
Adherence to Oral Antidiabetic Drugs in Patients with Type 2 Diabetes: Systematic Review and Meta-Analysis
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Information Sources and Search Strategy
2.4. Selection Process
2.5. Data Extraction Process
2.6. Risk of Bias (RoB) Assessment
2.7. Effect Measures
2.8. Synthesis Methods
3. Results
3.1. Systematic Review
3.2. Risk of Bias in Studies
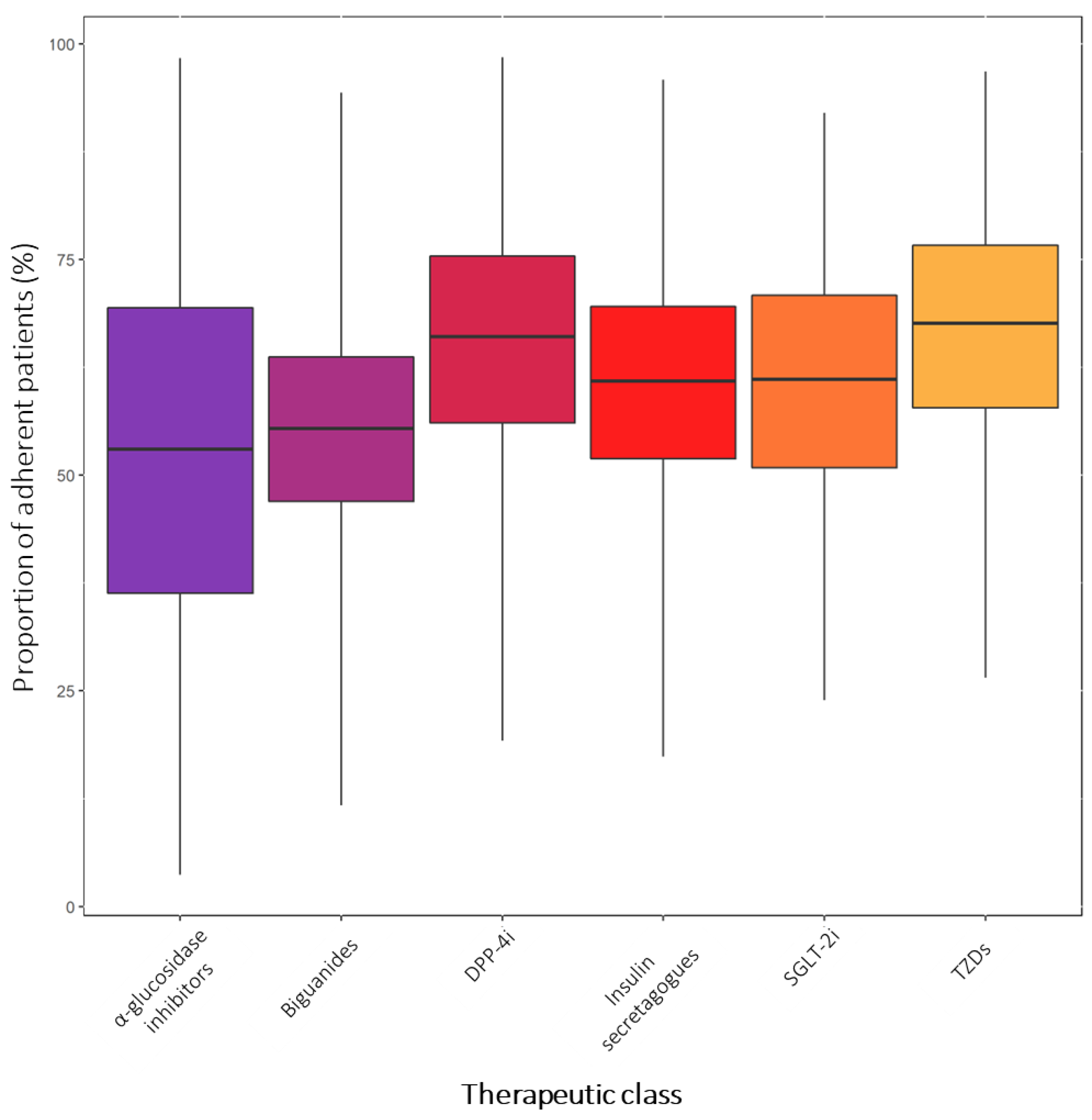
3.3. Proportion of Adherent Patients to Therapy with OADs
3.4. Stratified Analyses
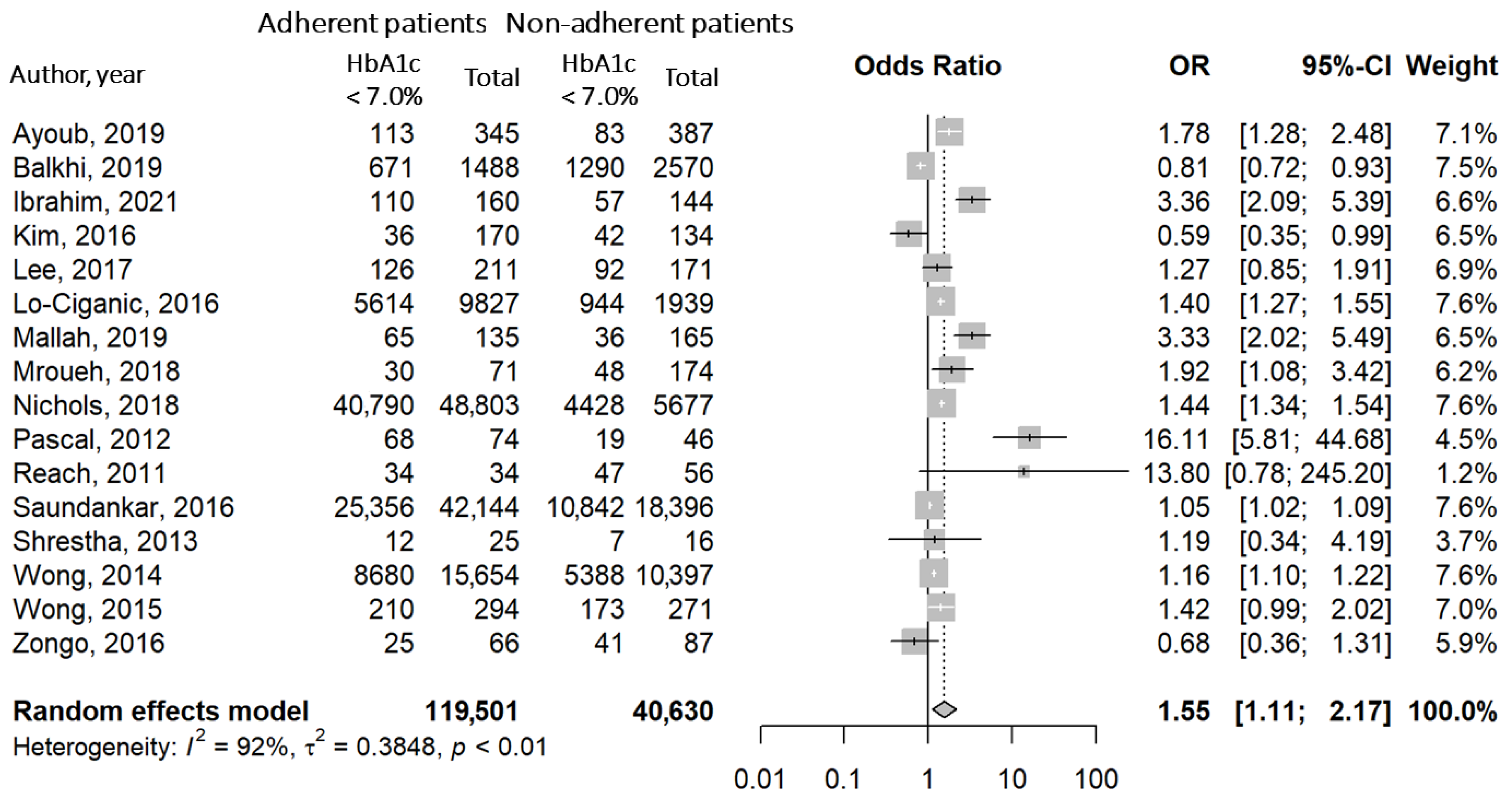
3.5. Association between Good Adherence and Blood Glucose Control
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.E.; Dorrance, K.A.; Oxenreiter, M.M.; Yan, K.R.; Close, K.L. The type 2 diabetes ‘modern preventable pandemic’ and replicable lessons from the COVID-19 crisis. Prev. Med. Rep. 2022, 25, 101636. [Google Scholar] [CrossRef]
- Lin, J.; Thompson, T.J.; Cheng, Y.J.; Zhuo, X.; Zhang, P.; Gregg, E.; Rolka, D.B. Projection of the future diabetes burden in the United States through 2060. Popul. Health Metr. 2018, 16, 9. [Google Scholar] [CrossRef] [Green Version]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [Green Version]
- Dal Canto, E.; Ceriello, A.; Ryden, L.; Ferrini, M.; Hansen, T.B.; Schnell, O.; Standl, E.; Beulens, J.W. Diabetes as a cardiovascular risk factor: An overview of global trends of macro and micro vascular complications. Eur. J. Prev. Cardiol. 2019, 26, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Harding, J.L.; Pavkov, M.E.; Magliano, D.J.; Shaw, J.E.; Gregg, E.W. Global trends in diabetes complications: A review of current evidence. Diabetologia 2019, 62, 3–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bommer, C.; Sagalova, V.; Heesemann, E.; Manne-Goehler, J.; Atun, R.; Barnighausen, T.; Davies, J.; Vollmer, S. Global Economic Burden of Diabetes in Adults: Projections From 2015 to 2030. Diabetes Care 2018, 41, 963–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Alles, B.; Debras, C.; Druesne-Pecollo, N.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultraprocessed Food Consumption and Risk of Type 2 Diabetes Among Participants of the NutriNet-Sante Prospective Cohort. JAMA Intern. Med. 2020, 180, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Wondmkun, Y.T. Obesity, Insulin Resistance, and Type 2 Diabetes: Associations and Therapeutic Implications. Diabetes Metab. Syndr. Obes. 2020, 13, 3611–3616. [Google Scholar] [CrossRef] [PubMed]
- Moradi, S.; Hojjati Kermani, M.A.; Bagheri, R.; Mohammadi, H.; Jayedi, A.; Lane, M.M.; Asbaghi, O.; Mehrabani, S.; Suzuki, K. Ultra-Processed Food Consumption and Adult Diabetes Risk: A Systematic Review and Dose-Response Meta-Analysis. Nutrients 2021, 13, 4410. [Google Scholar] [CrossRef] [PubMed]
- Hamburg, N.M.; McMackin, C.J.; Huang, A.L.; Shenouda, S.M.; Widlansky, M.E.; Schulz, E.; Gokce, N.; Ruderman, N.B.; Keaney, J.F., Jr.; Vita, J.A. Physical inactivity rapidly induces insulin resistance and microvascular dysfunction in healthy volunteers. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2650–2656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S111–S124. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Myers, R.; Li, Y.; Chen, Y.; Shen, X.; Fenyk-Melody, J.; Wu, M.; Ventre, J.; Doebber, T.; Fujii, N.; et al. Role of AMP-activated protein kinase in mechanism of metformin action. J. Clin. Investig. 2001, 108, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Moin, T.; Schmittdiel, J.A.; Flory, J.H.; Yeh, J.; Karter, A.J.; Kruge, L.E.; Schillinger, D.; Mangione, C.M.; Herman, W.H.; Walker, E.A. Review of Metformin Use for Type 2 Diabetes Prevention. Am. J. Prev. Med. 2018, 55, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Gebregergish, S.B.; Hashim, M.; Heeg, B.; Wilke, T.; Rauland, M.; Hostalek, U. The cost-effectiveness of metformin in pre-diabetics: A systematic literature review of health economic evaluations. Expert Rev. Pharmacoecon. Outcomes Res. 2020, 20, 207–219. [Google Scholar] [CrossRef]
- Lv, W.; Wang, X.; Xu, Q.; Lu, W. Mechanisms and Characteristics of Sulfonylureas and Glinides. Curr. Top. Med. Chem. 2020, 20, 37–56. [Google Scholar] [CrossRef]
- Rizos, C.V.; Kei, A.; Elisaf, M.S. The current role of thiazolidinediones in diabetes management. Arch. Toxicol. 2016, 90, 1861–1881. [Google Scholar] [CrossRef]
- Lebovitz, H.E. Thiazolidinediones: The Forgotten Diabetes Medications. Curr. Diabetes Rep. 2019, 19, 151. [Google Scholar] [CrossRef] [Green Version]
- Derosa, G.; Maffioli, P. alpha-Glucosidase inhibitors and their use in clinical practice. Arch. Med. Sci. 2012, 8, 899–906. [Google Scholar] [CrossRef]
- Simes, B.C.; MacGregor, G.G. Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors: A Clinician’s Guide. Diabetes Metab. Syndr. Obes. 2019, 12, 2125–2136. [Google Scholar] [CrossRef] [Green Version]
- Scheen, A.J. DPP-4 inhibitors in the management of type 2 diabetes: A critical review of head-to-head trials. Diabetes Metab. 2012, 38, 89–101. [Google Scholar] [CrossRef]
- Williams, D.M.; Jones, H.; Stephens, J.W. Personalized Type 2 Diabetes Management: An Update on Recent Advances and Recommendations. Diabetes Metab. Syndr. Obes. 2022, 15, 281–295. [Google Scholar] [CrossRef]
- Polonsky, W.H.; Henry, R.R. Poor medication adherence in type 2 diabetes: Recognizing the scope of the problem and its key contributors. Patient Prefer. Adherence 2016, 10, 1299–1307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- McGovern, A.; Tippu, Z.; Hinton, W.; Munro, N.; Whyte, M.; de Lusignan, S. Comparison of medication adherence and persistence in type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2018, 20, 1040–1043. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Brooks, P.; Woolf, A.; Blyth, F.; March, L.; Bain, C.; Baker, P.; Smith, E.; Buchbinder, R. Assessing risk of bias in prevalence studies: Modification of an existing tool and evidence of interrater agreement. J. Clin. Epidemiol. 2012, 65, 934–939. [Google Scholar] [CrossRef]
- Piragine, E.; Petri, D.; Martelli, A.; Janowska, A.; Dini, V.; Romanelli, M.; Calderone, V.; Lucenteforte, E. Adherence and Persistence to Biological Drugs for Psoriasis: Systematic Review with Meta-Analysis. J. Clin. Med. 2022, 11, 1506. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rucker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid.-Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions, version 6.3 (updated February 2022); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 7 December 2022).
- Abdullah, N.F.; Khuan, L.; Theng, C.A.; Sowtali, S.N.; Juni, M.H. Effect of patient characteristics on medication adherence among patients with type 2 diabetes mellitus: A cross-sectional survey. Contemp. Nurse 2019, 55, 27–37. [Google Scholar] [CrossRef]
- Acharya, A.S.; Gupta, E.; Prakash, A.; Singhal, N. Self-reported Adherence to Medication among Patients with Type II Diabetes Mellitus attending a Tertiary Care Hospital of Delhi. J. Assoc. Physicians India 2019, 67, 26–29. [Google Scholar]
- Adisa, R.; Fakeye, T.O. Effect of number and type of antidiabetes medications on adherence and glycemia of ambulatory type 2 diabetes patients in southwestern Nigeria. Pharm. Pract. (Granada) 2013, 11, 156–165. [Google Scholar] [CrossRef] [Green Version]
- Aditama, L.; Athiyah, U.; Utami, W.; Rahem, A. Adherence behavior assessment of oral antidiabetic medication use: A study of patient decisions in long-term disease management in primary health care centers in Surabaya. J. Basic Clin. Physiol. Pharmacol. 2020, 30, 20190257. [Google Scholar] [CrossRef] [PubMed]
