

The Effect of High-Intensity Interval Training Type on Body Fat Percentage, Fat and Fat-Free Mass: A Systematic Review and Meta-Analysis of Randomized Clinical Trials

 , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Search Strategies
2.2. Study Selection and Inclusion/Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
2.6. Certainty Assessment
3. Results
3.1. Selection and Identification of RCTs
3.2. Characteristics of the Included RCTs
3.3. Findings from the Systematic Review
3.4. Findings from the Meta-Analysis
3.5. Quality of Evidence
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martland, R.; Korman, N.; Firth, J.; Vancampfort, D.; Thompson, T.; Stubbs, B. Can high-intensity interval training improve mental health outcomes in the general population and those with physical illnesses? A systematic review and meta-analysis. Br. J. Sport Med. 2022, 56, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.; Winzer, E.B.; Duvinage, A.; Gevaert, A.B.; Edelmann, F.; Haller, B.; Pieske-Kraigher, E.; Beckers, P.; Bobenko, A.; Hommel, J.; et al. Effect of high-intensity interval training, moderate continuous training, or guideline-based physical activity advice on peak oxygen consumption in patients with heart failure with preserved ejection fraction: A randomized clinical trial. JAMA 2021, 325, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Hooshmand Moghadam, B.; Golestani, F.; Bagheri, R.; Cheraghloo, N.; Eskandari, M.; Wong, A.; Nordvall, M.; Suzuki, K.; Pournemati, P. The effects of high-intensity interval training vs. moderate-intensity continuous training on inflammatory markers, body composition, and physical fitness in overweight/obese survivors of breast cancer: A randomized controlled clinical trial. Cancers 2021, 13, 4386. [Google Scholar] [CrossRef]
- Atakan, M.M.; Li, Y.; Koşar, Ş.N.; Turnagöl, H.H.; Yan, X. Evidence-based effects of high-intensity interval training on exercise capacity and health: A review with historical perspective. Int. J. Environ. Res. Public Health 2021, 18, 7201. [Google Scholar] [CrossRef]
- Milanović, Z.; Sporiš, G.; Weston, M. Effectiveness of high-intensity interval training (HIT) and continuous endurance training for VO2max improvements: A systematic review and meta-analysis of controlled trials. Sport Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef] [Green Version]
- Engel, F.A.; Ackermann, A.; Chtourou, H.; Sperlich, B. High-intensity interval training performed by young athletes: A systematic review and meta-analysis. Front. Physiol. 2018, 9, 1012. [Google Scholar] [CrossRef] [Green Version]
- Bagheri, R.; Robinson, I.; Moradi, S.; Purcell, J.; Schwab, E.; Silva, T.; Baker, B.; Camera, D.M. Muscle protein synthesis responses following aerobic-based exercise or high-intensity interval training with or without protein ingestion: A systematic review. Sport Med. 2022, 52, 2713–2732. [Google Scholar] [CrossRef]
- Gibala, M.J.; Jones, A.M. Physiological and performance adaptations to high-intensity interval training. Limits Hum. Endur. 2013, 76, 51–60. [Google Scholar]
- Jelleyman, C.; Yates, T.; O’Donovan, G.; Gray, L.J.; King, J.A.; Khunti, K.; Davies, M.J. The effects of high-intensity interval training on glucose regulation and insulin resistance: A meta-analysis. Obes. Rev. 2015, 16, 942–961. [Google Scholar] [CrossRef] [Green Version]
- Taylor, J.L.; Holland, D.J.; Spathis, J.G.; Beetham, K.S.; Wisløff, U.; Keating, S.E.; Coombes, J.S. Guidelines for the delivery and monitoring of high intensity interval training in clinical populations. Prog. Cardiovasc. Dis. 2019, 62, 140–146. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alarcon Hormazabal, M.; Delgado Floody, P.; Castillo Mariqueo, L.; Thuiller Lepelegy, N.; Borquez Becerra, P.; Sepulveda Mancilla, C.; Rebolledo Quezada, S. Effects of 8 weeks of high intensity interval training program on the levels of basal blood glucose, anthropometric profile and VO2 max of young sedentary with overweight or obesity. Nutr. Hosp. 2016, 33, 284–288. [Google Scholar]
- Gillen, J.B.; Percival, M.E.; Ludzki, A.; Tarnopolsky, M.A.; Gibala, M.J. Interval training in the fed or fasted state improves body composition and muscle oxidative capacity in overweight women. Obesity 2013, 21, 2249–2255. [Google Scholar] [CrossRef]
- Hazell, T.J.; Hamilton, C.D.; Olver, T.D.; Lemon, P.W. Running sprint interval training induces fat loss in women. Appl. Physiol. Nutr. Metab. 2014, 39, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Mandrup, C.M.; Egelund, J.; Nyberg, M.; Enevoldsen, L.H.; Kjær, A.; Clemmensen, A.E.; Christensen, A.N.; Suetta, C.; Frikke-Schmidt, R.; Steenberg, D.E.; et al. Effects of menopause and high-intensity training on insulin sensitivity and muscle metabolism. Menopause 2018, 25, 165–175. [Google Scholar] [CrossRef]
- Molina, C.; Cifuentes, G.; Martinez, C.; Mancilla, R.; Diaz, E. Effects of 12 sessions of high intensity intermittent training and nutrition counseling on body fat in obese and overweight participants. Rev. Médica De Chile 2016, 144, 1254–1259. [Google Scholar] [CrossRef] [Green Version]
- Sultana, R.N.; Sabag, A.; Keating, S.E.; Johnson, N.A. The effect of low-volume high-intensity interval training on body composition and cardiorespiratory fitness: A systematic review and meta-analysis. Sport Med. 2019, 49, 1687–1721. [Google Scholar] [CrossRef]
