

Calcification Propensity (T50) Predicts a Rapid Decline of Renal Function in Kidney Transplant Recipients
 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Statistical Analysis
2.2. Outcomes
3. Results
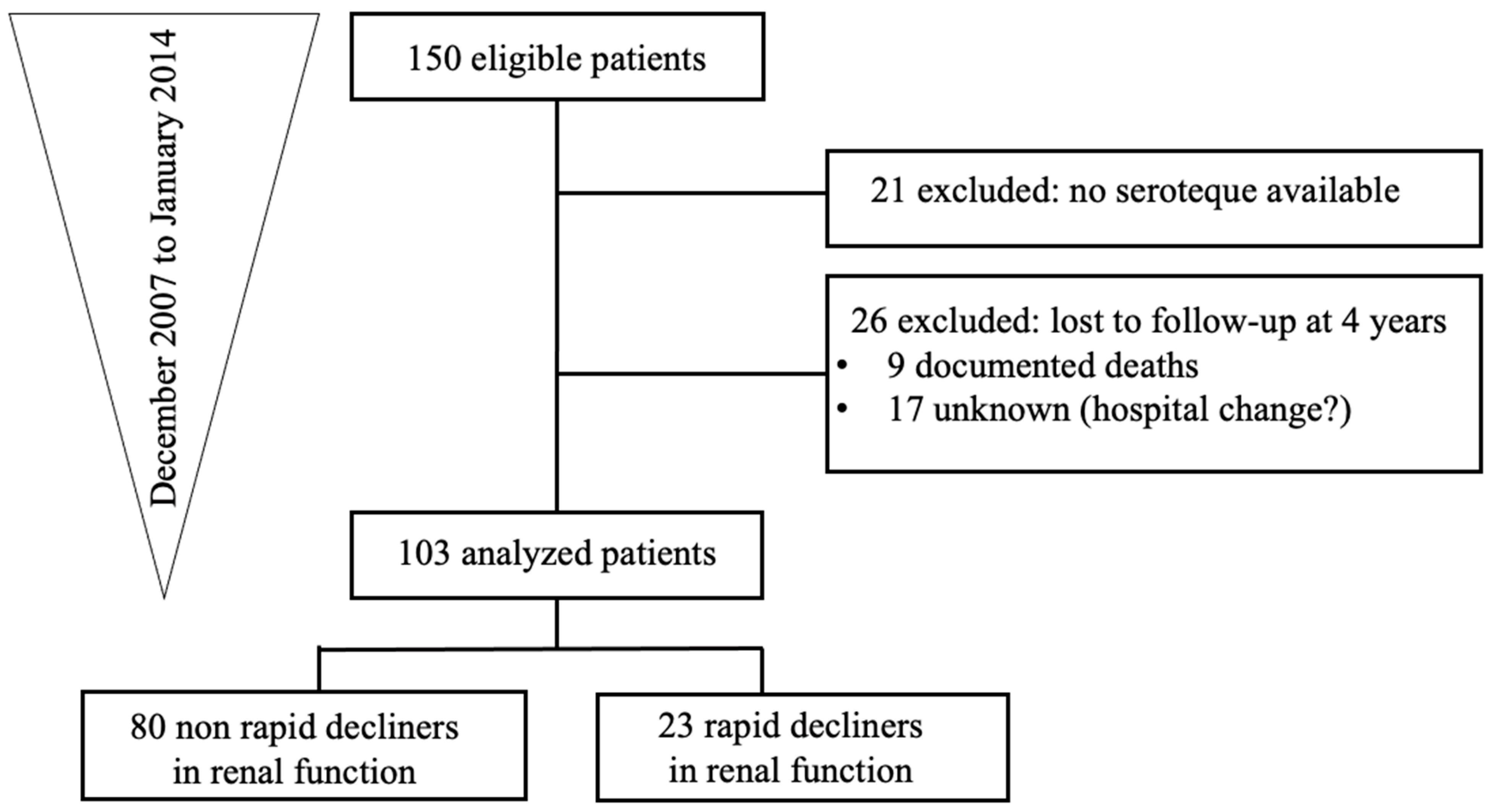
3.1. Characteristics of the Study Population
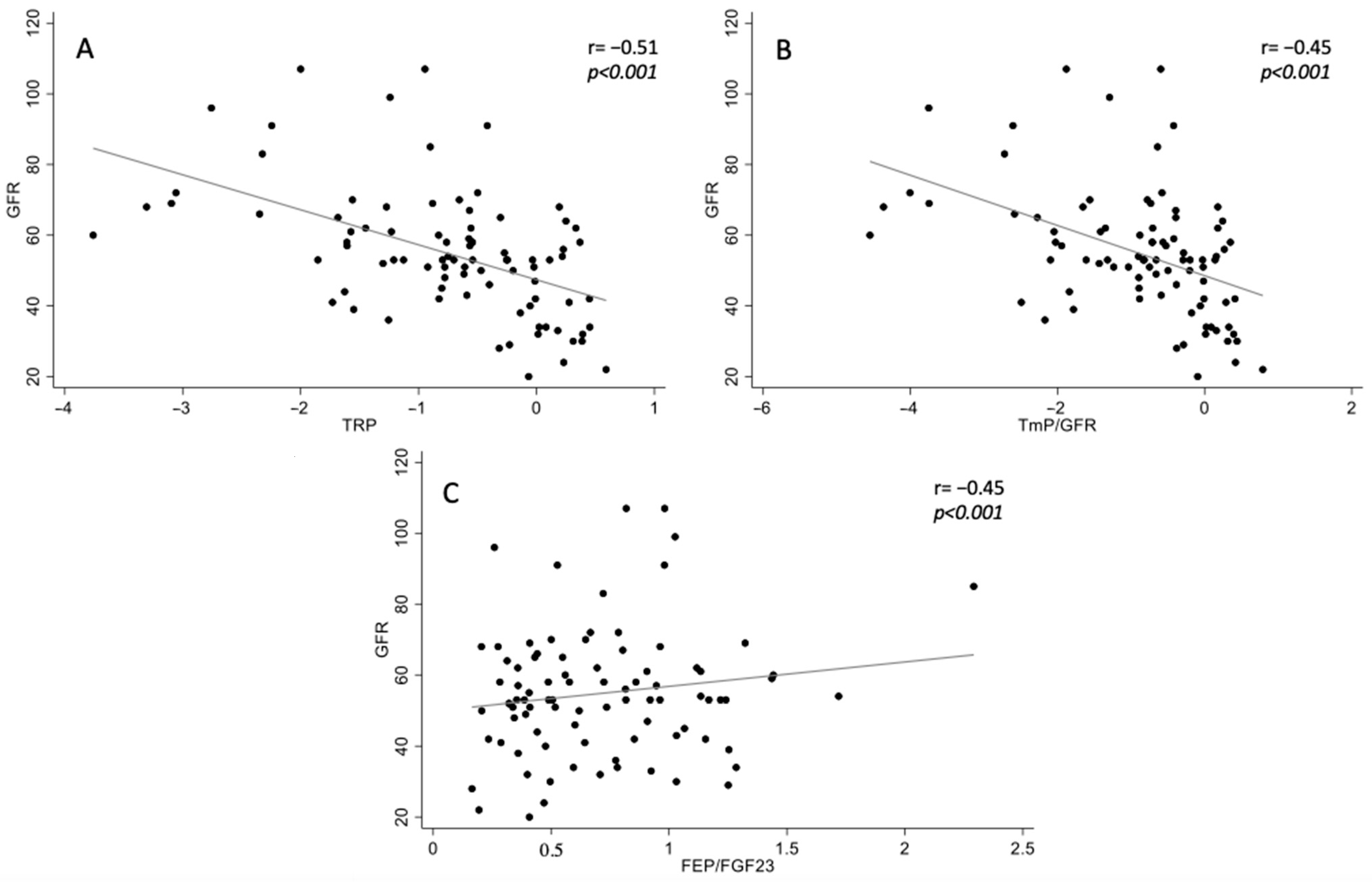
3.2. Association between Phosphocalcic Biomarkers and Renal Function at Baseline
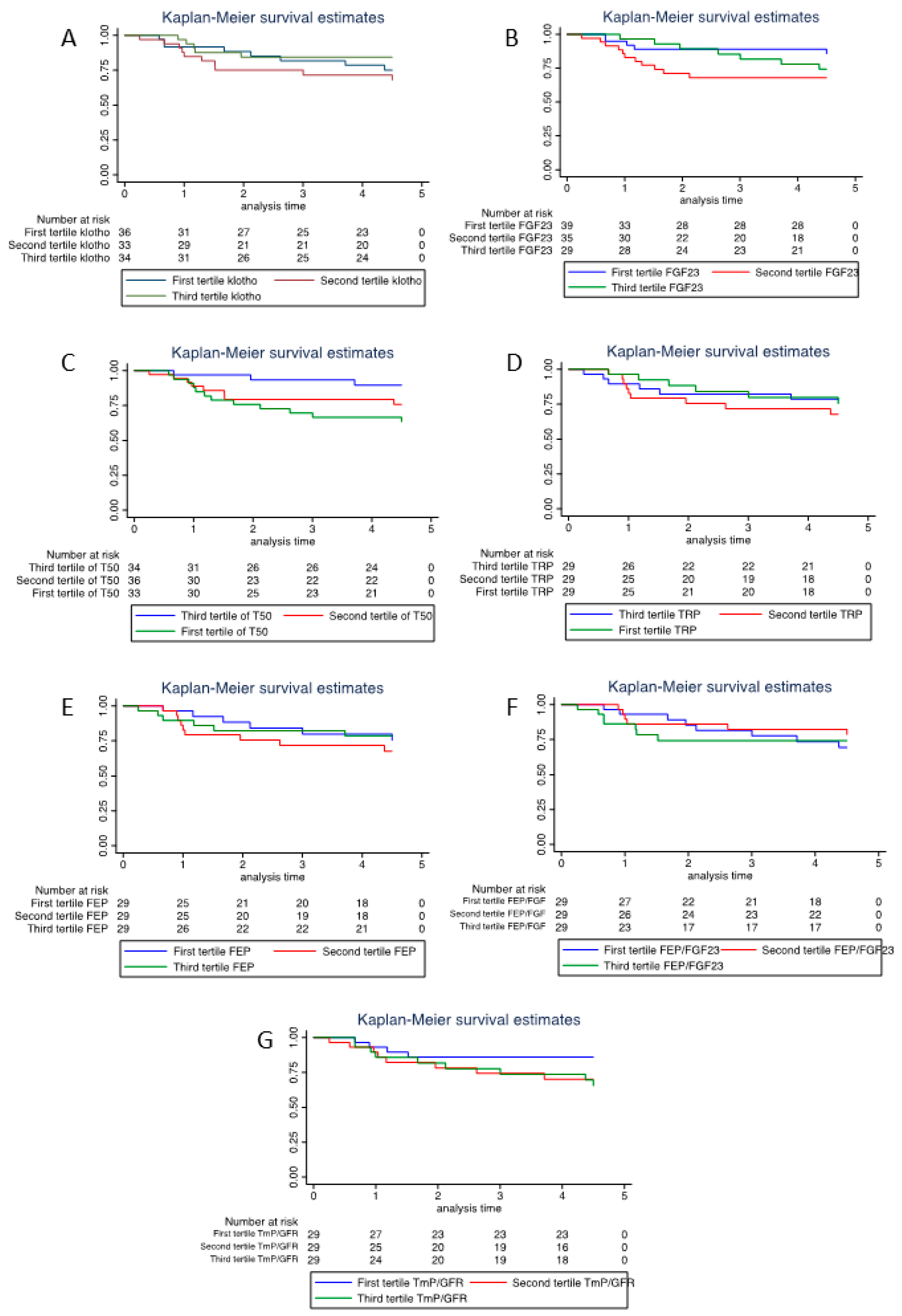
3.3. Univariable and Multivariable Analysis of Predictors of Renal Function Decline
3.4. Multivariable Analysis of Predictors of Renal Function Decline
4. Discussion
5. Conclusions
6. Three Statements
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith-Palmer, J.; Kalsekar, A.; Valentine, W. Influence of renal function on long-term graft survival and patient survival in renal transplant recipients. Curr. Med. Res. Opin. 2014, 30, 235–242. [Google Scholar] [CrossRef]
- Stratta, R.J.; Rohr, M.S.; Sundberg, A.K.; Farney, A.C.; Hartmann, E.L.; Moore, P.S.; Rogers, J.; Iskandar, S.S.; Gautreaux, M.D.; Kiger, D.F.; et al. Intermediate-term outcomes with expanded criteria deceased donors in kidney transplantation: A spectrum or specter of quality? Ann. Surg. 2006, 243, 594–601. [Google Scholar] [CrossRef]
- Sarier, M.; Demir, M.; Goktas, S.; Duman, I.; Buyukkinaci, M.; Yuksel, Y.; Tekin, S.; Yavuz, A.; Sengul, A. Results of Real-time Multiplex Polymerase Chain Reaction Assay in Renal Transplant Recipients With Sterile Pyuria. Transpl. Proc. 2017, 49, 1307–1311. [Google Scholar] [CrossRef]
- Berchtold, L.; Ponte, B.; Moll, S.; Hadaya, K.; Seyde, O.; Bachtler, M.; Vallée, J.-P.; Martin, P.-Y.; Pasch, A.; de Seigneux, S. Phosphocalcic markers and calcification propensity for assessment of interstitial fibrosis and vascular lesions in kidney allograft recipients. PLoS ONE 2016, 11, e0167929. [Google Scholar] [CrossRef] [Green Version]
- Kuro-o, M.; Matsumura, Y.; Arawa, H.; Kawaguchi, H.; Suga, T.; Utsugi, T.; Ohyama, Y.; Kurabayashi, M.; Kaname, T.; Kume, E.; et al. Mutation of the mouse klotho gene leads to a syndrome resembling ageing. Chemtracts 1999, 12, 703–707. [Google Scholar] [CrossRef]
- Hu, M.C.; Kuro-o, M.; Moe, O.W. Renal and Extrarenal Actions of Klotho. Semin. Nephrol. 2013, 33, 118–129. [Google Scholar] [CrossRef] [Green Version]
- Semba, R.D.; Cappola, A.R.; Sun, K.; Bandinelli, S.; Dalal, M.; Bs, C.C.; Guralnik, J.M.; Ferrucci, L. Plasma klotho and cardiovascular disease in adults. J. Am. Geriatr. Soc. 2011, 59, 1596–1601. [Google Scholar] [CrossRef] [Green Version]