- Afaya, R.A.; Bam, V.; Azongo, T.B.; Afaya, A.; Kusi-Amponsah, A.; Ajusiyine, J.M.; Abdul Hamid, T. Medication adherence and self-care behaviours among patients with type 2 diabetes mellitus in Ghana. PLoS ONE 2020, 15, e0237710. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.S.; Ramli, A.; Islahudin, F.; Paraidathathu, T. Medication adherence in patients with type 2 diabetes mellitus treated at primary health clinics in Malaysia. Patient Prefer. Adherence 2013, 7, 525–530. [Google Scholar] [CrossRef] [Green Version]
- Aloudah, N.M.; Scott, N.W.; Aljadhey, H.S.; Araujo-Soares, V.; Alrubeaan, K.A.; Watson, M.C. Medication adherence among patients with Type 2 diabetes: A mixed methods study. PLoS ONE 2018, 13, e0207583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlQarni, K.; AlQarni, E.A.; Naqvi, A.A.; AlShayban, D.M.; Ghori, S.A.; Haseeb, A.; Raafat, M.; Jamshed, S. Assessment of Medication Adherence in Saudi Patients With Type II Diabetes Mellitus in Khobar City, Saudi Arabia. Front. Pharmacol. 2019, 10, 1306. [Google Scholar] [CrossRef] [Green Version]
- Aminde, L.N.; Tindong, M.; Ngwasiri, C.A.; Aminde, J.A.; Njim, T.; Fondong, A.A.; Takah, N.F. Adherence to antidiabetic medication and factors associated with non-adherence among patients with type-2 diabetes mellitus in two regional hospitals in Cameroon. BMC Endocr. Disord. 2019, 19, 35. [Google Scholar] [CrossRef] [Green Version]
- Andanalusia, M.; Athiyah, U.; Nita, Y. Medication adherence in diabetes mellitus patients at Tanjung Karang Primary Health Care Center, Mataram. J. Basic Clin. Physiol. Pharmacol. 2019, 30, 20190287. [Google Scholar] [CrossRef]
- Ashur, S.T.; Shah, S.A.; Bosseri, S.; Morisky, D.E.; Shamsuddin, K. Illness perceptions of Libyans with T2DM and their influence on medication adherence: A study in a diabetes center in Tripoli. Libyan. J. Med. 2015, 10, 29797. [Google Scholar] [CrossRef]
- Ayoub, D.; Mroueh, L.; El-Hajj, M.; Awada, S.; Rachidi, S.; Zein, S.; Al-Hajje, A. Evaluation of antidiabetic medication adherence in the Lebanese population: Development of the Lebanese Diabetes Medication Adherence Scale. Int. J. Pharm. Pract. 2019, 27, 468–476. [Google Scholar] [CrossRef]
- Balkhi, B.; Alwhaibi, M.; Alqahtani, N.; Alhawassi, T.; Alshammari, T.M.; Mahmoud, M.; Almetwazi, M.; Ata, S.; Kamal, K.M. Oral antidiabetic medication adherence and glycaemic control among patients with type 2 diabetes mellitus: A cross-sectional retrospective study in a tertiary hospital in Saudi Arabia. BMJ Open 2019, 9, e029280. [Google Scholar] [CrossRef] [Green Version]
- Basak, R.; McCaffrey Iii, D.J.; Bentley, J.P.; Przybyla, S.M.; West-Strum, D.; Banahan, B.F. Adherence to multiple medications prescribed for a chronic disease: A methodological investigation. J. Manag. Care Spec. Pharm. 2014, 20, 815–823. [Google Scholar] [CrossRef]
- Bell, K.F.; Cappell, K.; Liang, M.; Kong, A.M. Comparing Medication Adherence and Persistence Among Patients with Type 2 Diabetes Using Sodium-Glucose Cotransporter 2 Inhibitors or Sulfonylureas. Am. Health Drug Benefits 2017, 10, 165–174. [Google Scholar] [PubMed]
- Bloomgarden, Z.T.; Tunceli, K.; Liu, J.; Brodovicz, K.G.; Mavros, P.; Engel, S.S.; Radican, L.; Chen, Y.; Rajpathak, S.; Qiu, Y.; et al. Adherence, persistence, and treatment discontinuation with sitagliptin compared with sulfonylureas as add-ons to metformin: A retrospective cohort database study. J. Diabetes 2017, 9, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Bonger, Z.; Shiferaw, S.; Tariku, E.Z. Adherence to diabetic self-care practices and its associated factors among patients with type 2 diabetes in Addis Ababa, Ethiopia. Patient Prefer. Adherence 2018, 12, 963–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, S.P.; Acheampong, F.; Kretchy, I. Adherence to oral anti-diabetic drugs among patients attending a Ghanaian teaching hospital. Pharm. Pract. 2015, 13, 533. [Google Scholar] [CrossRef] [Green Version]
- Bryson, C.L.; Au, D.H.; Maciejewski, M.L.; Piette, J.D.; Fihn, S.D.; Jackson, G.L.; Perkins, M.; Wong, E.S.; Yano, E.M.; Liu, C.F. Wide clinic-level variation in adherence to oral diabetes medications in the VA. J. Gen. Intern. Med. 2013, 28, 698–705. [Google Scholar] [CrossRef] [Green Version]
- Buysman, E.K.; Anderson, A.; Bacchus, S.; Ingham, M. Retrospective Study on the Impact of Adherence in Achieving Glycemic Goals in Type 2 Diabetes Mellitus Patients Receiving Canagliflozin. Adv. Ther. 2017, 34, 937–953. [Google Scholar] [CrossRef]
- Cai, J.; Wang, Y.; Baser, O.; Xie, L.; Chow, W. Comparative persistence and adherence with newer anti-hyperglycemic agents to treat patients with type 2 diabetes in the United States. J. Med. Econ. 2016, 19, 1175–1186. [Google Scholar] [CrossRef]
- Cai, J.; Divino, V.; Burudpakdee, C. Adherence and persistence in patients with type 2 diabetes mellitus newly initiating canagliflozin, dapagliflozin, dpp-4s, or glp-1s in the United States. Curr. Med. Res. Opin. 2017, 33, 1317–1328. [Google Scholar] [CrossRef]
- Carls, G.S.; Tan, R.; Zhu, J.Y.; Tuttle, E.; Yee, J.; Edelman, S.V.; Polonsky, W.H. Real-world weight change among patients treated with glucagon-like peptide-1 receptor agonist, dipeptidyl peptidase-4 inhibitor and sulfonylureas for type 2 diabetes and the influence of medication adherence. Obes. Sci. Pract. 2017, 3, 342–351. [Google Scholar] [CrossRef]
- Carls, G.S.; Tuttle, E.; Tan, R.D.; Huynh, J.; Yee, J.; Edelman, S.V.; Polonsky, W.H. Understanding the Gap Between Efficacy in Randomized Controlled Trials and Effectiveness in Real-World Use of GLP-1 RA and DPP-4 Therapies in Patients With Type 2 Diabetes. Diabetes Care 2017, 40, 1469–1478. [Google Scholar] [CrossRef] [Green Version]
- Chang, P.Y.; Chien, L.N.; Lin, Y.F.; Chiou, H.Y.; Chiu, W.T. Nonadherence of Oral Antihyperglycemic Medication Will Increase Risk of End-Stage Renal Disease. Medicine 2015, 94, e2051. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Tseng, C.H.; Cheng, S.H. Continuity of care, medication adherence, and health care outcomes among patients with newly diagnosed type 2 diabetes: A longitudinal analysis. Med. Care 2013, 51, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Cheng, S.H. Continuity of care and changes in medication adherence among patients with newly diagnosed diabetes. Am. J. Manag. Care 2016, 22, 136–142. [Google Scholar] [PubMed]
- Cheng, S.H.; Chen, C.C.; Tseng, C.H. Does medication adherence lead to lower healthcare expenses for patients with diabetes? Am. J. Manag. Care 2013, 19, 662–670. [Google Scholar] [PubMed]
- Chepulis, L.; Mayo, C.; Morison, B.; Keenan, R.; Lao, C.; Paul, R.; Lawrenson, R. Metformin adherence in patients with type 2 diabetes and its association with glycated haemoglobin levels. J. Prim. Health Care 2020, 12, 318–326. [Google Scholar] [CrossRef]
- Chew, B.H.; Hassan, N.H.; Sherina, M.S. Determinants of medication adherence among adults with type 2 diabetes mellitus in three Malaysian public health clinics: A cross-sectional study. Patient Prefer. Adherence 2015, 9, 639–648. [Google Scholar] [CrossRef] [Green Version]
- Chong, E.; Wang, H.; King-Shier, K.M.; Quan, H.; Rabi, D.M.; Khan, N.A. Prescribing patterns and adherence to medication among South-Asian, Chinese and white people with type 2 diabetes mellitus: A population-based cohort study. Diabet. Med. 2014, 31, 1586–1593. [Google Scholar] [CrossRef]
- de Vries, S.T.; Keers, J.C.; Visser, R.; de Zeeuw, D.; Haaijer-Ruskamp, F.M.; Voorham, J.; Denig, P. Medication beliefs, treatment complexity, and non-adherence to different drug classes in patients with type 2 diabetes. J. Psychosom. Res. 2014, 76, 134–138. [Google Scholar] [CrossRef] [Green Version]
- Degefa, G.; Wubshet, K.; Tesfaye, S.; Hirigo, A.T. Predictors of Adherence Toward Specific Domains of Diabetic Self-Care Among Type-2 Diabetes Patients. Clin. Med. Insights Endocrinol. Diabetes 2020, 13, 1179551420981909. [Google Scholar] [CrossRef]
