
Following Evidence-Based Recommendations for Perioperative Pain Management after Cesarean Section Is Associated with Better Pain-Related Outcomes: Analysis of Registry Data †
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Data Collection for Each Woman Involved Two Questionnaires Addressing
- (1)
- Demographic characteristics, anesthesia, and surgery data include age, country of birth, type of CS (International Classification of Disease Procedure Codes, [ICD9] Code 74.x), anesthetic technique (general anesthesia, [GA]; regional anesthesia, [RA]: spinal, epidural, combined spinal epidural; GA and RA [=combined]), duration of surgery, and medications for pain administered intra-operatively and on the obstetric ward. Lastly, whether there was a record of post-operative assessment made by the nursing or medical staff.
- (2)
- Pain-related PROs using the International Pain Outcomes Questionnaire [11]. The questionnaire consists of 13 questions evaluating four outcome domains, all in relation to the time since surgery: (a) intensity of pain (worst, least pain, time spent in severe pain); (b) interference of pain with activities (changing position in bed, taking a deep breath or coughing, sleep) and with emotions (anxiety and helplessness); (c) side effects (nausea, drowsiness, itch, dizziness); and (d) perception of care (would have liked more pain treatment than received, satisfied with results of pain treatment). Most PROs are scored using a 0–10 numerical rating scale (NRS), and “I would have liked more treatment” is dichotomous (Yes/No). Lastly, women