

Prediction Value of KREBS Von Den Lungen-6 (KL-6) Biomarker in COVID-19 Patients: A Systematic Review and Meta-Analysis
 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
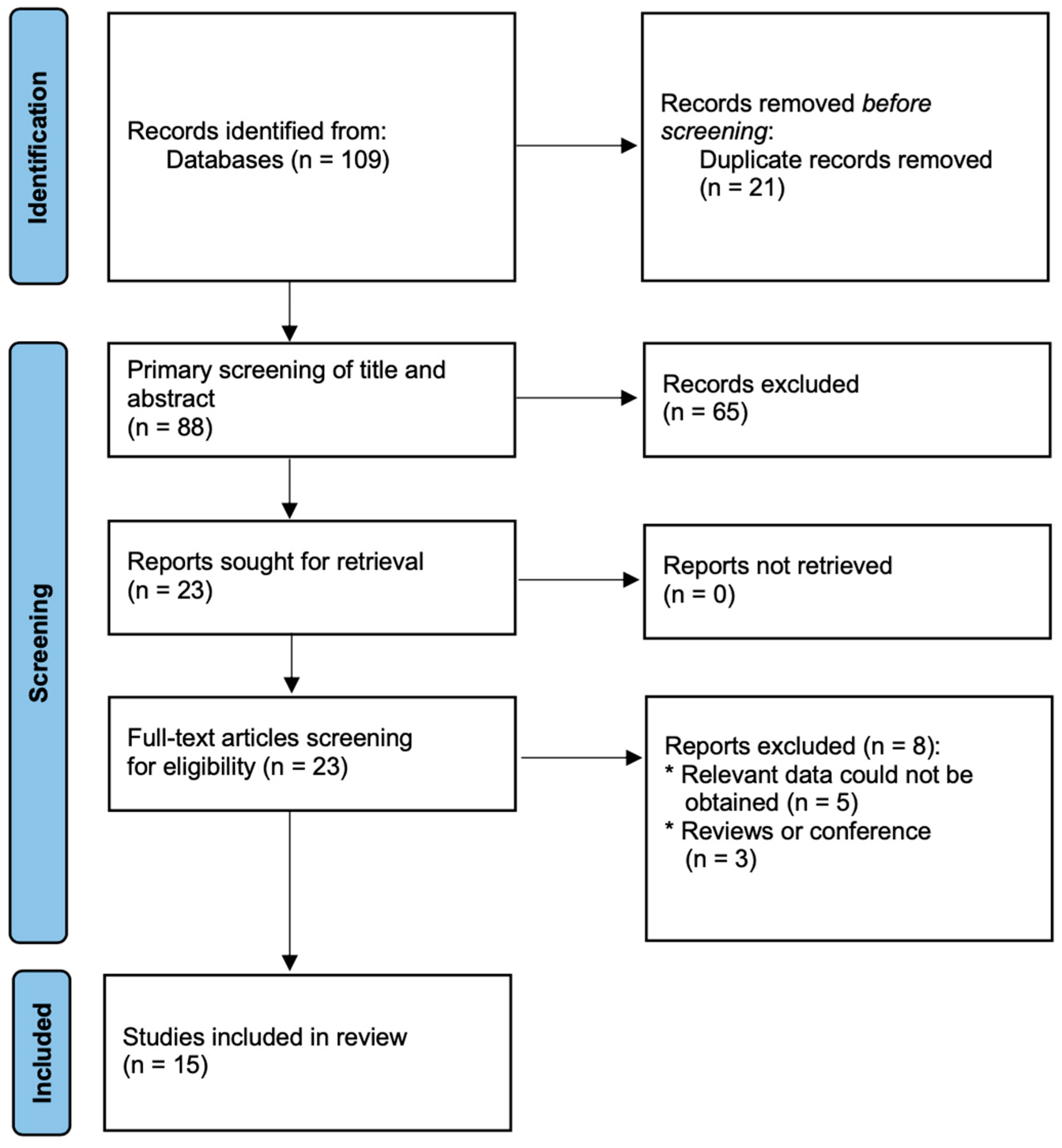
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality and Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
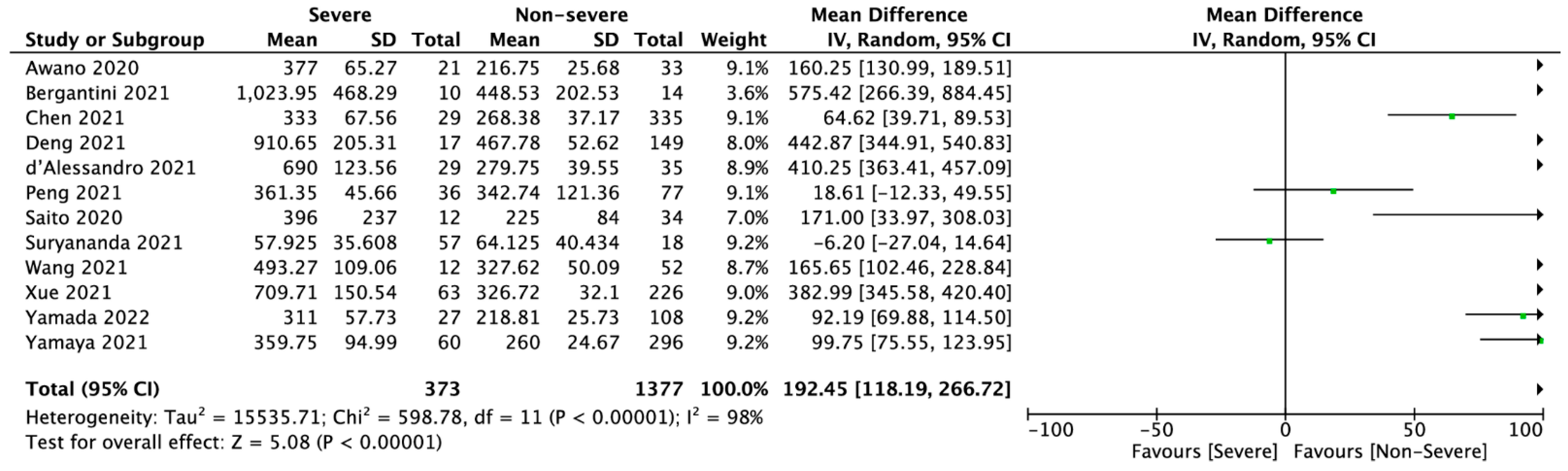
3.2. KL-6 Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dzieciatkowski, T.; Szarpak, L.; Filipiak, K.J.; Jaguszewski, M.; Ladny, J.R.; Smereka, J. COVID-19 challenge for modern medicine. Cardiol. J. 2020, 27, 175–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drożdżal, S.; Rosik, J.; Lechowicz, K.; Machaj, F.; Szostak, B.; Przybyciński, J.; Lorzadeh, S.; Kotfis, K.; Ghavami, S.; Łos, M.J. An update on drugs with therapeutic potential for SARS-CoV-2 (COVID-19) treatment. Drug Resist. Updates 2021, 59, 100794. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Szarpak, L.; Nowak, B.; Kosior, D.; Zaczynski, A.; Filipiak, K.J.; Jaguszewski, M.J. Cytokines as a predictor of COVID-19 severity: Evidence from meta-analysis. Pol. Arch. Intern. Med. 2021, 131, 98–99. [Google Scholar] [CrossRef]
- Bergantini, L.; Bargagli, E.; D’Alessandro, M.; Refini, R.; Cameli, P.; Galasso, L.; Scapellato, C.; Montagnani, F.; Scolletta, S.; Franchi, F.; et al. Prognostic bioindicators in severe COVID-19 patients. Cytokine 2021, 141, 155455. [Google Scholar] [CrossRef] [PubMed]
- Fialek, B.; Pruc, M.; Smereka, J.; Jas, R.; Rahnama-Hezavah, M.; Denegri, A.; Szarpak, A.; Jaguszewski, M.J.; Peacock, F.W.; Szarpak, L. Diagnostic value of lactate dehydrogenase in COVID-19: A systematic review and meta-analysis. Cardiol. J. 2022. [Google Scholar] [CrossRef] [PubMed]
- Fialek, B.; Yanvarova, O.; Pruc, M.; Gasecka, A.; Skrobucha, A.; Boszko, M.; Ducki, C.; Cyran, M.; Szarpak, L. Systematic review and meta-analysis of serum amyloid a prognostic value in patients with COVID-19. Disaster Emerg. Med. J. 2022, 7, 107–113. [Google Scholar] [CrossRef]
- Awano, N.; Inomata, M.; Kuse, N.; Tone, M.; Takada, K.; Muto, Y.; Fujimoto, K.; Akagi, Y.; Mawatari, M.; Ueda, A.; et al. Serum KL-6 level is a useful biomarker for evaluating the severity of coronavirus disease 2019. Respir. Investig. 2020, 58, 440–447. [Google Scholar] [CrossRef]
