: A Case Report and Literature Review. J. Int. Med. Res. 2018, 46, 4775–4780. [Google Scholar] [CrossRef]
- Bai, Y.-F.; Niu, J.-Q.; Zhang, C.; Wang, W.; Liu, J.-Z. Computed Tomography and Magnetic Resonance Imaging Appearances of Abdomen and Pelvis Gossypibomas at the Varied Durations After Cesarean Section. Cureus 2021, 13, e18588. [Google Scholar] [CrossRef]
- Lincourt, A.E.; Harrell, A.; Cristiano, J.; Sechrist, C.; Kercher, K.; Heniford, B.T. Retained Foreign Bodies after Surgery. J. Surg. Res. 2007, 138, 170–174. [Google Scholar] [CrossRef]
- Casal, M.A.; Jimenez, A.P.; Canessa, N. Jejunocolonic fistula caused by a gauze compress. Rev. Espanola Las Enfermedades Apar. Dig. Nutr. 1961, 20, 1097–1104. [Google Scholar]
- Al-Salem, A.H.; Khwaja, S. Intestinal Obstruction Due to Retained, Eroding Surgical Sponge. Case Report. Acta Chir. Scand. 1989, 155, 199–200. [Google Scholar] [PubMed]
- Reinke, J.; Biermann, F.J.; Bosse, U.; Krings, W. An unclear abdominal tumor. A pseudocyst in the mid abdomen caused by a retained abdominal towel from a previous cesarean section. Radiologe 1992, 32, 525–527. [Google Scholar] [PubMed]
- Haddad, B.R.; Usta, I.M.; Khalil, A.; Mufarrij, I. Spontaneous Closure of Enterovaginal Fistula Caused by a Neglected Foreign Body. Acta Obstet. Gynecol. Scand. 1994, 73, 598–600. [Google Scholar] [CrossRef]
- Rajagopal, A.; Martin, J. Gossypiboma—“a Surgeon’s Legacy”: Report of a Case and Review of the Literature. Dis. Colon Rectum 2002, 45, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Yuh-Feng, T.; Chin-Chu, W.; Cheng-Tau, S.; Min-Tsung, T. FDG PET CT Features of an Intraabdominal Gossypiboma. Clin. Nucl. Med. 2005, 30, 561–563. [Google Scholar] [CrossRef]
- Saidi, H.; Mohammed, U.; Machoki, M. An Unusual Abdominal Mass: Case Report. East Afr. Med. J. 2007, 84, 88–92. [Google Scholar] [CrossRef]
- Aminian, A. Gossypiboma: A Case Report. Cases J. 2008, 1, 220. [Google Scholar] [CrossRef]
- Zantvoord, Y.; van der Weiden, R.M.F.; van Hooff, M.H.A. Transmural Migration of Retained Surgical Sponges: A Systematic Review. Obstet. Gynecol. Surv. 2008, 63, 465–471. [Google Scholar] [CrossRef]
- Tandon, A.; Bhargava, S.K.; Gupta, A.; Bhatt, S. Spontaneous Transmural Migration of Retained Surgical Textile into Both Small and Large Bowel: A Rare Cause of Intestinal Obstruction. Br. J. Radiol. 2009, 82, e72–e75. [Google Scholar] [CrossRef]
- Uluçay, T.; Dizdar, M.G.; SunayYavuz, M.; Aşirdizer, M. The Importance of Medico-Legal Evaluation in a Case with Intraabdominal Gossypiboma. Forensic Sci. Int. 2010, 198, e15–e18. [Google Scholar] [CrossRef]
- Dash, B.B.; Mahey, R.; Kriplani, A.; Agarwal, N.; Bhatla, N. Textiloma, a Rare Pelvic Tumor. Arch. Gynecol. Obstet. 2010, 282, 707–709. [Google Scholar] [CrossRef]
- Patil, K.K.; Patil, S.K.; Gorad, K.P.; Panchal, A.H.; Arora, S.S.; Gautam, R.P. Intraluminal Migration of Surgical Sponge: Gossypiboma. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2010, 16, 221–222. [Google Scholar] [CrossRef]
- Govarjin, H.M.; Talebianfar, M.; Fattahi, F.; Akbari, M.E. Textiloma, Migration of Retained Long Gauze from Abdominal Cavity to Intestine. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2010, 15, 54–57. [Google Scholar]