were asked about the existence and severity of pain lasting for at least 3 months before surgery. The questionnaire’s psychometric properties have been validated. The questionnaire has been translated into 29 languages using a standardized methodology. The questionnaire can be downloaded from the PAIN OUT website.
2.3. Elements of Perioperative Pain Care That Were Evaluated
- The three elements of care included:
- Intra-operative phase:
- Post-operative phase:
- (1)
- “Full peri-operative care” (= “full” care): if all three elements were administered during the intra- and post-operative phases, we regarded this as treatment conforming to the recommendations.
- (2)
- “Intra-operative care”: if only the ‘intra-operative phase’ elements were administered.
- (3)
- “Post-operative care”: if only the recovery and ward elements were administered.
- (4)
- “Incomplete care”: if at least one element was missing from each of the two treatment phases, above.
2.4. A Pain Composite Score
2.5. Study Outcomes
2.6. Statistical Analysis
3. Results
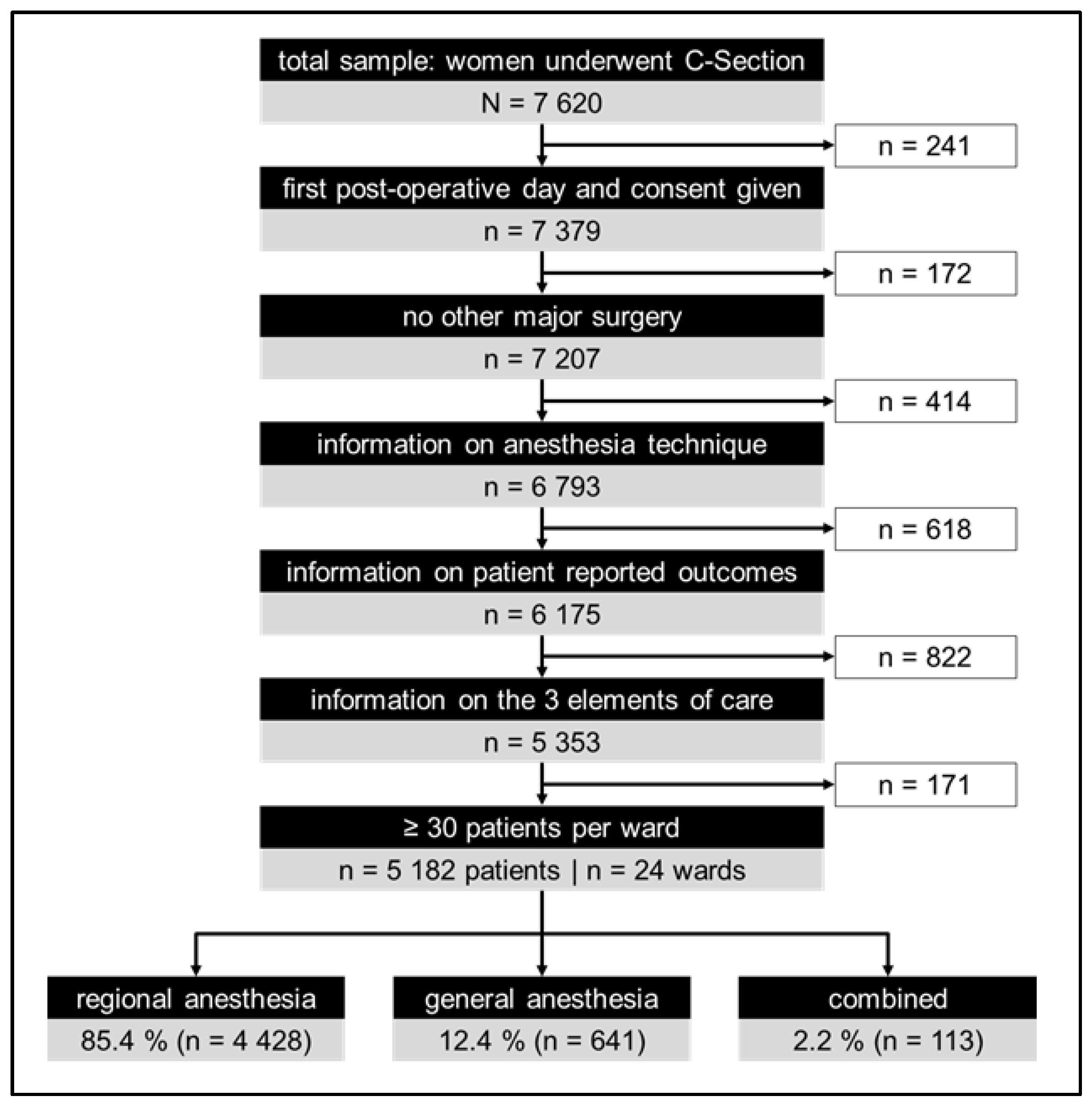
3.1. Sample Description
3.2. Analgesics Administered
3.2.1. Neuraxial Opioids
3.2.2. Non-Opioid Analgesics
3.3. Perioperative Care Groups
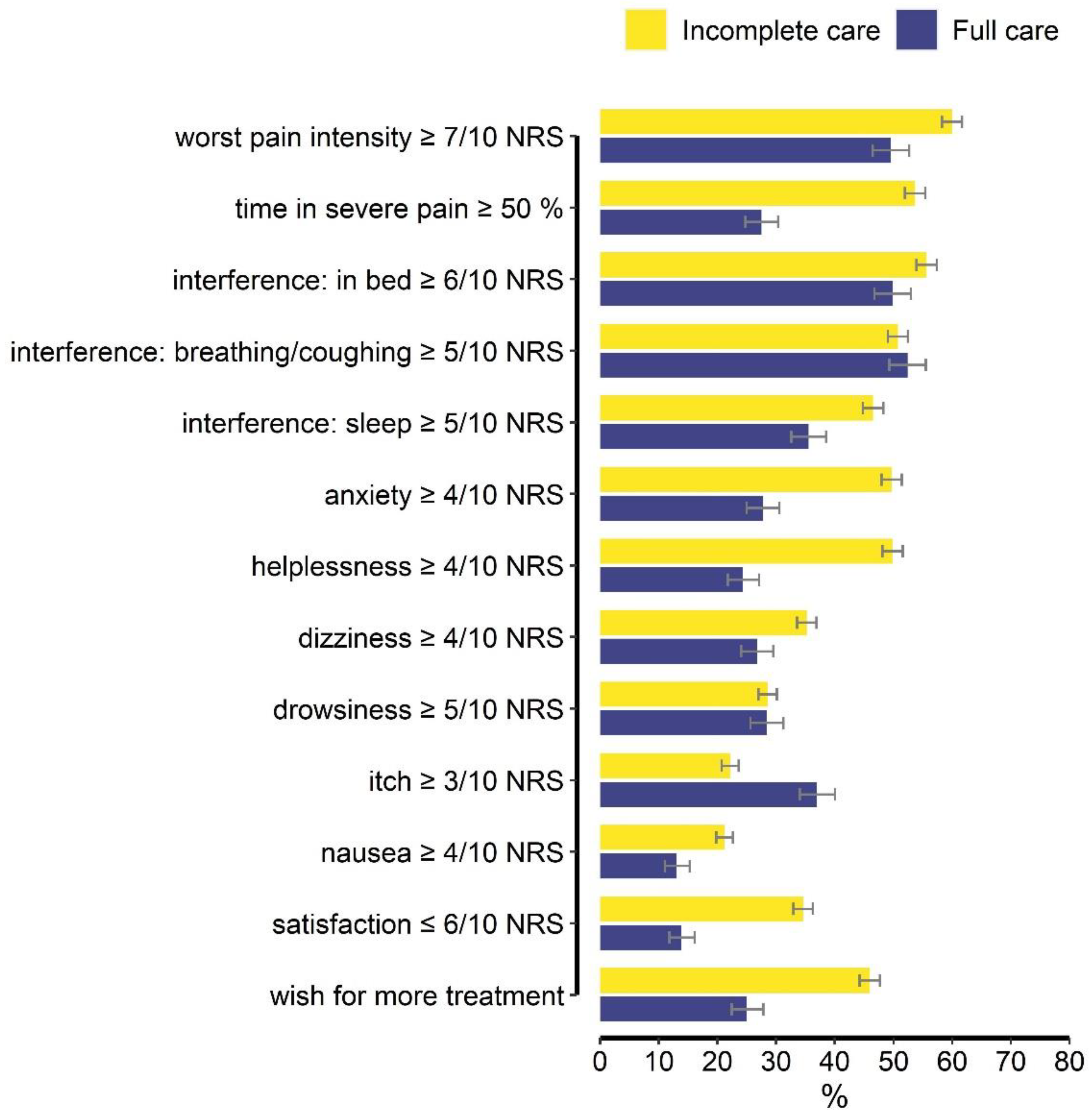
3.4. PROs for the Total Cohort
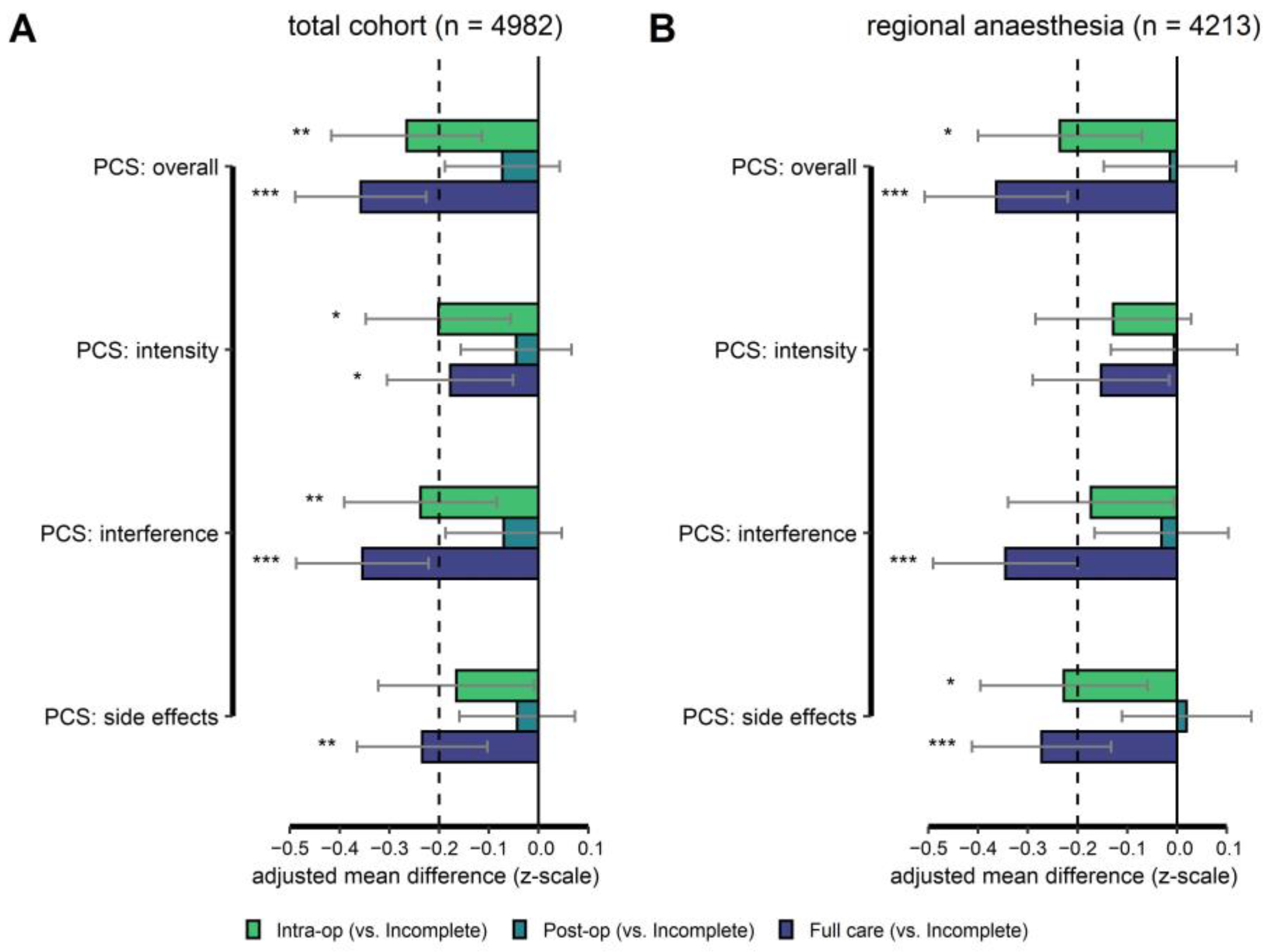
3.5. Regression Models
3.5.1. Primary Endpoint
3.5.2. Secondary Endpoints
3.5.3. Additional Associations with PCStotal
4. Discussion
4.1. Individual PROs in “Full” versus “Incomplete” Care Groups
4.2. Evidence about the Treatment Elements We Evaluated
