Nursing Activities Score at Discharge from the Intensive Care Unit Is Associated with Unplanned Readmission to the Intensive Care Unit


Abstract
:1. Introduction
2. Materials and Methods
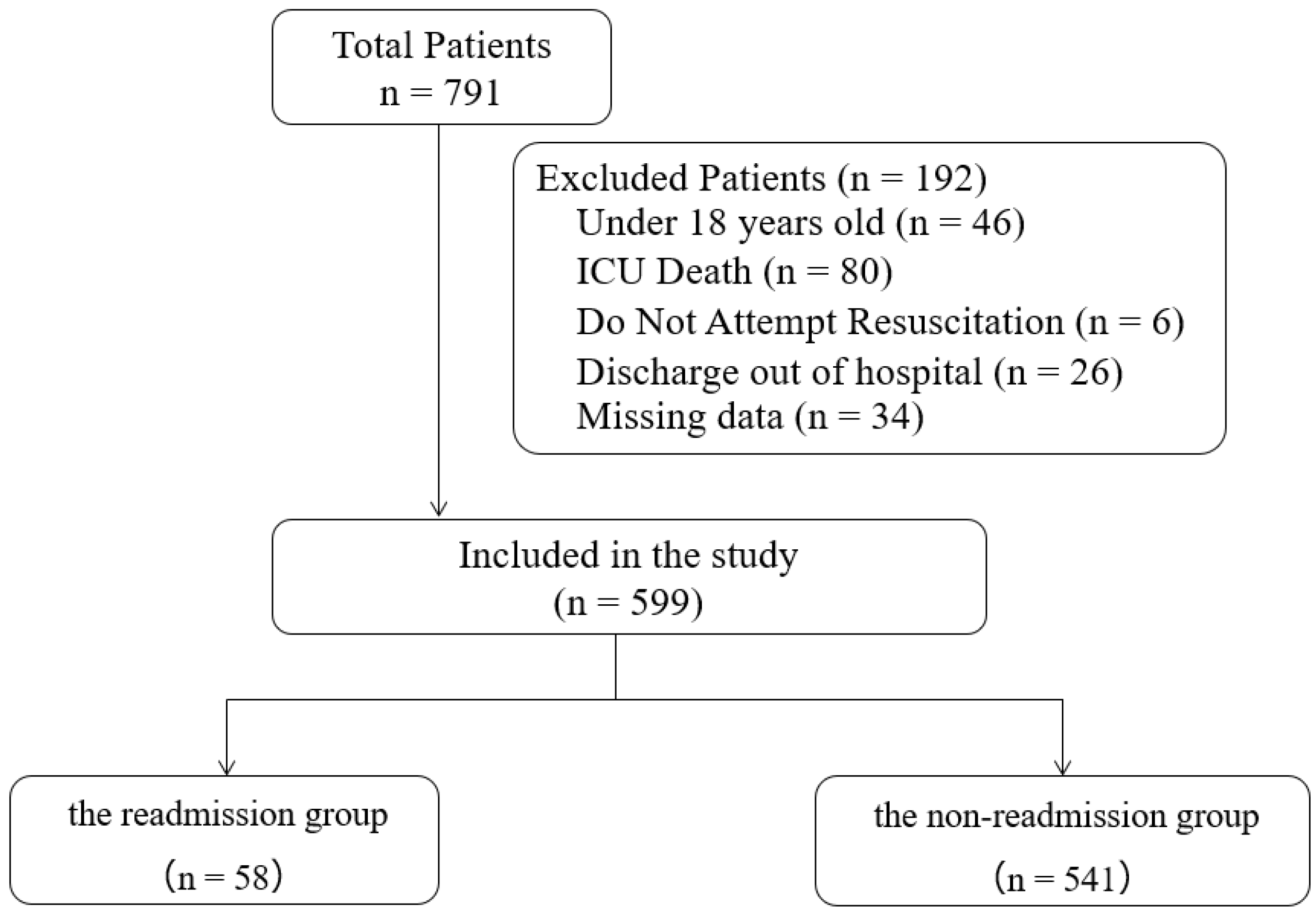
2.1. Design, Setting, and Inclusion Criteria
2.2. Exclusion Criteria
2.3. Population
2.4. Data Collection
2.5. Criteria for ICU Discharge
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
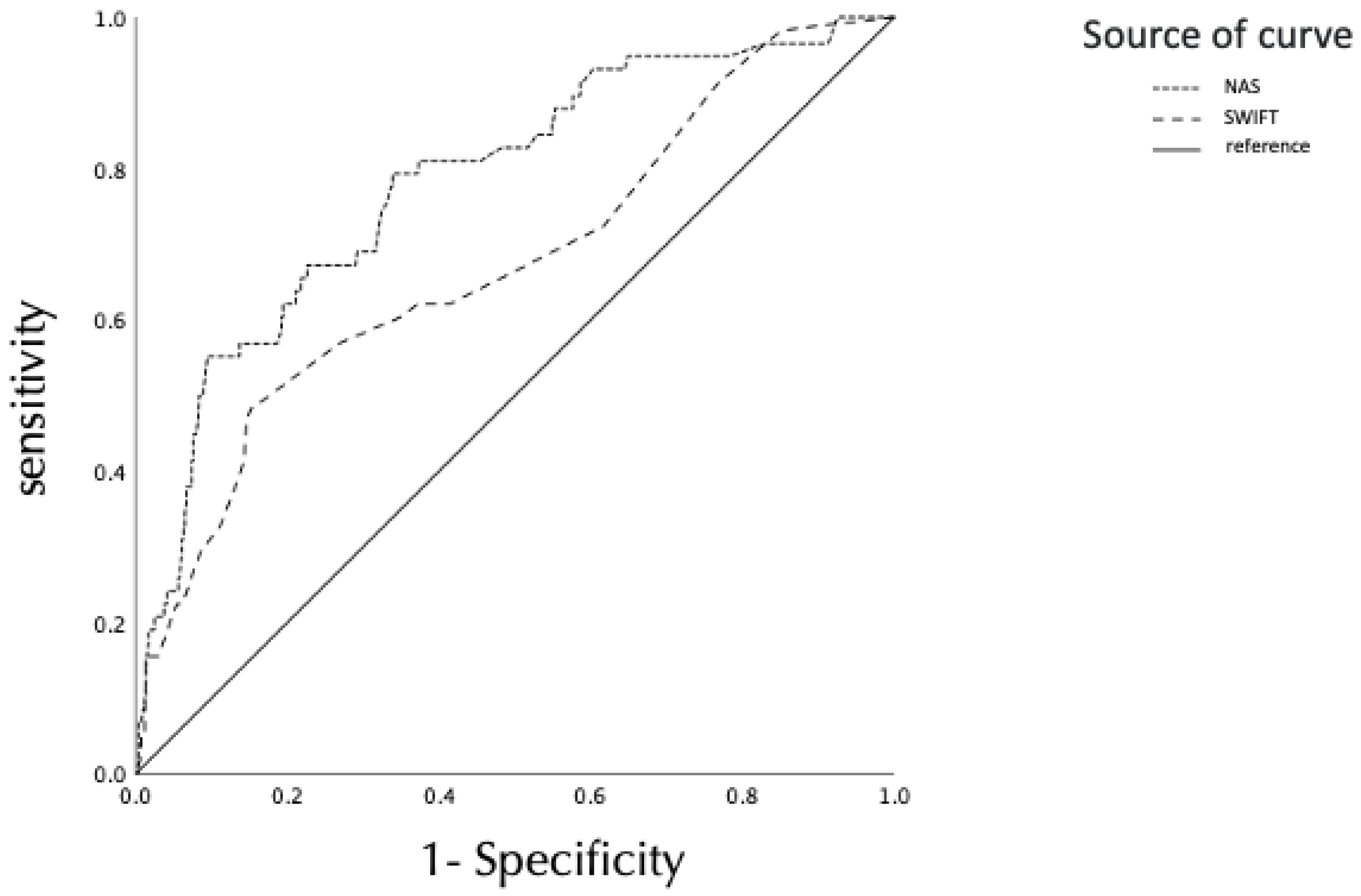
3.2. Comparison of ROC Curves for Unplanned ICU Readmission between the SWIFT Score and NAS
3.3. Odds Ratio of the SWIFT Score and the NAS to Predict ICU Readmission
3.4. Comparison of Each Item in the Nursing Activities Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | Score |
|---|---|
| Original source of this ICU admission | |
| Emergency department | 0 |
| Transfer from a ward or outside hospital (any type of nursing care unit) | 8 |
| Total ICU length of stay (duration in days) | |
| <2 | 0 |
| 2–10 | 1 |
| >10 | 14 |
| Last measured PaO2/FIO2 ratio (during this ICU admission) | |
| >400 | 0 |
| <400 and >150 | 5 |
| <150 and >100 | 10 |
| <100 | 13 |
| Glasgow Coma Scale score at time of ICU discharge | |
| >14 | 0 |
| 11–14 | 6 |
| 8–10 | 14 |
| <8 | 24 |
| Last arterial blood gas PaCO2 | |
| <45 mm Hg | 0 |
| >45 mm Hg | 5 |
Appendix B
| Basic Activities | Score | |
|---|---|---|
| 1 | Monitoring and titration | |
| 1a | Hourly vital signs, regular registration and calculation of fluid balance | 4.5 |
| 1b | Present at bedside and continuous observation or active for 2 h or more in any shift, for reasons of safety, severity, or therapy such as noninvasive mechanical ventilation, weaning procedures, restlessness, mental disorientation, prone position, donation procedures, preparation and administration of fluids or medication, assisting specific procedures | 12.1 |
| 1c | Present at bedside and active for 4 h or more in any shift for reasons of safety, severity, or therapy such as those | 19.6 |
| examples above (1b) | ||
| 2 | Laboratory, biochemical and microbiological investigations | 4.3 |
| 3 | Medication, vasoactive drugs excluded | 5.6 |
| 4 | Hygiene procedures | |
| 4a | Performing hygiene procedures such as dressing of wounds and intravascular catheters, changing linen, washing | 4.1 |
| patient, incontinence, vomiting, burns, leaking wounds, complex surgical dressing with irrigation, and special procedures (e.g., barrier nursing, cross-infection related, room cleaning following infections, staff hygiene) | ||
| 4b | The performance of hygiene procedures took 2 h in any shift | 16.5 |
| 4c | The performance of hygiene procedures took 4 h in any shift | 20 |
| 5 | Care of drains, all (except gastric tube) | 1.8 |