- Mavrigiannaki, P.E.; Dastamani, C.; Vouza, E.; Lambropoulou, E.; Kairi-Vassilatou, E.; Kondi-Pafiti, A. Gossypiboma: A Rare Abdominal Lesion of Women after Cesarean Section, Usually Misdiagnosed as a Neoplasm. Clin. Exp. Obstet. Gynecol. 2011, 38, 294–296. [Google Scholar] [PubMed]
- Kawamura, Y.; Ogasawara, N.; Yamamoto, S.; Sasaki, M.; Kawamura, N.; Izawa, S.; Kobayashi, Y.; Kamei, S.; Miyachi, M.; Kasugai, K. Gossypiboma Mimicking Gastrointestinal Stromal Tumor Causing Intestinal Obstruction: A Case Report. Case Rep. Gastroenterol. 2012, 6, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Quraishi, A.H.M. Beyond a Gossypiboma. Case Rep. Surg. 2012, 2012, 263841. [Google Scholar] [CrossRef]
- Karasaki, T.; Nomura, Y.; Nakagawa, T.; Tanaka, N. Beware of Gossypibomas. BMJ Case Rep. 2013, 2013, bcr2013010059. [Google Scholar] [CrossRef] [PubMed]
- Rafie, B.A.; AbuHamdan, O.J.; Trengganu, N.S. Intraluminal Migration of Retained Surgical Sponge as a Cause of Intestinal Obstruction. J. Surg. Case Rep. 2013, 2013, rjt032. [Google Scholar] [CrossRef]
- Usta, T.A.; Yildirim, D.; Ozyurek, S.E.; Gundogdu, E.C. Conservative Treatment of a Gossypiboma Causing Uterine Wound Dehiscence. Case Rep. Obstet. Gynecol. 2013, 2013, 578027. [Google Scholar] [CrossRef]
- Kashima, S.; Yamamoto, R.; Miura, Y.; Abe, A.; Togashi, H.; Ishida, T.; Matsuo, S.; Numakura, K.; Habuchi, T. An intravesical foreign body by migration of remnant gauze into the bladder: A case report. Hinyokika Kiyo 2014, 60, 83–86. [Google Scholar]
- Rehman, A.; Baloch, N.U.-A.; Awais, M. Gossypiboma Diagnosed Fifteen Years after a Cesarean Section: A Case Report. Qatar Med. J. 2014, 2014, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, K.N.; Agarwal, A. Gossypiboma Posing as a Diagnostic Dilemma: A Case Report and Review of the Literature. Case Rep. Surg. 2014, 2014, 713428. [Google Scholar] [CrossRef] [PubMed]
- Faghani, M.; Fazel, A.R.; Roshandel, G. Small Bowel Obstruction and Enterocolic Fistula from a Gossypiboma after Caesarean Section. West Indian Med. J. 2014, 63, 539–540. [Google Scholar] [CrossRef]
- Lee, D.H. Inflammatory Gossypiboma in Young Female Athlete. J. Exerc. Rehabil. 2015, 11, 236–238. [Google Scholar] [CrossRef]
- Rafat, D.; Hakim, S.; Sabzposh, N.A.; Noor, N. Gossypiboma Mimicking as Dermoid Cyst of Ovary: A Case Report. J. Clin. Diagn. Res. JCDR 2015, 9, QD01–QD02. [Google Scholar] [CrossRef]
- Rabie, M.E.; Hosni, M.H.; Al Safty, A.; Al Jarallah, M.; Ghaleb, F.H. Gossypiboma Revisited: A Never Ending Issue. Int. J. Surg. Case Rep. 2015, 19, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Margonis, E.; Vasdeki, D.; Diamantis, A.; Koukoulis, G.; Christodoulidis, G.; Tepetes, K. Intestinal Obstruction and Ileocolic Fistula Due to Intraluminal Migration of a Gossypiboma. Case Rep. Surg. 2016, 2016, 3258782. [Google Scholar] [CrossRef] [PubMed]
- Susmallian, S.; Raskin, B.; Barnea, R. Surgical Sponge Forgotten for Nine Years in the Abdomen: A Case Report. Int. J. Surg. Case Rep. 2016, 28, 296–299. [Google Scholar] [CrossRef]
- Konstantinidis, C.; Vlachos, S. Urinary Retention as the Only Symptom of Retained Surgical Sponge (Gossypiboma), 29 Years After Cesarean Procedure. Urol. Case Rep. 2017, 11, 9–10. [Google Scholar] [CrossRef]