- Dossa, A.R.; Gregoire, J.P.; Lauzier, S.; Guenette, L.; Sirois, C.; Moisan, J. Association Between Loyalty to Community Pharmacy and Medication Persistence and Compliance, and the Use of Guidelines-Recommended Drugs in Type 2 Diabetes: A Cohort Study. Medicine 2015, 94, e1082. [Google Scholar] [CrossRef] [PubMed]
- Elsous, A.; Radwan, M.; Al-Sharif, H.; Abu Mustafa, A. Medications Adherence and Associated Factors among Patients with Type 2 Diabetes Mellitus in the Gaza Strip, Palestine. Front. Endocrinol. 2017, 8, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fai, E.K.; Anderson, C.; Ferreros, V. Role of attitudes and intentions in predicting adherence to oral diabetes medications. Endocr. Connect. 2017, 6, 63–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farmer, A.J.; Rodgers, L.R.; Lonergan, M.; Shields, B.; Weedon, M.N.; Donnelly, L.; Holman, R.R.; Pearson, E.R.; Hattersley, A.T. Adherence to Oral Glucose-Lowering Therapies and Associations With 1-Year HbA1c: A Retrospective Cohort Analysis in a Large Primary Care Database. Diabetes Care 2016, 39, 258–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farr, A.M.; Sheehan, J.J.; Curkendall, S.M.; Smith, D.M.; Johnston, S.S.; Kalsekar, I. Retrospective analysis of long-term adherence to and persistence with DPP-4 inhibitors in US adults with type 2 diabetes mellitus. Adv. Ther. 2014, 31, 1287–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farr, A.M.; Sheehan, J.J.; Davis, B.M.; Smith, D.M. Comparison of adherence and persistence among adults with type 2 diabetes mellitus initiating saxagliptin or linagliptin. Patient Prefer. Adherence 2016, 10, 1471–1479. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.L.; Castaneda, S.F.; Allison, M.A.; Elder, J.P.; Talavera, G.A. Correlates of low-adherence to oral hypoglycemic medications among Hispanic/Latinos of Mexican heritage with Type 2 Diabetes in the United States. Diabetes Res. Clin. Pract. 2019, 155, 107692. [Google Scholar] [CrossRef]
- Gatwood, J.; Hohmeier, K.C.; Shuvo, S.; Mikaiel, D.; Kovesdy, C.P. Alignment of diagnosis and pharmacy claims data coding of medication adherence among patients with diabetes or hypertension. J. Manag. Care Spec. Pharm. 2021, 27, 497–506. [Google Scholar] [CrossRef]
- Gatwood, J.D.; Chisholm-Burns, M.; Davis, R.; Thomas, F.; Potukuchi, P.; Hung, A.; Kovesdy, C.P. Differences in health outcomes associated with initial adherence to oral antidiabetes medications among veterans with uncomplicated Type 2 diabetes: A 5-year survival analysis. Diabet. Med. 2018, 35, 1571–1579. [Google Scholar] [CrossRef]
- Gatwood, J.D.; Chisholm-Burns, M.; Davis, R.; Thomas, F.; Potukuchi, P.; Hung, A.; Kovesdy, C.P. Disparities in Initial Oral Antidiabetic Medication Adherence Among Veterans with Incident Diabetes. J. Manag. Care Spec. Pharm. 2018, 24, 379–389. [Google Scholar] [CrossRef]
- Gordon, J.; McEwan, P.; Idris, I.; Evans, M.; Puelles, J. Treatment choice, medication adherence and glycemic efficacy in people with type 2 diabetes: A UK clinical practice database study. BMJ Open Diabetes Res. Care 2018, 6, e000512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graetz, I.; Huang, J.; Muelly, E.R.; Fireman, B.; Hsu, J.; Reed, M.E. Association of Mobile Patient Portal Access With Diabetes Medication Adherence and Glycemic Levels Among Adults With Diabetes. JAMA Netw. Open 2020, 3, e1921429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guenette, L.; Moisan, J.; Breton, M.C.; Sirois, C.; Gregoire, J.P. Difficulty adhering to antidiabetic treatment: Factors associated with persistence and compliance. Diabetes Metab. 2013, 39, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Guenette, L.; Lauzier, S.; Guillaumie, L.; Giguere, G.; Gregoire, J.P.; Moisan, J. Patients’ beliefs about adherence to oral antidiabetic treatment: A qualitative study. Patient Prefer. Adherence 2015, 9, 413–420. [Google Scholar] [CrossRef] [Green Version]
- Guenette, L.; Breton, M.C.; Guillaumie, L.; Lauzier, S.; Gregoire, J.P.; Moisan, J. Psychosocial factors associated with adherence to non-insulin antidiabetes treatments. J. Diabetes Complicat. 2016, 30, 335–342. [Google Scholar] [CrossRef]
- Hagen, S.E.; Wright, D.W.; Finch, R.; Talamonti, W.J.; Edington, D.W. Impact of compliance to oral hypoglycemic agents on short-term disability costs in an employer population. Popul. Health Manag. 2014, 17, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Haines, L.; Coppa, N.; Harris, Y.; Wisnivesky, J.P.; Lin, J.J. The Impact of Partnership Status on Diabetes Control and Self-Management Behaviors. Health Educ. Behav. 2018, 45, 668–671. [Google Scholar] [CrossRef]
- Hansen, R.A.; Voils, C.I.; Farley, J.F.; Powers, B.J.; Sanders, L.L.; Sleath, B.; Maciejewski, M.L. Prescriber continuity and medication adherence for complex patients. Ann. Pharmacother. 2015, 49, 293–302. [Google Scholar] [CrossRef]
- Hayashi, I.; Watanabe, N.; Nakata, S.; Komatsu, R.; Motoda, S.; Fujita, Y.; Ishibashi, C.; Yamaguchi Baden, M.; Kimura, T.; Takahara, M.; et al. Factors associated with treatment satisfaction in patients with type 2 diabetes mellitus using oral glucose-lowering agents: A cross-sectional study in urban districts in Japan. Endocr. J. 2018, 65, 1001–1009. [Google Scholar] [CrossRef] [Green Version]
- Hedna, K.; Hagg, S.; Andersson Sundell, K.; Petzold, M.; Hakkarainen, K.M. Refill adherence and self-reported adverse drug reactions and sub-therapeutic effects: A population-based study. Pharmacoepidemiol. Drug Saf. 2013, 22, 1317–1325. [Google Scholar] [CrossRef] [Green Version]
- Heissam, K.; Abuamer, Z.; El-Dahshan, N. Patterns and obstacles to oral antidiabetic medications adherence among type 2 diabetics in Ismailia, Egypt: A cross section study. Pan Afr. Med. J. 2015, 20, 177. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.S.; Kang, H.C. Relationship between continuity of ambulatory care and medication adherence in adult patients with type 2 diabetes in Korea: A longitudinal analysis. Med. Care 2014, 52, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Horii, T.; Momo, K.; Yasu, T.; Kabeya, Y.; Atsuda, K. Determination of factors affecting medication adherence in type 2 diabetes mellitus patients using a nationwide claim-based database in Japan. PLoS ONE 2019, 14, e0223431. [Google Scholar] [CrossRef] [Green Version]
- Horsburgh, S.; Barson, D.; Zeng, J.; Sharples, K.; Parkin, L. Adherence to metformin monotherapy in people with type 2 diabetes mellitus in New Zealand. Diabetes Res. Clin. Pract. 2019, 158, 107902. [Google Scholar] [CrossRef] [PubMed]
- Horvat, O.; Poprzen, J.; Tomas, A.; Paut Kusturica, M.; Tomic, Z.; Sabo, A. Factors associated with non-adherence among type 2 diabetic patients in primary care setting in eastern Bosnia and Herzegovina. Prim. Care Diabetes 2018, 12, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Huber, C.A.; Rapold, R.; Brungger, B.; Reich, O.; Rosemann, T. One-year adherence to oral antihyperglycemic medication and risk prediction of patient outcomes for adults with diabetes mellitus: An observational study. Medicine 2016, 95, e3994. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, L.; Ibrahim, L.; Hallit, S.; Salameh, P.; Sacre, H.; Akel, M.; Bou Serhal, R.; Saleh, N. Validation of the Lebanese Medication Adherence Scale among Lebanese diabetic patients. Int. J. Clin. Pharm. 2021, 43, 918–927. [Google Scholar] [CrossRef]
- Iyengar, R.N.; Balagere, D.S.; Henderson, R.R.; LeFrancois, A.L.; Rabbitt, R.M.; Frazee, S.G. Association between dispensing channel and medication adherence among medicare beneficiaries taking medications to treat diabetes, high blood pressure, or high blood cholesterol. J. Manag. Care Spec. Pharm. 2014, 20, 851–861. [Google Scholar] [CrossRef]