| 6 | Mobilization and positioning, including procedures such as: turning the patient; mobilization of the patient; moving from bed to chair; team lifting (e.g., immobile patient, traction, prone position) | |
| 6a | Performing procedure(s) up to three times per 24 h | 5.5 |
| 6b | Performing procedure(s) more frequently than 3 times per 24 h, or with two nurses, any frequency | 12.4 |
| 6c | Performing procedure with three or more nurses, any frequency | 17 |
| 7 | Support and care of relatives and patient, including procedures such as telephone calls, interviews, counseling; often, the support and care of either relatives or the patient allow staff to continue with other nursing activities (e.g., communication with patients during hygiene procedures, communication with relatives while present at bedside, and observing the patient) | |
| 7a | Support and care of either relatives or the patient requiring full dedication for about 1 h in any shift such as to explain the clinical condition, dealing with pain and distress, difficult family circumstances | 4 |
| 7b | Support and care of either relatives or the patient requiring full dedication for 3 h or more in any shift such as death, demanding circumstances (e.g., large number of relatives, language problems, hostile relatives) | 32 |
| 8 | Administrative and managerial tasks | |
| 8a | Performing routine tasks such as processing of clinical data, ordering examinations, professional exchange of information (e.g., ward rounds) | 4.2 |
| 8b | Performing administrative and managerial tasks requiring full dedication for about 2 h in any shift such as research activities, protocols in use, admission and discharge procedures | 23.2 |
| 8c | Performing administrative and managerial tasks requiring full dedication for about 4 h or more of the time in any shift such as death and organ donation procedures, coordination with other disciplines | 30 |
| Ventilatory support | ||
| 9 | Respiratory support: any form of mechanical ventilation/assisted ventilation with or without positive end-expiratory pressure, with or without muscle relaxants, spontaneous breathing with or without positive end-expiratory pressure with or without endotracheal tube supplementary oxygen by any method | 1.4 |
| 10 | Care of artificial airways: endotracheal tube or tracheostomy cannula | 1.8 |
| 11 | Treatment for improving lung function: thorax physiotherapy, incentive spirometry, inhalation therapy, intratracheal suctioning | 4.4 |
| Cardiovascular support | ||
| 12 | Vasoactive medication, disregard type and dose | 1.2 |
| 13 | Intravenous replacement of large fluid losses. Fluid administration 3 L/m2/day, irrespective of type of fluid administered | 2.5 |