- Oran, E.; Yetkin, G.; Aygün, N.; Celayir, F.; Uludağ, M. Intraabdominal Gossypiboma: Report of Two Cases. Turk. J. Surg. 2018, 34, 77–79. [Google Scholar] [CrossRef]
- Kondo, T.; Murayama, A. Two Pelvic Masses. N. Engl. J. Med. 2018, 378, 752. [Google Scholar] [CrossRef] [PubMed]
- Fatima, K. Intraabdominal Gossypibomas with Variable CT Appearance: A Case Report. JPMA J. Pak. Med. Assoc. 2019, 69, 123–126. [Google Scholar] [PubMed]
- Bilali, V.; Bilali, S.; Mitrushi, A.; Pirushi, R.; Nina, H.; Ktona, E. Gossypiboma in Abdomen: Retained Surgical Gauze after a Cesarean Section. Il Giornale Di Chirurgia—J. Ital. Surg. Assoc. 2019, 40, 338–342. [Google Scholar]
- Mejri, A.; Arfaoui, K.; Aloui, B.; Yaakoubi, J. Gossypiboma: The Failure of a Successful Intervention. Pan Afr. Med. J. 2020, 36, 335. [Google Scholar] [CrossRef] [PubMed]
- Alemu, B.N.; Tiruneh, A.G. Gossypiboma: A Case Series and Literature Review. Ethiop. J. Health Sci. 2020, 30, 147–149. [Google Scholar] [CrossRef]
- Sankpal, J.; Tayade, M.; Rathore, J.; Parikh, A.; Gadekar, D.; S, S.F.; Sankpal, S. Oh, My Gauze !!!- A Rare Case Report of Laparoscopic Removal of an Incidentally Discovered Gossypiboma during Laparoscopic Cholecystectomy. Int. J. Surg. Case Rep. 2020, 72, 643–646. [Google Scholar] [CrossRef]
- Omar, A.S.; Mohammed, A.A. Retained Intra-Abdominal Surgical Sponge Causing Ileocolic Fistula Diagnosed by Colonoscopy. Int. J. Surg. Case Rep. 2020, 67, 62–65. [Google Scholar] [CrossRef]
- El Zemity, H.; Hakami, N.; Alfaki, M.A.A.; Khurizi, M.; Al-Zahrani, A. Intra-Abdominal Gossypiboma: A Rare Cause of Palpable Abdominal Mass with a Review of Literature. Cureus 2020, 12, e10930. [Google Scholar] [CrossRef]
- Amodeo, S.; Di Simone, N.; Chiantera, V.; Scambia, G.; Masciullo, V. Hysteroscopic Removal of a Gauze Inadvertently Retained in Uterus for Two Years Following Caesarean Section. J. Obstet. Gynaecol. J. Inst. Obstet. Gynaecol. 2021, 41, 481–483. [Google Scholar] [CrossRef]
- Jha, P.K.; Verma, A.; Ansari, M.A.; Srivastava, V. Gossypiboma Complicating as Colouterine Fistula in a Young Woman Post-Cesarean Section. Cureus 2021, 13, e17846. [Google Scholar] [CrossRef]
- lal Bairwa, B. Gossypiboma-an Unusual Cause of Surgical Abdomen and Surgeon’s Nightmare: A Rare Case Report. Int. J. Surg. Case Rep. 2021, 80, 105521. [Google Scholar] [CrossRef] [PubMed]
- Munihire, J.B.; Valimugighe, M.M.; Martin, N.W. Mesenteric Textiloma Early Discovery in a 31-Year-Old Female: A Case Report. Int. J. Surg. Case Rep. 2022, 97, 107439. [Google Scholar] [CrossRef]
- Ammar, A.S. A Case Report of Abdominal Sponge in Ileum in a Patient with Intestinal Obstruction. JPMA J. Pak. Med. Assoc. 2021, 71, 373–375. [Google Scholar] [CrossRef] [PubMed]
- Khanduri, A.; Gupta, J.; Ammar, H.; Gupta, R. Laparoscopic Removal of Retained Surgical Sponge After Caesarean Section: A Case Report. Cureus 2022, 14, e21375. [Google Scholar] [CrossRef] [PubMed]
- Elci, E. Foreign Body under the Skin after Caesarean Section: Case Report. J. Obstet. Gynaecol. J. Inst. Obstet. Gynaecol. 2021, 41, 477–478. [Google Scholar] [CrossRef] [PubMed]