- Iyengar, R.N.; LeFrancois, A.L.; Henderson, R.R.; Rabbitt, R.M. Medication Nonadherence Among Medicare Beneficiaries with Comorbid Chronic Conditions: Influence of Pharmacy Dispensing Channel. J. Manag. Care Spec. Pharm. 2016, 22, 550–560. [Google Scholar] [CrossRef]
- Jamous, R.M.; Sweileh, W.M.; Abu-Taha, A.S.; Sawalha, A.F.; Zyoud, S.H.; Morisky, D.E. Adherence and satisfaction with oral hypoglycemic medications: A pilot study in Palestine. Int. J. Clin. Pharm. 2011, 33, 942–948. [Google Scholar] [CrossRef]
- Jannuzzi, F.F.; Rodrigues, R.C.; Cornelio, M.E.; Sao-Joao, T.M.; Gallani, M.C. Beliefs related to adherence to oral antidiabetic treatment according to the Theory of Planned Behavior. Rev. Lat.-Am. Enferm. 2014, 22, 529–537. [Google Scholar] [CrossRef] [Green Version]
- Jannuzzi, F.F.; Cornelio, M.E.; Sao-Joao, T.M.; Gallani, M.C.; Godin, G.; Rodrigues, R.C.M. Psychosocial determinants of adherence to oral antidiabetic medication among people with type 2 diabetes. J. Clin. Nurs. 2020, 29, 909–921. [Google Scholar] [CrossRef] [PubMed]
- Jarab, A.S.; Almrayat, R.; Alqudah, S.; Thehairat, E.; Mukattash, T.L.; Khdour, M.; Pinto, S. Predictors of non-adherence to pharmacotherapy in patients with type 2 diabetes. Int. J. Clin. Pharm. 2014, 36, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Babazono, A.; Fujita, T. Health Inequalities Among Elderly Type 2 Diabetes Mellitus Patients in Japan. Popul. Health Manag. 2020, 23, 264–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kharjul, M.D.; Cameron, C.; Braund, R. Using the Pharmaceutical Collection Database to identify patient adherence to oral hypoglycaemic medicines. J. Prim. Health Care 2019, 11, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.Y.; Lee, J.S.; Kang, H.J.; Park, S.M. Effect of medication adherence on long-term all-cause-mortality and hospitalization for cardiovascular disease in 65,067 newly diagnosed type 2 diabetes patients. Sci. Rep. 2018, 8, 12190. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.J.; Park, E.; Schlenk, E.A.; Kim, M.; Kim, D.J. Psychometric Evaluation of a Korean Version of the Adherence to Refills and Medications Scale (ARMS) in Adults With Type 2 Diabetes. Diabetes Educ. 2016, 42, 188–198. [Google Scholar] [CrossRef]
- Koyanagi, K.; Kubota, T.; Kobayashi, D.; Kihara, T.; Yoshida, T.; Miisho, T.; Miura, T.; Sakamoto, Y.; Takaki, J.; Seo, T.; et al. Prescription Factors Associated with Medication Non-adherence in Japan Assessed from Leftover Drugs in the SETSUYAKU-BAG Campaign: Focus on Oral Antidiabetic Drugs. Front. Pharmacol. 2016, 7, 212. [Google Scholar] [CrossRef] [Green Version]
- Kumar, K.M.P.; Chawla, M.; Sanghvi, A.; Sastry, N.G.; Kotla, C.; Phatak, S.; Choudhari, S. Adherence, satisfaction, and experience with metformin 500 mg prolonged release formulation in Indian patients with type 2 diabetes mellitus: A postmarketing observational study. Int. J. Gen. Med. 2019, 12, 147–159. [Google Scholar] [CrossRef] [Green Version]
- Kurtyka, K.; Nishikino, R.; Ito, C.; Brodovicz, K.; Chen, Y.; Tunceli, K. Adherence to dipeptidyl peptidase-4 inhibitor therapy among type 2 diabetes patients with employer-sponsored health insurance in Japan. J. Diabetes Investig. 2016, 7, 737–743. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.S.; Tan, J.H.M.; Sankari, U.; Koh, Y.L.E.; Tan, N.C. Assessing oral medication adherence among patients with type 2 diabetes mellitus treated with polytherapy in a developed Asian community: A cross-sectional study. BMJ Open 2017, 7, e016317. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.Y.; Ahn, J.; Kim, J.H.; Hong, Y.P.; Hong, S.K.; Kim, Y.T.; Lee, S.H.; Morisky, D.E. Reliability and validity of a self-reported measure of medication adherence in patients with type 2 diabetes mellitus in Korea. J. Int. Med. Res. 2013, 41, 1098–1110. [Google Scholar] [CrossRef] [Green Version]
- Leporini, C.; Piro, R.; Ursini, F.; Maida, F.; Palleria, C.; Arturi, F.; Pavia, M.; De Sarro, G.; Russo, E. Monitoring safety and use of old and new treatment options for type 2 diabetic patients: A two-year (2013–2016) analysis. Expert. Opin. Drug Saf. 2016, 15, 17–34. [Google Scholar] [CrossRef]
- Lo-Ciganic, W.H.; Donohue, J.M.; Jones, B.L.; Perera, S.; Thorpe, J.M.; Thorpe, C.T.; Marcum, Z.A.; Gellad, W.F. Trajectories of Diabetes Medication Adherence and Hospitalization Risk: A Retrospective Cohort Study in a Large State Medicaid Program. J. Gen. Intern. Med. 2016, 31, 1052–1060. [Google Scholar] [CrossRef] [Green Version]
- Lo-Ciganic, W.H.; Donohue, J.M.; Thorpe, J.M.; Perera, S.; Thorpe, C.T.; Marcum, Z.A.; Gellad, W.F. Using machine learning to examine medication adherence thresholds and risk of hospitalization. Med. Care 2015, 53, 720–728. [Google Scholar] [CrossRef] [Green Version]
- Lokhandwala, T.; Smith, N.; Sternhufvud, C.; Sorstadius, E.; Lee, W.C.; Mukherjee, J. A retrospective study of persistence, adherence, and health economic outcomes of fixed-dose combination vs. loose-dose combination of oral anti-diabetes drugs. J. Med. Econ. 2016, 19, 203–212. [Google Scholar] [CrossRef]
- Lopez-Simarro, F.; Brotons, C.; Moral, I.; Aguado-Jodar, A.; Cols-Sagarra, C.; Miravet-Jimenez, S. Concordance between two methods in measuring treatment adherence in patients with type 2 diabetes. Patient Prefer. Adherence 2016, 10, 743–750. [Google Scholar] [CrossRef] [Green Version]
- Mallah, Z.; Hammoud, Y.; Awada, S.; Rachidi, S.; Zein, S.; Ballout, H.; Al-Hajje, A. Validation of diabetes medication adherence scale in the Lebanese population. Diabetes Res. Clin. Pract. 2019, 156, 107837. [Google Scholar] [CrossRef]
- Manteuffel, M.; Williams, S.; Chen, W.; Verbrugge, R.R.; Pittman, D.G.; Steinkellner, A. Influence of patient sex and gender on medication use, adherence, and prescribing alignment with guidelines. J. Women’s Health (Larchmt) 2014, 23, 112–119. [Google Scholar] [CrossRef]
- Martinez-Perez, P.; Orozco-Beltran, D.; Pomares-Gomez, F.; Hernandez-Rizo, J.L.; Borras-Gallen, A.; Gil-Guillen, V.F.; Quesada, J.A.; Lopez-Pineda, A.; Carratala-Munuera, C. Validation and psychometric properties of the 8-item Morisky Medication Adherence Scale (MMAS-8) in type 2 diabetes patients in Spain. Aten. Primaria. 2021, 53, 101942. [Google Scholar] [CrossRef]
- Mhatre, S.K.; Serna, O.; Sansgiry, S.; Fleming, M.L.; Essien, E.J.; Sansgiry, S.S. Risk of Nondherence to Diabetes Medications Among Medicare Advantage Enrollees: Development of a Validated Risk Prediction Tool. J. Manag. Care Spec. Pharm. 2016, 22, 1293–1301. [Google Scholar] [CrossRef]
- Miller, G.E.; Sarpong, E.M.; Hill, S.C. Does increased adherence to medications change health care financial burdens for adults with diabetes? J. Diabetes 2015, 7, 872–880. [Google Scholar] [CrossRef]
- Min, J.Y.; Griffin, M.R.; Chipman, J.; Hackstadt, A.J.; Greevy, R.A.; Grijalva, C.G.; Hung, A.M.; Roumie, C.L. Recent metformin adherence and the risk of hypoglycaemia in the year following intensification with a sulfonylurea. Diabet. Med. 2019, 36, 482–490. [Google Scholar] [CrossRef] [Green Version]
- Mirahmadizadeh, A.; Khorshidsavar, H.; Seif, M.; Sharifi, M.H. Adherence to Medication, Diet and Physical Activity and the Associated Factors Amongst Patients with Type 2 Diabetes. Diabetes Ther. 2020, 11, 479–494. [Google Scholar] [CrossRef] [Green Version]
- Mroueh, L.; Ayoub, D.; El-Hajj, M.; Awada, S.; Rachidi, S.; Zein, S.; Al-Hajje, A. Evaluation of medication adherence among Lebanese diabetic patients. Pharm. Pract. 2018, 16, 1291. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, S.; Sharmasarkar, B.; Das, K.K.; Bhattacharyya, A.; Deb, A. Compliance to anti-diabetic drugs: Observations from the diabetic clinic of a medical college in kolkata, India. J. Clin. Diagn. Res. 2013, 7, 661–665. [Google Scholar] [CrossRef]