| 14 | Left atrium monitoring: pulmonary artery catheter with or without cardiac output measurement | 1.7 |
| 15 | Cardiopulmonary resuscitation after arrest, in the past period of 24 h (single precordial thump not included) | 7.1 |
| Renal support | ||
| 16 | Hemofiltration techniques, dialysis techniques | 7.7 |
| 17 | Quantitative urine output measurement (e.g., by indwelling urinary catheter) | 7 |
| Neurologic support | ||
| 18 | Measurement of intracranial pressure | 1.6 |
| Metabolic support | ||
| 19 | Treatment of complicated metabolic acidosis/alkalosis | 1.3 |
| 20 | Intravenous hyperalimentation | 2.8 |
| 21 | Enteral feeding through gastric tube or other gastrointestinal route (e.g., jejunostomy) | 1.3 |
| Specific interventions | ||
| 22 | Specific intervention(s) in the intensive care unit: endotracheal intubation, insertion of pacemaker, cardioversion, endoscopies, emergency surgery in the previous 24 h, gastric lavage; routine interventions without direct consequences to the clinical condition of the patient, such as: radiographs, echography, electrocardiogram, dressings, or insertion of venous or arterial catheters, are not included | 2.8 |
| 23 | Specific interventions outside the intensive care unit: surgery or diagnostic procedures | 1.9 |
References
- Kramer, A.A.; Higgins, T.L.; Zimmerman, J.E. The association between ICU readmission rate and patient outcomes. Crit. Care Med. 2013, 41, 24–33. [Google Scholar] [CrossRef]
- Chan, K.S.; Tan, C.K.; Fang, C.S.; Tsai, C.L.; Hou, C.C.; Cheng, K.C.; Lee, M.C. Readmission to the intensive care unit: An indicator that reflects the potential risks of morbidity and mortality of surgical patients in the intensive care unit. Surg. Today 2009, 39, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, S.M.; Leon, S.; Derderian, C.; Al-Harakeh, H.; Ferguson, P.L. Intensive care unit bounce back in trauma patients: An analysis of unplanned returns to the intensive care unit. J. Trauma Acute Care Surg. 2013, 74, 1528–1533. [Google Scholar] [CrossRef] [PubMed]
- Christmas, A.B.; Freeman, E.; Chisolm, A.; Fischer, P.E.; Sachdev, G.; Jacobs, D.G.; Sing, R.F. Trauma intensive care unit “bouncebacks”: Identifying risk factors for unexpected return admission to the intensive care unit. Am. Surg. 2014, 80, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.E.S.; Ratcliffe, S.J.; Halpern, S.D. An empirical comparison of key statistical attributes among potential ICU quality indicators. Crit. Care Med. 2014, 42, 1821–1831. [Google Scholar] [CrossRef] [PubMed]
- Bice, T. ICU readmissions: Good for reflection on performance but not a reflection of quality. Crit. Care Med. 2016, 44, 1790–1791. [Google Scholar] [CrossRef]