- Szarpak, L.; Ruetzler, K.; Safiejko, K.; Hampel, M.; Pruc, M.; Koda, L.K.; Filipiak, K.J.; Jaguszewski, M.J. Lactate dehydrogenase level as a COVID-19 severity marker. Am. J. Emerg. Med. 2021, 45, 638–639. [Google Scholar] [CrossRef]
- Napolitano, F.; Di Spigna, G.; Vargas, M.; Iacovazzo, C.; Pinchera, B.; Cernia, D.S.; Ricciardone, M.; Covelli, B.; Servillo, G.; Gentile, I.; et al. Soluble Urokinase Receptor as a Promising Marker for Early Prediction of Outcome in COVID-19 Hospitalized Patients. J. Clin. Med. 2021, 10, 4914. [Google Scholar] [CrossRef]
- Ishikawa, N.; Hattori, N.; Yokoyama, A.; Kohno, N. Utility of KL-6/MUC1 in the clinical management of interstitial lung diseases. Respir. Investig. 2012, 50, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anastasi, E.; Manganaro, L.; Guiducci, E.; Ciaglia, S.; Dolciami, M.; Spagnoli, A.; Alessandri, F.; Angeloni, A.; Vestri, A.; Catalano, C.; et al. Association of serum Krebs von den Lungen-6 and chest CT as potential prognostic factors in severe acute respiratory syndrome SARS-CoV-2: A preliminary experience. Radiol. Med. 2022, 127, 725–732. [Google Scholar] [CrossRef]
- Arnold, D.T.; Donald, C.; Lyon, M.; Hamilton, F.W.; Morley, A.J.; Attwood, M.; Dipper, A.; Barratt, S.L. Krebs von den Lungen 6 (KL-6) as a marker for disease severity and persistent radiological abnormalities following COVID-19 infection at 12 weeks. PLoS ONE 2021, 16, e0249607. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Qin, R.; Huang, Z.; Luo, W.; Zheng, P.; Huang, H.; Hu, H.; Wang, H.; Sun, B. Clinical relevance of serum Krebs von den Lungen-6 levels in patients with coronavirus disease 2019. Cytokine 2021, 148, 155513. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- d’Alessandro, M.; Cameli, P.; Refini, R.M.; Bergantini, L.; Alonzi, V.; Lanzarone, N.; Bennett, D.; Rana, G.D.; Montagnani, F.; Scolletta, S.; et al. Serum KL-6 concentrations as a novel biomarker of severe COVID-19. J. Med. Virol. 2020, 92, 2216–2220. [Google Scholar] [CrossRef]
- Deng, K.; Fan, Q.; Yang, Y.; Deng, X.; He, R.; Tan, Y.; Lan, Y.; Deng, X.; Pan, Y.; Wang, Y.; et al. Prognostic roles of KL-6 in disease severity and lung injury in COVID-19 patients: A longitudinal retrospective analysis. J. Med. Virol. 2021, 93, 2505–2512. [Google Scholar] [CrossRef]
