
Pathways between Risk/Protective Factors and Maternal Postnatal Depressive Symptoms: The ELFE Cohort
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
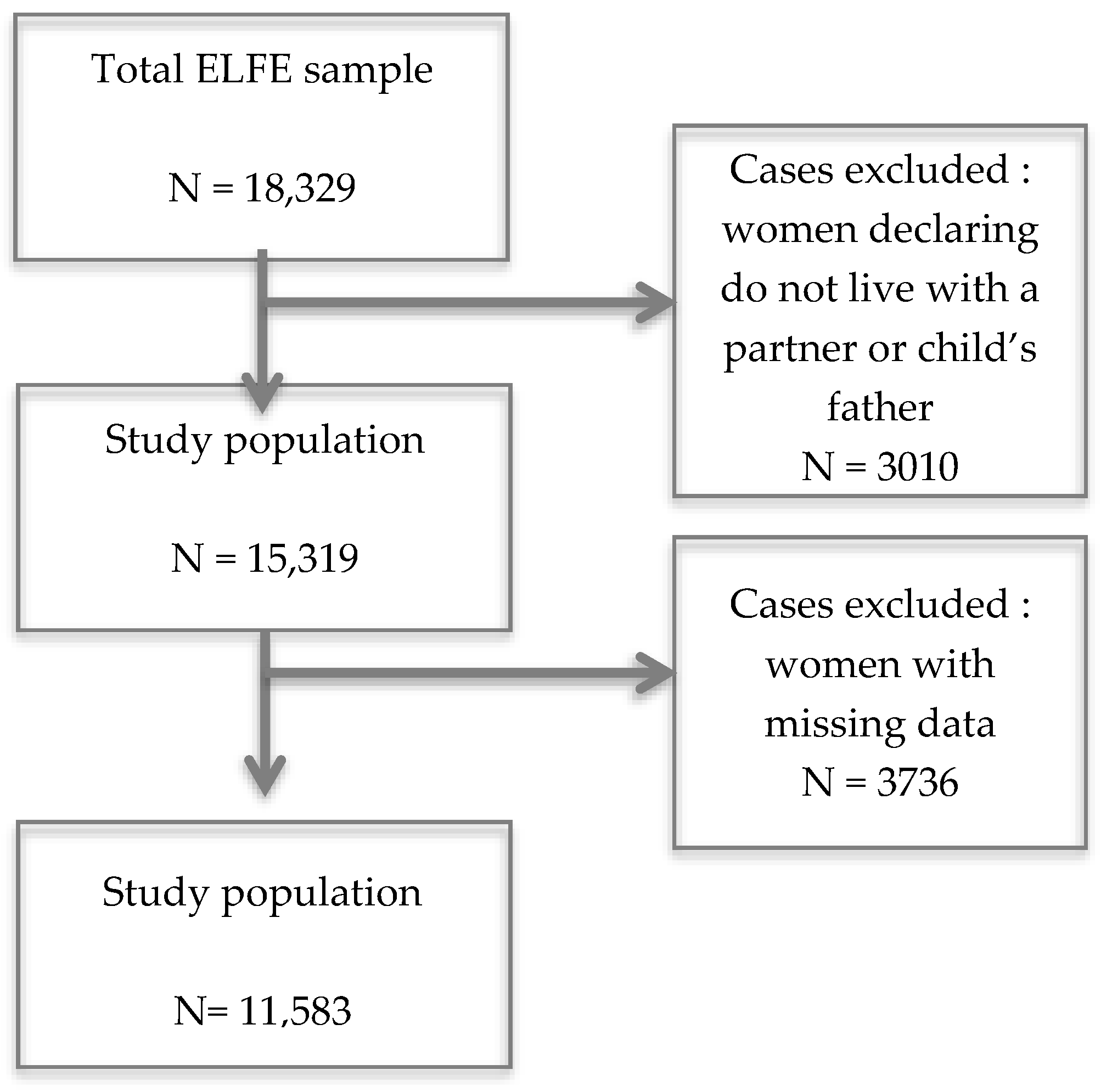
2.1. Data Source
2.2. Theoretical Model
2.3. Assessment of Postnatal Depressive Symptoms (PNDS)
2.4. Maternal and Environmental Vulnerability Factors
2.5. Maternal and Environmental Risk or Protective Factors
2.6. Infant Characteristics and Environmental Factors Specific to Parenthood
2.7. Infant Risk or Protective Factors
2.8. Statistical Analyses
3. Results
3.1. Characteristics of the Sample
3.2. EFA
3.3. Structural Equation Modeling
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bauer, A.; Parsonage, M.; Knapp, M.; Lemmi, V.; Adelaja, B. The costs of perinatal mental health problems. J. Affect. Disord. 2016, 192, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverman, M.E.; Reichenberg, A.; Savitz, D.A.; Cnattingius, S.; Lichtenstein, P.; Hultman, C.M.; Larsson, H.; Sandin, S. The risk factors for postpartum depression: A population-based study. Depress. Anxiety 2017, 34, 178–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, E.; Celasun, N.; Stewart, D.E. Risk factors for postpartum depression. In Postpartum Depression: Literature Review of Risk Factors and Interventions; University Health Network Women’s Health Program for Toronto Public Health: Toronto, ON, Canada, 2003. [Google Scholar]
- Beck, C.T. Predictors of Postpartum Depression: An Update. Nurs. Res. 2001, 50, 275–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milgrom, J.; Gemmill, A.W.; Bilszta, J.L.; Hayes, B.; Barnett, B.; Brooks, J.; Ericksen, J.; Ellwood, D.; Buist, A. Antenatal risk factors for postnatal depression: A large prospective study. J. Affect. Disord. 2008, 108, 147–157. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.W.; Swain, A.M. Rates and risk of postpartum depression—A meta-analysis. Int. Rev. Psychiatry 1996, 8, 37–54. [Google Scholar] [CrossRef]
- Robertson, E.; Grace, S.; Wallington, T.; E Stewart, D. Antenatal risk factors for postpartum depression: A synthesis of recent literature. Gen. Hosp. Psychiatry 2004, 26, 289–295. [Google Scholar] [CrossRef]
- Reid, K.M.; Taylor, M.G. Social support, stress, and maternal postpartum depression: A comparison of supportive relationships. Soc. Sci. Res. 2015, 54, 246–262. [Google Scholar] [CrossRef]
