
A Longitudinal Follow-Up Study of Intellectual Function in Duchenne Muscular Dystrophy over Age: Is It Really Stable?
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Cognitive Tests
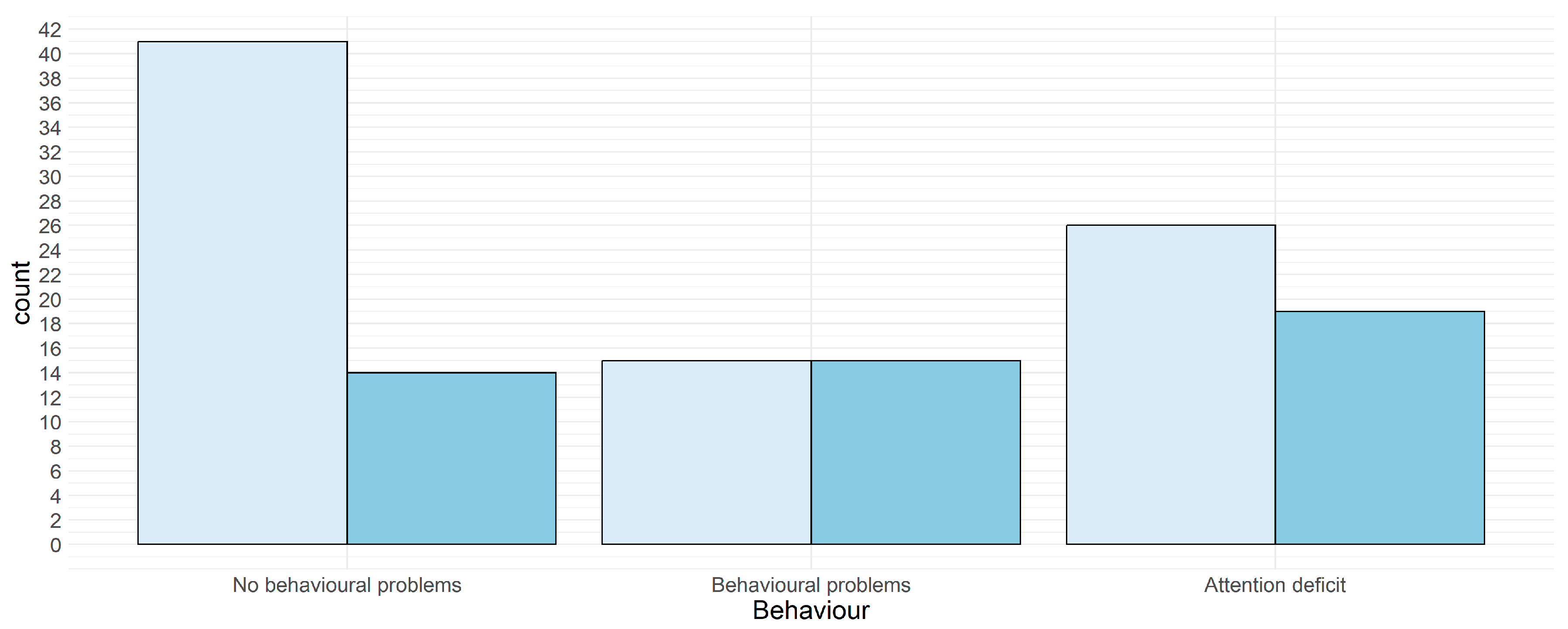
3.2. Behavioral Problems
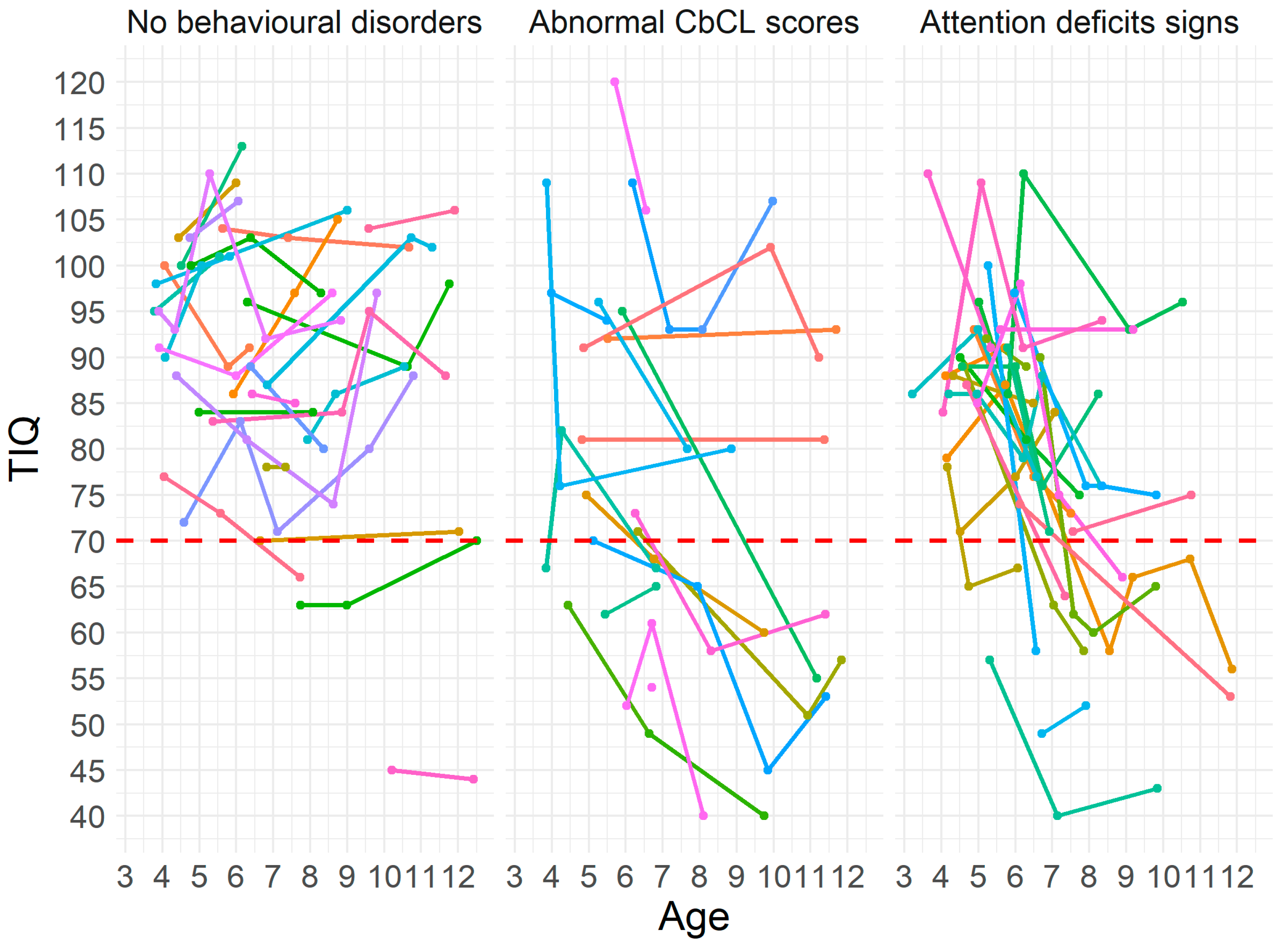
3.2.1. Cognitive Changes and Behavioral Findings
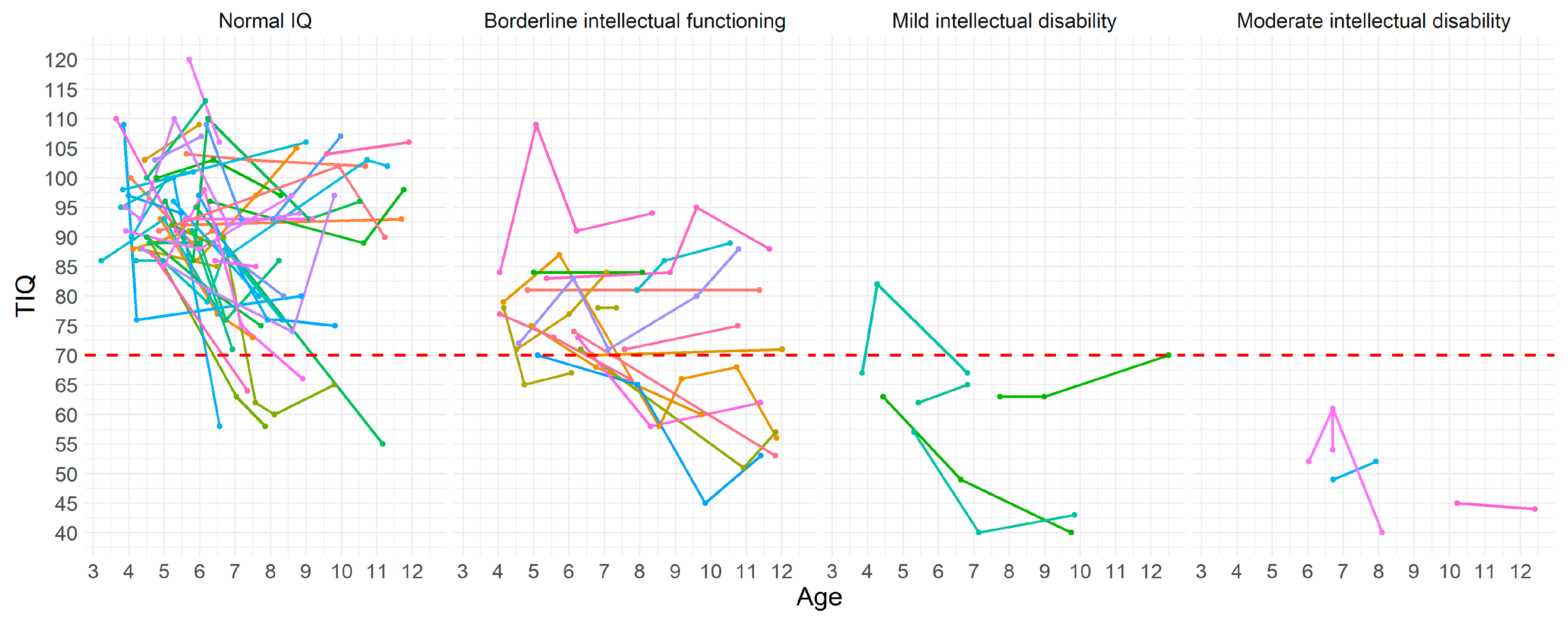
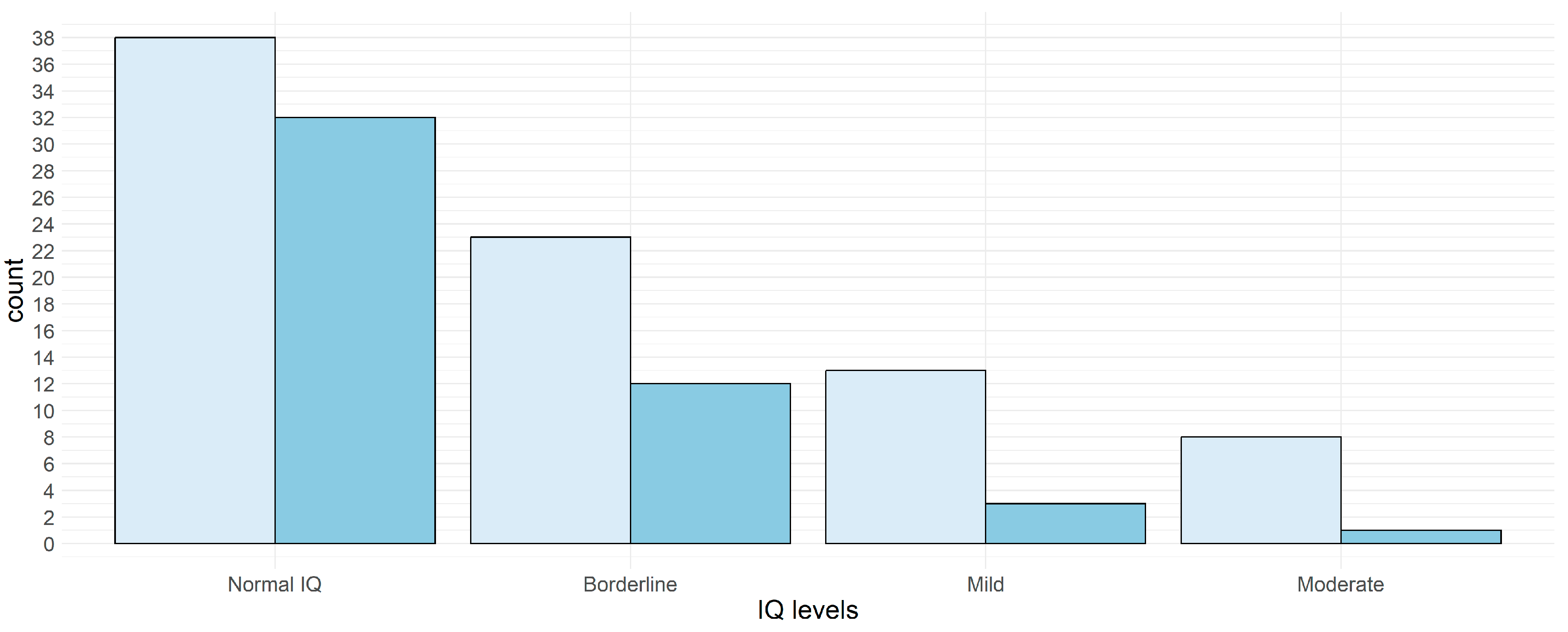
3.2.2. Cognitive Changes and Cognitive Profile
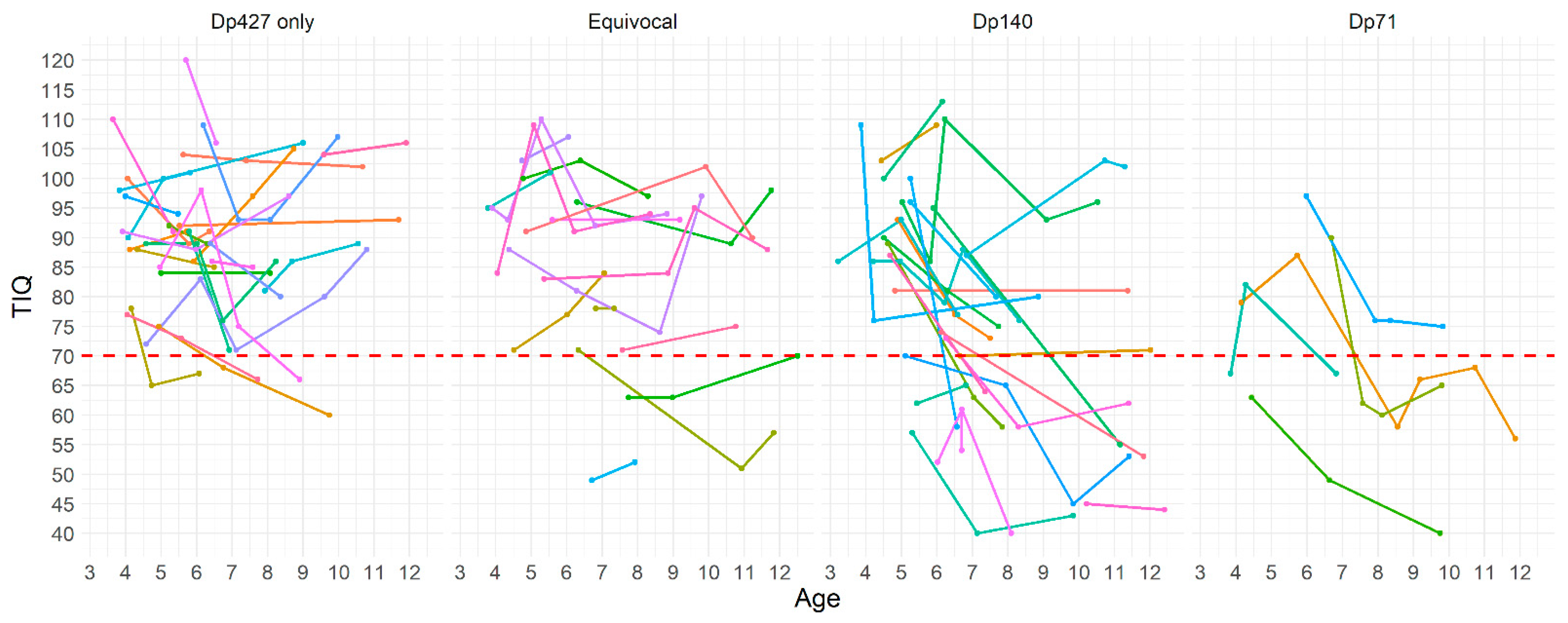
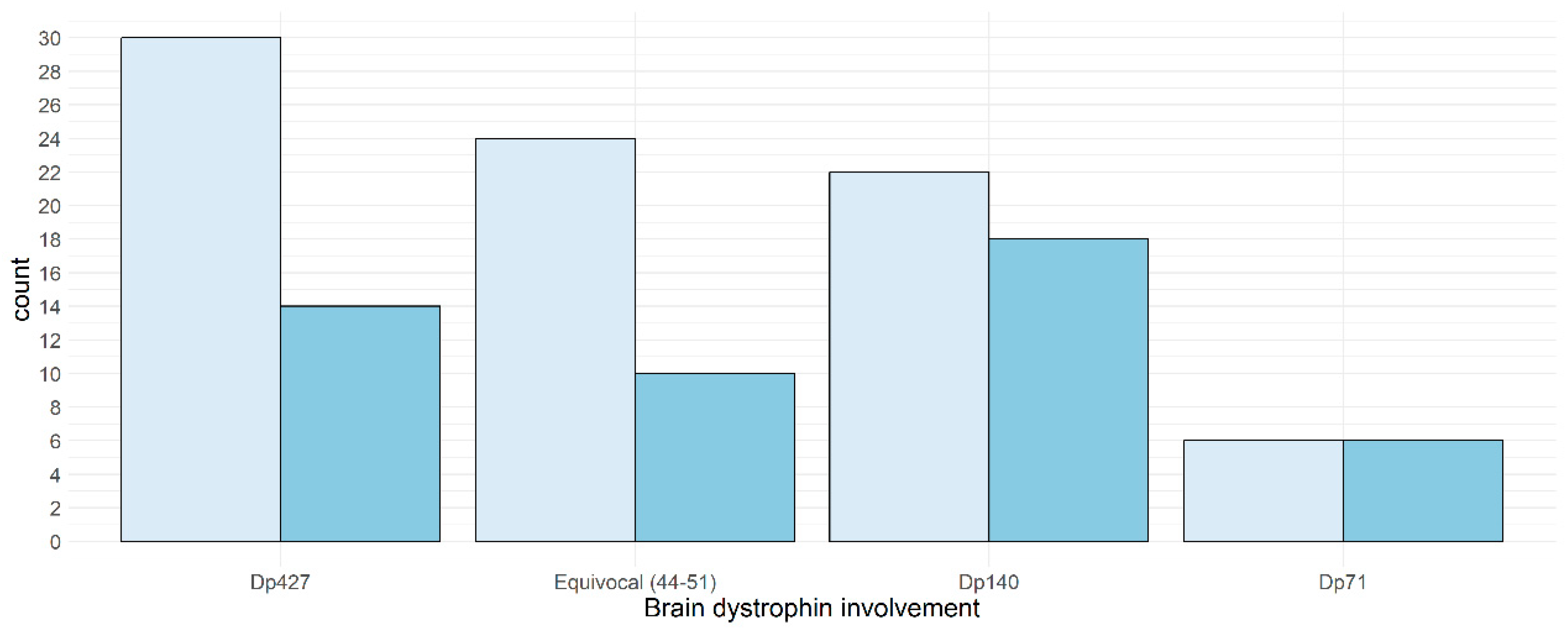
3.2.3. Cognitive Changes and Brain Dystrophins Involvement
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leibowitz, D.; Dubowitz, V. Intellect and Behaviour in Duchenne Muscular Dystrophy. Dev. Med. Child. Neurol. 1981, 23, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Chieffo, D.; Brogna, C.; Berardinelli, A.; D’Angelo, G.; Mallardi, M.; D’Amico, A.; Alfieri, P.; Mercuri, E.; Pane, M. Early Neurodevelopmental Findings Predict School Age Cognitive Abilities