- Kitagawa, M.; Sugiyama, H.; Morinaga, H.; Inoue, T.; Takiue, K.; Ogawa, A.; Yamanari, T.; Kikumoto, Y.; Uchida, H.A.; Kitamura, S.; et al. A Decreased Level of Serum Soluble Klotho Is an Independent Biomarker Associated with Arterial Stiffness in Patients with Chronic Kidney Disease. PLoS ONE 2013, 8, e56695. [Google Scholar] [CrossRef] [Green Version]
- Hu, M.C.; Shi, M.; Zhang, J.; Quiñones, H.; Griffith, C.; Kuro-O, M.; Moe, O.W. Klotho deficiency causes vascular calcification in chronic kidney disease. J. Am. Soc. Nephrol. 2011, 22, 124–136. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.F.; Yu, L.X.; Feng, J.H.; Sun, Q.; Li, S.S.; Ye, J.M. The prognostic role of Klotho in patients with chronic kidney disease: A Systematic Review and Meta-analysis. Dis. Markers 2019, 2019, 6468729. [Google Scholar] [CrossRef] [Green Version]
- Castellano, G.; Intini, A.; Stasi, A.; Divella, C.; Gigante, M.; Pontrelli, P.; Franzin, R.; Accetturo, M.; Zito, A.; Fiorentino, M.; et al. Complement modulation of anti-aging factor klotho in ischemia/reperfusion injury and delayed graft function. Am. J. Transplant. 2016, 16, 325–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, M.C.; Moe, O.W. Klotho as a potential biomarker and therapy for acute kidney injury. Nat. Rev. Nephrol. 2012, 8, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Fliser, D.; Kollerits, B.; Neyer, U.; Ankerst, D.P.; Lhotta, K.; Lingenhel, A.; Ritz, E.; Kronenberg, F. Fibroblast Growth Factor 23 (FGF23) predicts progression of chronic kidney disease: The Mild to Moderate Kidney Disease (MMKD) study. J. Am. Soc. Nephrol. 2007, 18, 2601–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Seigneux, S.; Courbebaisse, M.; Rutkowski, J.M.; Wilhelm-Bals, A.; Metzger, M.; Khodo, S.N.; Hasler, U.; Chehade, H.; Dizin, E.; Daryadel, A.; et al. Proteinuria increases plasma phosphate by altering its tubular handling. J. Am. Soc. Nephrol. 2015, 26, 1608–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Y.A.; Lim, J.H.; Kim, M.Y.; Kim, Y.; Yang, K.S.; Chung, B.H.; Chung, S.; Choi, B.S.; Yang, C.W.; Kim, Y.-S.; et al. Assessment of tubular reabsorption of phosphate as a surrogate marker for phosphate regulation in chronic kidney disease. Clin. Exp. Nephrol. 2015, 19, 208–215. [Google Scholar] [CrossRef]