- Min, J.; Lee, S.; Kim, W.; Kim, S.E. A Case Report of Neglected Gossypiboma Causing Abdominal Pain for 20 Years Post-Cesarean Section. J. Menopausal Med. 2022, 28, 139–141. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Age | Obstetric Diagnosis | Type of Surgery | Clinical Manifestations | Duration since the C-Section | Diagnostic Mode | Gossypiboma Characteristics | Relaparotomy | Complications |
|---|---|---|---|---|---|---|---|---|---|
| Casal [10] 1961 | N/A | N/A | CS | N/A | N/A | N/A | N/A | Resection anastomosis of the involved loops | Jejunocolonic fistula |
| Al-Salem [11] 1989 | N/A | N/A | CS | N/A | 3 years | N/A | Bowel transluminal migration of the sponge | Enterotomy and removal of the mass, resection, and anastomosis | Intestinal obstruction |
| Reinke [12] 1992 | N/A | N/A | CS | N/A | N/A | N/A | Mid-abdomen mass | N/A | N/A |
| Haddad [13] 1994 | 27 | II G, II P | CS, postpartum supracervical HT | Vaginal discharge, pelvic heaviness | 6 weeks | N/A | Seven 4 × 4 cm2 gauzes in the vagina | Conservative management | Jejunovaginal fistula |
| Rajagopal [14] 2002 | 31 | III P | CS | Abdominal mass | 12 weeks | USG *, CT * | 7.5 cm entangled small-bowel mass adherent to the sigmoid | Ileal resection of the fistulous segment and end-to-end anastomosis | Ileoileal fistula |
| Yuh-Feng [15] 2005 | 42 | II P | CS | Incidentaloma | N/A | CT **, PET CT * | Mass in the anterior right paramedian abdomen | Yes | No |
| Saidi [16] 2007 | 40 | I P | CS | Right mid-abdominal pain | 1 year | USG *, CT * | 10 cm mass in the right iliac fossa | Yes | No |
| Aminian [17] 2008 | 27 | I P | CS | Abdominal mass | 5 years | X-ray *, CT * | Retained gauze in the center of the abdomen | Yes | No |
| Zantvoord [18] 2008 | 39 | I P | CS | Tiredness | 12 weeks | X-ray *, CT * | Transmural migration of a 60 × 40 cm2 surgical gauze | - | No |
| Tandon [19] 2009 | 30 | I P | CS | Colicky abdominal pain and distension | 2 years | USG *, CECT * | Mass in the left lumbar region | Resection anastomosis of the involved loops | Mid-transverse colon and jejunal fistulization |
| Uluçay [20] 2010 | 22 | I P | CS | Left side abdominal pain, diarrhea | 7 months | Clinical *, X-ray **, USG *, CT * | 15 cm in diameter mass settled in the sigmoid colon | Resection of the sigmoid colon and small bowel | Sigmoid colon and ileum fistulization |
| Dash [21] 2010 | 30 | II P | CS | Abdominal pain | 9 years | USG * | 18 × 15 cm2 mass arising from the anterior and right part of the uterus | Yes | No |
| Patil [22] 2010 | 23 | I P | CS | Colicky pain in left iliac fossa, vomiting | 3 months | X-ray *, CT * | Mass in the lower abdomen | Proximal enterotomy to extrude the mop | No |
| Govarjin [23] 2010 | 35 | II G, II P | CS | Anorexia, partial bowel obstruction | 5 months | X-ray ** | Retained gauze migration in the terminal ileum | Enterolysis, terminal ileotomy, right hemicolectomy with ileocolic anastomoses, and removal of the fistula tract | Periumbilical fistula |
| Mavrigiannaki [24] 2011 | 20 | I P | CS | N/A | N/A | N/A | N/A | N/A | N/A |
| Kawamura [25] 2012 | 41 | I P | CS | Abdominal pain | 1 year | CT ** MRI ** | 5.5 cm diameter pelvic mass | Yes | No |
| Quraishi [26] 2012 | 24 | N/A | CS | Fever, abdominal pain, vomiting | 1 month | USG **, X-ray **, CT * | Retained surgical sponge in the lower abdomen | Ileal perforations followed by anastomosis | Ileal perforations |