4.3. Factors Associated with a Higher Pain Composite Score (PCStotal)
4.4. Strategies of Evaluating Care and Effect on Outcomes
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boerma, T.; Ronsmans, C.; Melesse, D.Y.; Barros, A.J.D.; Barros, F.C.; Juan, L.; Moller, A.B.; Say, L.; Hosseinpoor, A.R.; Yi, M.; et al. Global epidemiology of use of and disparities in caesarean sections. Lancet 2018, 392, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Cruz, J.J.; Kather, A.; Nicolaus, K.; Rengsberger, M.; Mothes, A.R.; Schleussner, E.; Meissner, W.; Runnebaum, I.B. Acute postoperative pain in 23 procedures of gynaecological surgery analysed in a prospective open registry study on risk factors and consequences for the patient. Sci. Rep. 2021, 11, 22148. [Google Scholar] [CrossRef] [PubMed]
- Marcus, H.; Gerbershagen, H.J.; Peelen, L.M.; Aduckathil, S.; Kappen, T.H.; Kalkman, C.J.; Meissner, W.; Stamer, U.M. Quality of pain treatment after caesarean section: Results of a multicentre cohort study. Eur. J. Pain 2015, 19, 929–939. [Google Scholar] [CrossRef] [PubMed]
- Lavand’homme, P. Postoperative cesarean pain: Real but is it preventable? Curr. Opin. Anaesthesiol. 2018, 31, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Sutton, C.D.; Carvalho, B. Optimal Pain Management After Cesarean Delivery. Anesthesiol. Clin. 2017, 35, 107–124. [Google Scholar] [CrossRef]
- Reed, S.E.; Tan, H.S.; Fuller, M.E.; Krishnamoorthy, V.; Ohnuma, T.; Raghunathan, K.; Habib, A.S. Analgesia After Cesarean Delivery in the United States 2008-2018: A Retrospective Cohort Study. Anesth. Analg. 2021, 133, 1550–1558. [Google Scholar] [CrossRef]