- Bellasi, A.; Di Micco, L.; Russo, D.; De Simone, E.; Di Iorio, M.; Vigilante, R.; Di Lullo, L.; Di Iorio, B.R. Fractional Excretion of Phosphate (FeP) Is Associated with End-Stage Renal Disease Patients with CKD 3b and 5. J. Clin. Med. 2019, 8, 1026. [Google Scholar] [CrossRef] [Green Version]
- Yamada, H.; Kuro-O, M.; Hara, K.; Ueda, Y.; Kusaka, I.; Kakei, M.; Ishikawa, S.-E. The urinary phosphate to serum fibroblast growth factor 23 ratio is a useful marker of atherosclerosis in early-stage chronic kidney disease. PLoS ONE 2016, 11, e0160782. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Park, J.; Nam, K.H.; Jhee, J.H.; Yun, H.-R.; Park, J.T.; Han, S.H.; Chung, W.; Oh, K.-H.; Park, S.K.; et al. The effect of interactions between proteinuria, activity of fibroblast growth factor 23 and serum phosphate on renal progression in patients with chronic kidney disease: A result from the Korean cohort study for Outcome in patients with Chronic Kidney Disease study. Nephrol. Dial. Transplant. 2020, 35, 438–446. [Google Scholar]
- Craver, L.; Dusso, A.; Martinez-Alonso, M.; Sarro, F.; Valdivielso, J.M.; Fernández, E. A low fractional excretion of Phosphate/Fgf23 ratio is associated with severe abdominal Aortic calcification in stage 3 and 4 kidney disease patients. BMC Nephrol. 2013, 14, 221. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez, O.M.; Januzzi, J.L.; Isakova, T.; Laliberte, K.; Smith, K.; Collerone, G.; Sarwar, A.; Hoffmann, U.; Coglianese, E.; Christenson, R.; et al. Fibroblast growth factor 23 and left ventricular hypertrophy in chronic kidney disease. Circulation 2009, 119, 2545–2552. [Google Scholar] [CrossRef] [Green Version]
- Bleskestad, I.H.; Thorsen, I.S.; Jonsson, G.; Skadberg, Ø.; Bergrem, H.; Gøransson, L.G. Soluble Klotho and intact fibroblast growth factor 23 in long-term kidney transplant patients. Eur. J. Endocrinol. 2015, 172, 343–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, M.; Molnar, M.Z.; Amaral, A.P.; Czira, M.E.; Rudas, A.; Ujszaszi, A.; Kiss, I.; Rosivall, L.; Kosa, J.; Lakatos, P.; et al. Elevated fibroblast growth factor 23 is a risk factor for kidney transplant loss and mortality. J. Am. Soc. Nephrol. 2011, 22, 956–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baia, L.C.; Heilberg, I.P.; Navis, G.; De Borst, M.H. Phosphate and FGF-23 homeostasis after kidney transplantation. Nat. Rev. Nephrol. 2015, 11, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.; Elitok, S.; Zeng, S.; Xiong, Y.; Hocher, C.-F.; Hasan, A.A.; Krämer, B.K.; Hocher, B. C-terminal and intact FGF23 in kidney transplant recipients and their associations with overall graft survival. BMC Nephrol. 2021, 22, 125. [Google Scholar] [CrossRef] [PubMed]