| Karasaki [27] 2013 | 33 | I P | CS | Epigastric pain, fever | 6 weeks | USG *, CT * | 10 cm diameter mass in the left upper quadrant | Partial resection of the descending colon, small intestine | Descending colon fistula |
| Rafie [28] 2013 | 29 | I P | CS | Colicky abdominal pain and distension, nausea, vomiting, constipation | 9 months | X-ray ** | Jejunal transluminal migration of the sponge | Enterotomy and removal of the mass, resection, and anastomosis | No |
| Usta [29] 2013 | 30 | N/A | Emergency CS | Sepsis, abdominal mass, disseminated tenderness, defense, and rebound | 4 months | Clinical *, USG *, X-ray *, CECT * | 10 cm diameter wide mass lesion image was seen retrovesically | Wound debridements of the abscess with uterine dehiscence and necrosis of the edges, ileal resection, and an end-to-end anastomosis | Uterine wound dehiscence and ileal injury |
| Kashima [30] 2014 | 35 | II P | CS | Miction pain | 11 years | Cystoscopy * | Remnant gauze migration in the bladder (a calcified mass) | Transurethral operation | No |
| Rehman [31] 2014 | 40 | N/A | CS | Nausea, loss of appetite, and lower abdominal discomfort | 15 years | USG **, EGDS **, colonoscopy **, CT * | Mass in the lower left abdomen | Laparoscopy | No |
| Srivastava [32] 2014 | 38 | N/A | CS | Pain and a chronic lump in the right iliac fossa | 4 years | USG **, CECT **, MRI ** | 20 × 15 cm2 mass in the right iliac fossa | Resection of the mass along with an area of the terminal ileum | Fistula and intestinal obstruction |
| Faghani [33] 2014 | 35 | N/A | CS | Colicky abdominal pain, vomiting, and constipation | 2 years | USG **, X-ray ** | One sponge in the omentum and the other one in an enterocolic fistula in the distal ileum | Omentectomy and end-to-end anastomosis after resection of the fistulized segment (ileum, right colon) | Enterocolic fistula |
| Lee [34] 2015 | 38 | I P | CS | Lower quadrant pain | 24 years | X-ray **, CECT * | 9 cm diameter mass in the right lower quadrant | Laparoscopy with bladder repair | Bladder injury |
| Rafat [35] 2015 | 22 | I P | CS | Discomfort, heaviness in the lower abdomen | 2 years | Clinical *, USG * | 6 × 7 cm2 well-encapsulated mass in the pelvic cavity | Yes | No |
| Chopra [1] 2015 | N/A | N/A | Emergency CS | Abdominal wound discharge | 3 weeks | Clinical * | Abdominal wound | No | |
| Chopra [1] 2015 | N/A | N/A | Emergency CS | Adnexal mass | 1 year | USG * | Yes | No | |
| Chopra [1] 2015 | N/A | N/A | Peripartum HT | Puerperal sepsis | 2 weeks | USG **, CECT * | A mass in the right flank | Yes | No |
| Chopra [1] 2015 | N/A | N/A | Peripartum HT—scar rupture | Sepsis, abdominal mass | 8 months | CECT * | Buried in the lumen of the intestinal loop | Excision of the fistulous tract and end-to-end anastomosis | Gut perforation |
| Rabie [36] 2016 | 39 | I P | Elective cesarean HT—placenta increta | Abdominal pain, constipation, vomiting | 18 days | USG *, X-ray **, CT * | 10 × 10 cm2 mass in the right upper quadrant | Yes | No |
| Rabie [36] 2016 | 46 | II P | Cesarean HT | Abdominal pain | 9 years | USG *, CT * | 13 × 18 cm2 pelvic mass | Colonic resection | N/A |
| Rabie [36] 2016 | 35 | I P | CS | Abdominal pain, nausea, fever, vomiting | 2 months | X-ray **, CT * | Mass in the left lower quadrant | Yes | No |