- Wong, E.G.; Parker, A.M.; Leung, D.G.; Brigham, E.P.; Arbaje, A.I. Association of severity of illness and intensive care unit readmission: A systematic review. Heart Lung 2016, 45, 3–9.e2. [Google Scholar] [CrossRef]
- Rosenberg, A.L.; Hofer, T.P.; Hayward, R.A.; Strachan, C.; Watts, C.M. Who bounces back? Physiologic and other predictors of intensive care unit readmission. Crit. Care Med. 2001, 29, 511–518. [Google Scholar] [CrossRef]
- Jeong, B.H.; Na, S.J.; Lee, D.S.; Chung, C.R.; Suh, G.Y.; Jeon, K. Readmission and hospital mortality after ICU discharge of critically ill cancer patients. PLoS ONE 2019, 14, e0211240. [Google Scholar] [CrossRef]
- Mcneill, H.; Khairat, S. Impact of Intensive Care Unit readmissions on patient outcomes and the evaluation of the national early warning score to prevent readmissions: Literature review. JMIR Perioper. Med. 2020, 3, e13782. [Google Scholar] [CrossRef]
- Gajic, O.; Malinchoc, M.; Comfere, T.B.; Harris, M.R.; Achouiti, A.; Yilmaz, M.; Schultz, M.J.; Hubmayr, R.D.; Afessa, B.; Farmer, J.C. The Stability and Workload Index for Transfer score predicts unplanned intensive care unit patient readmission: Initial development and validation. Crit. Care Med. 2008, 36, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.C.; Sousa, R.M.; Padilha, K.G. Factors associated with death and readmission into the Intensive Care Unit. Rev. Lat. Am. Enfermagem. 2011, 19, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Miranda, D.R.; de Rijk, A.; Schaufeli, W. Simplified Therapeutic Intervention Scoring System: The TISS-28 items-results from a multicenter study. Crit. Care Med. 1996, 24, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Reis Miranda, D.; Moreno, R.; Iapichino, G. Nine equivalents of nursing manpower use score (NEMS). Intensive Care Med. 1997, 23, 760–765. [Google Scholar] [CrossRef]
- Miranda, D.R.; Nap, R.; de Rijk, A.; Schaufeli, W.; Iapichino, G.; TISS Working Group. Therapeutic Intervention Scoring System. Nursing activities score. Crit. Care Med. 2003, 31, 374–382. [Google Scholar] [CrossRef]
- Racy, S.; Davidson, P.M.; Peeler, A.; Hager, D.N.; Street, L.; Koirala, B. A review of inpatient nursing workload measures. J. Clin. Nurs. 2021, 30, 1799–1809. [Google Scholar] [CrossRef]
- Azevedo, A.V.; Tonietto, T.A.; Boniatti, M.M. Nursing workload on the day of discharge from the intensive care unit is associated with readmission. Intensive Crit. Care Nurs. 2022, 69, 103162. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Saha, R.; Wilson, J.; Prescott, H.C.; Harrison, D.; Rowan, K.; Rubenfeld, G.D.; Adhikari, N.K.J. Rate and risk factors for rehospitalisation in sepsis survivors: Systematic review and meta-analysis. Intensive Care Med. 2020, 46, 619–636. [Google Scholar] [CrossRef]