- Wu, Z.-J.; Wang, Z.-Y.; Gao, H.-E.; Zhou, X.-F.; Li, F.-H. Impact of high-intensity interval training on cardiorespiratory fitness, body composition, physical fitness, and metabolic parameters in older adults: A meta-analysis of randomized controlled trials. Exp. Gerontol. 2021, 150, 111345. [Google Scholar] [CrossRef]
- Wewege, M.; van den Berg, R.; Ward, R.E.; Keech, A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: A systematic review and meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2017, 18, 635–646. [Google Scholar] [CrossRef]
- Millet, G.P.; Vleck, V.E.; Bentley, D.J. Physiological differences between cycling and running. Sport Med. 2009, 39, 179–206. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Hayashino, Y.; Noguchi, Y.; Fukui, T. Systematic evaluation and comparison of statistical tests for publication bias. J. Epidemiol. 2005, 15, 235–243. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Chuensiri, N.; Suksom, D.; Tanaka, H. Effects of High-Intensity Intermittent Training on Vascular Function in Obese Preadolescent Boys. Child. Obes. 2018, 14, 41–49. [Google Scholar] [CrossRef]
- Blüher, S.; Käpplinger, J.; Herget, S.; Reichardt, S.; Böttcher, Y.; Grimm, A.; Kratzsch, J.; Petroff, D. Cardiometabolic risk markers, adipocyte fatty acid binding protein (aFABP) and the impact of high-intensity interval training (HIIT) in obese adolescents. Metabolism 2017, 68, 77–87. [Google Scholar] [CrossRef]
- Plavsic, L.; Knezevic, O.M.; Sovtic, A.; Minic, P.; Vukovic, R.; Mazibrada, I.; Stanojlovic, O.; Hrncic, D.; Rasic-Markovic, A.; Macut, D. Effects of high-intensity interval training and nutrition advice on cardiometabolic markers and aerobic fitness in adolescent girls with obesity. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2020, 45, 294–300. [Google Scholar] [CrossRef]
- García-Pinillos, F.; González-Fernández, F.T.; Soto-Hermoso, V.M.; Latorre-Román, P.A. A high-intensity intermittent-based running programme allows triathletes to reduce weekly running distances without impairing muscular performance and body composition. Isokinet. Exerc. Sci. 2016, 24, 313–321. [Google Scholar] [CrossRef]
- Afzalpour, M.E.; Ghasemi, E.; Zarban, A. Effects of 10 weeks of high intensity interval training and green tea supplementation on serum levels of Sirtuin-1 and peroxisome proliferator-activated receptor gamma co-activator 1-alpha in overweight women. Sci. Sport 2017, 32, 82–90. [Google Scholar] [CrossRef]
- Ghasemi, E.; Afzalpour, M.E.; Nayebifar, S. Combined high-intensity interval training and green tea supplementation enhance metabolic and antioxidant status in response to acute exercise in overweight women. J. Physiol. Sci. JPS 2020, 70, 31. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, T.S.; Sverrisdottir, Y.; Bangsbo, J.; Gunnarsson, T.P. High-Intensity Interval Training Decreases Muscle Sympathetic Nerve Activity in Men With Essential Hypertension and in Normotensive Controls. Front. Neurosci. 2020, 14, 841. [Google Scholar] [CrossRef] [PubMed]
- De Strijcker, D.; Lapauw, B.; Ouwens, D.M.; Van de Velde, D.; Hansen, D.; Petrovic, M.; Cuvelier, C.; Tonoli, C.; Calders, P. High intensity interval training is associated with greater impact on physical fitness, insulin sensitivity and muscle mitochondrial content in males with overweight/obesity, as opposed to continuous endurance training: A randomized controlled trial. J. Musculoskelet. Neuronal Interact. 2018, 18, 215–226. [Google Scholar] [PubMed]
- Evangelista, A.L.; La Scala Teixeira, C.; Machado, A.F.; Pereira, P.E.; Rica, R.L.; Bocalini, D.S. Effects of a short-term of whole-body, high-intensity, intermittent training program on morphofunctional parameters. J. Bodyw. Mov. Ther. 2019, 23, 456–460. [Google Scholar] [CrossRef]
- Schjerve, I.E.; Tyldum, G.A.; Tjønna, A.E.; Stølen, T.; Loennechen, J.P.; Hansen, H.E.; Haram, P.M.; Heinrich, G.; Bye, A.; Najjar, S.M.; et al. Both aerobic endurance and strength training programmes improve cardiovascular health in obese adults. Clin. Sci. 2008, 115, 283–293. [Google Scholar] [CrossRef] [Green Version]
- Nunes, P.R.P.; Martins, F.M.; Souza, A.P.; Carneiro, M.A.S.; Nomelini, R.S.; Michelin, M.A.; Murta, E.F.C.; de Oliveira, E.P.; Orsatti, F.L. Comparative effects of high-intensity interval training with combined training on physical function markers in obese postmenopausal women: A randomized controlled trial. Menopause 2019, 26, 1242–1249. [Google Scholar] [CrossRef]
- Alizadeh, H.; Safarzade, A. High intensity intermittent training induces anti-inflammatory cytokine responses and improves body composition in overweight adolescent boys. Horm. Mol. Biol. Clin. Investig. 2019, 39, 1–10. [Google Scholar] [CrossRef]
- Azar, J.T.; Hemmatinafar, M.; Nemati, J. Effect of six weeks of high intensity interval training on leptin levels, lipid profile and fat percentage in sedentary young men. Sport Sci. 2018, 11, 78–82. [Google Scholar]
- Chin, E.C.; Yu, A.P.; Lai, C.W.; Fong, D.Y.; Chan, D.K.; Wong, S.H.; Sun, F.; Ngai, H.H.; Yung, P.S.H.; Siu, P.M. Low-Frequency HIIT Improves Body Composition and Aerobic Capacity in Overweight Men. Med. Sci. Sport Exerc. 2020, 52, 56–66. [Google Scholar] [CrossRef]