| Margonis [37] 2016 | 36 | N/A | CS | Abdominal pain, nausea, vomiting | 6 months | USG **, X-ray **, CT ** | The 20 × 25 cm2 sponge in the lumen of the small intestine. | Bowel resection en bloc with the affected sigmoid and a loop sigmoidostomy | Intestinal obstruction and ileocolic fistula |
| Susmallian [38] 2016 | 34 | I P | CS | Abdominal pain, fever | 9 years | CT * | Intraabdominal and pelvic mass | Yes | No |
| Kostandinidis [39] 2017 | 68 | N/A | CS | Acute urinary retention | 29 years | USG **, CT ** | 12 cm diameter mass at the left side of the pelvis | Yes | No |
| Oran [40] 2018 | 36 | II P | CS | Painful mass in the left lower quadrant | 15 years | USG **, CT * | 11 × 9 × 7 cm3 mass on the left lower abdomen near the ovary | Yes | No |
| Kondo [41] 2018 | 42 | II P | CS | Lower abdominal bloating | 9 years | X-ray **, CT * | Two smooth masses partially adherent to the omentum and colon | Yes | No |
| Gavrić [7] 2018 | 45 | II P | CS and laparotomies for retained needle | Recurrent pelvic pain | 11 years | USG * | Structure with mixed echogenicity laterouterine right with a diameter of 4.9 cm | Total abdominal HT, bilateral salpingo-oophorectomy, remove gauze from the right obturator fossa | No |
| Fatima [42] 2019 | 30 | I P | CS | Abdominal pain | 3 months | USG *, CT * | 7.2 × 4.5 cm2 mass in the right upper and left lower quadrant | Right hemicolectomy was done with double-barrel ileostomy | Deceased |
| Bilali [43] 2019 | 42 | I P | CS | Abdominal mass | 2 years | USG *, MRI * | Mass in the right quadrant | Laparoscopy | No |
| Mejri [44] 2020 | 29 | I P | CS | Abdominal pain, fever | 5 months | MRI * | Two collections located in the right and left iliac fossa | Sigmoidectomy with a Hartmann procedure and ileostomy | Sigmoid colon and small bowel perforation |
| Alemu [45] 2020 | 32 | II P | CS | Lower abdominal pain, vomiting, nausea, transit stopped for gas and feces. | 4 months | X-ray **, USG **, CECT ** | In the lower left quadrant complex mass of 6 × 2.6 cm2 with central shadowing gas bubbles | The 10 × 8 cm2 surgical sponge came out through the rectum | Jejunal perforation on the antimesenteric border |
| Sankpal [46] 2020 | 40 | I P | CS | Incidentaloma | 5 years | N/A | 15 × 10 cm2 mass in the gastrocolic omentum | Yes | No |
| Omar [47] 2020 | 40 | I P | CS | Abdominal pain, diarrhea, bilious vomiting | 4 months | USG **, CT ** | Retained surgical sponge in the pelvic cavity | Resection of the involved parts of the ileum and the sigmoid colon with end–end anastomosis | Transmural erosion and ulceration of the sigmoid colon |
| El Zemity [48] 2020 | 26 | I P | Elective CS | Abdominal pain, fever | 18 months | Clinical *, CT * | 15 × 14 × 12 cm3 intra-abdominal mass in the umbilical region | Yes | No |
| Amodeo [49] 2021 | 35 | I P | CS | Pelvic pain | 2 years | USG ** | Surgical gauze in the uterine isthmus at the c-section scar site | Hysteroscopy | No |
| Jha [50] 2021 | 28 | IP | CS | Abdominal pain, fecal discharge | 4 months | Clinical *, USG *, MRI * | Multiple loculated abscesses, a mass of 15 × 10 cm2 in the left parauterine space | Colouterine fistula resection with end sigmoid colostomy | Colouterine fistula |