- Brown, S.E.S.; Ratcliffe, S.J.; Halpern, S.D. An empirical derivation of the optimal time interval for defining ICU readmissions. Med. Care 2013, 51, 706–714. [Google Scholar] [CrossRef]
- Kastrup, M.; Powollik, R.; Balzer, F.; Röber, S.; Ahlborn, R.; von Dossow-Hanfstingl, V.; Wernecke, K.D.; Spies, C.D. Predictive ability of the stability and workload index for transfer score to predict unplanned readmissions after ICU discharge. Crit. Care Med. 2013, 41, 1608–1615. [Google Scholar] [CrossRef] [Green Version]
- Nates, J.L.; Nunnally, M.; Kleinpell, R.; Blosser, S.; Goldner, J.; Birriel, B.; Fowler, C.S.; Byrum, D.; Miles, W.S.; Bailey, H.; et al. ICU admission, discharge, and triage guidelines: A framework to enhance clinical operations, development of institutional policies, and further research. Crit. Care Med. 2016, 44, 1553–1602. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.M.; Dobb, G.J.; Lee, K.Y.; Finn, J.; Knuiman, M.; Webb, S.A.R. The effect of comorbidities on risk of intensive care readmission during the same hospitalization: A linked data cohort study. J. Crit. Care 2009, 24, 101–107. [Google Scholar] [CrossRef]
- Rosa, R.G.; Roehrig, C.; Oliveira, R.P.; Maccari, J.G.; Antônio, A.C.; Castro, S.; Neto, F.L.; Balzano, C.; Teixeira, C. Comparison of unplanned Intensive Care Unit readmission scores: A prospective cohort study. PLoS ONE 2015, 10, e0143127. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lim, C.W.; Hong, H.P.; Ju, J.W.; Jeon, Y.T.; Hwang, J.W.; Park, H.P. Efficacy of the Apache II score at ICU discharge in predicting post-ICU mortality and ICU readmission in critically ill surgical patients. Anaesth. Intensive Care 2015, 43, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Fasoi, G.; Patsiou, E.C.; Stavropoulou, A.; Kaba, E.; Papageorgiou, D.; Toylia, G.; Goula, A.; Kelesi, M. Assessment of nursing workload as a mortality predictor in intensive care units (ICU) using the Nursing Activities Score (NAS) scale. Int. J. Environ. Res. Public Health 2020, 18, 79. [Google Scholar] [CrossRef]
- Rivera, D.I.C.; Torres, C.C.; Romero, L.A.L. Factors associated with nursing workload in three intensive care units. Rev. Esc. Enferm. USP 2021, 55, e20200272. [Google Scholar] [CrossRef] [PubMed]
- Serafim, C.T.R.; Dell’Acqua, M.C.Q.; Castro, M.C.N.E.; Spiri, W.C.; Nunes, H.R.C. Severity and workload related to adverse events in the ICU. Rev. Bras. Enferm. 2017, 70, 942–948. [Google Scholar] [CrossRef]
- Rubano, J.A.; Vosswinkel, J.A.; McCormack, J.E.; Huang, E.C.; Shapiro, M.J.; Jawa, R.S. Unplanned intensive care unit admission following trauma. J. Crit. Care 2016, 33, 174–179. [Google Scholar] [CrossRef]