- Naffaa, M.E.; Rosenberg, V.; Watad, A.; Tiosano, S.; Yavne, Y.; Chodick, G.; Amital, H.; Shalev, V. Adherence to metformin and the onset of rheumatoid arthritis: A population-based cohort study. Scand. J. Rheumatol. 2020, 49, 173–180. [Google Scholar] [CrossRef]
- Nichols, G.A.; Rosales, A.G.; Kimes, T.M.; Tunceli, K.; Kurtyka, K.; Mavros, P. The Change in HbA1c Associated with Initial Adherence and Subsequent Change in Adherence among Diabetes Patients Newly Initiating Metformin Therapy. J. Diabetes Res. 2016, 2016, 9687815. [Google Scholar] [CrossRef] [Green Version]
- Nichols, G.A.; Raebel, M.A.; Dyer, W.; Schmittdiel, J.A. The Effect of Age and Comorbidities on the Association Between the Medicare STAR Oral Antihyperglycemic Adherence Metric and Glycemic Control. J. Manag. Care Spec. Pharm. 2018, 24, 856–861. [Google Scholar] [CrossRef]
- Nigam, S.; Virdi, N.S.; Daskiran, M.; Kozma, C.M.; Paris, A.; Dickson, W.M. Association between sitagliptin adherence and self-monitoring of blood glucose. J. Diabetes Sci. Technol. 2012, 6, 555–562. [Google Scholar] [CrossRef]
- Nishimura, R.; Kato, H.; Kisanuki, K.; Oh, A.; Onishi, Y.; Guelfucci, F.; Shimasaki, Y. Comparison of persistence and adherence between fixed-dose combinations and two-pill combinations in Japanese patients with type 2 diabetes. Curr. Med. Res. Opin. 2019, 35, 869–878. [Google Scholar] [CrossRef]
- Nishimura, R.; Kato, H.; Kisanuki, K.; Oh, A.; Hiroi, S.; Onishi, Y.; Guelfucci, F.; Shimasaki, Y. Treatment patterns, persistence and adherence rates in patients with type 2 diabetes mellitus in Japan: A claims-based cohort study. BMJ Open 2019, 9, e025806. [Google Scholar] [CrossRef] [Green Version]
- Ofori-Asenso, R.; Liew, D.; Lalic, S.; Mazidi, M.; Magliano, D.J.; Ademi, Z.; Bell, J.S.; Ilomaki, J. Adherence, Persistence, and Switching Among People Prescribed Sodium Glucose Co-transporter 2 Inhibitors: A Nationwide Retrospective Cohort Study. Adv. Ther. 2019, 36, 3265–3278. [Google Scholar] [CrossRef]
- Ofori-Asenso, R.; Ilomaki, J.; Chin, K.L.; Mazidi, M.; Zomer, E.; Bell, J.S.; Magliano, D.J.; Liew, D. Dynamics of switching, adherence, and persistence of dipeptidyl peptidase-4 inhibitors use: A nationwide cohort study. Diabetes Res. Clin. Pract. 2019, 158, 107909. [Google Scholar] [CrossRef]
- Oh, A.; Kisanuki, K.; Nishigaki, N.; Shimasaki, Y.; Sakaguchi, K.; Morimoto, T. Comparison of persistence and adherence between DPP-4 inhibitor administration frequencies in patients with type 2 diabetes mellitus in Japan: A claims-based cohort study. Curr. Med. Res. Opin. 2020, 36, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Olickal, J.J.; Chinnakali, P.; Suryanarayana, B.S.; Saya, G.K.; Ganapathy, K.; Subrahmanyam, D.K.S. Medication adherence and glycemic control status among people with diabetes seeking care from a tertiary care teaching hospital, south India. Clin. Epidemiol. Glob. Health 2021, 11, 100742. [Google Scholar] [CrossRef]
- O’Shea, M.P.; Teeling, M.; Bennett, K. An observational study examining the effect of comorbidity on the rates of persistence and adherence to newly initiated oral anti-hyperglycaemic agents. Pharmacoepidemiol. Drug Saf. 2013, 22, 1336–1344. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, M.P.; Teeling, M.; Bennett, K. Regional variation in medication-taking behaviour of new users of oral anti-hyperglycaemic therapy in Ireland. Ir. J. Med. Sci. 2015, 184, 403–410. [Google Scholar] [CrossRef]
- Oung, A.B.; Kosirog, E.; Chavez, B.; Brunner, J.; Saseen, J.J. Evaluation of medication adherence in chronic disease at a federally qualified health center. Ther. Adv. Chronic Dis. 2017, 8, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Pascal, I.G.; Ofoedu, J.N.; Uchenna, N.P.; Nkwa, A.A.; Uchamma, G.U. Blood Glucose Control and Medication Adherence Among Adult Type 2 Diabetic Nigerians Attending A Primary Care Clinic in Under-resourced Environment of Eastern Nigeria. N. Am. J. Med. Sci. 2012, 4, 310–315. [Google Scholar] [CrossRef]
- Peeters, B.; Van Tongelen, I.; Duran, Z.; Yuksel, G.; Mehuys, E.; Willems, S.; Remon, J.P.; Boussery, K. Understanding medication adherence among patients of Turkish descent with type 2 diabetes: A qualitative study. Ethn. Health 2015, 20, 87–105. [Google Scholar] [CrossRef] [PubMed]
- Quilliam, B.J.; Ozbay, A.B.; Sill, B.E.; Kogut, S.J. The association between adherence to oral anti-diabetic drugs and hypoglycaemia in persons with Type 2 diabetes. Diabet. Med. 2013, 30, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Rahmatullah; Qutubuddin, M.; Abdul Rahman, R.; Ghafoor, E.; Riaz, M. Assessment of Factors Associated with Non-Compliance to Self-Management Practices in People with Type 2 Diabetes. Cureus 2021, 13, e18918. [Google Scholar] [CrossRef]
- Rana, B.; Bukhsh, A.; Khan, T.M.; Sarwar, A.; Omer, M.O.; Jamshed, S.Q. Evaluation of Therapeutic Effectiveness of Prescribed Medications in Patients with Type 2 Diabetes Mellitus: Findings from a Tertiary Care Hospital, Lahore, Pakistan. J. Pharm. Bioallied Sci. 2017, 9, 121–125. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Jayawardena, R.; Katulanda, P.; Constantine, G.R.; Ramanayake, V.; Galappatthy, P. Translation and Validation of the Sinhalese Version of the Brief Medication Questionnaire in Patients with Diabetes Mellitus. J. Diabetes Res. 2018, 2018, 7519462. [Google Scholar] [CrossRef] [Green Version]
- Rascati, K.L.; Worley, K.; Meah, Y.; Everhart, D. Adherence, Persistence, and Health Care Costs for Patients Receiving Dipeptidyl Peptidase-4 Inhibitors. J. Manag. Care Spec. Pharm. 2017, 23, 299–306. [Google Scholar] [CrossRef]
- Rathish, D.; Hemachandra, R.; Premadasa, T.; Ramanayake, S.; Rasangika, C.; Roshiban, R.; Jayasumana, C. Comparison of medication adherence between type 2 diabetes mellitus patients who pay for their medications and those who receive it free: A rural Asian experience. J. Health Popul. Nutr. 2019, 38, 4. [Google Scholar] [CrossRef]
- Reach, G.; Pellan, M.; Crine, A.; Touboul, C.; Ciocca, A.; Djoudi, Y. Holistic psychosocial determinants of adherence to medication in people with type 2 diabetes. Diabetes Metab. 2018, 44, 500–507. [Google Scholar] [CrossRef]
- Reach, G.; Michault, A.; Bihan, H.; Paulino, C.; Cohen, R.; Le Clesiau, H. Patients’ impatience is an independent determinant of poor diabetes control. Diabetes Metab. 2011, 37, 497–504. [Google Scholar] [CrossRef]
- Rinne, S.T.; Wong, E.S.; Lemon, J.M.; Perkins, M.; Bryson, C.L.; Liu, C.F. Survey nonresponders incurred higher medical utilization and lower medication adherence. Am. J. Manag. Care 2015, 21, e1–e8. [Google Scholar]
- Romagnoli, A.; Santoleri, F.; Costantini, A. Drug utilisation pattern over 3 years in the real-world treatment of type II diabetes. Int. J. Clin. Pract. 2021, 75, e14120. [Google Scholar] [CrossRef]
- Sacks, N.C.; Burgess, J.F., Jr.; Cabral, H.J.; Pizer, S.D.; McDonnell, M.E. Cost sharing and decreased branded oral anti-diabetic medication adherence among elderly Part D Medicare beneficiaries. J. Gen. Intern. Med. 2013, 28, 876–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacks, N.C.; Burgess, J.F.; Cabral, H.J.; McDonnell, M.E.; Pizer, S.D. The Effects of Cost Sharing on Adherence to Medications Prescribed for Concurrent Use: Do Definitions Matter? J. Manag. Care Spec. Pharm. 2015, 21, 678–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sankar, U.V.; Lipska, K.; Mini, G.K.; Sarma, P.S.; Thankappan, K.R. The adherence to medications in diabetic patients in rural Kerala, India. Asia Pac. J. Public Health 2015, 27, NP513–NP523. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, E.M.S.; Coelho, J.L.G.; Dos Santos Figueiredo, F.W.; do Souto, R.P. Medication non-adherence in patients with type 2 diabetes mellitus with full access to medicines. J. Diabetes Metab. Disord. 2020, 19, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Satirapoj, B.; Pratipanawatr, T.; Ongphiphadhanakul, B.; Suwanwalaikorn, S.; Benjasuratwong, Y.; Nitiyanant, W. Real-world Evaluation of glycemic control and hypoglycemic Events among type 2 Diabetes mellitus study (REEDS): A multicentre, cross-sectional study in Thailand. BMJ Open 2020, 10, e031612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sattler, E.L.; Lee, J.S.; Bhargava, V. Food insecurity and medication adherence in low-income older Medicare beneficiaries with type 2 diabetes. J. Nutr. Gerontol. Geriatr. 2014, 33, 401–417. [Google Scholar] [CrossRef] [PubMed]