- Tomson, C.R.; van der Veer, S.N. Learning from practice variation to improve the quality of care. Clin. Med. 2013, 13, 19–23. [Google Scholar] [CrossRef]
- McGlynn, E.A. Improving the Quality of U.S. Health Care—What Will It Take? N. Engl. J. Med. 2020, 383, 801–803. [Google Scholar] [CrossRef]
- Schwann, N.M.; Engstrom, R.H.; Shernan, S.K.; Bollen, B.A. Clinical Practice Improvement: Mind the Gap or Fall Into the Chasm. Anesth. Analg. 2019, 128, 19–20. [Google Scholar] [CrossRef]
- Gerbershagen, H.J.; Aduckathil, S.; van Wijck, A.J.; Peelen, L.M.; Kalkman, C.J.; Meissner, W. Pain intensity on the first day after surgery: A prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013, 118, 934–944. [Google Scholar] [CrossRef]
- Rothaug, J.; Zaslansky, R.; Schwenkglenks, M.; Komann, M.; Allvin, R.; Backström, R.; Brill, S.; Buchholz, I.; Engel, C.; Fletcher, D.; et al. Patients’ perception of postoperative pain management: Validation of the International Pain Outcomes (IPO) questionnaire. J. Pain 2013, 14, 1361–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaslansky, R.; Rothaug, J.; Chapman, C.R.; Bäckström, R.; Brill, S.; Fletcher, D.; Fodor, L.; Gordon, D.B.; Komann, M.; Konrad, C.; et al. PAIN OUT: The making of an international acute pain registry. Eur. J. Pain 2015, 19, 490–502. [Google Scholar] [CrossRef] [PubMed]
- C-Section. Better Postoperative Pain Management (prospect). Available online: https://archive.postoppain.org/ (accessed on 20 December 2020).
