

Laparoendoscopic Single-Site Inguinal Herniorrhaphy: Experience of a Single Institute
 , , and
, , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Surgical Technique
2.2. Statistical Analysis
3. Results
3.1. Patients’ Demographic and Clinical Data
3.2. Perioperative Data
3.3. Postoperative Outcomes and Complications
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Memon, M.A.; Cooper, N.J.; Memon, B.; Memon, M.I.; Abrams, K.R. Meta-analysis of randomized clinical trials comparing open and laparoscopic inguinal hernia repair. Br. J. Surg. 2003, 90, 1479–1492. [Google Scholar] [CrossRef] [PubMed]
- Ielpo, B.; Nunez-Alfonsel, J.; Duran, H.; Diaz, E.; Fabra, I.; Caruso, R.; Malavé, L.; Ferri, V.; Barzola, E.; Quijano, Y.; et al. Cost-effectiveness of Randomized Study of Laparoscopic Versus Open Bilateral Inguinal Hernia Repair. Ann. Surg. 2018, 268, 725–730. [Google Scholar] [CrossRef] [PubMed]
- HerniaSurge, G. International guidelines for groin hernia management. Hernia 2018, 22, 1–165. [Google Scholar]
- Ahmed, I.; Paraskeva, P. A clinical review of single-incision laparoscopic surgery. Surgeon 2011, 9, 341–351. [Google Scholar] [CrossRef]
- Kommu, S.S.R.A. Devices for laparoendoscopic single-site surgery in urology. Expert Rev. Med. Devices 2009, 6, 95–103. [Google Scholar] [CrossRef]
- Rao, A.; Kynaston, J.; MacDonald, E.R.; Ahmed, I. Patient preferences for surgical techniques: Should we invest in new approaches? Surg. Endosc. 2010, 24, 3016–3025. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Bringman, S.; Blomqvist, P. Intestinal obstruction after inguinal and femoral hernia repair: A study of 33,275 operations during 1992–2000 in Sweden. Hernia 2005, 9, 178–183. [Google Scholar] [CrossRef]
- McCormack, K.; Wake, B.L.; Fraser, C.; Vale, L.; Perez, J.; Grant, A. Transabdominal pre-peritoneal (TAPP) versus totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair: A systematic review. Hernia 2005, 9, 109–114. [Google Scholar] [CrossRef]
- Bansal, V.K.; Misra, M.C.; Babu, D.; Victor, J.; Kumar, S.; Sagar, R.; Rajeshwari, S.; Krishna, A.; Rewari, V. A prospective, randomized comparison of long-term outcomes: Chronic groin pain and quality of life following totally extraperitoneal (TEP) and transabdominal preperitoneal (TAPP) laparoscopic inguinal hernia repair. Surg. Endosc. 2013, 27, 2373–2382. [Google Scholar] [CrossRef]
