
Morphometric Assessment for Functional Evaluation of Coronary Stenosis with Optical Coherence Tomography and the Optical Flow Ratio in a Vessel with Single Stenosis
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Coronary Angiography and QCA Analysis
2.3. QFR Analysis
2.4. OCT Analysis
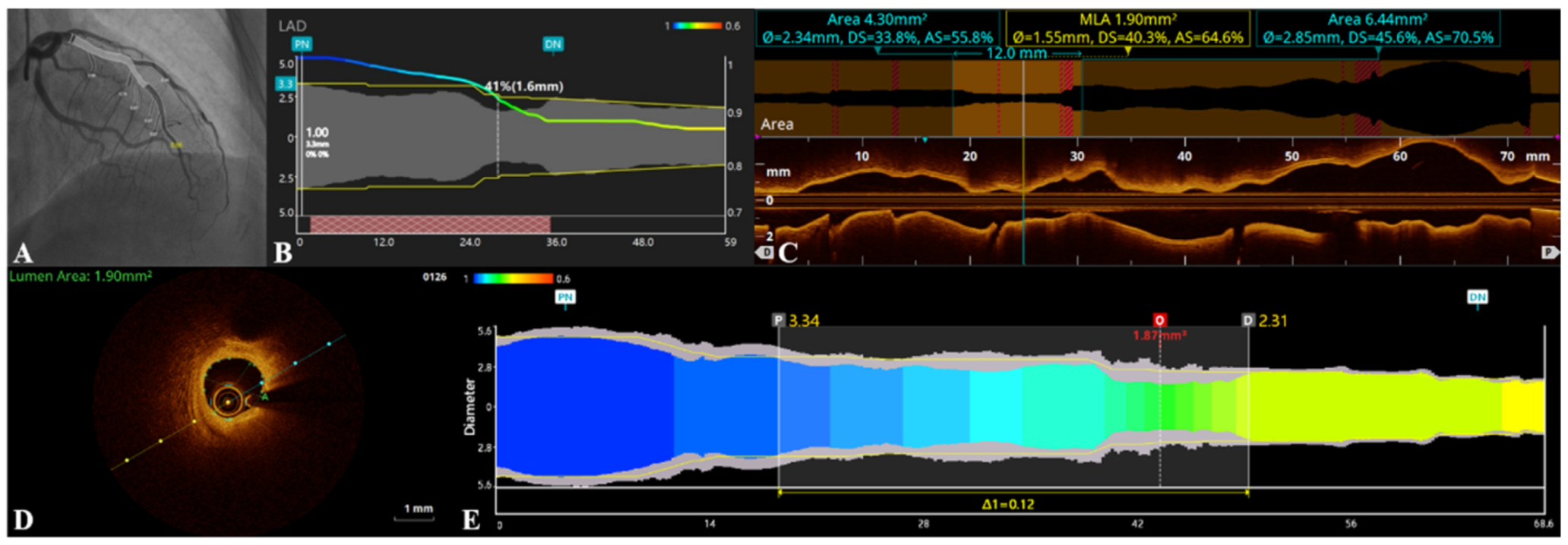
2.5. OFR Measurements
2.6. Statistical Analysis
3. Results
3.1. Baseline Clinical and Lesion Characteristics
3.2. Agreement between QFR and OFR
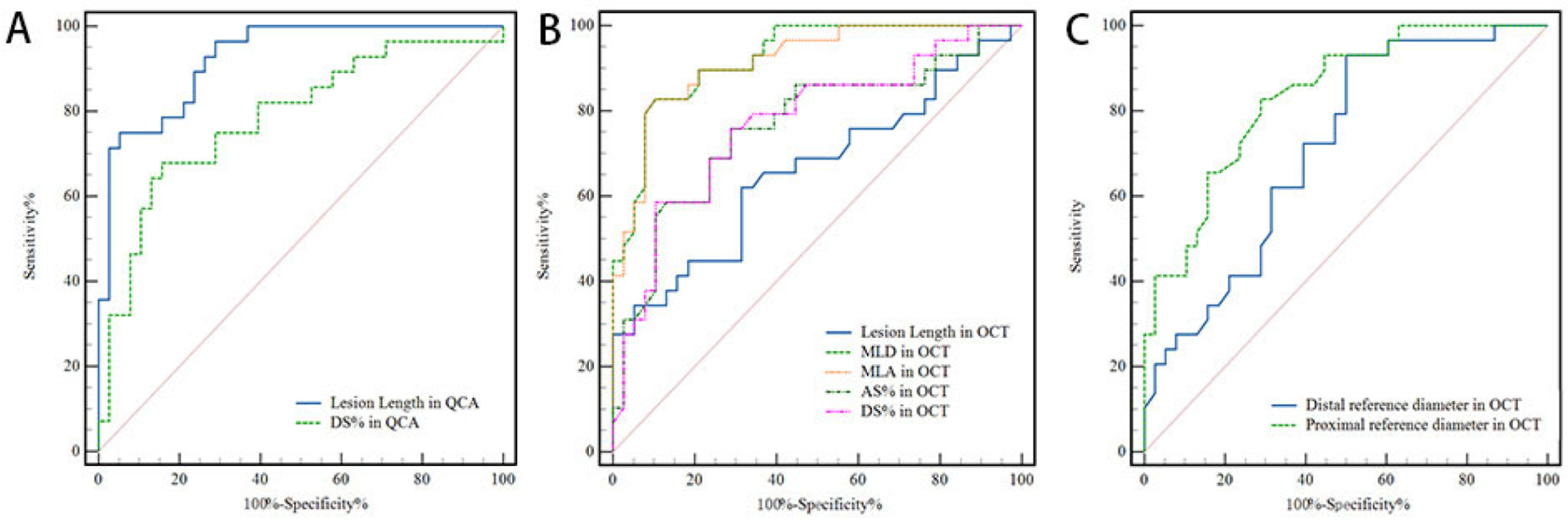
3.3. Diagnostic Performance of OFR
3.4. Hemodynamics Performed by QFR and OFR
3.5. The Correlation between OCT-Derived Intracoronary Stenosis Parameters and Functional Significance of Coronary Stenosis
4. Discussion
4.1. OFR with Coronary Hemodynamic Insufficiency
4.2. Difference between OFR and QFR
4.3. MLA and MLD in OCT with Coronary Hemodynamic Insufficiency
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bech, G.J.; De Bruyne, B.; Pijls, N.H.; de Muinck, E.D.; Hoorntje, J.C.; Escaned, J.; Stella, P.R.; Boersma, E.; Bartunek, J.; Koolen, J.J.; et al. Fractional flow reserve to determine the appropriateness of angioplasty in moderate coronary stenosis: A randomized trial. Circulation 2001, 103, 2928–2934. [Google Scholar] [CrossRef] [PubMed]
- Tonino, P.A.; De Bruyne, B.; Pijls, N.H.; Siebert, U.; Ikeno, F.; van’t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef] [PubMed]
- De Bruyne, B.; Pijls, N.H.; Kalesan, B.; Barbato, E.; Tonino, P.A.; Piroth, Z.; Jagic, N.; Mobius-Winkler, S.; Rioufol, G.; Witt, N.; et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N. Engl. J. Med. 2012, 367, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Lee, J.M.; Nam, C.-W.; Shin, E.-S.; Doh, J.-H.; Dai, N.; Ng, M.K.; Yong, A.; Tresukosol, D.; Mullasari, A.S.; et al. Consensus document for invasive coronary physiologic assessment in Asia-Pacific countries. Cardiol. J. 2019, 26, 215–225. [Google Scholar] [CrossRef]