- Schug, S.A.; Palmer, G.M.; Scott, D.A.; Alcock, M.; Halliwell, R.; Mott, J.F. (Eds.) Acute Pain Management: Scientific Evidence, 5th ed.; ANZCA & FPM: Melbourne, Australia, 2020. [Google Scholar]
- Chou, R.; Gordon, D.B.; de Leon-Casasola, O.A.; Rosenberg, J.M.; Bickler, S.; Brennan, T.; Carter, T.; Cassidy, C.L.; Chittenden, E.H.; Degenhardt, E.; et al. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J. Pain 2016, 17, 131–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colvin, J.R.; Pedon, C.J. (Eds.) Raising the Standard: A compendium of Audit Recipes for Continuous Quality Improvement in Anaesthesia; The Royal College of Anaesthetists: London, UK, 2012. [Google Scholar]
- National Collaborating Centre for Women’s and Children’s Health. Caesarean Section, NICE Clinical Guideline [CG132]; Royal College of Obstetricians and Gynaecologists: London, UK, 2011. [Google Scholar]
- Stamenkovic, D.M.; Bezmarevic, M.; Bojic, S.; Unic-Stojanovic, D.; Stojkovic, D.; Slavkovic, D.Z.; Bancevic, V.; Maric, N.; Karanikolas, M. Updates on Wound Infiltration Use for Postoperative Pain Management: A Narrative Review. J. Clin. Med. 2021, 10, 4659. [Google Scholar] [CrossRef]
- ACOG Committee. Clinical Guidelines and Standardization of Practice to Improve Outcomes: ACOG Committee Opinion Summary, Number 792. Obstet. Gynecol. 2019, 134, 894–895. [Google Scholar] [CrossRef]
- Joshi, G.P.; Van de Velde, M.; Kehlet, H. Development of evidence-based recommendations for procedure-specific pain management: PROSPECT methodology. Anaesthesia 2019, 74, 1298–1304. [Google Scholar] [CrossRef] [Green Version]
- Cooper, S.A.; Desjardins, P.J.; Turk, D.C.; Dworkin, R.H.; Katz, N.P.; Kehlet, H.; Ballantyne, J.C.; Burke, L.B.; Carragee, E.; Cowan, P.; et al. Research design considerations for single-dose analgesic clinical trials in acute pain: IMMPACT recommendations. Pain 2016, 157, 288–301. [Google Scholar] [CrossRef]
- Ultsch, A.; Lötsch, J. Computed ABC Analysis for Rational Selection of Most Informative Variables in Multivariate Data. PLoS ONE 2015, 10, e0129767. [Google Scholar] [CrossRef] [Green Version]
- Serlin, R.C.; Mendoza, T.R.; Nakamura, Y.; Edwards, K.R.; Cleeland, C.S. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain 1995, 61, 277–284. [Google Scholar] [CrossRef]
- Zaslansky, R. Status quo of pain-related patient reported outcomes and perioperative pain management in 10 415 patients from 10 countries: Analysis of registry data. Eur. J. Pain 2022, 26, 2120–2144. [Google Scholar] [CrossRef]
- Ip, H.Y.; Abrishami, A.; Peng, P.W.; Wong, J.; Chung, F. Predictors of postoperative pain and analgesic consumption: A qualitative systematic review. Anesthesiology 2009, 111, 657–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- R Studio Team. RStudio: Integrated Development for R; RStudio Inc.: Boston, MA, USA, 2019. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gewandter, J.S.; McDermott, M.P.; Evans, S.; Katz, N.P.; Markman, J.D.; Simon, L.S.; Turk, D.C.; Dworkin, R.H. Composite outcomes for pain clinical trials: Considerations for design and interpretation. Pain 2021, 162, 1899–1905. [Google Scholar] [CrossRef]
- Hofer, D.M.; Lehmann, T.; Zaslansky, R.; Harnik, M.; Meissner, W.; Stüber, F.; Stamer, U.M. Re-thinking the definition of CPSP: Composites of patient-reported pain-related outcomes versus pain intensities alone. Pain 2022, 163, 2457–2465. [Google Scholar] [CrossRef]
- Stamer, U.M.; Ehrler, M.; Lehmann, T.; Meissner, W.; Fletcher, D. Pain-related functional interference in patients with chronic neuropathic postsurgical pain: An analysis of registry data. Pain 2019, 160, 1856–1865. [Google Scholar] [CrossRef]
- Guasch, E.; Brogly, N.; Mercier, F.J.; Ioscovich, A.; Weiniger, C.F.; Lucas, N.; Chassard, D.; Kranke, P.; Whitaker, D.; Geldner, G.; et al. European minimum standards for obstetric analgesia and anaesthesia departments: An experts’ consensus. Eur. J. Anaesthesiol. 2020, 37, 1115–1125. [Google Scholar] [CrossRef]