- Kazemi, A.; Eslami, R.; Ali, M.G.; Ghanbarzadeh, M. Effects of 6 weeks of low volume high intensity interval training on serum levels of leptin, glucose, and body fat in young wrestlers. Sci. J. Kurd. Univ. Med. Sci. 2015, 20, 70–77. [Google Scholar]
- Kemmler, W.; Scharf, M.; Lell, M.; Petrasek, C.; Von Stengel, S. High versus moderate intensity running exercise to impact cardiometabolic risk factors: The randomized controlled rush-study. BioMed Res. Int. 2014, 2014, 843095. [Google Scholar] [CrossRef] [Green Version]
- Khammassi, M.; Ouerghi, N.; Hadj-Taieb, S.; Feki, M.; Thivel, D.; Bouassida, A. Impact of a 12-week high-intensity interval training without caloric restriction on body composition and lipid profile in sedentary healthy overweight/obese youth. J. Exerc. Rehabil. 2018, 14, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Mosallanezhad, Z.; Nikbakht, H.; Gaeini, A.A.; Gholami, M. The effect of high-intensity interval training on telomere length of leukocytes in sedentary young women. Adv. Environ. Biol. 2014, 8, 841–845. [Google Scholar]
- Zhang, H.; KTong, T.; Qiu, W.; Wang, J.; Nie, J.; He, Y. Effect of high-intensity interval training protocol on abdominal fat reduction in overweight Chinese women: A randomized controlled trial. Kinesiology 2015, 47, 57–66. [Google Scholar]
- Nybo, L.; Sundstrup, E.; Jakobsen, M.D.; Mohr, M.; Hornstrup, T.; Simonsen, L.; Bülow, J.; Randers, M.B.; Nielsen, J.J.; Aagaard, P.; et al. High-intensity training versus traditional exercise interventions for promoting health. Med. Sci. Sport Exerc. 2010, 42, 1951–1958. [Google Scholar] [CrossRef] [Green Version]
- TaheriChadorneshin, H.; Cheragh-Birjandi, S.; Goodarzy, S.; Ahmadabadi, F. The impact of high intensity interval training on serum chemerin, tumor necrosis factor-alpha and insulin resistance in overweight women. Obes. Med. 2019, 14, 100101. [Google Scholar] [CrossRef]
- Ahmadizad, S.; Avansar, A.S.; Ebrahim, K.; Avandi, M.; Ghasemikaram, M. The effects of short-term high-intensity interval training vs. moderate-intensity continuous training on plasma levels of nesfatin-1 and inflammatory markers. Horm. Mol. Biol. Clin. Investig. 2015, 21, 165–173. [Google Scholar] [CrossRef]
- Smith-Ryan, A.E.; Melvin, M.N.; Wingfield, H.L. High-intensity interval training: Modulating interval duration in overweight/obese men. Physician Sportsmed. 2015, 43, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Keating, S.E.; Machan, E.A.; O’Connor, H.T.; Gerofi, J.A.; Sainsbury, A.; Caterson, I.D.; Johnson, N.A. Continuous exercise but not high intensity interval training improves fat distribution in overweight adults. J. Obes. 2014, 2014, 834865. [Google Scholar] [CrossRef]
- Heydari, M.; Freund, J.; Boutcher, S.H. The effect of high-intensity intermittent exercise on body composition of overweight young males. J. Obes. 2012, 2012, 480467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sim, A.Y.; Wallman, K.E.; Fairchild, T.J.; Guelfi, K.J. Effects of high-intensity intermittent exercise training on appetite regulation. Med. Sci. Sport Exerc. 2015, 47, 2441–2449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillen, J.B.; Martin, B.J.; MacInnis, M.J.; Skelly, L.E.; Tarnopolsky, M.A.; Gibala, M.J. Twelve weeks of sprint interval training improves indices of cardiometabolic health similar to traditional endurance training despite a five-fold lower exercise volume and time commitment. PLoS ONE 2016, 11, e0154075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Astorino, T.A.; Heath, B.; Bandong, J.; Ordille, G.M.; Contreras, R.; Montell, M.; Schubert, M.M. Effect of periodized high intensity interval training (HIIT) on body composition and attitudes towards hunger in active men and women. J. Sport Med. Phys. Fit. 2018, 58, 1052–1062. [Google Scholar] [CrossRef] [PubMed]
- Arad, A.D.; DiMenna, F.J.; Thomas, N.; Tamis-Holland, J.; Weil, R.; Geliebter, A.; Albu, J.B. High-intensity interval training without weight loss improves exercise but not basal or insulin-induced metabolism in overweight/obese African American women. J. Appl. Physiol. 2015, 119, 352–362. [Google Scholar] [CrossRef] [Green Version]
- Atashak, S.; Stannard, S.R.; Daraei, A.; Soltani, M.; Saeidi, A.; Moradi, F.; Laher, I.; Hackney, A.C.; Zouhal, H. High-Intensity Interval Training Improves Lipocalin-2 and Omentin-1 Levels in Men with Obesity. Int. J. Sport Med. 2022, 43, 328–335. [Google Scholar] [CrossRef]
- Stavrinou, P.S.; Bogdanis, G.C.; Giannaki, C.D.; Terzis, G.; Hadjicharalambous, M. High-intensity Interval Training Frequency: Cardiometabolic Effects and Quality of Life. Int. J. Sport Med. 2018, 39, 210–217. [Google Scholar] [CrossRef]
- Ziemann, E.; Grzywacz, T.; Luszczyk, M.; Laskowski, R.; Olek, R.A.; Gibson, A.L. Aerobic and anaerobic changes with high-intensity interval training in active college-aged men. J. Strength Cond. Res. 2011, 25, 1104–1112. [Google Scholar] [CrossRef]
- Tong, T.K.; Zhang, H.; Shi, H.; Liu, Y.; Ai, J.; Nie, J.; Kong, Z. Comparing Time Efficiency of Sprint vs. High-Intensity Interval Training in Reducing Abdominal Visceral Fat in Obese Young Women: A Randomized, Controlled Trial. Front. Physiol. 2018, 9, 1048. [Google Scholar] [CrossRef] [Green Version]