- Aiolfi, A.; Cavalli, M.; Del Ferraro, S.; Manfredini, L.; Lombardo, F.; Bonitta, G.; Bruni, P.G.; Panizzo, V.; Campanelli, G.; Bona, D. Total extraperitoneal (TEP) versus laparoscopic transabdominal preperitoneal (TAPP) hernioplasty: Systematic review and trial sequential analysis of randomized controlled trials. Hernia 2021, 25, 1147–1157. [Google Scholar] [CrossRef]
- Lo, C.W.; Yang, S.S.; Tsai, Y.C.; Hsieh, C.H.; Chang, S.J. Comparison of laparoendoscopic single-site versus conventional multiple-port laparoscopic herniorrhaphy: A systemic review and meta-analysis. Hernia 2016, 20, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Kim, J.H.; Kim, C.H.; Lee, G.R.; Lee, Y.S.; Kim, H.J. Single incision laparoscopic totally extraperitoneal hernioplasty: Lessons learned from 1231 procedures. Ann. Surg. Treat. Res. 2021, 100, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Wakasugi, M.; Mikamori, M.; Tamaoka, K.; Nakahara, Y.; Tei, M.; Furukawa, K.; Ohtsuka, M.; Masuzawa, T.; Akamatsu, H. Long-term outcomes of single-incision versus multiport laparoscopic totally extra-peritoneal inguinal hernia repair: A single-institution experience of 186 consecutive cases. Surg. Today 2022, 52, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Li, C.-C.; Tseng, S.-I.; Lee, H.-Y.; Chueh, K.S.; Tsai, C.C.; Chou, Y.H.; Huang, C.N.; Wu, W.J. Retrospective comparison of open- versus single-incision laparoscopic extraperitoneal repair of inguinal hernia procedures: A single-institution experience. Urol. Sci. 2020, 31, 77. [Google Scholar] [CrossRef]
- Kocijan, R.; Sandberg, S.; Chan, Y.W.; Hollinsky, C. Anatomical changes after inguinal hernia treatment: A reason for chronic pain and recurrent hernia? Surg. Endosc. 2010, 24, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Bhangu, A.; Singh, P.; Pinkney, T.; Blazeby, J.M. A detailed analysis of outcome reporting from randomised controlled trials and meta-analyses of inguinal hernia repair. Hernia 2015, 19, 65–75. [Google Scholar] [CrossRef]
- Ruze, R.; Yan, Z.; Wu, Q.; Zhan, H.; Zhang, G. Correlation between laparoscopic transection of an indirect inguinal hernial sac and postoperative seroma formation: A prospective randomized controlled study. Surg. Endosc. 2019, 33, 1147–1154. [Google Scholar] [CrossRef]
- Dulucq, J.L.; Wintringer, P.; Mahajna, A. Totally extraperitoneal (TEP) hernia repair after radical prostatectomy or previous lower abdominal surgery: Is it safe? A prospective study. Surg. Endosc. 2006, 20, 473–476. [Google Scholar] [CrossRef]