- Bollag, L.; Lim, G.; Sultan, P.; Habib, A.S.; Landau, R.; Zakowski, M.; Tiouririne, M.; Bhambhani, S.; Carvalho, B. Society for Obstetric Anesthesia and Perinatology: Consensus Statement and Recommendations for Enhanced Recovery After Cesarean. Anesth. Analg. 2021, 132, 1362–1377. [Google Scholar] [CrossRef]
- Dahl, J.B.; Jeppesen, I.S.; Jørgensen, H.; Wetterslev, J.; Møiniche, S. Intraoperative and postoperative analgesic efficacy and adverse effects of intrathecal opioids in patients undergoing cesarean section with spinal anesthesia: A qualitative and quantitative systematic review of randomized controlled trials. Anesthesiology 1999, 91, 1919–1927. [Google Scholar] [CrossRef] [Green Version]
- Roofthooft, E.; Joshi, G.P.; Rawal, N.; Van de Velde, M. PROSPECT guideline for elective caesarean section: Updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia 2021, 76, 665–680. [Google Scholar] [CrossRef]
- Bernstein, J.; Spitzer, Y.; Ohaegbulam, K.; Reddy, S.; Song, J.; Romanelli, E.; Nair, S. The analgesic efficacy of IV acetaminophen for acute postoperative pain in C-section patients: A randomized, double-blind, placebo-controlled study. J. Matern. Fetal Neonatal Med. 2020, 35, 933–940. [Google Scholar] [CrossRef]
- Towers, C.V.; Shelton, S.; van Nes, J.; Gregory, E.; Liske, E.; Smalley, A.; Mobley, E.; Faircloth, B.; Fortner, K.B. Preoperative cesarean delivery intravenous acetaminophen treatment for postoperative pain control: A randomized double-blinded placebo control trial. Am. J. Obstet. Gynecol. 2018, 218, 353E.1–353E.4. [Google Scholar] [CrossRef] [PubMed]
- Bellos, I.; Pergialiotis, V.; Antsaklis, A.; Loutradis, D.; Daskalakis, G. Safety of non-steroidal anti-inflammatory drugs in postpartum period in women with hypertensive disorders of pregnancy: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2020, 56, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Levy, N.; Sturgess, J.; Mills, P. “Pain as the fifth vital sign” and dependence on the “numerical pain scale” is being abandoned in the US: Why? Br. J. Anaesth. 2018, 120, 435–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, D.B. Acute pain assessment tools: Let us move beyond simple pain ratings. Curr. Opin. Anaesthesiol. 2015, 28, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Ray-Griffith, S.L.; Wendel, M.P.; Stowe, Z.N.; Magann, E.F. Chronic pain during pregnancy: A review of the literature. Int. J. Women’s Health 2018, 10, 153–164. [Google Scholar] [CrossRef] [Green Version]
- Schug, S.A.; Bruce, J. Risk stratification for the development of chronic postsurgical pain. Pain Rep. 2017, 2, e627. [Google Scholar] [CrossRef]
- Schwenkglenks, M.; Gerbershagen, H.J.; Taylor, R.S.; Pogatzki-Zahn, E.; Komann, M.; Rothaug, J.; Volk, T.; Yahiaoui-Doktor, M.; Zaslansky, R.; Brill, S.; et al. Correlates of satisfaction with pain treatment in the acute postoperative period: Results from the international PAIN OUT registry. Pain 2014, 155, 1401–1411. [Google Scholar] [CrossRef]
- Nolan, T.; Berwick, D.M. All-or-none measurement raises the bar on performance. JAMA 2006, 295, 1168–1170. [Google Scholar] [CrossRef]
- Resar, R.; Pronovost, P.; Haraden, C.; Simmonds, T.; Rainey, T.; Nolan, T. Using a bundle approach to improve ventilator care processes and reduce ventilator-associated pneumonia. Jt. Comm. J. Qual. Patient Saf. 2005, 31, 243–248. [Google Scholar] [CrossRef]