- Tu, S.; Westra, J.; Yang, J.; von Birgelen, C.; Ferrara, A.; Pellicano, M.; Nef, H.; Tebaldi, M.; Murasato, Y.; Lansky, A.; et al. Diagnostic Accuracy of Fast Computational Approaches to Derive Fractional Flow Reserve From Diagnostic Coronary Angiography: The International Multicenter FAVOR Pilot Study. JACC Cardiovasc Interv. 2016, 9, 2024–2035. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Tu, S.; Qiao, S.; Qu, X.; Chen, Y.; Yang, J.; Guo, L.; Sun, Z.; Li, Z.; Tian, F.; et al. Diagnostic Accuracy of Angiography-Based Quantitative Flow Ratio Measurements for Online Assessment of Coronary Stenosis. J. Am. Coll. Cardiol. 2017, 70, 3077–3087. [Google Scholar] [CrossRef]
- Huang, J.; Emori, H.; Ding, D.; Kubo, T.; Yu, W.; Huang, P.; Zhang, S.; Gutiérrez-Chico, J.L.; Akasaka, T.; Wijns, W.; et al. Diagnostic performance of intracoronary optical coherence tomography-based versus angiography-based fractional flow reserve for the evaluation of coronary lesions. EuroIntervention 2020, 16, 568–576. [Google Scholar] [CrossRef]
- Gonzalo, N.; Escaned, J.; Alfonso, F.; Nolte, C.; Rodriguez, V.; Jimenez-Quevedo, P.; Bañuelos, C.; Fernandez-Ortiz, A.; Garcia, E.; Hernandez-Antolin, R.; et al. Morphometric Assessment of Coronary Stenosis Relevance With Optical Coherence Tomography: A Comparison With Fractional Flow Reserve and Intravascular Ultrasound. J. Am. Coll. Cardiol. 2012, 59, 1080–1089. [Google Scholar] [CrossRef]
- Ali, Z.A.; Maehara, A.; Généreux, P.; Shlofmitz, R.A.; Fabbiocchi, F.; Nazif, T.M.; Guagliumi, G.; Meraj, P.M.; Alfonso, F.; Samady, H.; et al. Optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation (ILUMIEN III: OPTIMIZE PCI): A randomised controlled trial. Lancet 2016, 388, 2618–2628. [Google Scholar] [CrossRef]
- Johnson, T.W.; Räber, L.; Di Mario, C.; Bourantas, C.; Jia, H.; Mattesini, A.; Gonzalo, N.; de la Torre Hernandez, J.M.; Prati, F.; Koskinas, K.; et al. Clinical use of intracoronary imaging. Part 2: Acute coronary syndromes, ambiguous coronary angiography findings, and guiding interventional decision-making: An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur. Heart J. 2019, 40, 2566–2584. [Google Scholar] [CrossRef]