- Kato, J.M.; Iuamoto, L.R.; Suguita, F.Y.; Essu, F.F.; Meyer, A.; Andraus, W. Impact of Obesity and Surgical Skills in Laparoscopic Totally Extraperitoneal Hernioplasty. Arq. Bras. Cir. Dig. 2017, 30, 169–172. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Park, S.M.; Kim, J.J.; Lee, Y.S. Initial experience of single port laparoscopic totally extraperitoneal hernia repair: Nearly-scarless inguinal hernia repair. J. Korean Surg. Soc. 2011, 81, 339–343. [Google Scholar] [CrossRef] [Green Version]
- Tai, H.C.; Lin, C.D.; Wu, C.C.; Tsai, Y.C.; Yang, S.S. Homemade transumbilical port: An alternative access for laparoendoscopic single-site surgery (LESS). Surg. Endosc. 2010, 24, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Tai, H.C.; Ho, C.H.; Tsai, Y.C. Laparoendoscopic single-site surgery: Adult hernia mesh repair with homemade single port. Surg. Laparosc. Endosc. Percutaneous Tech. 2011, 21, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, A.I. An anatomic and functional classification for the diagnosis and treatment of inguinal hernia. Am. J. Surg. 1989, 157, 331–333. [Google Scholar] [CrossRef] [PubMed]
- Nyhus, L.M.; Klein, M.S.; Rogers, F.B. Inguinal hernia. Curr. Probl. Surg. 1991, 28, 401–450. [Google Scholar] [CrossRef] [PubMed]
- Miserez, M.; Alexandre, J.H.; Campanelli, G.; Corcione, F.; Cuccurullo, D.; Pascual, M.H.; Hoeferlin, A.; Kingsnorth, A.N.; Mandala, V.; Palot, J.P.; et al. The European hernia society groin hernia classification: Simple and easy to remember. Hernia 2007, 11, 113–116. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unilateral | Bilateral | |
|---|---|---|
| Number of patients | 178 | 55 |
| Male | 166 | 55 |
| Female | 12 | 0 |
| Number of herniorrhaphies | 178 | 110 |
| Age (years), mean + SD | 57 ± 14 | 64 ± 10 |
| Body mass index (%) | ||
| <25 (kg/m2) | 121 (68%) | 39 (71%) |
| ≥25 (kg/m2) | 57 (32%) | 16 (29%) |
| ASA * (%) | ||
| I | 26 (14.6%) | 2 (3.6%) |
| II | 134 (75.3%) | 43 (78.2%) |
| III | 18 (10.1%) | 10 (18.2%) |
| History of abdominal operation (%) | 29 (16.3%) | 10 (18.2%) |
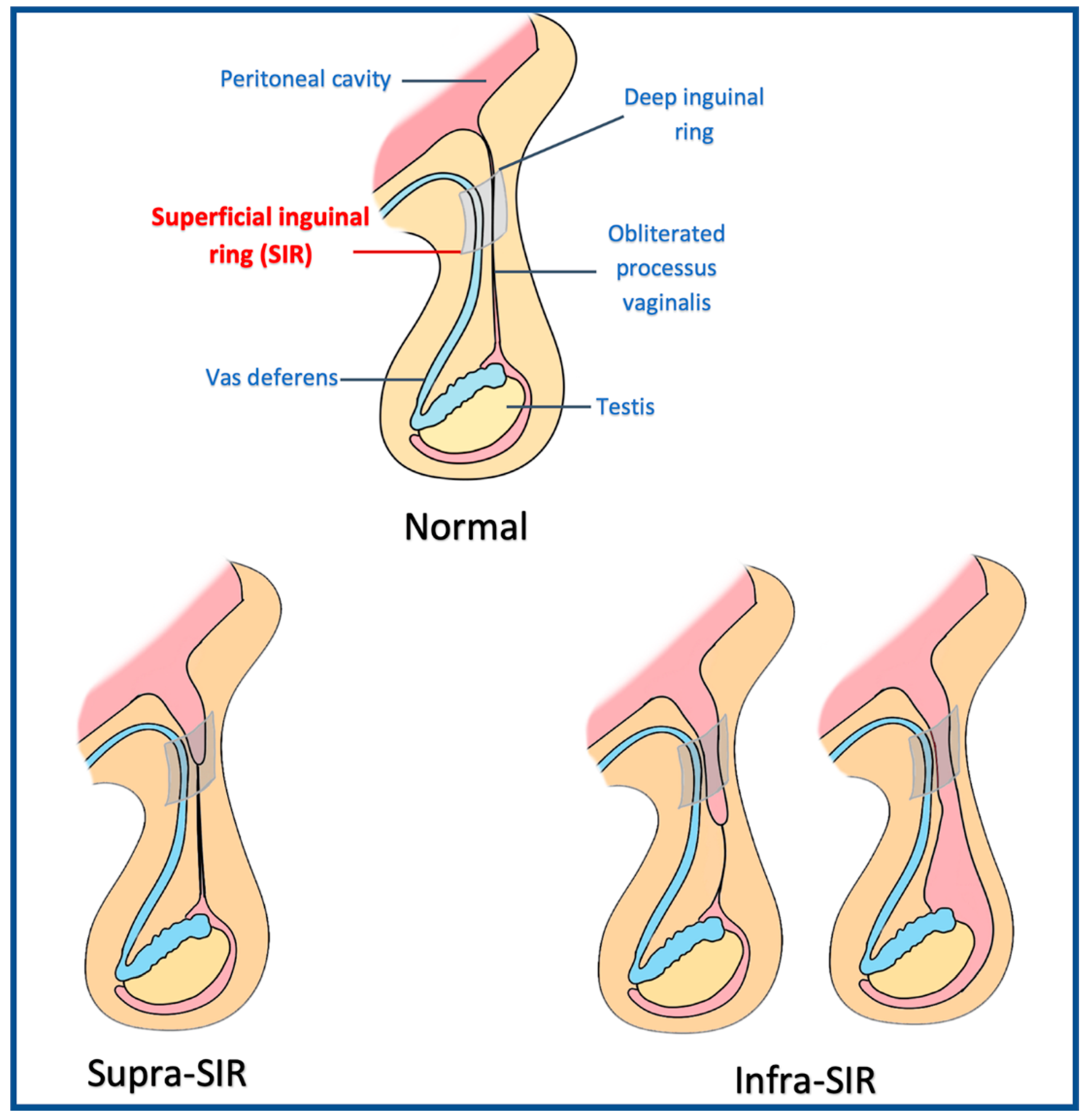
| Hernia size (%) | ||
| Supra-SIR | 137 (77%) | 80 (72%) |
| Infra-SIR | 41 (23%) | 30 (27%) |
| Unilateral | Bilateral | |
|---|---|---|
| Operative time (mins) | 66 ± 26 | 100 ± 39 |
| Hernia type (%) | ||
| Direct | 34 (13.5%) | 60 (54.5%) |
| Indirect | 135 (75.8%) | 42 (38.2%) |
| pantaloon | 5 (2.8%) | 4 (3.6%) |