- Lavallée, J.F.; Gray, T.A.; Dumville, J.; Russell, W.; Cullum, N. The effects of care bundles on patient outcomes: A systematic review and meta-analysis. Implement. Sci. 2017, 12, 142. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.S.; Warren, D.T.; Wu, C.L.; Ballantyne, J.C.; Ginsberg, B.; Rathmell, J.P.; Rosenquist, R.W.; Viscusi, E.R. A lovely idea: Forming an ASRA Acute Postoperative Pain (AcutePOP) database. Reg. Anesth. Pain Med. 2006, 31, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Houle, T.T.; Miller, S.; Lang, J.E.; Booth, J.L.; Curry, R.S.; Harris, L.; Aschenbrenner, C.A.; Eisenach, J.C. Day-to-day experience in resolution of pain after surgery. Pain 2017, 158, 2147–2154. [Google Scholar] [CrossRef] [PubMed]
- Resar, R.; Griffin, F.A.; Haraden, C.; Nolan, T.W. Using Care Bundles to Improve Health Care Quality; IHI Innovation Series white paper; Institute for Healthcare Improvement [IHI]: Cambridge, MA, USA, 2012. [Google Scholar]
- Levy, M.M.; Dellinger, R.P.; Townsend, S.R.; Linde-Zwirble, W.T.; Marshall, J.C.; Bion, J.; Schorr, C.; Artigas, A.; Ramsay, G.; Beale, R.; et al. The Surviving Sepsis Campaign: Results of an international guideline-based performance improvement program targeting severe sepsis. Crit. Care Med. 2010, 38, 367–374. [Google Scholar] [CrossRef] [Green Version]
- Pun, B.T.; Balas, M.C.; Barnes-Daly, M.A.; Thompson, J.L.; Aldrich, J.M.; Barr, J.; Byrum, D.; Carson, S.S.; Devlin, J.W.; Engel, H.J.; et al. Caring for Critically Ill Patients with the ABCDEF Bundle: Results of the ICU Liberation Collaborative in Over 15,000 Adults. Crit. Care Med. 2019, 47, 3–14. [Google Scholar] [CrossRef]
- Apfelbaum, J.L.; Hawkins, J.L.; Agarkar, M.; Bucklin, B.A.; Connis, R.T.; Gambling, D.R.; Mhyre, J.; Nickinovich, D.G.; Sherman, H.; Tsen, L.C.; et al. Practice Guidelines for Obstetric Anesthesia: An Updated Report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia and the Society for Obstetric Anesthesia and Perinatology. Anesthesiology 2016, 124, 270–300. [Google Scholar]
- Grape, S.; Kirkham, K.R.; Albrecht, E. Transversus abdominis plane block versus local anaesthetic wound infiltration for analgesia after caesarean section: A systematic review and meta-analysis with trial sequential analysis. Eur. J. Anaesthesiol. 2021, 39, 244–251. [Google Scholar] [CrossRef]
- Bamigboye, A.A.; Hofmeyr, G.J. Local anaesthetic wound infiltration and abdominal nerves block during caesarean section for postoperative pain relief. Cochrane Database Syst. Rev. 2009, Cd006954. [Google Scholar] [CrossRef]
- Principles of Analgesic Use in the Treatment of Acute Pain and Chronic Cancer Pain, 4th ed.; Clinical Pharmacy; American Pain Society: Chicago, IL, USA, 1999.
- Meissner, W. Akutschmerz Taschenbuch (Acute Pain Pocket Book); Medizinisch Wissenschaftliche Verlagsgesellschaft: Berlin, Germany, 2014. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | Median | Q1 | Q3 | nvalid | ||
|---|---|---|---|---|---|---|
| Age [years] | 31.0 | 27.0 | 35.0 | 5 018 | ||
| Duration of surgery [hh:mm] | 0:50 | 0:37 | 1:05 | 5 114 | ||
| Time to survey [hh:mm] | 23:00 | 19:05 | 26:06 | 5 125 | ||
| Cumulative dose of non-opioid analgesics a [%] | 93.5 | 39.4 | 177.3 | 5 182 | ||
| Total daily doses of opioids on the ward [mg] | ||||||
| Morphine | i.m. | 15 | 10 | 15 | 789 | |
| s.c. | 12 | 6.5 | 16 | 176 | ||
| p.o. | 15 | 15 | 15 | 123 | ||
| Pethidine | i.m. | 100 | 100 | 100 | 700 | |
| Papaveretum | i.m. | 20 | 20 | 20 | 401 | |
| Tramadol | p.o c.r. | 200 | 100 | 200 | 260 | |
| p.o.i.r. | 100 | 50 | 100 | 183 | ||
| i.v. | 300 | 200 | 300 | 147 | ||
| Pain Composite Score-total (PCStotal) [0–10] | Total Cohort | 3.5 | 2.4 | 4.8 | 5 182 | |
| Regional Anesthesia | 3.6 | 2.4 | 4.8 | 4 428 | ||
| General Anesthesia | 3.3 | 2.3 | 4.4 | 641 | ||
| Combined | 3.7 | 2.7 | 5.2 | 113 | ||
| Variable | N | % | nvalid | |||
| Chronic pain (≥3 months before surgery) b | 385 | 7.5 | 5 145 | |||
| Intra-operative: neuraxial morphine | 922 | 17.8 | 5182 | |||
| Ward: non-opioid analgesic | Any | 4 509 | 87.0 | 5 182 | ||
| Paracetamol | 3 369 | 65.0 | ||||
| NSAID | 3 187 | 61.5 | ||||
| Metamizole | 344 | 6.6 | ||||
| Pain assessment by ward staff since return from surgery | yes: | 2210 | 42.6 | 5182 | ||