- Hu, M.; Kong, Z.; Sun, S.; Zou, L.; Shi, Q.; Chow, B.C.; Nie, J. Interval training causes the same exercise enjoyment as moderate-intensity training to improve cardiorespiratory fitness and body composition in young Chinese women with elevated BMI. J. Sport Sci. 2021, 39, 1677–1686. [Google Scholar] [CrossRef]
- Sañudo, B.; Muñoz, T.; Davison, G.W.; Lopez-Lluch, G.; Del Pozo-Cruz, J. High-Intensity Interval Training Combined With Vibration and Dietary Restriction Improves Body Composition and Blood Lipids in Obese Adults: A Randomized Trial. Dose-Response A Publ. Int. Hormesis Soc. 2018, 16, 1559325818797015. [Google Scholar] [CrossRef] [Green Version]
- Reljic, D.; Frenk, F.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Low-volume high-intensity interval training improves cardiometabolic health, work ability and well-being in severely obese individuals: A randomized-controlled trial sub-study. J. Transl. Med. 2020, 18, 419. [Google Scholar] [CrossRef]
- Trapp, E.G.; Chisholm, D.J.; Freund, J.; Boutcher, S.H. The effects of high-intensity intermittent exercise training on fat loss and fasting insulin levels of young women. Int. J. Obes. 2008, 32, 684–691. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Tong, T.K.; Kong, Z.; Shi, Q.; Liu, Y.; Nie, J. Exercise training-induced visceral fat loss in obese women: The role of training intensity and modality. Scand. J. Med. Sci. Sport 2021, 31, 30–43. [Google Scholar] [CrossRef]
- Rentería, I.; García-Suárez, P.C.; Martínez-Corona, D.O.; Moncada-Jiménez, J.; Plaisance, E.P.; JiméNez-Maldonado, A. Short-term high-Intensity interval training increases systemic brain-derived neurotrophic factor (BDNF) in healthy women. Eur. J. Sport Sci. 2020, 20, 516–524. [Google Scholar] [CrossRef]
- Tsekouras, Y.E.; Magkos, F.; Kellas, Y.; Basioukas, K.N.; Kavouras, S.A.; Sidossis, L.S. High-intensity interval aerobic training reduces hepatic very low-density lipoprotein-triglyceride secretion rate in men. Am. J. Physiol. Endocrinol. Metab. 2008, 295, E851–E858. [Google Scholar] [CrossRef] [Green Version]
- ZilaeiBouri, S.H.; Peeri, M. The effect of exercise intensity on the response of some of adipocytokins and biochemical marker of bone in obese and overweight young female. Iran. J. Endocrinol. Metab. 2015, 16, 425–432. [Google Scholar]
- García-Suárez, P.C.; Rentería, I.; García Wong-Avilés, P.; Franco-Redona, F.; Gómez-Miranda, L.M.; Aburto-Corona, J.A.; Plaisance, E.P.; Moncada-Jiménez, J.; Jiménez-Maldonado, A. Hemodynamic Adaptations Induced by Short-Term Run Interval Training in College Students. Int. J. Environ. Res. Public Health 2020, 17, 4636. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-la, O.A.; Jurado-Fasoli, L.; Ruiz, J.R.; Castillo, M.J.; Gutiérrez, Á. Effects of different exercise training programs on body composition: A randomized control trial. Scand. J. Med. Sci. Sport 2019, 29, 968–979. [Google Scholar] [CrossRef]
- Mirghani, S.J.; Seydyousefi, M.; Pekkala, S.; Sharifian, S.; Beyshami, G. Shorter recovery time following high-intensity interval training induced higher body fat loss among overweight women. Sport Sci. Health 2019, 15, 157–165. [Google Scholar] [CrossRef]
- Øvretveit, K. Aerobic interval training improves maximal oxygen uptake and reduces body fat in grapplers. J. Sport Med. Phys. Fit. 2019, 59, 1985–1990. [Google Scholar] [CrossRef] [PubMed]
- Galedari, M.; Azarbayjani, M.A.; Peeri, M. Effects of type of exercise along with caloric restriction on plasma apelin 36 and HOMA-IR in overweight men. Sci. Sport 2017, 32, e137–e145. [Google Scholar] [CrossRef]
- Gahreman, D.; Heydari, M.; Boutcher, Y.; Freund, J.; Boutcher, S. The effect of green tea ingestion and interval sprinting exercise on the body composition of overweight males: A randomized trial. Nutrients 2016, 8, 510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirghani, S.J.; Yousefi, M.S. The effect of interval recovery periods during HIIT on liver enzymes and lipid profile in overweight women. Sci. Sport 2015, 30, 147–154. [Google Scholar] [CrossRef]
- Girard, O.; Malatesta, D.; Millet, G.P. Walking in hypoxia: An efficient treatment to lessen mechanical constraints and improve health in obese individuals? Front. Physiol. 2017, 8, 73. [Google Scholar] [CrossRef] [Green Version]
- Hinnouho, G.-M.; Czernichow, S.; Dugravot, A.; Nabi, H.; Brunner, E.J.; Kivimaki, M.; Singh-Manoux, A. Metabolically healthy obesity and the risk of cardiovascular disease and type 2 diabetes: The Whitehall II cohort study. Eur. Heart J. 2015, 36, 551–559. [Google Scholar] [CrossRef]
- Laaksonen, M.; Kivelä, R.; Kyröläinen, H.; Sipilä, S.; Selänne, H.; Lautamäki, R.; Nuutila, P.; Knuuti, J.; Kalliokoski, K.K.; Komi, P.V. Effects of exhaustive stretch-shortening cycle exercise on muscle blood flow during exercise. Acta Physiol. 2006, 186, 261–270. [Google Scholar] [CrossRef]
- Cheneviere, X.; Malatesta, D.; Gojanovic, B.; Borrani, F. Differences in whole-body fat oxidation kinetics between cycling and running. Eur. J. Appl. Physiol. 2010, 109, 1037–1045. [Google Scholar] [CrossRef]
- Wang, L.; Hong, Y.; Li, J.X. Muscular activity of lower extremity muscles running on treadmill compared with different overground surfaces. Am. J. Sport Sci. Med. 2014, 2, 161–165. [Google Scholar] [CrossRef] [Green Version]