- Ranney, S.E.; Amato, S.; Callas, P.; Patashnick, L.; Lee, T.H.; An, G.C.; Malhotra, A.K. Delay in ICU transfer is protective against ICU readmission in trauma patients: A naturally controlled experiment. Trauma Surg. Acute Care Open 2021, 6, e000695. [Google Scholar] [CrossRef]
- Lin, W.T.; Chen, W.L.; Chao, C.M.; Lai, C.C. The outcomes and prognostic factors of the patients with unplanned intensive care unit readmissions. Medicine 2018, 97, e11124. [Google Scholar] [CrossRef]
- Lee, J.Y.; Park, S.K.; Kim, H.J.; Hong, S.B.; Lim, C.M.; Koh, Y. Outcome of early intensive care unit patients readmitted in the same hospitalization. J. Crit. Care 2009, 24, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Ashton, C.M.; Del Junco, D.J.; Souchek, J.; Wray, N.P.; Mansyur, C.L. The association between the quality of inpatient care and early readmission: A meta-analysis of the evidence. Med. Care 1997, 35, 1044–1059. [Google Scholar] [CrossRef] [PubMed]
- Needleman, J.; Buerhaus, P.; Mattke, S.; Stewart, M.; Zelevinsky, K. Nurse-staffing levels and the quality of care in hospitals. N. Engl. J. Med. 2002, 346, 1715–1722. [Google Scholar] [CrossRef]
- Archibald, L.K.; Manning, M.L.; Bell, L.M.; Banerjee, S.; Jarvis, W.R. Patient density, nurse-to-patient ratio and nosocomial infection risk in a pediatric cardiac intensive care unit. Pediatr. Infect. Dis. J. 1997, 16, 1045–1048. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Clarke, S.P.; Sloane, D.M.; Sochalski, J.; Silber, J.H. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA 2002, 288, 1987–1993. [Google Scholar] [CrossRef]
- Hervé, M.E.W.; Zucatti, P.B.; Lima, M.A.D.D.S. Transition of care at discharge from the Intensive Care Unit: A scoping review. Rev. Lat. Am. Enfermagem. 2020, 28, e3325. [Google Scholar] [CrossRef]
- Oakes, D.F.; Borges, I.N.K.; Forgiarini Junior, L.A.; Rieder, M. Assessment of ICU readmission risk with the Stability and Workload Index for Transfer score. J. Bras. Pneumol. 2014, 40, 73–76. [Google Scholar] [CrossRef]
- Kareliusson, F.; De Geer, L.; Tibblin, A.O. Risk prediction of ICU readmission in a mixed surgical and medical population. J. Intensive Care 2015, 3, 30. [Google Scholar] [CrossRef] [Green Version]


| - | Readmission Group (n = 58) | Non-Readmission Group (n = 541) | p-Value |
|---|---|---|---|
| Age (years), Mean ± SD | 64.3 ± 15.4 | 63.6 ± 16.1 | 0.74 |
| Male, n (%) | 43 (52.7) | 313 (57.9) | 0.02 |
| Charlson Comorbidity Index, Mean ± SD | 2.1 ± 1.9 | 1.6 ± 1.6 | 0.09 |
| APACHE II, Mean ± SD | 19.7 ± 7.2 | 18.7 ± 5.8 | 0.15 |
| SOFA at ICU admission, Mean ± SD | 6.1 ± 3.5 | 5.4 ± 3.2 | 0.10 |
| ICU admission source | |||
| Medical | 46 (79.3) | 324 (59.9) | 0.004 |
| Surgical | 12 (20.7) | 217 (40.1) | 0.004 |
| ICU discharge after hour | 5 (8.6) | 30 (5.5) | 0.37 |
| Reasons for ICU admission | |||