- Waksman, R.; Legutko, J.; Singh, J.; Orlando, Q.; Marso, S.; Schloss, T.; Tugaoen, J.; DeVries, J.; Palmer, N.; Haude, M.; et al. FIRST: Fractional Flow Reserve and Intravascular Ultrasound Relationship Study. J. Am. Coll. Cardiol. 2013, 61, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Zafar, H.; Ullah, I.; Dinneen, K.; Matiullah, S.; Hanley, A.; Leahy, M.J.; Sharif, F. Evaluation of hemodynamically severe coronary stenosis as determined by fractional flow reserve with frequency domain optical coherence tomography measured anatomical parameters. J. Cardiol. 2014, 64, 19–24. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, F.; Barbero, U.; Cerrato, E.; Lipinski, M.J.; Omedè, P.; Montefusco, A.; Taha, S.; Naganuma, T.; Reith, S.; Voros, S.; et al. Accuracy of intravascular ultrasound and optical coherence tomography in identifying functionally significant coronary stenosis according to vessel diameter: A meta-analysis of 2,581 patients and 2,807 lesions. Am. Heart J. 2015, 169, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Milzi, A.; Dettori, R.; Burgmaier, K.; Marx, N.; Reith, S.; Burgmaier, M. Quantitative Flow Ratio Is Related to Intraluminal Coronary Stenosis Parameters as Assessed with Optical Coherence Tomography. J. Clin. Med. 2021, 10, 1856. [Google Scholar] [CrossRef]
- Xaplanteris, P.; Fournier, S.; Pijls, N.H.; Fearon, W.F.; Barbato, E.; Tonino, P.A.; Engstrøm, T.; Kääb, S.; Dambrink, J.-H.; Rioufol, G.; et al. Five-Year Outcomes with PCI Guided by Fractional Flow Reserve. N. Engl. J. Med. 2018, 379, 250–259. [Google Scholar] [CrossRef]
- van Nunen, L.X.; Zimmermann, F.M.; Tonino, P.A.L.; Barbato, E.; Baumbach, A.; Engstrøm, T.; Klauss, V.; MacCarthy, P.A.; Manoharan, G.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet 2015, 386, 1853–1860. [Google Scholar] [CrossRef]
- Kennedy, M.W.; Fabris, E.; Ijsselmuiden, A.J.; Nef, H.; Reith, S.; Escaned, J.; Alfonso, F.; Van Royen, N.; Wojakowski, W.; Witkowski, A.; et al. Combined optical coherence tomography morphologic and fractional flow reserve hemodynamic assessment of non- culprit lesions to better predict adverse event outcomes in diabetes mellitus patients: COMBINE (OCT-FFR) prospective study. Rationale and design. Cardiovasc. Diabetol. 2016, 15, 144. [Google Scholar] [CrossRef]
- Fabris, E.; Berta, B.; Roleder-Dylewska, T.; Hermanides, R.S.; Ijsselmuiden, A.J.; Kauer, F.; Alfonso, F.; von Birgelen, C.; Escaned, J.; Camaro, C.; et al. Thin-Cap Fibroatheroma Rather Than Any Lipid Plaques Increases the Risk of Cardiovascular Events in Diabetic Patients: Insights From the COMBINE OCT–FFR Trial. Circ. Cardiovasc. Interv. 2022, 15, e011728. [Google Scholar] [CrossRef]