| Bairwa [51] 2021 | 30 | N/A | CS | Abdominal pain | 2 weeks | CECT * | 6.2 × 6.1 cm2 well-defined mass in the left lumbar region | Yes | No |
| Bai [8] 2021 | 29 | N/A | CS | Intermittent abdominal pain, distension, constipation | 4 months | CECT *, MRI * | N/A | Enteroenterostomy | Intestinal ulcer and perforation |
| Bai [8] 2021 | 38 | N/A | CS | Intermittent abdominal pain, discomfort | 18 months | Clinical *, MRI * | Soft mass about 5.5 × 4.4 cm2 in size in the left middle-lower abdomen | Yes | No |
| Bai [8] 2021 | 30 | N/A | CS | Intermittent abdominal pain, abdominal mass | 5 years | MRI * | Mass in the right middle and lower abdominal cavity 13.1 × 9.7 cm2 | Yes | No |
| Munihire [52] 2022 | 31 | I P | CS | Abdominal and pelvic pain, fever | 22 days | USG * | 7 cm diameter mesenteric mass | Yes | No |
| Ammar [53] 2021 | 36 | III P | CS | Abdominal pain, vomiting | 3 years | X-ray ** | Retained sponge in the center of the abdomen | Resection and end-to-end anastomosis | Ileum perforation |
| Khanduri [54] 2022 | 38 | I P | CS | Left iliac fossa pain, fever | 1 month | USG *, CECT * | 12 × 11 × 9 cm3 mass in left iliac fossa | Laparoscopy | No |
| Elci [55] 2021 | 29 | II G, I P | Emergency CS | N/A | 2 months | USG * | 6.5 × 1.5 × 1 cm3 mass under the skin incision | Excision of the infected tissue | No |
| Min [56] 2022 | 54 | II P | Emergency CS | Abdominal mass | 19 years | USG **, CT * | 10.4 cm pelvic mass, partially penetrated the right ovary | Yes | No |
| Our case 2021 | 28 | I G, I P | Emergency CS supra-cervical HT—hematoma | Adnexal mass and subhepatic mass | 16 months | USG *, MRI ** | 9.6 × 5.4 cm2 left flank mass, 8.5 × 4.9 cm2 right hypochondrium mass. | Yes | No |
| Imagistic Findings | Diagnosis | Misdiagnosis |
|---|---|---|
| USG | 18 (60%) | 12 (40%) |
| X-ray | 4 (25%) | 12 (75%) |
| CT/CECT | 27 (81.8%) | 6 (18.2%) |
| MRI | 6 (66.67%) | 3 (33.33%) |
| Complications | N | References |
|---|---|---|
| Fistula | ||
| Ileocolic | 3 | [20,33,37] |
| Jejunocolic | 2 | [10,19] |
| Ileoileal | 2 | [14,32] |
| Descending colon | 1 | [27] |
| Jejunovaginal | 1 | [13] |
| Colouterine | 1 | [50] |
| Periumbilical | 1 | [23] |
| Obstruction | ||
| Intestinal | 3 | [11,32,37] |
| Perforations | ||
| Ileal | 5 | [1,26,29,51,53] |
| Jejunal | 1 | [45] |
| Sigmoid colon | 1 | [44] |
| Bladder injury | 1 | [34] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varlas, V.N.; Bors, R.G.; Mastalier, B.; Balescu, I.; Bacalbasa, N.; Cirstoiu, M.-M. Gossypiboma, the Hidden Enemy of an Emergency Cesarean Hysterectomy—Case Report and Review of the Literature. J. Clin. Med. 2023, 12, 5353. https://doi.org/10.3390/jcm12165353
Varlas VN, Bors RG, Mastalier B, Balescu I, Bacalbasa N, Cirstoiu M-M. Gossypiboma, the Hidden Enemy of an Emergency Cesarean Hysterectomy—Case Report and Review of the Literature. Journal of Clinical Medicine. 2023; 12(16):5353. https://doi.org/10.3390/jcm12165353
Chicago/Turabian StyleVarlas, Valentin Nicolae, Roxana Georgiana Bors, Bogdan Mastalier, Irina Balescu, Nicolae Bacalbasa, and Monica-Mihaela Cirstoiu. 2023. "Gossypiboma, the Hidden Enemy of an Emergency Cesarean Hysterectomy—Case Report and Review of the Literature" Journal of Clinical Medicine 12, no. 16: 5353. https://doi.org/10.3390/jcm12165353