- Frix, A.N.; Schoneveld, L.; Ladang, A.; Henket, M.; Duysinx, B.; Vaillant, F.; Misset, B.; Moutschen, M.; Louis, R.; Cavalier, E.; et al. Could KL-6 levels in COVID-19 help to predict lung disease? Respir. Res. 2020, 21, 309. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Lu, L.; Zong, M.; Zhou, H.; Wang, L.; Chen, N.Z.; Yuan, J.Y.; Jiang, E.P.; Zheng, L.; Li, Q.; et al. The Signicance of KL-6 as Prognosis Monitoring Biomarker in Patients with Severe COVID-19 From Stabilized Stage Toward Convalescence. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Peng, D.-H.; Luo, Y.; Huang, L.-J.; Liao, F.-L.; Liu, Y.-Y.; Tang, P.; Hu, H.-N.; Chen, W. Correlation of Krebs von den Lungen-6 and fibronectin with pulmonary fibrosis in coronavirus disease 2019. Clin. Chim. Acta 2021, 517, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Saito, A.; Kuronuma, K.; Moniwa, K.; Takahashi, S.; Takahashi, H.; Chiba, H. Serum surfactant protein A and D may be novel biomarkers of COVID-19 pneumonia severity. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Suryananda, T.D.; Yudhawati, R. Association of serum KL-6 levels on COVID-19 severity: A cross-sectional study design with purposive sampling. Ann. Med. Surg. 2021, 69, 102673. [Google Scholar] [CrossRef]
- Wang, H.; Chen, L.; Zhang, Y.; Liu, L.; Xu, M.; Gao, Y.; Li, M. Detection of serum KL-6 and SARS-CoV-2 antibody in patients with coronavirus disease 2019 and the diagnostic value in severe disease. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Xue, M.; Zhang, T.; Chen, H.; Zeng, Y.; Lin, R.; Zhen, Y.; Li, N.; Huang, Z.; Hu, H.; Zhou, L.; et al. Krebs Von den Lungen-6 as a predictive indicator for the risk of secondary pulmonary fibrosis and its reversibility in COVID-19 patients. Int. J. Biol. Sci. 2021, 17, 1565–1573. [Google Scholar] [CrossRef]
- Yamada, H.; Okamoto, M.; Nagasaki, Y.; Yoshio, S.; Nouno, T.; Yano, C.; Tanaka, T.; Watanabe, F.; Shibata, N.; Arimizu, Y.; et al. Analysis of Early Biomarkers Associated with the Development of Critical Respiratory Failure in Coronavirus Disease 2019 (COVID-19). Diagnostics 2022, 12, 339. [Google Scholar] [CrossRef]
- Yamaya, T.; Hagiwara, E.; Baba, T.; Kitayama, T.; Murohashi, K.; Higa, K.; Sato, Y.; Otoshi, R.; Tabata, E.; Shintani, R.; et al. Serum Krebs von den Lungen-6 levels are associated with mortality and severity in patients with coronavirus disease 2019. Respir. Investig. 2021, 59, 596–601. [Google Scholar] [CrossRef]
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Post-mortem examination of COVID19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings of lungs and other organs suggesting vascular dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef]