- Maréchal, C.; Coche, E.; Goffin, E.; Dragean, A.; Schlieper, G.; Nguyen, P.; Floege, J.; Kanaan, N.; Devuyst, O.; Jadoul, M. Progression of Coronary Artery Calcification and Thoracic Aorta Calcification in Kidney Transplant Recipients. Am. J. Kidney Dis. 2012, 59, 258–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández, D.; Rufino, M.; Bartolomei, S.; González-Rinne, A.; Lorenzo, V.; Cobo, M.; Torres, A. Clinical impact of preexisting vascular calcifications on mortality after renal transplantation. Kidney Int. 2005, 67, 2015–2020. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.T.; Henrard, S.; Coche, E.; Goffin, E.; Devuyst, O.; Jadoul, M. Coronary artery calcification: A strong predictor of cardiovascular events in renal transplant recipients. Nephrol. Dial. Transpl. 2010, 25, 3773–3778. [Google Scholar] [CrossRef] [Green Version]
- Pasch, A.; Farese, S.; Gräber, S.; Wald, J.; Richtering, W.; Floege, J.; Jahnen-Dechent, W. Nanoparticle-based test measures overall propensity for calcification in serum. J. Am. Soc. Nephrol. 2012, 23, 1744–1752. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.R.; Ford, M.L.; Tomlinson, L.A.; Bodenham, E.; McMahon, L.P.; Farese, S.; Rajkumar, C.; Holt, S.G.; Pasch, A. Serum calcification propensity predicts all-cause mortality in predialysis CKD. J. Am. Soc. Nephrol. 2014, 25, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Dahle, D.O.; Åsberg, A.; Hartmann, A.; Holdaas, H.; Bachtler, M.; Jenssen, T.G.; Dionisi, M.; Pasch, A. Serum calcification propensity is a strong and independent determinant of cardiac and all-cause mortality in kidney transplant recipients. Am. J. Transplant. 2016, 16, 204–212. [Google Scholar] [CrossRef]
- Keyzer, C.A.; de Borst, M.H.; Berg, E.V.D.; Jahnen-Dechent, W.; Arampatzis, S.; Farese, S.; Bergmann, I.P.; Floege, J.; Navis, G.; Bakker, S.J.; et al. Calcification Propensity and Survival among Renal Transplant Recipients. J. Am. Soc. Nephrol. 2016, 27, 239–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, J.E.; Crowe, S.E. Annals of internal medicine®. Ann. Intern. Med. 2020, 172, ITC1–ITC14. [Google Scholar] [CrossRef] [PubMed]