in Duchenne Muscular Dystrophy: A Longitudinal Study. PLoS ONE 2015, 10, e0133214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battini, R.; Lenzi, S.; Lucibello, S.; Chieffo, D.; Moriconi, F.; Cristofani, P.; Bulgheroni, S.; Cumbo, F.; Pane, M.; Baranello, G.; et al. Longitudinal data of neuropsychological profile in a cohort of Duchenne muscular dystrophy boys without cognitive impairment. Neuromuscul. Disord. 2021, 31, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, R.; Podder, V.; Arvind, H.; Mohanty, M.; Anand, A. The Role of Dystrophin Gene Mutations in Neuropsychological Domains of DMD Boys: A Longitudinal Study. Ann. Neurosci. 2019, 26, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Bresolin, N.; Castelli, E.; Comi, G.; Felisari, G.; Bardoni, A.; Perani, D.; Grassi, F.; Turconi, A.C.; Mazzucchelli, F.; Gallotti, D.; et al. Cognitive impairment in Duchenne muscular dystrophy. Neuromuscul. Disord. 1994, 4, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Hellebrekers, D.M.; Doorenweerd, N.; Sweere, D.J.; van Kuijk, S.M.; Aartsma-Rus, A.M.; Klinkenberg, S.; Vles, J.S.; Hendriksen, J.G. Longitudinal follow-up of verbal span and processing speed in Duchenne muscular dystrophy. Eur. J. Paediatr. Neurol. 2020, 25, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Doorenweerd, N. Combining genetics, neuropsychology and neuroimaging to improve understanding of brain involvement in Duchenne muscular dystrophy—A narrative review. Neuromuscul. Disord. 2020, 30, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Anand, A.; Tyagi, R.; Mohanty, M.; Goyal, M.; Silva, K.R.D.D.; Wijekoon, N. Dystrophin induced cognitive impairment: Mechanisms, models and therapeutic strategies. Ann. Neurosci. 2015, 22, 108–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naidoo, M.; Anthony, K. Dystrophin Dp71 and the Neuropathophysiology of Duchenne Muscular Dystrophy. Mol. Neurobiol. 