- Batah, S.S.; Fabro, A.T. Pulmonary pathology of ARDS in COVID-19: A pathological review for clinicians. Respir. Med. 2021, 176, 106239. [Google Scholar] [CrossRef]
- Inoue, Y.; Barker, E.; Daniloff, E.; Kohno, N.; Hiwada, K.; Newman, L.S. Pulmonary Epithelial Cell Injury and Alveolar–Capillary Permeability in Berylliosis. Am. J. Respir. Crit. Care Med. 1997, 156, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front Immunol 2018, 9, 754. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Yim, J.-J.; Park, J. Pulmonary function and chest computed tomography abnormalities 6–12 months after recovery from COVID-19: A systematic review and meta-analysis. Respir. Res. 2022, 23, 233. [Google Scholar] [CrossRef] [PubMed]
- Amin, B.J.H.; Kakamad, F.H.; Ahmed, G.S.; Ahmed, S.F.; Abdulla, B.A.; Mohammed, S.H.; Mikael, T.M.; Salih, R.Q.; Ali, R.K.; Salh, A.M.; et al. Post COVID-19 pulmonary fibrosis; a meta-analysis study. Ann. Med. Surg. 2022, 77, 103590. [Google Scholar] [CrossRef] [PubMed]
- Rai, D.K.; Sharma, P.; Kumar, R. Post covid 19 pulmonary fibrosis. Is it real threat? Indian J. Tuberc. 2021, 68, 330–333. [Google Scholar] [CrossRef]
- Xue, M.; Zheng, P.; Bian, X.; Huang, Z.; Huang, H.; Zeng, Y.; Hu, H.; Liu, X.; Zhou, L.; Sun, B.; et al. Exploration and correlation analysis of changes in Krebs von den Lungen-6 levels in COVID-19 patients with different types in China. Biosci. Trends 2020, 14, 290–296. [Google Scholar] [CrossRef]
- Ke, Y.; Zhu, Y.; Chen, S.; Hu, J.; Chen, R.; Li, W.; Liu, S. Clinical Utility of Circulating Pneumoproteins as Diagnostic and Prognostic Biomarkers in COVID-19: A Systematic Review and Meta-analysis. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Naderi, N.; Rahimzadeh, M. Krebs von den Lungen-6 (KL-6) as a clinical marker for severe COVID-19: A systematic review and meta-analyses. Virology 2022, 566, 106–113. [Google Scholar] [CrossRef]
- Witarto, A.P.; Witarto, B.S.; Putra, A.J.E.; Pramudito, S.L.; Rosyid, A.N. Serum Krebs von den Lungen-6 for Predicting the Severity of COVID-19 Lung Injury: A Systematic Review and Meta-Analysis. Iran. Biomed. J. 2021, 25, 381–389. [Google Scholar] [CrossRef]
- Lin, L.; Chu, H. Quantifying publication bias in meta-analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/results?cond=&term=KL-6+&cntry=&state=&city=&dist= (accessed on 4 November 2022).