- Coresh, J.; Turin, T.; Matsushita, K.; Sang, Y.; Ballew, S.; Appel, L.J.; Arima, H.; Chadban, S.J.; Cirillo, M.; Djurdjev, O.; et al. Decline in Estimated Glomerular Filtration Rate and Subsequent Risk of End-Stage Renal Disease and Mortality. JAMA 2014, 311, 2518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Inker, L.A.; Matsushita, K.; Greene, T.; Willis, K.; Lewis, E.; de Zeeuw, D.; Cheung, A.K.; Coresh, J. GFR decline as an end point for clinical trials in CKD: A scientific workshop sponsored by the National Kidney Foundation and the US Food and Drug Administration. Am. J. Kidney Dis. 2014, 64, 821–835. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, K.; Chen, J.; Sang, Y.; Ballew, S.H.; Shimazaki, R.; Fukagawa, M.; Imai, E.; Coresh, J.; Hishida, A. Risk of end-stage renal disease in Japanese patients with chronic kidney disease increases proportionately to decline in estimated glomerular filtration rate. Kidney Int. 2016, 90, 1109–1114. [Google Scholar] [CrossRef]
- Heijboer, A.C.; Levitus, M.; Vervloet, M.G.; Lips, P.; ter Wee, P.M.; Dijstelbloem, H.M.; Blankenstein, M. Determination of fibroblast growth factor 23. Ann. Clin. Biochem. 2009, 46, 338–340. [Google Scholar] [CrossRef]
- Pedersen, L.; Pedersen, S.M.; Brasen, C.L.; Rasmussen, L.M. Soluble serum Klotho levels in healthy subjects. Comparison of two different immunoassays. Clin. Biochem. 2013, 46, 1079–1083. [Google Scholar] [CrossRef]
- Pasch, A.; Block, G.A.; Bachtler, M.; Smith, E.R.; Jahnen-Dechent, W.; Arampatzis, S.; Chertow, G.M.; Parfrey, P.; Ma, X.; Floege, J. Blood calcification propensity, cardiovascular events, and survival in patients receiving hemodialysis in the EVOLVE Trial. Clin. J. Am. Soc. Nephrol. 2017, 12, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Pruijm, M.; Lu, Y.; Megdiche, F.; Piskunowicz, M.; Milani, B.; Stuber, M.; Bachtler, M.; Vogt, B.; Burnier, M.; Pasch, A. Serum calcification propensity is associated with renal tissue oxygenation and resistive index in patients with arterial hypertension or chronic kidney disease. J. Hypertens. 2017, 35, 2044–2052. [Google Scholar] [CrossRef]
- Daveau, M.; Christian-Davrinche Julen, N.; Hiron, M.; Amaud, P.; Lebreton, J.-P. The synthesis of human α-2-HS glycoprotein is down-regulated by cytokines in hepatoma HepG2 cells. FEBS Lett. 1988, 241, 191–194. [Google Scholar] [CrossRef] [Green Version]