- Sedlock, D.A. Post-exercise energy expenditure after cycle ergometer and treadmill exercise. J. Strength Cond. Res. 1992, 6, 19–23. [Google Scholar]
- Katch, F.I.; Mcardle, W.D.; Pechar, G.S. Relationship of maximal leg force and leg composition to treadmill and bicycle ergometer maximum oxygen uptake. Med. Sci. Sport 1974, 6, 38–43. [Google Scholar]
- Callahan, M.J.; Parr, E.B.; Snijders, T.; Conceição, M.S.; Radford, B.E.; Timmins, R.G.; Devlin, B.L.; Hawley, J.A.; Camera, D.M. Skeletal muscle adaptive responses to different types of short-term exercise training and detraining in middle-age men. Med. Sci. Sport Exerc. 2021, 53, 2023–2036. [Google Scholar] [CrossRef]
- Airin, S.; Linoby, A.; Mohamad Zaki, M.S.; Baki, H.; Sariman, H.; Esham, B. The effects of high-intensity interval training and continuous training on weight loss and body composition in overweight females. In Proceedings of the International Colloquium on Sports Science, Exercise, Engineering and Technology 2014 (ICoSSEET 2014); Springer: Singapore, 2014. [Google Scholar]
- Higgins, S.; Fedewa, M.V.; Hathaway, E.D.; Schmidt, M.D.; Evans, E.M. Sprint interval and moderate-intensity cycling training differentially affect adiposity and aerobic capacity in overweight young-adult women. Appl. Physiol. Nutr. Metab. 2016, 41, 1177–1183. [Google Scholar] [CrossRef]
- Rønnestad, B.; Hansen, J.; Vegge, G.; Tønnessen, E.; Slettaløkken, G. Short intervals induce superior training adaptations compared with long intervals in cyclists–An effort-matched approach. Scand. J. Med. Sci. Sport 2015, 25, 143–151. [Google Scholar] [CrossRef]
- Spencer, M.; Bishop, D.; Dawson, B.; Goodman, C.; Duffield, R. Metabolism and performance in repeated cycle sprints: Active versus passive recovery. Med. Sci. Sport Exerc. 2006, 38, 1492. [Google Scholar] [CrossRef]
- Brooks, G.A. Cell–cell and intracellular lactate shuttles. J. Physiol. 2009, 587, 5591–5600. [Google Scholar] [CrossRef]
- Duren, D.L.; Sherwood, R.J.; Czerwinski, S.A.; Lee, M.; Choh, A.C.; Siervogel, R.M.; Cameron Chumlea, W. Body composition methods: Comparisons and interpretation. J. Diabetes Sci. Technol. 2008, 2, 1139–1146. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Adult Population Cohorts (≥18 Years) |
|---|---|
| Intervention | Exercise training (HIIT) involving either cycling, overground running, or treadmill running |
| Comparison | Between HIIT modes and non-exercise control group |
| Outcomes | Body fat percentage, fat mass, and fat-free mass |
| Study design | Human randomized control trials |
| Study | Participants | No. (Control/Intervention) | Mean Age | BMI | Duration | Type of HIIT | Exercise Intervention | BF% | FFM (kg) | FM (kg) | Equipment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sim et al., 2015 [52] | Overweight inactive men | 20 10/10 | 27.2 ± 1.2 | 31 ± 8 | 3 d/12 wk | Cycling | 15 s at a power output equivalent to approximately 170% VO2peak with an active recovery period (60 s at a power output of approximately 32% VO2peak) between efforts | NR | NR | DEXA | |
| Keating et al., 2014 [50] | Inactive, overweight adult | 26 13/13 | 42.9 ± 2.3 | 28.3 ± 0.5 | 3 d/12 wk | Cycling | 1–12 sets of 30–60 s at 120% VO2peak with 120–180 s active recovery period | NR | NR | DEXA | |
| Smith-Ryan et al., 2015 (A) [49] | Overweight men | 25 10/5 | 38.3 ± 11.5 | 31.3 ± 4.9 | 3 d/3 wk | Cycling | 10 sets × 1 min at 90% VO2peak with 60 s active recovery period | NR | NR | DEXA | |
| Smith-Ryan et al., 2015 (B) [49] | Overweight men | 25 10/5 | 38.3 ± 11.5 | 31.3 ± 4.9 | 3 d/3 wk | Cycling | 5 sets of 2 min at 80–100% VO2peak with 60 s active recovery period | NR | NR | DEXA | |
| Heydari et al., 2012 [51] | Inactive, overweight men | 46 21/25 | 24.9 ± 4.3 | 28.7 ± 0.7 | 3 d/12 wk | Cycling | 8 s sprint, 12 s recovery, continuously throughout each 20-min session. | DEXA | |||
| Gillen et al., 2016 [53] | Sedentary men | 15 6/9 | 27 ± 8 | 26 ± 6 | 3 d/12 wk | Cycling | 3 sets × 20 s ‘all-out’ cycle sprints (~500 W) followed by 2 min of Cycling recovery | NR | NR | ADP | |
| Astorino et al., 2018 (A) [54] | Active men and women | 45 32/13 | 24.1 ± 5.8 | NR | 20 sessions/7 wk | Cycling | 10 sessions of low-volume HIIT and 10 sessions of sprint 8–12 sets 30–60 s at 90–150% PPO sprints Followed by 75–120 recovery | NR | NR | Caliper | |
| Astorino et al., 2018 (B) [54] | Active men and women | 45 32/13 | 23.8 ± 3.8 | NR | 20 sessions/7 wk | Cycling | 10 sessions of low-volume HIIT and 10 sessions of HIIT, 5–10 sets 60–150 s at 70–110% PPO sprints Followed by 60–75 recovery | NR | NR | Caliper | |
| Arad et al., 2015 [55] | Healthy, pre-menopausal | 28 11/9 | 29.5 ± 5.5 | 32.3 ± 3.4 | 3 d/14 wk | Cycling | Four work intervals (30–60 s at 75–90% HRR) were performed with recovery intervals (180–210 s at 50% HRR) interspersed. | DEXA | |||
| Atashak et al., 2021 [56] | Healthy but inactive males with obesity | 30 15/15 | 24.9 ± 3.1 | 30.9 ± 1.04 | 3 d/12 wk | Cycling | 5 × 2 min interval bout at an intensity of 85–95% HR max interspersed by 1 min passive recovery, three times per week | NR | NR | Caliper | |
| Stavrinou et al., 2018 (A) [57] | Healthy inactive adults | 22 8/13 | 31.8 ± 1.6 | 23.7 ± 3.6 | 3 d/8 wk | Cycling | 10 × 60 s cycling intervals at an intensity of ~83% of the Wpeak obtained, interspersed With 60 s of low-intensity exercise (~30% Wpeak at 50 rpm). | NR | NR | Caliper | |