| prior herniorrhaphy with recurrence | 4 (2.2%) | 4 (3.6%) |
| Peritoneal tear (%) | 35 (19.6%) | 8 (14.5%) |
| Mesh (%) | ||
| Parietex hydrophilic anatomical, polyester mesh (Medtronic, USA) | 111 (62.3%) | 10 (9.1%) |
| Lightweight monofilament polypropylene mesh (Davol, Bard, USA) | 67 (37.6%) | 100 (90.9%) |
| Conversion to open procedure (%) | 1 (0.5%) | 2 (1.18%) |
| Unilateral (n = 178) | Bilateral (n = 55) | p | |
|---|---|---|---|
| Hospital stays after surgery (days), mean ± SD | 1.2 ± 0.5 | 1.3 ± 0.5 | 0.215 |
| Numerical pain rating scale, mean ± SD | 1.6 ± 0.9 | 1.9 ± 1 | 0.138 |
| Number of patients using additional analgesics * | 30 (16.9%) | 7 (12.7%) | 0.243 |
| Number of complications | |||
| Seroma | 5 (2.8 %) | 2 (3.6%) | 0.237 |
| Prolonged Spermatic cord pain | 11 (6.2%) | 6 (10.9%) | 0.243 |
| Urinary retention | 2 (1.1%) | 0 | 0.999 |
| Delayed abscess | 0 | 1 (1.8%) | 0.236 |
| Obesity (BMI ≥ 25) (n = 57) | Non-Obesity (BMI < 23) (n = 60) | p | |
|---|---|---|---|
| Hernia size (%) | 0.558 | ||
| Supra-SIR | 41 (71.9%) | 46 (76.7%) | |
| Infra-SIR | 16 (28.1%) | 14 (23.3%) | |
| Peritoneal tear (%) | 9 (15.8%) | 17 (28.3%) | 0.103 |
| Operative time (mins) | 68.6 ± 23 | 66.5 ± 30.1 | 0.671 |
| Hospitalization (days), mean ± SD | 1.2 ± 0.5 | 1.2 ± 0.5 | 0.788 |
| Numerical pain rating scale, mean ± SD | 1.6 ± 0.9 | 1.8 ± 0.9 | 0.255 |
| Number of complications | |||
| Seroma | 2 (3.5%) | 1 (1.7%) | 0.612 |
| Prolonged spermatic cord pain | 4 (7.0%) | 2 (3.3%) | 0.431 |
| Urinary retention | 1 (1.8%) | 1 (1.7%) | 0.999 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tee, W.-Q.; Wu, Y.-T.; Wang, H.-J.; Chuang, Y.-C.; Lee, W.-C.; Tsai, C.-H.; Lee, L.-Y.; Chen, C.-H. Laparoendoscopic Single-Site Inguinal Herniorrhaphy: Experience of a Single Institute. J. Clin. Med. 2023, 12, 1786. https://doi.org/10.3390/jcm12051786
Tee W-Q, Wu Y-T, Wang H-J, Chuang Y-C, Lee W-C, Tsai C-H, Lee L-Y, Chen C-H. Laparoendoscopic Single-Site Inguinal Herniorrhaphy: Experience of a Single Institute. Journal of Clinical Medicine. 2023; 12(5):1786. https://doi.org/10.3390/jcm12051786
Chicago/Turabian StyleTee, Wei-Quen, Yen-Ting Wu, Hung-Jen Wang, Yao-Chi Chuang, Wei-Chia Lee, Chia-Hung Tsai, Long-Yuan Lee, and Chien-Hsu Chen. 2023. "Laparoendoscopic Single-Site Inguinal Herniorrhaphy: Experience of a Single Institute" Journal of Clinical Medicine 12, no. 5: 1786. https://doi.org/10.3390/jcm12051786