- Saundankar, V.; Peng, X.; Fu, H.; Ascher-Svanum, H.; Rodriguez, A.; Ali, A.; Slabaugh, L.; Young, P.; Louder, A. Predictors of Change in Adherence Status from 1 Year to the Next Among Patients with Type 2 Diabetes Mellitus on Oral Antidiabetes Drugs. J. Manag. Care Spec. Pharm. 2016, 22, 467–482. [Google Scholar] [CrossRef]
- Schwab, P.; Racsa, P.; Rascati, K.; Mourer, M.; Meah, Y.; Worley, K. A Retrospective Database Study Comparing Diabetes-Related Medication Adherence and Health Outcomes for Mail-Order Versus Community Pharmacy. J. Manag. Care Spec. Pharm. 2019, 25, 332–340. [Google Scholar] [CrossRef]
- Shields, B.M.; Hattersley, A.T.; Farmer, A.J. Identifying routine clinical predictors of non-adherence to second-line therapies in type 2 diabetes: A retrospective cohort analysis in a large primary care database. Diabetes Obes. Metab. 2020, 22, 59–65. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, S.S.; Shakya, R.; Karmacharya, B.M.; Thapa, P. Medication adherence to oral hypoglycemic agents among type II diabetic patients and their clinical outcomes with special reference to fasting blood glucose and glycosylated hemoglobin levels. Kathmandu Univ. Med. J. (KUMJ) 2013, 11, 226–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simard, P.; Presse, N.; Roy, L.; Dorais, M.; White-Guay, B.; Rakel, A.; Perreault, S. Association Between Metformin Adherence and All-Cause Mortality Among New Users of Metformin: A Nested Case-Control Study. Ann. Pharmacother. 2018, 52, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Simard, P.; Presse, N.; Roy, L.; Dorais, M.; White-Guay, B.; Rakel, A.; Perreault, S. Persistence and adherence to oral antidiabetics: A population-based cohort study. Acta Diabetol. 2015, 52, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Simon-Tuval, T.; Shmueli, A.; Harman-Boehm, I. Adherence of patients with type 2 diabetes mellitus to medications: The role of risk preferences. Curr. Med. Res. Opin. 2018, 34, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Sicras-Mainar, A.; Navarro-Artieda, R. Use of metformin and vildagliptin for treatment of type 2 diabetes in the elderly. Drug Des. Devel. Ther. 2014, 8, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Singhal, M.; Tan, H.; Coleman, C.I.; Han, M.; Nguyen, C.; Ingham, M. Effectiveness, treatment durability, and treatment costs of canagliflozin and glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes in the USA. BMJ Open Diabetes Res. Care 2019, 7, e000704. [Google Scholar] [CrossRef] [Green Version]
- Taira, D.A.; Seto, B.K.; Davis, J.W.; Seto, T.B.; Landsittel, D.; Sumida, W.K. Examining Factors Associated With Nonadherence And Identifying Providers Caring For Nonadherent Subgroups. J. Pharm. Health Serv. Res. 2017, 8, 247–253. [Google Scholar] [CrossRef]
- Tanabe, M.; Motonaga, R.; Terawaki, Y.; Nomiyama, T.; Yanase, T. Prescription of oral hypoglycemic agents for patients with type 2 diabetes mellitus: A retrospective cohort study using a Japanese hospital database. J. Diabetes Investig. 2017, 8, 227–234. [Google Scholar] [CrossRef]
- Tandon, S.; Chew, M.; Eklu-Gadegbeku, C.K.; Shermock, K.M.; Morisky, D.E. Validation and psychometric properties of the 8-item Morisky Medication Adherence Scale (MMAS-8) in Type 2 diabetes patients in sub-Saharan Africa. Diabetes Res. Clin. Pract. 2015, 110, 129–136. [Google Scholar] [CrossRef]
- Tang, Y.; Weiss, T.; Liu, J.; Rajpathak, S.; Khunti, K. Metformin adherence and discontinuation among patients with type 2 diabetes: A retrospective cohort study. J. Clin. Transl. Endocrinol. 2020, 20, 100225. [Google Scholar] [CrossRef]
- Tiv, M.; Viel, J.F.; Mauny, F.; Eschwege, E.; Weill, A.; Fournier, C.; Fagot-Campagna, A.; Penfornis, A. Medication adherence in type 2 diabetes: The ENTRED study 2007, a French Population-Based Study. PLoS ONE 2012, 7, e32412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tunceli, K.; Zhao, C.; Davies, M.J.; Brodovicz, K.G.; Alexander, C.M.; Iglay, K.; Radican, L. Factors associated with adherence to oral antihyperglycemic monotherapy in patients with type 2 diabetes. Patient Prefer. Adherence 2015, 9, 191–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tunceli, K.; Iglay, K.; Zhao, C.; Brodovicz, K.G.; Radican, L. Factors associated with adherence to oral antihyperglycemic monotherapy in patients with type 2 diabetes mellitus in the United Kingdom. Diabetes Res. Clin. Pract. 2015, 109, e27–e31. [Google Scholar] [CrossRef] [PubMed]
- Vichayanrat, A.; Matawaran, B.J.; Wibudi, A.; Ferdous, H.S.; Aamir, A.H.; Aggarwal, S.K.; Bajpai, S. Assessment of baseline characteristics, glycemic control and oral antidiabetic treatment in Asian patients with diabetes: The Registry for Assessing OAD Usage in Diabetes Management (REASON) Asia study. J. Diabetes 2013, 5, 309–318. [Google Scholar] [CrossRef]
- Vietri, J.T.; Wlodarczyk, C.S.; Lorenzo, R.; Rajpathak, S. Missed doses of oral antihyperglycemic medications in US adults with type 2 diabetes mellitus: Prevalence and self-reported reasons. Curr. Med. Res. Opin. 2016, 32, 1519–1527. [Google Scholar] [CrossRef]
- Vittorino Gaddi, A.; Benedetto, D.; Capello, F.; Di Pietro, C.; Cinconze, E.; Rossi, E.; De Sando, V.; Cevenini, M.; D’Alo, G. Oral antidiabetic therapy in a large Italian sample: Drug supply and compliance for different therapeutic regimens. Public Health 2014, 128, 70–76. [Google Scholar] [CrossRef]
- Vlacho, B.; Mata-Cases, M.; Mundet-Tuduri, X.; Valles-Callol, J.A.; Real, J.; Farre, M.; Cos, X.; Khunti, K.; Mauricio, D.; Franch-Nadal, J. Analysis of the Adherence and Safety of Second Oral Glucose-Lowering Therapy in Routine Practice From the Mediterranean Area: A Retrospective Cohort Study. Front. Endocrinol. 2021, 12, 708372. [Google Scholar] [CrossRef]
- Waari, G.; Mutai, J.; Gikunju, J. Medication adherence and factors associated with poor adherence among type 2 diabetes mellitus patients on follow-up at Kenyatta National Hospital, Kenya. Pan Afr. Med. J. 2018, 29, 82. [Google Scholar] [CrossRef]
- Walz, L.; Pettersson, B.; Rosenqvist, U.; Deleskog, A.; Journath, G.; Wandell, P. Impact of symptomatic hypoglycemia on medication adherence, patient satisfaction with treatment, and glycemic control in patients with type 2 diabetes. Patient Prefer. Adherence 2014, 8, 593–601. [Google Scholar] [CrossRef] [Green Version]
- White, A.J.; Kellar, I.; Prevost, A.T.; Kinmonth, A.L.; Sutton, S.; Canny, M.; Griffin, S.J. Adherence to hypoglycaemic medication among people with type 2 diabetes in primary care. Prim. Care Diabetes 2012, 6, 27–33. [Google Scholar] [CrossRef]