| Stavrinou et al., 2018 (B) [57] | Healthy inactive adults | 22 8/14 | 31.6 ± 2.15 | 23.5 ± 3.8 | 2 d/8 wk | Cycling | 10 × 60 s cycling intervals at an intensity of ~83% of the Wpeak obtained, interspersed With 60 s of low-intensity exercise (~30% Wpeak at 50 rpm). | NR | NR | Caliper | |
| Ziemann et al., 2011 [58] | Healthy, physically active but not highly trained, college-aged men | 21 11/10 | 21.3 ± 1 | 23.7 ± 1.85 | 3 d/6 wk | Cycling | 6 × 90 s bouts at 80% of VO2max (each followed by 180 s passive recovery) | BIA | |||
| Tong et al., 2018 (A) [59] | Female university students | 30 14/16 | 21 ± 1.2 | NR | 3 d/12 wk | Cycling | 80 × 6 s all-out cycle sprints interspersed with 9 s passive recovery | NR | DEXA | ||
| Tong et al., 2018 (B) [59] | Female university students | 30 14/16 | 21 ± 1.2 | NR | 3 d/12 wk | Cycling | Repeated 4 min bouts of cycling at 90% VO2max alternated with 3 min passive recovery until the work of 400 KJ was achieved | NR | DEXA | ||
| Hu et al., 2021 (A) [60] | Overweight/obese females | 30 15/15 | 21.2 ± 1.4 | 25.7 ± 2.4 | 3 d/12 wk | Cycling | 4 min cycling at 90% VO2peak followed by 3 min passive recovery for ~60 min | DEXA | |||
| Hu et al., 2021 (B) [60] | Overweight/obese females | 30 15/15 | 21.1 ± 1.05 | 25.7 ± 2.3 | 3 d/12 wk | Cycling | 80 × 6 s “all-out” Cycling interspersed with 9 s passive recovery | DEXA | |||
| Sañudo et al., 2018 [61] | Obese/overweight adults | 27 13/14 | 36.5 ± 8 | 31.7 ± 5.2 | 3 d/8 wk | Cycling | 6–10 sets × 1 min of HIIT at 90% HRpeak followed by 6–10 × 2 min passive recovery | NR | BIA | ||
| Reljic, D et al., 2020 [62] | Obese individuals with a sedentary occupation | 49 19/30 | 48.7 ± 9.9 | 39.4 ± 7.05 | 2 d/12 wk | Cycling | 5 interval bouts of 1 min at 80–95% HRmax interspersed with 1 min of low-intensity recovery | BIA | |||
| Trapp et al., 2008 [63] | Inactive but healthy women | 30 15/15 | 22.3 ± 0.4 | 24.1 ± 1.4 | 3 d/15 wk | Cycling | 60 sets of 8 s at a resistance of 0.5 kg and worked as hard as they could followed by 12 s of slow Cycling recovery | NR | DEXA | ||
| Zhang et al., 2021 (A) [64] | Obese young women | 24 13/11 | 21.05 ± 1.9 | 25.4 ± 2.1 | 44 se/12 wk | Cycling | 40 bouts of 6 s all-out SIT (SIT all-out) interspersed with 9 s passive recovery | NR | DEXA | ||
| Zhang et al., 2021 (B) [64] | Obese young women | 25 13/12 | 20.4 ± 1.7 | 25.6 ± 2.5 | 44 se/12 wk | Cycling | Supramaximal SIT (SIT120) The total work done per training session was confined to 200 KJ 1-min exercise bouts at the work rate corresponding to 120% VO2peak, interspersed with 1.5-min passive recovery intervals | NR | DEXA | ||
| Zhang et al., 2021 (C) [64] | Obese young women | 25 13/12 | 20.4 ± 1.6 | 25.6 ± 2.3 | 44 se/12 wk | Cycling | Submaximal HIIT (HIIT90) The total work done per training session was confined to 200 KJ 4-min exercise bouts at the work rate corresponding to 90% VO2peak, interspersed with 3-min passive recovery intervals | NR | DEXA | ||
| Rentería et al., 2020 [65] | Healthy young adult women | 17 8/9 | 21.5 ± 1.2 | 24.1 ± 1.8 | 3 d/4 wk | Cycling | 3–5 sets × 30 s HIIT at 80% maximal aerobic power, followed by 4 min of recovery at 40% MAP | NR | NR | BIA | |
| Gahreman et al., 2016 (A) [73] | Overweight males | 24 12/12 | 26.1 + 0.7 | 27.9 ± 0.7 | 3 d/12 wk | Cycling | Green tea plus interval sprinting exercise (consumed three GT capsules daily) 60 sets of 8 s at 85% to 90% heart rate (high-intensity cycling) followed by 12 s of slow cycling recovery | NR | NR | DEXA | |
| Gahreman et al., 2016 (B) [73] | Overweight males | 24 12/12 | 26.1 + 0.7 | 29.09 ± 1.04 | 3 d/12 wk | Cycling | Interval sprinting exercise 5 min warm-up, 20 min of ISE, 5-min cool-down 60 sets of 8 s at 85% to 90% heart rate (high-intensity cycling) followed by 12 s of slow cycling recovery | NR | NR | DEXA | |
| Overground running | |||||||||||
| Ahmadizad et al., 2015 [48] | Sedentary overweight men | 20 10/10 | 25 ± 1 | 27.6 ± 1.9 | 3 d/6 wk | Overground running | Eight exercise intervals per session with 2–3 min of active rest (rest/exercise ratio was 2:1) 90% VO2max. | NR | NR | BIA | |
| Nybo et al., 2010 [46] | Untrained men | 19 11/8 | 33.5 ± 2.5 | NR | 3 d/12 wk | Overground running | Five intervals of 2 min of near-maximal running (HR above 95% of their HRmax at the end of the 2-min period) | NR | NR | DEXA | |
| Kazemi et al., 2015 [41] | Young wrestlers | 20 10/10 | 20–25 | NR | 3 d/6 wk | Overground running | 3 sets of RAST protocol (6 efforts in the 35 m distance followed by a 10 s rest interval after each effort) with 4 min rest after each set in the first week. Each week one set was added to the protocol for 4 weeks. | NR | NR | Caliper | |
| TaheriChadorneshin et al., 2019 [47] | Overweight, healthy, and young women | 28 14/14 | 30.03 ± 3.13 | 27.9 ± 2.9 | 3 d/8 wk | Overground running | 4–6 sets 30 s with maximum speed and then walked for 30 s. Training progression was implemented by increasing one repetition every 2 weeks and in the 6th week, it reached 6 repetitions | NR | NR | BIA | |
| Khammassi et al., 2018 [43] | Healthy untrained overweight/obese males | 20 | 18–21 | 29.1 ± 2.3 | 3 d/12 wk | Overground running | 30 s of work at 100% MAV interspersed by 30 s of active recovery at 50% MAV, starting with 15 repetitions to reach 27 by the end of the program | NR | NR | Caliper | |