- Bezerra, H.G.; Costa, M.A.; Guagliumi, G.; Rollins, A.M.; Simon, D.I. Intracoronary Optical Coherence Tomography: A Comprehensive Review: Clinical and Research Applications. JACC Cardiovasc. Interv. 2009, 2, 1035–1046. [Google Scholar] [CrossRef]
- Yu, W.; Huang, J.; Jia, D.; Chen, S.-L.; Raffel, O.C.; Ding, D.; Tian, F.; Kan, J.; Zhang, S.; Yan, F.; et al. Diagnostic accuracy of intracoronary optical coherence tomography-derived fractional flow reserve for assessment of coronary stenosis severity. EuroIntervention 2019, 15, 189–197. [Google Scholar] [CrossRef] [Green Version]
- Tu, S.; Ding, D.; Chang, Y.; Li, C.; Wijns, W.; Xu, B. Diagnostic accuracy of quantitative flow ratio for assessment of coronary stenosis significance from a single angiographic view: A novel method based on bifurcation fractal law. Catheter. Cardiovasc. Interv. 2021, 97 (Suppl. 2), 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Imola, F.; Mallus, M.; Ramazzotti, V.; Manzoli, A.; Pappalardo, A.; Di Giorgio, A.; Albertucci, M.; Prati, F. Safety and feasibility of frequency domain optical coherence tomography to guide decision making in percutaneous coronary intervention. EuroIntervention 2010, 6, 575–581. [Google Scholar] [CrossRef]
- Reith, S.; Battermann, S.; Hellmich, M.; Marx, N.; Burgmaier, M. Correlation between optical coherence tomography-derived intraluminal parameters and fractional flow reserve measurements in intermediate grade coronary lesions: A comparison between diabetic and non-diabetic patients. Clin. Res. Cardiol. 2015, 104, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Shiono, Y.; Kitabata, H.; Kubo, T.; Masuno, T.; Ohta, S.; Ozaki, Y.; Sougawa, H.; Orii, M.; Shimamura, K.; Ishibashi, K.; et al. Optical Coherence Tomography-Derived Anatomical Criteria for Functionally Significant Coronary Stenosis Assessed by Fractional Flow Reserve. Circ. J. 2012, 76, 2218–2225. [Google Scholar] [CrossRef] [PubMed]