- Kohno, N.; Ishikawa, N.; Deguchi, N.; Iwamoto, H.; Ohshimo, S.; Fujitaka, K.; Haruta, Y.; Murai, H.; Hattori, N. KL-6 is a useful serum biomarker for early detection of interstitial lung disease. Eur. Respir. J. 2012, 40, P1766. [Google Scholar]
- Zhang, T.; Shen, P.; Duan, C.; Gao, L. KL-6 as an Immunological Biomarker Predicts the Severity, Progression, Acute Exacerbation, and Poor Outcomes of Interstitial Lung Disease: A Systematic Review and Meta-Analysis. Front. Immunol 2021, 12, 745233. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04816760?term=KL-6+COVID-19&draw=2&rank=4 (accessed on 3 November 2022).
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT05074875?term=KL-6+COVID-19&draw=2&rank=5 (accessed on 3 November 2022).
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04392531?term=KL-6+COVID-19&draw=2&rank=2 (accessed on 3 November 2022).
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04390061?term=KL-6+COVID-19&draw=2&rank=3 (accessed on 3 November 2022).
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04541680?term=KL-6+COVID-19&draw=2&rank=7 (accessed on 3 November 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Group | No. of Participants | Age (Years) | Sex, Male (n, %) | NOS Score |
|---|---|---|---|---|---|---|
| Anastasi et al., 2022 [12] | Italy | COVID-19 (+) | 37 | 66.5 ± 6.08 | 18 (48.6%) | 8 |
| COVID-19 (−) | 26 | 71.81 ± 7.27 | 10 (38.5%) | |||
| Awano et al., 2020 [8] | Japan | Severe | 21 | 65.5 ± 6.36 | 15 (71.4%) | 9 |
| Non-severe | 33 | 40.75 ± 4.91 | 23 (69.7%) | |||
| Bergantini et al., 2021 [5] | Italy | Severe | 10 | 65.2 ± 8 | 8 (80.0%) | 8 |
| Non-severe | 14 | 62.2 ± 15.6 | 11 (78.6%) | |||
| COVID-19 (−) | 30 | 59 ± 9.8 | 18 (60.0%) | |||
| Chen et al., 2021 [14] | China | Mild | 37 | NS | NS | 8 |
| Moderate | 298 | NS | NS | |||
| Severe | 29 | NS | NS | |||
| d’Alessandro et al., 2020 [19] | Italy | Severe | 12 | 63 ± 2.34 | 9 (75.0%) | 8 |
| Non-severe | 10 | 60.75 ± 3.71 | 6 (60.0%) | |||
| Deng et al., 2021 [20] | China | Severe | 17 | 57.75 ± 4.35 | 9 (52.9%) | 9 |
| Non-severe | 149 | 48.13 ± 7.94 | 65 (43.6%) | |||
| Frix et al., 2020 [21] | Belgium | COVID-19 (+) | 83 | 71 ± 4 | 52 (62.6%) | 8 |
| COVID-19 (−) | 70 | 58 ± 3 | 35 (50.0%) | |||
| He et al., 2021 [22] | China | COVID-19 (+) | 28 | 64.56 ± 1.55 | 14 (50.0%) | 8 |
| COVID-19 (−) | 25 | 64.93 ± 1.63 | 16 (64.0%) | |||
| Peng et al. 2021 [23] | China | Mild | 49 | 44.5 ± 14 | 25 (51.0%) | 9 |
| Moderate | 28 | 51 ± 13.86 | 12 (42.9%) | |||
| Severe | 36 | 56.5 ± 16.74 | 24 (66.7%) | |||
| COVID-19 (−) | 65 | 47.75 ± 13.56 | 28 (43.1%) | |||
| Saito et al., 2020 [24] | Japan | COVID-19 (+) | 12 | 65.1 ± 10.7 | 7 (58.3%) | 9 |
| COVID-19 (−) | 34 | 49.6 ± 15.7 | 14 (41.2%) | |||
| Suryananda et al., 2021 [25] | Indonesia | Severe | 57 | 50.5 ± 13.85 | 38 (66.7%) | 9 |
| Non-severe | 18 | 49.75 ± 15.59 | 8 (44.4%) | |||
| Wang et al., 2021 [26] | China | Severe | 12 | NS | NS | 8 |
| Non-severe | 52 | NS | NS | |||