| Chin et al., 2020 (A) [40] | Overweight or obese adults | 28 14/14 | 22.8 ± 3.1 | 26.4 ± 2.9 | 3 d/8 wk | Overground running | 12 bouts × 1 min of high-intensity exercise at 90% HRR and was interspersed with 11 bouts × 1 min of active recovery at 70% HRR. | BIA | |||
| Chin et al., 2020 (B) [40] | Overweight or obese adults | 24 14/10 | 22.8 ± 3.1 | 26.4 ± 2.9 | 2 d/8 wk | Overground running | 12 bouts × 1 min of high-intensity exercise at 90% HRR and was interspersed with 11 bouts × 1 min of active recovery at 70% HRR. | BIA | |||
| Chin et al., 2020 (C) [40] | Overweight or obese adults | 23 14/9 | 22.8 ± 3.1 | 26.4 ± 2.9 | 1 d/8 wk | Overground running | 12 bouts × 1 min of high-intensity exercise at 90% HRR and was interspersed with 11 bouts × 1 min of active recovery at 70% HRR. | BIA | |||
| Afzalpour et al., 2017 [31] | Overweight women | 20 10/10 | 21.1 ± 1.4 | 27.5 ±1.2 | 3 d/10 wk | Overground running | 4–8 sets 30 s at 85–95% HR max followed by 30 s active rest | NR | NR | Caliper | |
| Alizadeh et al., 2019 [38] | Overweight adolescent boys | 20 10/10 | 18 ± 1.5 | 27.6 ± 0.8 | 3 d/6 wk | Overground running | 4–6 sets 30 s at 90% of HR max followed by 30 s active rest | NR | NR | Caliper | |
| Azar et al., 2018 [39] | Sedentary young men | 18 9/9 | 23.8 ± 1.7 | 23.4 ± 2.4 | 3 d/6 wk | Overground running | Each session consisted of either four to six repeats of maximal sprint running within a 20 m area with 20–30 s recovery. | NR | NR | Caliper | |
| Mosallanezhad et al., 2014 [44] | Inactive normal young women | 21 10/11 | 23.8 ± 1.6 | 23.7 ± 4.3 | 3 d/8 wk | Overground running | 3–6 times of running with maximum speed in a 20-m area with 30 s rest from each other | NR | NR | NR | |
| Treadmill running | |||||||||||
| Tsekouras et al., 2008 [66] | Young nonobese men | 15 8/7 | 20–40 | 24.3 ± 0.9 | 3 d/8 wk | Treadmill | Subjects alternated four times between 4 min at 60% of pre-training VO2peak and 4 min at 90% of pre-training VO2peak for a total of 32 min | DEXA | |||
| Zhang et al., 2015 [45] | Overweight women | 23 11/12 | 20.9 ± 1 | 25.6 ± 2.1 | 4 d/12 wk | Treadmill | 4 × 4-min running at 85–95% HRpeak, interspersed by 3-min walking at 50–60% HRpeak | NR | BIA | ||
| GarcíaSuárez et al., 2020 [68] | Physically active male | 19 10/9 | 21.5 ± 1.6 | 22.8 ± 2.05 | 3 d/over 4 wk | Treadmill | The initial three sessions started with a 2 min run warm-up at 40% VO2peak. Then, a high-intensity interval was performed for 2 min at 100% VO2peak, for a total of three high-intensity and low-intensity bouts | NR | NR | BIA | |
| ZilaeiBouri et al., 2015 [67] | Obese and overweight female | 14 7/7 | 23.1 ± 2.6 | 29.1 ± 2.3 | 3 d/over 8 wk | Treadmill | 4 × 4 min intervals at 85–95% peak heart rate, separated by 3 × 3 min of active recovery at 50–70% peak heart rate | NR | |||
| Amaro-Gahete et al., 2019 [69] | Middle-aged adults men and women | 30 14/16 | 52.7 ± 4.9 | 26.5 ± 3.5 | 2 d/12 wk | Treadmill | The training volume was 40–65 min/week at >95% of the maximum oxygen uptake | NR | DEXA | ||
| Mirghani et al., 2015 (A) [74] | Overweight to obese low active volunteer women | 16 8/8 | 34 ± 5.3 | 30.1 ± 2.4 | 3 d/4 wk | Treadmill | 4–10 set 60/60 s activity-rest at 80% reserved heart rate | NR | NR | Caliper | |
| Mirghani et al., 2015 (B) [74] | Overweight to obese low active volunteer women | 16 8/8 | 33.5 ± 5.3 | 28.1 ± 2.2 | 3 d/4 wk | Treadmill | 4–10 set 60/30 s activity-rest at 80% reserved heart rate | NR | NR | Caliper | |
| Øvretveit et al., 2019 [71] | Active males | 12 6/6 | 30.3 ± 4.0 | NR | 2 d/6 wk | Treadmill | 4 × 4-min intervals at 85–95% of HRmax separated by 3 min of active recovery at 70% of HRmax on a Treadmill | NR | NR | BIA | |
| Galedari et al., 2017 [72] | 40 non-trained overweight men | 18 8/10 | 31.7 ± 7.2 | 29.4 ± 1.9 | 3 d/12 wk | Treadmill | 6–12 × 1 min intervals running on a Treadmill at 90–95% maximal heart rate with 1 min of active rest between the intervals | NR | NR | DEXA | |
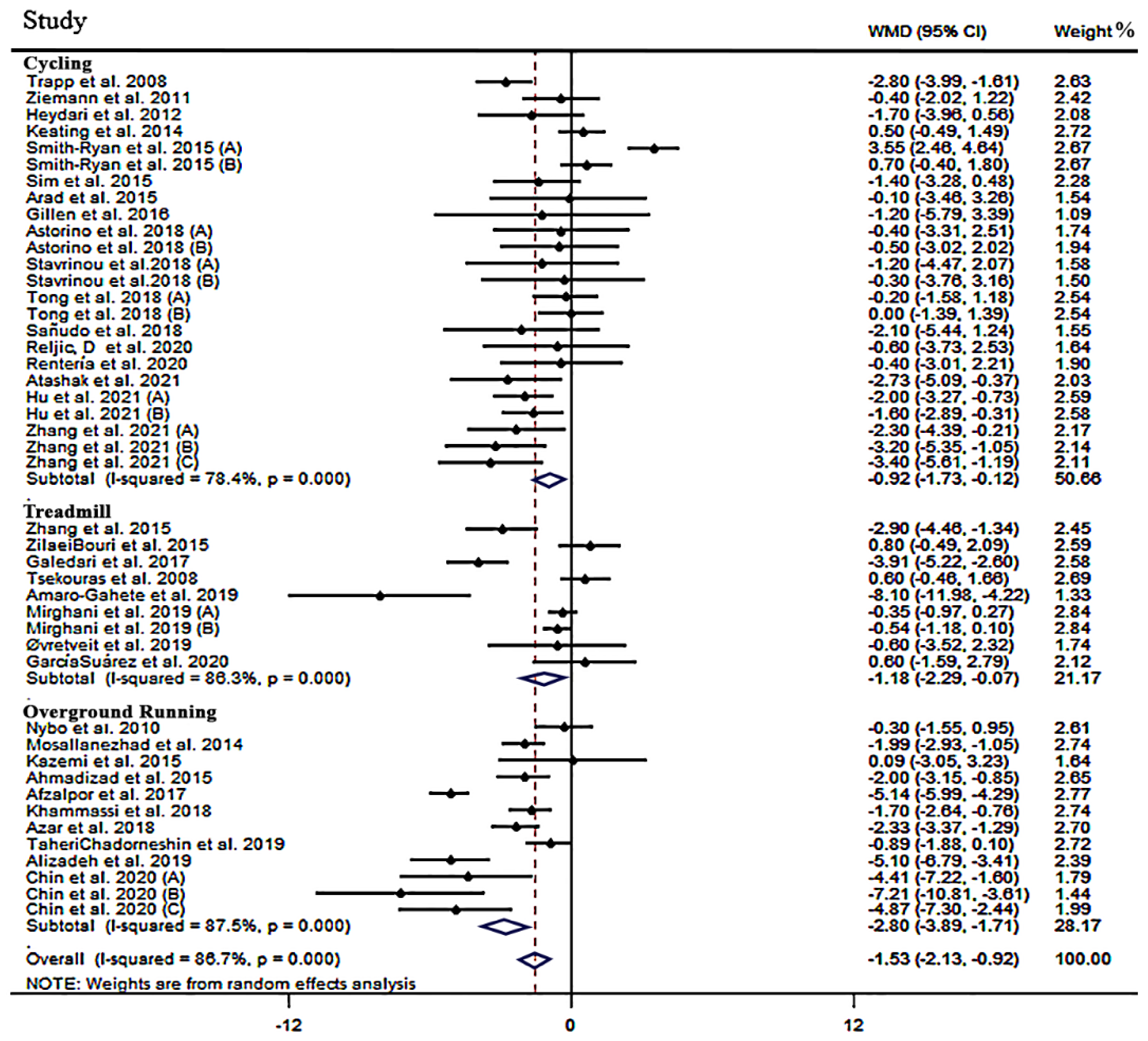
| BF% | ||||||
|---|---|---|---|---|---|---|
| Subcategories | Effect Size, n | I2 (%) | P-Heterogeneity | WMD | (95% CI) | p-Value |
| Type | ||||||
| Cycling | 24 | 78.4 | 0.001 | −0.92 | −1.73 to −0.12 | 0.025 |
| Overground Running | 12 | 87.5 | 0.001 | −2.80 | −3.89 to −1.71 | 0.001 |
| Treadmill Running | 9 | 86.3 | 0.001 | −1.18 | −2.29 to −0.07 | 0.037 |
| Pooled | 45 | 86.7 | 0.001 | −1.53 | −2.13 to −0.92 | 0.001 |
| Duration | ||||||
| ≤8 wk | 24 | 85.4 | 0.001 | −0.62 | −0.89 to −0.36 | 0.001 |
| >8 wk | 21 | 84.1 | 0.001 | −2.08 | −2.40 to −1.76 | 0.001 |
| Frequency | ||||||
| 2 sessions/wk | 5 | 79.0 | 0.001 | −3.23 | −6.52 to 0.04 | 0.054 |
| 3 sessions/wk | 33 | 88.7 | 0.001 | −1.17 | −1.85 to −0.50 | 0.001 |
| Time of training (per repetition) | ||||||
| ≤60 s | 27 | 89.4 | 0.001 | −1.87 | −2.78 to −0.96 | 0.001 |
| >60 s | 13 | 70.0 | 0.001 | −0.92 | −1.71 to −0.13 | 0.022 |
| Rest time | ||||||
| ≤90 s | 26 | 89.9 | 0.001 | −1.94 | −2.83 to −1.06 | 0.001 |
| >90 s | 13 | 66.3 | 0.001 | −1.01 | −1.84 to −0.10 | 0.017 |
| Active | 30 | 89.7 | 0.001 | −1.60 | −2.43 to −0.77 | 0.001 |
| Passive | 10 | 47.6 | 0.046 | −1.56 | −2.33 to −0.79 | 0.001 |