| no: | 2972 | 57.4 | ||||
| Ward: systemic opioid | 3 108 | 60.0 | 5 182 | |||
| Ward: Patients reporting worst pain ≥ 7/10 NRS and received an opioid | 1160 | 39.1 | 2 968 | |||
| Peri-operative care groups | Total cohort | N | % | nvalid | ||
| Incomplete care | Cohort | 3 251 | 62.7 | 5 182 | ||
| Regional anesthesia | 2 703 | 61.0 | 4 428 | |||
| General anesthesia | 485 | 75.7 | 641 | |||
| Combined RA & GA | 63 | 55.8 | 113 | |||
| Intra-operative care [only] | Cohort | 190 | 3.7 | |||
| Regional anesthesia | 171 | 3.9 | ||||
| General anesthesia | 12 | 1.9 | ||||
| Combined RA & GA | 7 | 6.2 | ||||
| Post-operative care [only] | Cohort | 722 | 13.9 | |||
| Regional anesthesia | 611 | 13.8 | ||||
| General anesthesia | 89 | 13.9 | ||||
| Combined RA & GA | 22 | 19.5 | ||||
| Full peri-operative care | Cohort | 1 019 | 19.7 | |||
| Regional anesthesia | 943 | 21.3 | ||||
| General anesthesia | 55 | 8.6 | ||||
| Combined RA & GA | 21 | 18.6 | ||||
| Substances and Combinations | |||||
|---|---|---|---|---|---|
| n | % | Morphine | Fentanyl | Sufentanil | |
| 2735 | 52.8 | No | yes | no | |
| 532 | 10.3 | Yes | yes | no | |
| 285 | 5.5 | No | no | yes | |
| 242 | 4.7 | Yes | no | yes | |
| 142 | 2.8 | Yes | no | no | |
| 38 | 0.7 | other opioid combinations | |||
| 1212 | 23.4 | no NA or with local anesthetics only | |||
| total: | 5182 | 100 | 922 (17.8%) | 3275 (63.2%) | 537 (10.4%) |
| (A). Total Cohort [n = 4982] | (B). Regional Anesthesia (RA) [n = 4213] | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Reference | βz | 95% CI | p | βz | 95% CI | p | ||
| (intercept) | −0.27 | −0.58 | 0.05 | 0.114 | −0.30 | −0.66 | 0.07 | 0.125 | |
| Peri-operative care group: | |||||||||
| Intra-operative [only] | [vs. Incomplete] | −0.27 | −0.42 | −0.11 | 0.001 | −0.24 | −0.40 | −0.07 | 0.005 |
| Post-operative [only] | [vs. Incomplete] | −0.07 | −0.19 | 0.04 | 0.206 | −0.01 | −0.15 | 0.12 | 0.837 |
| Full care | [vs. Incomplete] | −0.36 | −0.49 | −0.23 | <0.001 | −0.36 | −0.51 | −0.22 | <0.001 |
| Anesthesia: | not modelled | ||||||||
| General anesthesia | [vs. RA ] | 0.16 | 0.04 | 0.28 | 0.009 | ||||
| Combined RA & GA | [vs. RA] | 0.04 | −0.14 | 0.22 | 0.663 | ||||
| Age | [years] | 0.00 | −0.01 | 0.00 | 0.140 | 0.00 | −0.01 | 0.00 | 0.266 |
| Pre-existing chronic pain | [vs. no] | 0.21 | 0.11 | 0.31 | <0.001 | 0.17 | 0.07 | 0.28 | 0.002 |
| Intra-operative: neuraxial morphine | [vs. others/none] | not modelled | −0.16 | −0.27 | −0.05 | 0.004 | |||
| Ward: opioid | [vs. no] | 0.17 | 0.10 | 0.25 | <0.001 | 0.20 | 0.12 | 0.28 | <0.001 |
| Income level: high | [vs. others] | 0.32 | −0.06 | 0.70 | 0.119 | 0.31 | −0.11 | 0.73 | 0.162 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaslansky, R.; Baumbach, P.; Edry, R.; Chetty, S.; Min, L.S.; Schaub, I.; Cruz, J.J.; Meissner, W.; Stamer, U.M. Following Evidence-Based Recommendations for Perioperative Pain Management after Cesarean Section Is Associated with Better Pain-Related Outcomes: Analysis of Registry Data. J. Clin. Med. 2023, 12, 676. https://doi.org/10.3390/jcm12020676
Zaslansky R, Baumbach P, Edry R, Chetty S, Min LS, Schaub I, Cruz JJ, Meissner W, Stamer UM. Following Evidence-Based Recommendations for Perioperative Pain Management after Cesarean Section Is Associated with Better Pain-Related Outcomes: Analysis of Registry Data. Journal of Clinical Medicine. 2023; 12(2):676. https://doi.org/10.3390/jcm12020676
Chicago/Turabian StyleZaslansky, Ruth, Philipp Baumbach, Ruth Edry, Sean Chetty, Lim Siu Min, Isabelle Schaub, Jorge Jimenez Cruz, Winfried Meissner, and Ulrike M. Stamer. 2023. "Following Evidence-Based Recommendations for Perioperative Pain Management after Cesarean Section Is Associated with Better Pain-Related Outcomes: Analysis of Registry Data" Journal of Clinical Medicine 12, no. 2: 676. https://doi.org/10.3390/jcm12020676