- Wong, M.C.; Kong, A.P.; So, W.Y.; Jiang, J.Y.; Chan, J.C.; Griffiths, S.M. Adherence to oral hypoglycemic agents in 26,782 Chinese patients: A cohort study. J. Clin. Pharmacol. 2011, 51, 1474–1482. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.; Wu, C.H.; Wang, H.H.; Li, H.W.; Hui, E.M.; Lam, A.T.; Chung, R.Y.; Yip, B.H.; Morisky, D.E. Association between the 8-item Morisky medication adherence scale (MMAS-8) score and glycaemic control among Chinese diabetes patients. J. Clin. Pharmacol. 2015, 55, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.S.; Bryson, C.L.; Hebert, P.L.; Liu, C.F. Estimating the Impact of Oral Diabetes Medication Adherence on Medical Costs in VA. Ann. Pharmacother. 2014, 48, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.S.; Piette, J.D.; Liu, C.F.; Perkins, M.; Maciejewski, M.L.; Jackson, G.L.; Blough, D.K.; Fihn, S.D.; Au, D.H.; Bryson, C.L. Measures of adherence to oral hypoglycemic agents at the primary care clinic level: The role of risk adjustment. Med. Care 2012, 50, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Liu, N. Association between patients’ beliefs and oral antidiabetic medication adherence in a Chinese type 2 diabetic population. Patient Prefer. Adherence 2016, 10, 1161–1167. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Liao, L.; Sun, M.; He, G. Self-care practices of Chinese individuals with diabetes. Exp. Ther. Med. 2013, 5, 1137–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, V.J.; Tu, W.; Rosenman, M.B.; Overhage, J.M. Nonadherence to Oral Antihyperglycemic Agents: Subsequent Hospitalization and Mortality among Patients with Type 2 Diabetes in Clinical Practice. Stud. Health Technol. Inform. 2015, 216, 60–63. [Google Scholar] [PubMed]
- Zomahoun, H.T.V.; Moisan, J.; Lauzier, S.; Guillaumie, L.; Gregoire, J.P.; Guenette, L. Predicting Noninsulin Antidiabetic Drug Adherence Using a Theoretical Framework Based on the Theory of Planned Behavior in Adults With Type 2 Diabetes: A Prospective Study. Medicine 2016, 95, e2954. [Google Scholar] [CrossRef]
- Zongo, A.; Guenette, L.; Moisan, J.; Gregoire, J.P. Predictive Validity of Self-Reported Measures of Adherence to Noninsulin Antidiabetes Medication against Control of Glycated Hemoglobin Levels. Can. J. Diabetes 2016, 40, 58–65. [Google Scholar] [CrossRef] [Green Version]
- An, S.-Y.; Kim, H.J.; Chun, K.H.; Kim, T.H.; Jeon, J.Y.; Kim, D.J.; Han, S.J.; Kim, Y.S.; Woo, J.T.; Ahn, K.J.; et al. Clinical and Economic Outcomes in Medication-Adherent and -Nonadherent Patients with Type 2 Diabetes Mellitus in the Republic of Korea. Clin. Ther. 2014, 36, 245–254. [Google Scholar] [CrossRef]
- Arulmozhi, S.; Mahalakshmy, T. Self Care and Medication Adherence among Type 2 Diabetics in Puducherry, Southern India: A Hospital Based Study. J. Clin. Diagn. Res. 2014, 8, UC01–UC03. [Google Scholar]
- Benrazavy, L.; Khalooei, A. Medication Adherence and its Predictors in Type 2 Diabetic Patients Referring to Urban Primary Health Care Centers in Kerman City, Southeastern Iran. Shiraz E-Med. J. 2019, 20, e84746. [Google Scholar] [CrossRef] [Green Version]
- Khan, G.H.; Aqil, M.; Pillai, K.K.; Ahmad, M.A.; Kapur, P.; Ain, M.R.; Al-Ghamdi, S.S.; Shahzad, N. Therapeutic adherence: A prospective drug utilization study of oral hypoglycemic in patients with type 2 diabetes mellitus. Asian Pac. J. Trop. Dis. 2014, 4, S347–S352. [Google Scholar] [CrossRef]
- Iuga, A.O.; McGuire, M.J. Adherence and health care costs. Risk Manag. Healthc. Policy 2014, 7, 35–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, R.; Khan, H.; Heydon, E.; Shroufi, A.; Fahimi, S.; Moore, C.; Stricker, B.; Mendis, S.; Hofman, A.; Mant, J.; et al. Adherence to cardiovascular therapy: A meta-analysis of prevalence and clinical consequences. Eur. Heart J. 2013, 34, 2940–2948. [Google Scholar] [CrossRef] [Green Version]
- Abegaz, T.M.; Shehab, A.; Gebreyohannes, E.A.; Bhagavathula, A.S.; Elnour, A.A. Nonadherence to antihypertensive drugs: A systematic review and meta-analysis. Medicine 2017, 96, e5641. [Google Scholar] [CrossRef]
- Suviranta, T.; Timonen, J.; Martikainen, J.; Aarnio, E. The effects of reimbursement reform of antidiabetic medicines from the patients’ perspective—A survey among patients with type 2 diabetes in Finland. BMC Health Serv. Res. 2019, 19, 769. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Feldman, R.; Rothenberger, S.D.; Hernandez, I.; Gellad, W.F. Coverage, Formulary Restrictions, and Out-of-Pocket Costs for Sodium-Glucose Cotransporter 2 Inhibitors and Glucagon-Like Peptide 1 Receptor Agonists in the Medicare Part D Program. JAMA Netw. Open 2020, 3, e2020969. [Google Scholar] [CrossRef]
- Carratala-Munuera, C.; Cortes-Castell, E.; Marquez-Contreras, E.; Castellano, J.M.; Perez-Paramo, M.; Lopez-Pineda, A.; Gil-Guillen, V.F. Barriers and Solutions to Improve Therapeutic Adherence from the Perspective of Primary Care and Hospital-Based Physicians. Patient Prefer. Adherence 2022, 16, 697–707. [Google Scholar] [CrossRef]
- Atreja, A.; Bellam, N.; Levy, S.R. Strategies to enhance patient adherence: Making it simple. Medscape Gen. Med. 2005, 7, 4. [Google Scholar]
- Cutler, R.L.; Torres-Robles, A.; Wiecek, E.; Drake, B.; Van der Linden, N.; Benrimoj, S.I.C.; Garcia-Cardenas, V. Pharmacist-led medication non-adherence intervention: Reducing the economic burden placed on the Australian health care system. Patient Prefer. Adherence 2019, 13, 853–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Robles, A.; Benrimoj, S.I.; Gastelurrutia, M.A.; Martinez-Martinez, F.; Peiro, T.; Perez-Escamilla, B.; Rogers, K.; Valverde-Merino, I.; Varas-Doval, R.; Garcia-Cardenas, V. Effectiveness of a medication adherence management intervention in a community pharmacy setting: A cluster randomised controlled trial. BMJ Qual. Saf. 2022, 31, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Presley, B.; Groot, W.; Pavlova, M. Pharmacy-led interventions to improve medication adherence among adults with diabetes: A systematic review and meta-analysis. Res. Soc. Adm. Pharm. 2019, 15, 1057–1067. [Google Scholar] [CrossRef]
- Chen, S.L.; Lee, W.L.; Liang, T.; Liao, I.C. Factors associated with gender differences in medication adherence: A longitudinal study. J. Adv. Nurs. 2014, 70, 2031–2040. [Google Scholar] [CrossRef] [PubMed]
- Billimek, J.; Malik, S.; Sorkin, D.H.; Schmalbach, P.; Ngo-Metzger, Q.; Greenfield, S.; Kaplan, S.H. Understanding disparities in lipid management among patients with type 2 diabetes: Gender differences in medication nonadherence after treatment intensification. Women’s Health Issues 2015, 25, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olagbemide, O.J.; Omosanya, O.E.; Ayodapo, A.O.; Agboola, S.M.; Adeagbo, A.O.; Olukokun, T.A. Family support and medication adherence among adult type 2 diabetes: Any meeting point? Ann. Afr. Med. 2021, 20, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Kopp, W. How Western Diet And Lifestyle Drive The Pandemic Of Obesity And Civilization Diseases. Diabetes Metab. Syndr. Obes. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [Green Version]
- Trief, P.M.; Kalichman, S.C.; Wang, D.; Drews, K.L.; Anderson, B.J.; Bulger, J.D.; Weinstock, R.S. Medication adherence in young adults with youth-onset type 2 diabetes: iCount, an observational study. Diabetes Res. Clin. Pract. 2022, 184, 109216. [Google Scholar] [CrossRef]
- Shrivastava, T.P.; Goswami, S.; Gupta, R.; Goyal, R.K. Mobile App Interventions to Improve Medication Adherence Among Type 2 Diabetes Mellitus Patients: A Systematic Review of Clinical Trials. J. Diabetes Sci. Technol. 2021; online first. [Google Scholar] [CrossRef]
- Enricho Nkhoma, D.; Jenya Soko, C.; Joseph Banda, K.; Greenfield, D.; Li, Y.J.; Iqbal, U. Impact of DSMES app interventions on medication adherence in type 2 diabetes mellitus: Systematic review and meta-analysis. BMJ Health Care Inform. 2021, 28, e100291. [Google Scholar] [CrossRef]
- Islam, S.M.S.; Mishra, V.; Siddiqui, M.U.; Moses, J.C.; Adibi, S.; Nguyen, L.; Wickramasinghe, N. Smartphone Apps for Diabetes Medication Adherence: Systematic Review. JMIR Diabetes 2022, 7, e33264. [Google Scholar] [CrossRef]