- Palumbo, G.; Mirabella, F.; Gigantesco, A. Positive screening and risk factors for postpartum depression. Eur. Psychiatry 2017, 42, 77–85. [Google Scholar] [CrossRef]
- McCurdy, K.; Tovar, A.; Kaar, J.L.; Vadiveloo, M. Pathways between maternal depression, the family environment, and child BMI z scores. Appetite 2018, 134, 148–154. [Google Scholar] [CrossRef]
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Chien, L.-Y.; Tai, C.-J.; Hwang, F.-M.; Huang, C.-M. Postpartum physical symptoms and depressive symptomatology at 1 month and 1 year after delivery: A longitudinal questionnaire survey. Int. J. Nurs. Stud. 2009, 46, 1201–1208. [Google Scholar] [CrossRef]
- Eckerdal, P.; Kollia, N.; Löfblad, J.; Hellgren, C.; Karlsson, L.; Högberg, U.; Wikström, A.-K.; Skalkidou, A. Delineating the Association between Heavy Postpartum Haemorrhage and Postpartum Depression. PLoS ONE 2016, 11, e0144274. [Google Scholar] [CrossRef]
- Kita, S.; Haruna, M.; Matsuzaki, M.; Kamibeppu, K. Associations between intimate partner violence (IPV) during pregnancy, mother-to-infant bonding failure, and postnatal depressive symptoms. Arch. Women’s Ment. Health 2016, 19, 623–634. [Google Scholar] [CrossRef]
- Logsdon, M.C.; Usui, W. Psychosocial Predictors of Postpartum Depression in Diverse Groups of Women. West. J. Nurs. Res. 2001, 23, 563–574. [Google Scholar] [CrossRef]
- Shwartz, N.; O’Rourke, N.; Daoud, N. Pathways Linking Intimate Partner Violence and Postpartum Depression Among Jewish and Arab Women in Israel. J. Interpers. Violence 2022, 37, 301–321. [Google Scholar] [CrossRef]
- Stapleton, L.R.T.; Schetter, C.D.; Westling, E.; Rini, C.; Glynn, L.M.; Hobel, C.J.; Sandman, C.A. Perceived Partner Support in Pregnancy Predicts Lower Maternal and Infant Distress. J. Div. Fam. Psychol. Am. Psychol. Assoc. 2012, 26, 453–463. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Jin, S. The impact of social support on postpartum depression: The mediator role of self-efficacy. J. Health Psychol. 2014, 21, 720–726. [Google Scholar] [CrossRef]
- Murray, L.; Arteche, A.; Fearon, P.; Halligan, S.; Croudace, T.; Cooper, P. The effects of maternal postnatal depression and child sex on academic performance at age 16 years: A developmental approach. J. Child Psychol. Psychiatry 2010, 51, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Milgrom, J.; Martin, P.R.; Negri, L.M. Psychosocial risk factors for postnatal depression. In Treating Postnatal Depression: A Psychological Approach for Health Care Practioners; Milgrom, J., Martin, P.R., Negri, L.M., Eds.; Wiley: Chichester, UK, 1999; pp. 20–28. [Google Scholar]