| Xue et al., 2021 [27] | China | Severe | 63 | 61.38 ± 4.19 | 31 (49.2%) | 8 |
| Non-severe | 226 | 54.75 ± 4.17 | 99 (43.8%) | |||
| Yamada et al., 2022 [28] | Japan | Severe | 27 | 64.25 ± 6.05 | 21 (77.8%) | 8 |
| Non-severe | 108 | 47 ± 12.85 | 48 (44.4%) | |||
| Yamaya et al., 2021 [29] | Japan | Severe | 60 | NS | NS | 8 |
| Non-severe | 296 | NS | NS |
| ClinicalTrial identifer | Study name | Status | Purpose of using KL-6 | Time Frame |
|---|---|---|---|---|
| NCT04816760 [45] | Immune Cells Phenotypes During COVID-19 (IMMUNO-COVID) | Recruiting | Serum alveolar epithelial and endothelial cells biomarkers during SARS-CoV-2 infection incl. measurement of KL-6 using ELISA. | Day 0, Day 7, Day 14, Day 28 |
| NCT05074875 [46] | COVID-19 Respiratory Outcomes Registry | Active, not recruiting | Examine the effects of COVID-19 on the presence of molecular biomarkers associated with Interstitial Lung Disease. Biomarkers prognostic for progression in PF patients incl. Krebs von den Lungen-6 (KL-6). Biomarkers elevated in PF (vs age-matched controls) incl. Krebs von den Lungen-6 (KL-6). | 72 weeks |
| NCT04392531 [47] | Clinical Trial to Assess Efficacy of cyclosporine Plus Standard of Care in Hospitalized Patients with COVID-19 | Completed- No Results Posted | Change in KL-6 change from baseline in KL-6 levels | Days 1, 8, 15, and end of study visit (14 days after discharge or 14 days after end of study treatment) |
| NCT04390061 [48] | TOFAcitinib Plus Hydroxycloroquine vs Hydroxycloroquine in Patients With COVID-19 Interstitial Pneumonia (TOFACoV-2) | Unknown | Identification of predictors of outcome. Role of some clinical and laboratory factors in predicting outcome incl. KL-6. | 14 days |
| NCT04541680 [49] | Nintedanib for the Treatment of SARS-CoV-2 Induced Pulmonary Fibrosis (NINTECOR) | Recruiting | Compare change in lung injury, pulmonary hypertension, and inflammation biomarkers. Biomarker assay (KL-6, NT-proBNP, CRP, D-dimers) | At inclusion and 12 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matuszewski, M.; Szarpak, L.; Rafique, Z.; Peacock, F.W.; Pruc, M.; Szwed, P.; Chirico, F.; Navolokina, A.; Ladny, J.R.; Denegri, A. Prediction Value of KREBS Von Den Lungen-6 (KL-6) Biomarker in COVID-19 Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 6600. https://doi.org/10.3390/jcm11216600
Matuszewski M, Szarpak L, Rafique Z, Peacock FW, Pruc M, Szwed P, Chirico F, Navolokina A, Ladny JR, Denegri A. Prediction Value of KREBS Von Den Lungen-6 (KL-6) Biomarker in COVID-19 Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(21):6600. https://doi.org/10.3390/jcm11216600
Chicago/Turabian StyleMatuszewski, Michal, Lukasz Szarpak, Zubaid Rafique, Frank W. Peacock, Michal Pruc, Piotr Szwed, Francesco Chirico, Alla Navolokina, Jerzy R. Ladny, and Andrea Denegri. 2022. "Prediction Value of KREBS Von Den Lungen-6 (KL-6) Biomarker in COVID-19 Patients: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 21: 6600. https://doi.org/10.3390/jcm11216600