- Bostom, A.; Pasch, A.; Madsen, T.; Roberts, M.B.; Franceschini, N.; Steubl, D.; Garimella, P.S.; Ix, J.H.; Tuttle, K.R.; Ivanova, A.; et al. Serum Calcification Propensity and Fetuin-A: Biomarkers of Cardiovascular Disease in Kidney Transplant Recipients. Am. J. Nephrol. 2018, 48, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Ishida, H.; Nakamura, M.; Komaba, H.; Uehara, S.; Takiguchi, S.; Fukagawa, M. Post-kidney transplant soluble Klotho levels are determined by pretransplant soluble Klotho levels in both living donors and recipients. Clin. Exp. Nephrol. 2021, 25, 1367–1374. [Google Scholar] [CrossRef] [PubMed]
- Pazik, J.; Rembek, K.; Sadowska-Jakubowicz, A.; Sitarek, E.; Kosieradzki, M.; Durlik, M. Donor Klotho KL-VS Polymorphism Predicts Allograft Glomerulosclerosis and Early Post-Transplant Kidney Function. Transpl. Proc. 2020, 52, 2371–2375. [Google Scholar] [CrossRef] [PubMed]
- Baia, L.C.; Humalda, J.K.; Vervloet, M.G.; Navis, G.; Bakker, S.J.L.; de Borst, M.H. Fibroblast growth factor 23 and cardiovascular mortality after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2013, 8, 1968–1978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bienaimé, F.; Dechartres, A.; Anglicheau, D.; Sabbah, L.; Montgermont, P.; Friedlander, G.; Ravaud, P.; Legendre, C.; Prié, D. The Association Between Fibroblast Growth Factor 23 and Renal Transplantation Outcome Is Modified by Follow-up Duration and Glomerular Filtration Rate Assessment Method. Kidney Int. Rep. 2017, 2, 881–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 103) | eGFR Decline at 4 Years ≤ 30% (n = 80) | eGFR Decline at 4 Years > 30% (n = 23) | p Value | |
|---|---|---|---|---|
| Characteristics | - | |||
| Age, years | 56 ± 14 | 56 ± 14 | 57 ± 13 | 0.57 |
| Male, n (%) | 63 (61.2) | 48 (60) | 15 (65.2) | 0.65 |
| Caucasian, n (%) | 98 (95.2) | 76 (95) | 22 (95.7) | 0.89 |
| Clinical parameters | ||||
| Systolic blood pressure (mmHg) *a | 132 ± 16 | 132 ± 15 | 131 ± 20 | 0.76 |
| Diastolic blood pressure (mmHg) *a | 80 ± 12 | 80 ± 12 | 78 ± 12 | 0.44 |
| BMI (kg/m2) | 25.3 ± 4.3 | 25.4 ± 4.3 | 24.8 ± 4.4 | 0.57 |
| Dialysis before tx, n (%) *c | 40 (72.7) | 31 (73.8) | 9 (69.2) | 0.75 |
| Dialysis duration, mths, *c | 24.2 ± 29.4 | 24.45 ± 30.8 | 23.3 ± 25.6 | 0.90 |
| Donor age, years, *c | 53 ± 14 | 54 ± 14 | 54 ± 15 | 0.94 |
| Living donor transplant, n (%) | 40 (38.8) | 32 (40) | 8 (34.8) | 0.65 |
| Graft vintage (year) | 9.48 ± 7.3 | 9.45 ± 7.1 | 9.6 ± 8.2 | 0.94 |
| 2nd or 3rd transplant, n (%) | 14 (13.6) | 11 (13.8) | 3 (13) | 0.93 |
| Rejection episodes, n (%) | 46 (44.7) | 32 (40) | 14 (60.9) | 0.08 |
| Infections, n (%) | 52 (66.7) | 40 (66.7) | 12 (66.7) | 1 |