- Wang, G.S.; Hoyte, C. Review of Biguanide (Metformin) Toxicity. J. Intensive Care Med. 2019, 34, 863–876. [Google Scholar] [CrossRef]
- Hirst, J.A.; Farmer, A.J.; Dyar, A.; Lung, T.W.; Stevens, R.J. Estimating the effect of sulfonylurea on HbA1c in diabetes: A systematic review and meta-analysis. Diabetologia 2013, 56, 973–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sola, D.; Rossi, L.; Schianca, G.P.; Maffioli, P.; Bigliocca, M.; Mella, R.; Corliano, F.; Fra, G.P.; Bartoli, E.; Derosa, G. Sulfonylureas and their use in clinical practice. Arch. Med. Sci. 2015, 11, 840–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmasi, S.; De Vera, M.A.; Safari, A.; Lynd, L.D.; Koehoorn, M.; Barry, A.R.; Andrade, J.G.; Deyell, M.W.; Rush, K.; Zhao, Y.; et al. Longitudinal Oral Anticoagulant Adherence Trajectories in Patients With Atrial Fibrillation. J. Am. Coll. Cardiol. 2021, 78, 2395–2404. [Google Scholar] [CrossRef] [PubMed]
- Convertino, I.; Giometto, S.; Gini, R.; Cazzato, M.; Fornili, M.; Valdiserra, G.; Cappello, E.; Ferraro, S.; Bartolini, C.; Paoletti, O.; et al. Trajectories of Adherence to Biologic Disease-Modifying Anti-Rheumatic Drugs in Tuscan Administrative Databases: The Pathfinder Study. J. Clin. Med. 2021, 10, 5743. [Google Scholar] [CrossRef]
- Gallwitz, B. Clinical Use of DPP-4 Inhibitors. Front. Endocrinol. 2019, 10, 389. [Google Scholar] [CrossRef] [Green Version]
- Halimi, S.; Verges, B. Adverse effects and safety of SGLT-2 inhibitors. Diabetes Metab. 2014, 40, S28–S34. [Google Scholar] [CrossRef]
- Filippatos, T.D.; Athyros, V.G.; Elisaf, M.S. The pharmacokinetic considerations and adverse effects of DPP-4 inhibitors [corrected]. Expert. Opin. Drug Metab. Toxicol. 2014, 10, 787–812. [Google Scholar] [CrossRef]
- Richard, K.R.; Shelburne, J.S.; Kirk, J.K. Tolerability of dipeptidyl peptidase-4 inhibitors: A review. Clin. Ther. 2011, 33, 1609–1629. [Google Scholar] [CrossRef]
- Wu, S.; Chai, S.; Yang, J.; Cai, T.; Xu, Y.; Yang, Z.; Zhang, Y.; Ji, L.; Sun, F.; Zhan, S. Gastrointestinal Adverse Events of Dipeptidyl Peptidase 4 Inhibitors in Type 2 Diabetes: A Systematic Review and Network Meta-analysis. Clin. Ther. 2017, 39, 1780–1789.e33. [Google Scholar] [CrossRef]
- Parati, G.; Kjeldsen, S.; Coca, A.; Cushman, W.C.; Wang, J. Adherence to Single-Pill Versus Free-Equivalent Combination Therapy in Hypertension: A Systematic Review and Meta-Analysis. Hypertension 2021, 77, 692–705. [Google Scholar] [CrossRef] [PubMed]
- Anghel, L.A.; Farcas, A.M.; Oprean, R.N. An overview of the common methods used to measure treatment adherence. Med. Pharm. Rep. 2019, 92, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Compton, J.; Glass, N.; Fowler, T. Evidence of Selection Bias and Non-Response Bias in Patient Satisfaction Surveys. Iowa Orthop. J. 2019, 39, 195–201. [Google Scholar] [PubMed]
- Kaaffah, S.; Soewondo, P.; Riyadina, W.; Renaldi, F.S.; Sauriasari, R. Adherence to Treatment and Glycemic Control in Patients with Type 2 Diabetes Mellitus: A 4-Year Follow-up PTM Bogor Cohort Study, Indonesia. Patient Prefer. Adherence 2021, 15, 2467–2477. [Google Scholar] [CrossRef] [PubMed]
- Aikens, J.E.; Piette, J.D. Longitudinal association between medication adherence and glycaemic control in Type 2 diabetes. Diabet. Med. 2013, 30, 338–344. [Google Scholar] [CrossRef] [Green Version]
- Choudhry, N.K.; Kronish, I.M.; Vongpatanasin, W.; Ferdinand, K.C.; Pavlik, V.N.; Egan, B.M.; Schoenthaler, A.; Houston Miller, N.; Hyman, D.J.; American Heart Association Council on Hypertension; et al. Medication Adherence and Blood Pressure Control: A Scientific Statement From the American Heart Association. Hypertension 2022, 79, e1–e14. [Google Scholar] [CrossRef] [PubMed]
- Cedillo-Couvert, E.A.; Ricardo, A.C.; Chen, J.; Cohan, J.; Fischer, M.J.; Krousel-Wood, M.; Kusek, J.W.; Lederer, S.; Lustigova, E.; Ojo, A.; et al. Self-reported Medication Adherence and CKD Progression. Kidney Int. Rep. 2018, 3, 645–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhury, A.; Duvoor, C.; Reddy Dendi, V.S.; Kraleti, S.; Chada, A.; Ravilla, R.; Marco, A.; Shekhawat, N.S.; Montales, M.T.; Kuriakose, K.; et al. Clinical Review of Antidiabetic Drugs: Implications for Type 2 Diabetes Mellitus Management. Front. Endocrinol. 2017, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Blankart, K.E.; Lichtenberg, F.R. Are patients more adherent to newer drugs? Health Care Manag. Sci. 2020, 23, 605–618. [Google Scholar] [CrossRef]
- Krass, I.; Schieback, P.; Dhippayom, T. Adherence to diabetes medication: A systematic review. Diabet. Med. 2015, 32, 725–737. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Good/High Adherence Definition/Calculation | Number of Studies |
|---|---|
| Self-reported (65) | |
| MMAS-8 questionnaire Score = 8 [30,35,64,76,91,103,104,111,115,135,160,169,180] Score ≥ 6 [39,58,145,173,176,183] Score ≥ 7 [78] Score > 8 [30] | 21 13 6 1 1 |
| MMAS-4 questionnaire Score = 4 [63,75,94,138,146,184] Score > 3 [46] | 7 6 1 |
| LMAS-14 questionnaire Score ≥ 38 [40,116] Score > 11 [88] | 3 2 1 |
| MCQ questionnaire (score > 27) [29,34,37] | 3 |
| MARS questionnaire Score > 20 [60] Score = 25 [102] | 2 1 1 |
| ARMS questionnaire (score = 12) [38,98] | 2 |
| Verbal interview >80% of the prescribed antidiabetic medications taken [61,92,93,117] >90% of the prescribed antidiabetic medications taken [177] Compliance ≥ 90% [165] | 6 4 1 1 |
| Other questionnaires a [31,32,33,36,37,45,80,82,100,109,127,131,132,134,136,139,140,147,162,166,170] | 21 |
| Pill counting b (3) [86,99,171] | |
| Use of administrative data (88) | |
| PDC ≥ 80% [42,43,44,47,48,49,50,51,52,59,62,66,67,68,69,70,71,73,77,84,87,89,90,95,96,97,101,105,106,112,114,118,120,122,123,124,125,126,130,137,144,148,149,150,155,157,161,163,164,178,179] Follow-up period: * <12 months (1–9 months) =12 months >12 months (24–48 months) Not specified | 51 5 35 13 4 |
| MPR ≥ 80% [53,54,55,56,57,65,72,74,83,85,107,110,113,128,129,133,141,143,151,153,154,158,167,168,172,174] Follow-up period: * <12 months (3–6 months) =2 months >12 months (18 months–7 years) Not specified | 26 4 15 9 3 |
| Other calculations a [41,79,81,108,119,121,142,156,159,175,181] | 11 |
| Reasons for Non-Adherence | Number of Studies |
|---|---|
| Forgetfulness 1 | 28 |
| Experiencing of side effects | 15 |
| High costs | 12 |
| Absence/disappearance of symptoms | 9 |
| Carelessness | 8 |
| Multiple medications | 6 |
| Procrastinating on refills or renewals of prescriptions | 6 |
| Feeling hassled or bored to take medication regularly | 5 |
| Worry about using medication regularly due to possible risk of unintended effects | 5 |
| Not accepting disease/feeling disease under control | 4 |
| Lack of confidence or poor communication with the physician/healthcare provider | 4 |
| Being too busy/time constraints | 4 |
| Social influence and environmental context | 3 |
| Complexity of treatment regimen | 2 |
| Inefficacy | 2 |
| Preference for herbal remedies | 2 |
| Others 2 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piragine, E.; Petri, D.; Martelli, A.; Calderone, V.; Lucenteforte, E. Adherence to Oral Antidiabetic Drugs in Patients with Type 2 Diabetes: Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 1981. https://doi.org/10.3390/jcm12051981
Piragine E, Petri D, Martelli A, Calderone V, Lucenteforte E. Adherence to Oral Antidiabetic Drugs in Patients with Type 2 Diabetes: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(5):1981. https://doi.org/10.3390/jcm12051981
Chicago/Turabian StylePiragine, Eugenia, Davide Petri, Alma Martelli, Vincenzo Calderone, and Ersilia Lucenteforte. 2023. "Adherence to Oral Antidiabetic Drugs in Patients with Type 2 Diabetes: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 5: 1981. https://doi.org/10.3390/jcm12051981