| Sepsis, n (%) | 15 (25.9) | 99 (18.3) | 0.16 |
| Cardiovascular surgery, n (%) | 5 (8.6) | 85 (15.7) | 0.18 |
| Other surgery | 5 (8.6) | 88 (16.3) | 0.18 |
| Respiratory failure, n (%) | 12 (20.7) | 85 (15.7) | 0.35 |
| Circulatory failure, n (%) | 2 (3.4) | 73 (13.5) | 0.02 |
| Cerebrovascular disease, n (%) | 7 (12.0) | 63 (11.6) | 0.83 |
| Acute kidney injury, n (%) | 3 (5.1) | 17 (3.1) | 0.43 |
| Acute pancreatitis, n (%) | 4 (6.9) | 12 (2.2) | 0.06 |
| Endocrine disease, n (%) | 1 (1.7) | 10 (1.8) | 1.00 |
| Liver failure, n (%) | 3 (5.2) | 6 (1.1) | 0.04 |
| Metabolic disorder, n (%) | 1 (1.7) | 4 (0.7) | 0.40 |
| ICU length of stay (days), Mean ± SD | 6.7 ± 7.4 | 4.5 ± 4.4 | 0.02 |
| Mechanical ventilation, n (%) | 35 (60.3) | 303 (54.5) | 0.05 |
| Ventilator days, Mean ± SD | 3.4 ± 4.2 | 2.1 ± 2.9 | 0.58 |
| CRRT, n (%) | 19 (32.8) | 83 (15.3) | 0.003 |
| Mortality for 28 days | 2 (3.4) | 10 (1.8) | 0.33 |
| Reason for ICU readmission | |||
| Respiratory failure | 26 (44.8) | - | - |
| Circulatory failure | 20 (34.5) | - | - |
| Renal failure | 5 (8.6) | - | - |
| Electrolyte disturbances | 5 (8.6) | - | - |
| Neurological failure | 2 (3.4) | - | - |
| NAS and SWIFT score at ICU discharge | |||
| NAS | 22.9 ± 11.1 | 16.3 ± 7.6 | <0.001 |
| SWIFT | 65.2 ± 15.7 | 49.2 ± 13.0 | <0.001 |
| - | AUROC (95% CI) | p-Value | Cutoff | Sensitivity | Specificity |
|---|---|---|---|---|---|
| SWIFT | 0.68 (0.60–0.75) | <0.001 | 21 | 0.48 | 0.85 |
| NAS | 0.78 (0.72–0.85) | <0.001 | 53 | 0.79 | 0.66 |
| - | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| SOFA at ICU admission | 0.82 (0.92–1.11) | 0.824 |
| Age | 1.00 (0.97–1.02) | 0.61 |
| Men | 1.81 (0.94–3.49) | 0.08 |
| CCI | 1.26 (1.05–1.51) | 0.013 |
| SWIFT > 21 | 3.61 (1.94–6.69) | <0.001 |
| NAS > 53 | 6.07 (3.04–12.1) | <0.001 |
| Readmission Group (n = 58) | Non-Readmission Group (n = 541) | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Characteristic | N | % | N | % | |||
| 1 | Monitoring and titration | ||||||
| 1a Normal | 20 | 34.5 | 392 | 72.5 | <0.001 | ||
| 1b More than normal | 35 | 60.3 | 146 | 27.0 | <0.001 | ||
| 1c Much more than normal | 3 | 5.2 | 3 | 0.6 | 0.014 | ||
| 2 | Laboratory, biochemical and microbiological investigations | 58 | 100.0 | 539 | 99.6 | 1 | |
| 3 | Medication, vasoactive drugs excluded | 58 | 100.0 | 540 | 99.8 | 1 | |
| 4 | Hygiene procedures | ||||||
| 4a Normal | 16 | 27.6 | 413 | 76.3 | <0.001 | ||
| 4b More than normal | 35 | 60.3 | 88 | 16.3 | <0.001 | ||
| 4c Much more than normal | 0 | 0.0 | 2 | 0.4 | 1 | ||
| 5 | Care of drains, all (except gastric tube) | 33 | 56.9 | 290 | 53.6 | 0.679 | |
| 6 | Mobilization and positioning | ||||||
| 6a Normal | 14 | 24.1 | 246 | 45.5 | 0.002 | ||