| Gender | ||||||
| Women | 17 | 87.8 | 0.001 | −1.44 | −1.72 to −1.17 | 0.001 |
| Men | 20 | 88.9 | 0.001 | −1.03 | −1.36 to −0.69 | 0.001 |
| BMI (kg·m−2) | ||||||
| <25 | 9 | 72.5 | 0.001 | −1.33 | −1.79 to −0.86 | 0.001 |
| 25–30 | 21 | 88.4 | 0.001 | −1.96 | −2.25 to −1.67 | 0.001 |
| >30 | 8 | 86.1 | 0.001 | 0.29 | −0.15 to 0.73 | 0.197 |
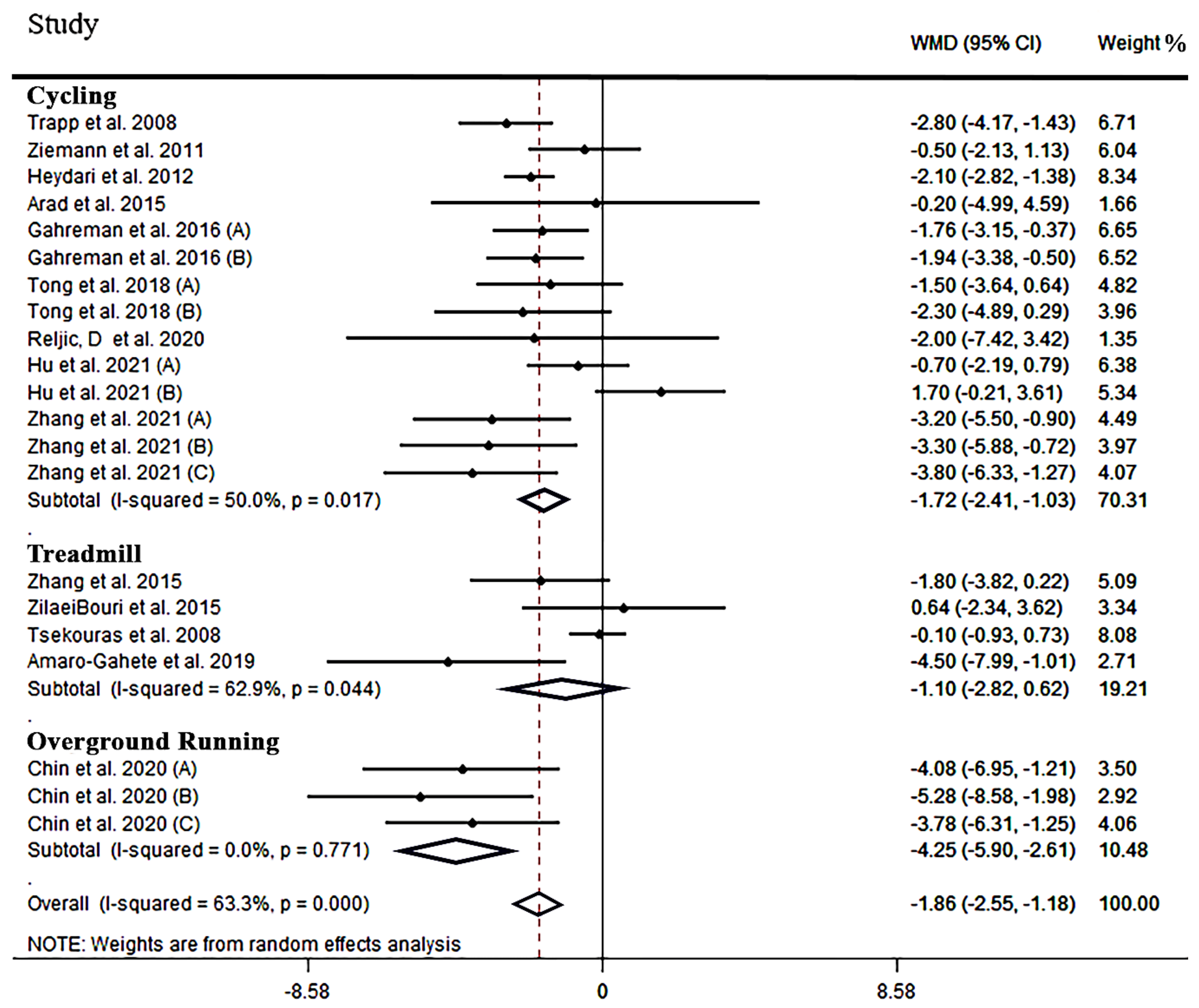
| FM (kg) | ||||||
| Subcategories | Effect Size, n | I2 (%) | P-Heterogeneity | WMD | (95% CI) | p-Value |
| Type | ||||||
| Cycling | 14 | 50.0 | 0.017 | −1.72 | −2.41 to −1.30 | 0.001 |
| Overground Running | 4 | 0.0 | 0.771 | −4.25 | −5.90 to −2.61 | 0.001 |
| Treadmill Running | 3 | 62.9 | 0.044 | −1.10 | −2.82 to 0.62 | 0.210 |
| Pooled | 21 | 63.3 | 0.001 | −1.86 | −2.55 to −1.18 | 0.001 |
| Durations | ||||||
| ≤8 wk | 6 | 76.4 | 0.001 | −0.80 | −1.46 to −0.14 | 0.018 |
| >8 wk | 15 | 45.1 | 0.030 | −1.92 | −2.35 to −1.50 | 0.001 |
| Frequency | ||||||
| 2 sessions/wk | 3 | 0.0 | 0.598 | −4.43 | −6.62 to −2.24 | 0.001 |
| 3 sessions/wk | 13 | 66.3 | 0.001 | −1.24 | −2.00 to −0.48 | 0.001 |
| Time of training (per repetition) | ||||||
| ≤60 s | 13 | 54.2 | 0.010 | −2.20 | −3.01 to −1.39 | 0.001 |
| >60 s | 6 | 52.1 | 0.064 | −1.14 | −2.13 to −0.15 | 0.023 |
| Rest time | ||||||
| ≤90 s | 12 | 57.0 | 0.007 | −2.26 | −3.08 to −1.43 | 0.001 |
| >90 s | 7 | 42.8 | 0.106 | −1.07 | −1.99 to −0.15 | 0.021 |
| Active | 11 | 64.4 | 0.002 | −2.13 | −2.99 to −1.27 | 0.001 |
| Passive | 8 | 65.5 | 0.005 | −1.52 | −2.77 to −0.27 | 0.017 |
| Gender | ||||||
| Women | 11 | 60.1 | 0.005 | −1.62 | −2.25 to −0.99 | 0.001 |
| Men | 8 | 73.8 | 0.001 | −1.53 | −1.97 to −1.08 | 0.001 |
| BMI (kg·m−2) | ||||||
| <25 | 3 | 81.9 | 0.004 | −0.78 | −1.43 to −0.13 | 0.019 |
| 25–30 | 14 | 62.0 | 0.001 | −1.97 | −2.42 to −1.52 | 0.001 |
| >30 | 2 | 0.0 | 0.626 | −0.99 | −4.58 to 2.60 | 0.589 |
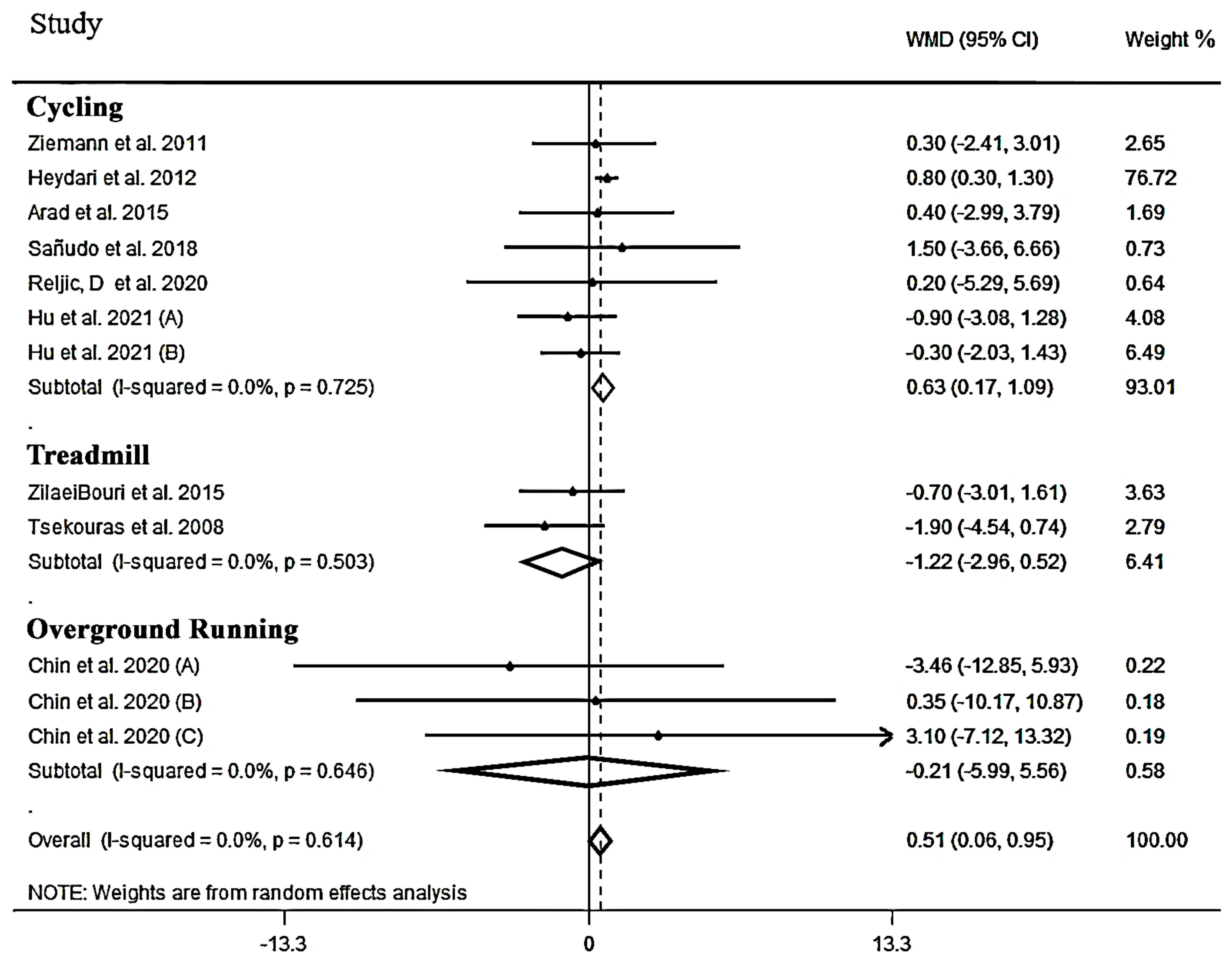
| FFM (kg) | ||||||
| Subcategories | Effect Size, n | I2 (%) | P−Heterogeneity | WMD | (95% CI) | p-Value |
| Type | ||||||
| Cycling | 7 | 0.0 | 0.725 | 0.63 | 0.17 to 1.09 | 0.007 |
| Overground Running | 3 | 0.0 | 0.646 | −0.21 | −5.99 to 5.56 | 0.942 |
| Treadmill Running | 2 | 0.0 | 0.503 | −1.22 | −2.96 to 0.52 | 0.169 |
| Pooled | 12 | 0.0 | 0.614 | 0.50 | 0.06 to 0.94 | 0.025 |
| Durations | ||||||
| ≤8 wk | 7 | 0.0 | 0.822 | −0.58 | −1.95 to 0.78 | 0.402 |
| >8 wk | 5 | 0.0 | 0.481 | 0.63 | 0.17 to 1.10 | 0.008 |
| Frequency | ||||||
| 2 sessions/wk | 2 | 0.0 | 0.980 | 0.23 | −4.63 to 5.10 | 0.926 |
| 3 sessions/wk | 9 | 9.4 | 0.357 | 0.50 | 0.06 to 0.94 | 0.026 |
| Time of training (per repetition) | ||||||
| ≤60 s | 8 | 0.0 | 0.923 | 0.57 | 0.29 to 1.44 | 0.003 |
| >60 s | 6 | 0.0 | 0.521 | −0.85 | −2.28 to 0.57 | 0.239 |
| Rest time | ||||||
| ≤90 s | 6 | 0.0 | 0.786 | 0.70 | 0.22 to 1.18 | 0.004 |
| >90 s | 5 | 0.0 | 0.664 | −0.53 | −1.81 to 0.73 | 0.410 |
| Active | 7 | 0.0 | 0.556 | 0.68 | 0.20 to 1.17 | 0.004 |
| Passive | 4 | 0.0 | 0.815 | −0.26 | −1.44 to 0.91 | 0.657 |
| Gender | ||||||
| Women | 4 | 0.0 | 0.924 | −0.47 | −1.58 to 0.63 | 0.404 |
| Men | 6 | 0.0 | 0.425 | 0.69 | 0.20 to 1.17 | 0.006 |
| BMI (kg·m−2) | ||||||
| <25 | 2 | 23.2 | 0.254 | −0.83 | −2.72 to 1.06 | 0.391 |
| 25–30 | 7 | 0.0 | 0.467 | − 0.58 | 0.12 to 1.04 | 0.014 |
| >30 | 3 | 0.0 | 0.928 | 0.62 | −1.90 to 3.14 | 0.629 |
| Quality Assessment | Summary of Findings | Quality of Evidence | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Outcomes | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Number of Intervention/Control | WMD (95% CI) | Heterogeneity (I2) | |
| BF% | No serious limitations | Very serious Limitations | No serious limitations | No serious limitations | No serious limitations | 527/555 | −1.53 (−2.13, −0.92) | 86.7% | ⊕⊕◯◯ Low |
| FM | No serious limitations | Serious Limitations | No serious limitations | No serious limitations | No serious limitations | 280/285 | −1.86 (−2.55,−1.18) | 63.3% | ⊕⊕⊕◯ Medium |
| FFM | No serious limitations | No serious limitations | No serious limitations | No serious limitations | No serious limitations | 165/162 | 0.51 (0.06, 0.95) | 0.0% | ⊕⊕⊕⊕ High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khodadadi, F.; Bagheri, R.; Negaresh, R.; Moradi, S.; Nordvall, M.; Camera, D.M.; Wong, A.; Suzuki, K. The Effect of High-Intensity Interval Training Type on Body Fat Percentage, Fat and Fat-Free Mass: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Clin. Med. 2023, 12, 2291. https://doi.org/10.3390/jcm12062291
Khodadadi F, Bagheri R, Negaresh R, Moradi S, Nordvall M, Camera DM, Wong A, Suzuki K. The Effect of High-Intensity Interval Training Type on Body Fat Percentage, Fat and Fat-Free Mass: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Journal of Clinical Medicine. 2023; 12(6):2291. https://doi.org/10.3390/jcm12062291
Chicago/Turabian StyleKhodadadi, Fatemeh, Reza Bagheri, Raoof Negaresh, Sajjad Moradi, Michael Nordvall, Donny M. Camera, Alexei Wong, and Katsuhiko Suzuki. 2023. "The Effect of High-Intensity Interval Training Type on Body Fat Percentage, Fat and Fat-Free Mass: A Systematic Review and Meta-Analysis of Randomized Clinical Trials" Journal of Clinical Medicine 12, no. 6: 2291. https://doi.org/10.3390/jcm12062291