- Hassert, S.; Kurpius, S.E.R.; Tracey, T.J.G. Testing a Conceptual Model of Postpartum Depressive Symptoms in the First Year. Women Health 2015, 55, 700–716. [Google Scholar] [CrossRef] [PubMed]
- Ross, L.E.; Sellers, E.M.; Evans, S.E.G.; Romach, M.K. Mood changes during pregnancy and the postpartum period: Development of a biopsychosocial model. Acta Psychiatr. Scand. 2004, 109, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Charles, M.A. Cohort profile: The French national cohort of children (ELFE): Birth to 5 years. Int. J. Epidemiol. 2020, 49, 368–369. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Guedeney, N.; Fermanian, J.; Guelfi, J.D.; Delour, M. Premiers résultats de la traduction de l’Edingburgh Postnatal Depression Scale sur une population parisienne. Devenir 1995, 7, 69–92. [Google Scholar]
- Guedeney, N.; Fermanian, J. Validation study of the French version of the Edinburgh Postnatal Depression Scale (EPDS): New results about use and psychometric properties. Eur. Psychiatry 1998, 13, 83–89. [Google Scholar] [CrossRef]
- Sutter-Dallay, A.; Giaconne-Marcesche, V.; Glatigny-Dallay, E.; Verdoux, H. Women with anxiety disorders during pregnancy are at increased risk of intense postnatal depressive symptoms: A prospective survey of the MATQUID cohort. Eur. Psychiatry 2004, 19, 459–463. [Google Scholar] [CrossRef]
- Dennis, C.L. Can We Identify Mothers at Risk for Postpartum Depression in the Immediate Postpartum Period Using the Edinburgh Postnatal Depression Scale? J. Affect. Disord. 2004, 78, 163–169. [Google Scholar] [CrossRef]
- McNeil, T.; Sjöström, K. Mcneil-Sjöström Scale for Obstetric Complications; Lund University Department of Psychiatry, Malmö University Hospital: Malmö, Sweden, 1995. [Google Scholar]
- Du, H.; Bentler, P.M. Distributionally weighted least squares in structural equation modeling. Psychol. Methods 2022, 27, 519–540. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- SAS Institute Inc. SAS 9.1.3 Help and Documentation; SAS Institute Inc.: Cary, NC, USA, 2004. [Google Scholar]
- Arbuckle, J.L. Amos, Version 7.0. Computer Program; SPSS: Chicago, IL, USA, 2006.