| Opportunistic inf, n (%) *c | 0.76 | |||
| None | 41 (51.3) | 30 (49.2) | 11 (57.9) | |
| 1 | 31 (38.8) | 25 (41) | 6 (31.6) | |
| 2 | 8 (10) | 6 (9.8) | 2 (10.5) | |
| NODAT, n (%) | 11 (10.7) | 9 (11.3) | 2 (8.7) | 0.73 |
| Etiology of kidney disease, n (%) | ||||
| Diabetes | 4 (3.9) | 3 (3.8) | 1 (4.4) | 0.89 |
| Hypertension | 20 (19.4) | 13 (16.3) | 7 (30.4) | 0.13 |
| Glomerulonephritis | 22 (21.4) | 18 (22.5) | 4 (17.4) | 0.6 |
| Polycystic kidney disease | 20 (19.4) | 15 (18.8) | 5 (21.7) | 0.75 |
| Others (tubulo-interstitial nephritis…) | 41 (39.8) | 34 (42.5) | 7 (30.4) | 0.3 |
| Treatment, n (%) | ||||
| CNI | 92 (89.3) | 77 (87.5) | 22 (95.7) | 0.27 |
| Mycophenolate mofetil | 80 (77.7) | 61 (76.3) | 19 (82.6) | 0.52 |
| Corticostéroids | 60 (58.3) | 43 (53.8) | 17 (73.9) | 0.08 |
| ACE-I/ARB | 54 (52.4) | 39 (48.8) | 15 (65.2) | 0.16 |
| Calcium channel blockers | 50 (48.5) | 37 (46.3) | 13 (56.5) | 0.39 |
| Diuretics | 7 (6.8) | 4 (5) | 3 (13) | 0.18 |
| Beta-blockers | 56 (54.4) | 44 (55) | 12 (52.2) | 0.81 |
| Calcium | 69 (67) | 54 (67.5) | 15 (65.2) | 0.84 |
| Vitamine D | 88 (85.4) | 68 (85) | 20 (87) | 0.82 |
| Laboratory | ||||
| eGFR at baseline (mL/min/1.73 m2) | 55.6 ± 18.6 | 56 ± 18.4 | 54.4 ± 19.9 | 0.72 |
| eGFR at 4 years (mL/min/1.73 m2) | 48.3 ± 19.7 | 53.9 ± 16.9 | 28.8 ± 16.1 | <0.001 |
| Proteinuria (g/d) *b | 0.4 ± 1.4 | 0.4 ± 1.6 | 0.2 ± 0.2 | 0.5 |
| Alb/Creat ratio (mg/d) *b | 148.8 ± 283 | 116.5 ± 272.1 | 255.6 ± 298 | 0.04 |
| Hemoglobine (g/L) | 129 ± 14 | 129.8 ± 13.4 | 126.4 ± 15.9 | 0.31 |
| Calcium (mmol/L) | 2.41 ± 0.14 | 2.41 ± 0.13 | 2.42 ± 0.17 | 0.9 |
| Phosphate (mmol/L) | 1.09 ± 0.23 | 1.07 ± 0.2 | 1.13 ± 0.32 | 0.32 |
| Vitamine D (nmol/L) *a | 68.6 ± 21.6 | 68.7 ± 21.6 | 68.3 ± 22.1 | 0.94 |
| Parathormone (pmol/L) *a | 9.14 ± 4.6 | 8.8 ± 4.1 | 10.1 ± 6.1 | 0.25 |
| Bicarbonate (mmol/L) *a | 24.3 ± 3.4 | 24.3 ± 3.6 | 24.3 ±2.6 | 0.99 |
| Albumin (g/L) | 37.4 ± 3.6 | 37.7 ± 3.6 | 36.5 ± 3.4 | 0.18 |
| FEP/FGF23 § ratio *b | 0.72 ± 0.39 | 0.73 ± 0.4 | 0.7 ± 0.4 | 0.77 |
| FEP (%) | 26.2 ± 11.1 | 25.9 ± 10.3 | 27.1 ± 13.5 | 0.68 |
| FGF23 (pg/mL) | 43.6 ± 28.7 | 43.2 ± 29.7 | 45.2 ± 25.5 | 0.77 |
| TRP ‡,*b | 0.98 ± 0.01 | 0.98 ± 0 | 0.98 ± 0.01 | 0.68 |
| TmP/GFR ¶ (mmol/L) *b | 1.48 ± 0.3 | 1.45 ± 0.3 | 1.58 ± 0.5 | 0.12 |
| Klotho (pg/mL) | 734.9 ± 244.2 | 751.6 ±264 | 676.6 ± 147.4 | 0.2 |
| T50 (min) | 285.2 ± 56.7 | 291.9 ± 55.9 | 262 ± 54.6 | 0.03 |