2019, 57, 1748–1767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricotti, V.; Mandy, W.P.L.; Scoto, M.; Pane, M.; Deconinck, N.; Messina, S.; Mercuri, E.; Skuse, D.H.; Muntoni, F. Neurodevelopmental, emotional, and behavioural problems in Duchenne muscular dystrophy in relation to underlying dystrophin gene mutations. Dev. Med. Child Neurol. 2015, 58, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Pane, M. Attention Deficit Hyperactivity Disorder and Cognitive Function in Duchenne Muscular Dystrophy: Pheno-type-Genotype Correlation. J. Pediatr. 2012, 161, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Hendriksen, J.G.M.; Vles, J.S.H. Neuropsychiatric Disorders in Males With Duchenne Muscular Dystrophy: Frequency Rate of Attention-Deficit Hyperactivity Disorder (ADHD), Autism Spectrum Disorder, and Obsessive—Compulsive Disorder. J. Child Neurol. 2008, 23, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Banihani, R.; Smile, S.; Yoon, G.; Dupuis, A.; Mosleh, M.; Snider, A.; McAdam, L. Cognitive and Neurobehavioral Profile in Boys With Duchenne Muscular Dystrophy. J. Child. Neurol. 2015, 30, 1472–1482. [Google Scholar] [CrossRef]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Hellebrekers, D.M.J.; Lionarons, J.M.; Faber, C.G.; Klinkenberg, S.; Vles, J.S.H.; Hendriksen, J.G.M. Instruments for the Assessment of Behavioral and Psychosocial Functioning in Duchenne and Becker Muscular Dystrophy; a Systematic Review of the Literature. J. Pediatr. Psychol. 2019, 44, 1205–1223. [Google Scholar] [CrossRef] [PubMed]
- Darmahkasih, A.J.; Rybalsky, I.; Tian, C.; Shellenbarger, K.C.; Horn, P.S.; Ma, J.T.L.; Wong, B.L. Neurodevelopmental, behavioral, and emotional symptoms common in Duchenne muscular dystrophy. Muscle Nerve 2020, 61, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Lionarons, J.M.; Hellebrekers, D.M.; Klinkenberg, S.; Faber, C.G.; Vles, J.S.; Hendriksen, J.G. Methylphenidate use in males with Duchenne muscular dystrophy and a comorbid attention-deficit hyperactivity disorder. Eur. J. Paediatr. Neurol. 2018, 23, 152–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.J.; Buckingham, E.; Kauer, A.; Mathews, K. Descriptive Phenotype of Obsessive Compulsive Symptoms in Males With Duchenne Muscular Dystrophy. J. Child. Neurol. 