| 6b More than normal | 36 | 62.1 | 221 | 40.9 | 0.003 | ||
| 6c Much more than normal | 6 | 10.3 | 8 | 1.5 | 0.001 | ||
| 7 | Support and care of relatives and patient | 0.0 | 0.0 | ||||
| 7a About 1 h | 11 | 19.0 | 26 | 4.8 | <0.001 | ||
| 7b About 3 h | 1 | 1.7 | 0 | 0.0 | 0.097 | ||
| 8 | Administrative and managerial tasks | 0.0 | 0.0 | ||||
| 8a Normal | 57 | 98.3 | 536 | 99.1 | 0.459 | ||
| 8b More than normal | 1 | 1.7 | 10 | 1.8 | 1 | ||
| 8c Much more than normal | 0 | 0.0 | 0 | 0.0 | 1.000 | ||
| Ventilatory support | |||||||
| 9 | Respiratory support | 53 | 91.4 | 398 | 73.6 | 0.002 | |
| 10 | Care of artificial airways | 21 | 36.2 | 134 | 24.8 | 0.081 | |
| 11 | Treatment for improving lung function | 28 | 48.3 | 149 | 27.5 | 0.002 | |
| Cardiovascular support | 0.0 | 0.0 | |||||
| 12 | Vasoactive medication | 8 | 13.8 | 16 | 3.0 | 0.001 | |
| 13 | Intravenous replacement of large fluid losses. | 0 | 0.0 | 0 | 0.0 | 1 | |
| 14 | Left atrium monitoring | 6 | 10.3 | 1 | 0.2 | 0.005 | |
| 15 | Cardiopulmonary resuscitation after arrest, in the past period of 24 h | 0 | 0.0 | 0 | 0.0 | 1 | |
| Renal support | |||||||
| 16 | Hemofiltration techniques, dialysis techniques | 10 | 17.2 | 28 | 5.2 | 0.002 | |
| 17 | Quantitative urine output measurement | 55 | 94.8 | 514 | 95.0 | 1 | |
| Neurologic support | |||||||
| 18 | Measurement of intracranial pressure | 0 | 0.0 | 0 | 0.0 | 1 | |
| Metabolic support | |||||||
| 19 | Treatment of complicated metabolic acidosis/alkalosis | 0 | 0.0 | 0 | 0.0 | 1 | |
| 20 | Intravenous hyperalimentation | 58 | 100.0 | 515 | 95.2 | 0.163 | |
| 21 | Enteral feeding through gastric tube or another gastrointestinal route | 28 | 48.3 | 157 | 29.0 | 0.004 | |
| 22 | Specific intervention(s) in the ICU | 5 | 8.6 | 9 | 1.7 | 0.007 | |
| 23 | Specific interventions outside the ICU | 19 | 32.8 | 93 | 17.2 | 0.007 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haruna, J.; Masuda, Y.; Tatsumi, H.; Sonoda, T. Nursing Activities Score at Discharge from the Intensive Care Unit Is Associated with Unplanned Readmission to the Intensive Care Unit. J. Clin. Med. 2022, 11, 5203. https://doi.org/10.3390/jcm11175203
Haruna J, Masuda Y, Tatsumi H, Sonoda T. Nursing Activities Score at Discharge from the Intensive Care Unit Is Associated with Unplanned Readmission to the Intensive Care Unit. Journal of Clinical Medicine. 2022; 11(17):5203. https://doi.org/10.3390/jcm11175203
Chicago/Turabian StyleHaruna, Junpei, Yoshiki Masuda, Hiroomi Tatsumi, and Tomoko Sonoda. 2022. "Nursing Activities Score at Discharge from the Intensive Care Unit Is Associated with Unplanned Readmission to the Intensive Care Unit" Journal of Clinical Medicine 11, no. 17: 5203. https://doi.org/10.3390/jcm11175203