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2015, 191, 62–77. [Google Scholar] [CrossRef] [Green Version]
- Della Corte, L.; La Rosa, V.L.; Cassinese, E.; Ciebiera, M.; Zaręba, K.; De Rosa, N.; Verrazzo, P.; Improda, F.P.; Vitale, S.G.; Giampaolino, P.; et al. Prevalence and associated psychological risk factors of postpartum depression: A cross-sectional study. J. Obstet. Gynaecol. 2021, 42, 976–980. [Google Scholar] [CrossRef]
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pr. Res. Clin. Obstet. Gynaecol. 2013, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Pilkington, P.D.; Milne, L.C.; Cairns, K.E.; Lewis, J.; Whelan, T.A. Modifiable partner factors associated with perinatal depression and anxiety: A systematic review and meta-analysis. J. Affect. Disord. 2015, 178, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Yamada, A.; Isumi, A.; Fujiwara, T. Association between Lack of Social Support from Partner or Others and Postpartum Depression among Japanese Mothers: A Population-Based Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 4270. [Google Scholar] [CrossRef] [PubMed]
- Barandon, S.; Balès, M.; Melchior, M.; Glangeaud-Freudenthal, N.; Pambrun, E.; Bois, C.; Verdoux, H.; Sutter-Dallay, A.L. Early prenatal interview and antenatal education for childbirth and parenthood: Associated psychosocial and obstet-ric characteristics in women of the ELFE cohort. J. Gynecol. Obstet. Biol. Reprod. 2016, 45, 599–607. [Google Scholar] [CrossRef]
- Nakamura, A.; Sutter-Dallay, A.-L.; Lesueur, F.E.-K.; Thierry, X.; Gressier, F.; Melchior, M.; van der Waerden, J. Informal and formal social support during pregnancy and joint maternal and paternal postnatal depression: Data from the French representative ELFE cohort study. Int. J. Soc. Psychiatry 2020, 66, 431–441. [Google Scholar] [CrossRef] [Green Version]
- Blondel, B.; Kermarrec, M. Enquête Nationale Périnatale 2010. Les Naissances en 2010 et leur Évolution Depuis 2003; INSERM: Paris, France, 2011. [Google Scholar]
- Kim, W.; Jang, S.Y.; Lee, T.H.; Lee, J.E.; Park, E.C. Association between continuity of care and subsequent hospitalization and mortality in patients with mood disorders: Results from the Korea National Health In-surance cohort. PLoS ONE 2018, 13, e0207740. [Google Scholar] [CrossRef]
- Cutrona, C.E.; Troutman, B.R. Social support, infant temperament, and parenting self-efficacy: A mediational model of postpartum depression. Child Dev. 1986, 57, 1507–1518. [Google Scholar] [CrossRef]
- Vik, T.; Grote, V.; Escribano, J.; Socha, J.; Verduci, E.; Fritsch, M.; Carlier, C.; Kries, R.V.; Koletzko, B.; European Childhood Obesity Trial Study Group. Infantile colic, prolonged crying and maternal postnatal depression. Acta Paediatr. 2009, 98, 1344–1348. [Google Scholar] [CrossRef]
- Eastwood, J.G.; Jalaludin, B.B.; Kemp, L.A.; Phung, H.N.; Barnett, B.E. Relationship of postnatal depres-sive symptoms to infant temperament, maternal expectations, social support and other potential risk factors: Findings from a large Australian cross-sectional study. BMC Pregnancy Childbirth 2012, 12, 148. [Google Scholar] [CrossRef] [Green Version]
- Trost, M.J.; Molas-Torreblanca, K.; Man, C.; Casillas, E.; Sapir, H.; Schrager, S.M. Screening for maternal postpartum depression during infant hospitalizations. J. Hosp. Med. 2016, 11, 840–846. [Google Scholar] [CrossRef] [Green Version]
- Baker, P.; Mott, F. NLSY Child Handbook 1989: A Guide and ResourceDocument for the National Longitudinal Study of Youth 1986 Child Data; Center for Human Resource Research, The Ohio State University: Columbus, OH, USA, 1989. [Google Scholar]
- Smith, K.; Joshi, H. The Millennium Cohort Study. Popul. Trends 2002, 107, 30–34. [Google Scholar]
- van der Zee-van den Berg, A.I.; Boere-Boonekamp, M.M.; IJzerman, M.J.; Haasnoot-Smallegange, R.M.; Reijneveld, S.A. Reijneveld. Screening for Postpartum Depression in Well-Baby Care Settings: A Systematic Re-view. Matern. Child Health J. 2017, 21, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Gałecka, M.; Bliźniewska-Kowalska, K.; Maes, M.; Su, K.P.; Gałecki, P. Update on the Neurodevelopmental Theory of Depression: Is There Any “Unconscious Code”? Pharmacol. Rep. 2021, 73, 346–356. [Google Scholar] [CrossRef]