2018, 33, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Hendriksen, J.G.; Klinkenberg, S.; Collin, P.; Wong, B.; Niks, E.H.; Vles, J.S. Diagnosis and treatment of obsessive compulsive behavior in a boy with Duchenne muscular dystrophy and autism spectrum disorder: A case report. Neuromuscul. Disord. 2016, 26, 659–661. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal IQ | BIF | MID | MoID | ||
|---|---|---|---|---|---|
| No behavioral disorders (N) | Dp427 only | 9 | 4 | 0 | 0 |
| Equivocal | 6 | 2 | 1 | 0 | |
| Dp140 | 3 | 1 | 0 | 1 | |
| Dp71 | 0 | 0 | 0 | 0 | |
| Behavioral disorders (N) | Dp427 only | 4 | 1 | 0 | 0 |
| Equivocal | 1 | 1 | 0 | 0 | |
| Dp140 | 3 | 3 | 1 | 1 | |
| Dp71 | 0 | 0 | 2 | 0 | |
| Attention deficits (N) | Dp427 only | 6 | 1 | 0 | 1 |
| Equivocal | 1 | 3 | 0 | 1 | |
| Dp140 | 8 | 1 | 2 | 0 | |
| Dp71 | 2 | 1 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chieffo, D.P.R.; Moriconi, F.; Pane, M.; Lucibello, S.; Ferraroli, E.; Norcia, G.; Ricci, M.; Capasso, A.; Cicala, G.; Buchignani, B.; et al. A Longitudinal Follow-Up Study of Intellectual Function in Duchenne Muscular Dystrophy over Age: Is It Really Stable? J. Clin. Med. 2023, 12, 403. https://doi.org/10.3390/jcm12020403
Chieffo DPR, Moriconi F, Pane M, Lucibello S, Ferraroli E, Norcia G, Ricci M, Capasso A, Cicala G, Buchignani B, et al. A Longitudinal Follow-Up Study of Intellectual Function in Duchenne Muscular Dystrophy over Age: Is It Really Stable? Journal of Clinical Medicine. 2023; 12(2):403. https://doi.org/10.3390/jcm12020403
Chicago/Turabian StyleChieffo, Daniela P. R., Federica Moriconi, Marika Pane, Simona Lucibello, Elisabetta Ferraroli, Giulia Norcia, Martina Ricci, Anna Capasso, Gianpaolo Cicala, Bianca Buchignani, and et al. 2023. "A Longitudinal Follow-Up Study of Intellectual Function in Duchenne Muscular Dystrophy over Age: Is It Really Stable?" Journal of Clinical Medicine 12, no. 2: 403. https://doi.org/10.3390/jcm12020403