| HR | 95% CI | p Value | |
|---|---|---|---|
| Tertile Klotho | |||
| First tertile | Reference | ||
| Second tertile | 1.41 | 0.56–3.58 | 0.47 |
| Third tertile | 0.63 | 0.21–1.92 | 0.42 |
| Tertile FGF23 | |||
| First tertile | Reference | ||
| Second tertile | 2.65 | 0.92–7.64 | 0.07 |
| Third tertile | 1.72 | 0.55–5.42 | 0.35 |
| Tertile FEP | |||
| First tertile | Reference | ||
| Second tertile | 1.52 | 0.54–4.28 | 0.43 |
| Third tertile | 0.97 | 0.31–3.02 | 0.96 |
| Tertile FEP/FGF23 | |||
| First tertile | Reference | ||
| Second tertile | 0.72 | 0.25–2.08 | 0.54 |
| Third tertile | 1.01 | 0.37–2.8 | 0.98 |
| Tertile T50 | |||
| Third tertile | Reference | ||
| Second tertile | 2.78 | 0.74–10.48 | 0.13 |
| First tertile | 4.26 | 1.2–15.09 | 0.025 |
| Tertile TRP | |||
| First tertile | Reference | ||
| Second tertile | 1.56 | 0.56–4.4 | 0.4 |
| Third tertile | 1.03 | 0.33–3.19 | 0.96 |
| Tertile TmP/GFR | |||
| Third tertile | Reference | ||
| Second tertile | 2.29 | 0.69–7.62 | 0.18 |
| First tertile | 2.53 | 0.78–8.22 | 0.12 |
| HR | 95% CI | p Value | |
|---|---|---|---|
| eGFR | |||
| ≥45 & <60 mL/min/1.73 m2 | 0.27 | 0.05–1.51 | 0.14 |
| <45 & ≥30 mL/min /1.73 m2 | 0.28 | 0.06–1.33 | 0.11 |
| <30 mL/min/1.73 m2 | 0.1 | 0.01–0.97 | 0.047 |
| Albuminuria | |||
| 30–300 mg/24 h | 1.89 | 0.65–5.48 | 0.24 |
| >300 mg/24 h | 4.47 | 1.39–14.52 | 0.012 |
| Tertile T50 | |||
| Second tertile | 2.5 | 0.62–10.01 | 0.2 |
| First tertile | 3.86 | 1.01–14.7 | 0.048 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hammer, N.; Legouis, D.; Pasch, A.; Huber, A.; Al-Qusairi, L.; Martin, P.-Y.; de Seigneux, S.; Berchtold, L. Calcification Propensity (T50) Predicts a Rapid Decline of Renal Function in Kidney Transplant Recipients. J. Clin. Med. 2023, 12, 3965. https://doi.org/10.3390/jcm12123965
Hammer N, Legouis D, Pasch A, Huber A, Al-Qusairi L, Martin P-Y, de Seigneux S, Berchtold L. Calcification Propensity (T50) Predicts a Rapid Decline of Renal Function in Kidney Transplant Recipients. Journal of Clinical Medicine. 2023; 12(12):3965. https://doi.org/10.3390/jcm12123965
Chicago/Turabian StyleHammer, Nathalie, David Legouis, Andreas Pasch, Aurélie Huber, Lama Al-Qusairi, Pierre-Yves Martin, Sophie de Seigneux, and Lena Berchtold. 2023. "Calcification Propensity (T50) Predicts a Rapid Decline of Renal Function in Kidney Transplant Recipients" Journal of Clinical Medicine 12, no. 12: 3965. https://doi.org/10.3390/jcm12123965