- Gałecki, P.; Talarowska, M. Neurodevelopmental theory of depression. Prog. Neuro-Pharmacol. Biol. Psychiatry 2018, 80, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Lima-Ojeda, J.M.; Rupprecht, R.; Baghai, T.C. Neurobiology of depression: A neurodevelopmental approach. World J. Biol. Psychiatry 2017, 19, 349–359. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Maternal and Environmental Vulnerability Factors | Maternal and Environmental Risk or Protective Factors | Infant Characteristics and Environmental Factors Specific to Parenthood | Infant Risk or Protective Factors |
|---|---|---|---|
| Socio-demographic and economic variables | Perceived antenatal emotional support from partner | Early maternal parenting behaviour | Infants’ self-regulation skills |
Mother’s age
| Antenatal emotional support from spouse
| Sing songs
| Self-appeasement
|
Nationality
| Quarrels with or without insults within the couple
| Talk to the child
| Frequency of crying
|
Educational level
| Perceived postnatal instrumental support | Maternal ability to understand infant cries
| Nocturnal awakenings
|
For baby’s care (Changing diapers, feeding, wash, put it to sleep, taking it for a walk, getting up in the night because of cries, taking it to the doctor)
| |||
Mother’s employment status during pregnancy
| For household chores (Washing dishes, doing shopping, preparing meals, doing laundry, doing the housework, repairs)
| Respect of infant’s feeding rhythm
| |
Number of children
| Maternal antenatal preventive measures | Mother’s reaction if baby eats little or don’t finish his bottle (without illness context)
| |
Attending early prenatal interview, attending antenatal classes
| |||
Familial financial status
| Obstetrical complications | Infant’s physical health | |
Complications during pregnancy
| Infant’s condition evaluated by the mother
| ||
| Psychiatric History | Complications at birth, or neonatal complications
| Infant hospitalization since returning from maternity hospital stay
| |
Consultation with a mental health specialist before pregnancy (psychiatrist, psychologist, psychotherapist or another doctor)
| |||
Depression during a previous pregnancy
| Psychological factors | ||
Reaction about the current pregnancy
| |||
Experience of pregnancy
| |||
Desire of pregnancy
| |||
Prenatal psychological distress
|
| Maternal and Environmental Vulnerability Factors | |
|---|---|
| Socio-Demographic and Economic Variables | n (%) |
| Mother’s age | |
| 18–24 | 1049 (9.1) |
| 25–34 | 8180 (70.6) |
| ≥35 years | 2354 (20.3) |
| Nationality | |
| French | 10,727 (92.6) |
| French by naturalisation | 325 (2.8) |
| Foreigner | 531 (4.6) |
| Educational level | |
| <9 | 1429 (12.3) |
| 9–11 | 2081 (18.0) |
| ≥12 years | 8073 (69.7) |
| Mother’s employment status during pregnancy | |
| Employed or student | 10,108 (87.3) |
| Housewife, on parental leave or retired | 939 (8.1) |
| Unemployed | 536 (4.6) |
| Number of children | |
| 1 | 5296 (45.7) |
| 2 | 4251 (36.7) |
| 3 or more | 2036 (17.6) |
| Familial financial status | |
| High and middle | 6764 (58.4) |
| Low | 4022 (34.7) |
| Very low | 797 (6.9) |
| Psychiatric history | n (%) |
| Consultation with a mental health specialist before pregnancy (psychiatrist, psychologist, psychotherapist or another doctor) | |
| Yes | 832 (7.2) |
| No | 10,751 (92.8) |
| Depression during a previous pregnancy | |
| Yes | 832 (7.2) |
| No | 10,751 (92.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bales, M.; Pambrun, E.; Maguet, C.; van der Waerden, J.; Glangeaud-Freudenthal, N.; Charles, M.-A.; Bois, C.; Melchior, M.; Milgrom, J.; Falissard, B.; et al. Pathways between Risk/Protective Factors and Maternal Postnatal Depressive Symptoms: The ELFE Cohort. J. Clin. Med. 2023, 12, 3204. https://doi.org/10.3390/jcm12093204
Bales M, Pambrun E, Maguet C, van der Waerden J, Glangeaud-Freudenthal N, Charles M-A, Bois C, Melchior M, Milgrom J, Falissard B, et al. Pathways between Risk/Protective Factors and Maternal Postnatal Depressive Symptoms: The ELFE Cohort. Journal of Clinical Medicine. 2023; 12(9):3204. https://doi.org/10.3390/jcm12093204
Chicago/Turabian StyleBales, Mélanie, Elodie Pambrun, Charlotte Maguet, Judith van der Waerden, Nine Glangeaud-Freudenthal, Marie-Aline Charles, Corinne Bois, Maria Melchior, Jeannette Milgrom, Bruno Falissard, and et al. 2023. "Pathways between Risk/Protective Factors and Maternal Postnatal Depressive Symptoms: The ELFE Cohort" Journal of Clinical Medicine 12, no. 9: 3204. https://doi.org/10.3390/jcm12093204