- Pyxaras, S.A.; Tu, S.; Barbato, E.; Barbati, G.; Di Serafino, L.; De Vroey, F.; Toth, G.; Mangiacapra, F.; Sinagra, G.; De Bruyne, B.; et al. Quantitative angiography and optical coherence tomography for the functional assessment of nonobstructive coronary stenoses: Comparison with fractional flow reserve. Am. Heart J. 2013, 166, 1010–1018.e1. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n = 69 | |
|---|---|
| Age, yrs | 63.14 ± 8.57 |
| Female | 15 (21.74%) |
| Left ventricular ejection fraction, % | 63.43 ± 6.46 |
| Diabetes mellitus | 14 (20.29%) |
| Hyperlipidemia | 3 (4.35%) |
| Current smoker | 18 (26.09%) |
| Hypertension | 23 (33.33%) |
| Family history of coronary artery disease | 2 (2.90%) |
| Previous myocardial infarction | 8 (11.59%) |
| Stable angina pectoris | 59 (85.51%) |
| Unstable angina pectoris | 10 (14.49%) |
| Overall (n = 74) | QFR > 0.80 (n = 43) | QFR ≤ 0.80 (n = 31) | p | |
|---|---|---|---|---|
| LAD | 51 (68.92%) | 25 (58.14%) | 26 (83.87%) | 0.018 |
| LCX | 7 (9.46%) | 5 (11.63%) | 2 (6.45%) | 0.728 |
| RCA | 14 (18.92%) | 11 (25.58%) | 3 (9.68%) | 0.085 |
| Diagonal branch | 2 (2.70%) | 2 (4.65%) | 0 (0.00%) | 0.506 |
| Lesion length in QCA, mm | 14.87 ± 8.71 | 12.23 ± 5.44 | 18.64 ± 10.98 | 0.002 |
| Reference vessel diameter, mm | 3.07 ± 0.56 | 3.16 ± 0.57 | 2.94 ± 0.54 | 0.105 |
| Diameter stenosis in QCA, % | 52.32 ± 11.23 | 47.94 ± 9.97 | 58.58 ± 10.03 | <0.001 |
| QFR (per vessel) | 0.78 ± 0.16 | 0.89 ± 0.05 | 0.63 ± 0.12 | <0.001 |
| Vessels with QFR ≤ 0.80 | 31 | 0 | 31 | |
| OFR (per vessel) | 0.79 ± 0.15 | 0.88 ± 0.08 | 0.66 ± 0.13 | <0.001 |
| Vessels with OFR ≤ 0.80 | 34 | 5 | 29 |
| QFR ≤ 0.80, (95% CI) | No. of Vessels in Group | |
|---|---|---|
| Accuracy, % | 90.54 (80.91–95.79) | 74 |
| Sensitivity, % | 93.55 (77.16–98.87) | 31 |
| Specificity, % | 88.37 (74.12–95.64) | 43 |
| PPV, % | 85.29 (68.17–94.46) | 34 |
| NPV, % | 95.00 (81.79–99.13) | 40 |
| (+) LR | 8.04 (3.51–18.43) | |
| (−) LR | 0.07 (0.01–0.20) |
| No | Vessel | Age | Gender | Lesion Length in QCA (mm) | MLA in OCT (mm2) | MLD in OCT (mm) | DS% in OCT (%) | AS% in OCT (%) | Distal Reference Diameter in OCT (mm) | Proximal Reference Diameter in OCT (mm) | OFR | QFR |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | LAD | 62 | M | 9.91 | 1.60 | 1.42 | 47.8 | 72.8 | 2.46 | 2.98 | 0.80 | 0.82 |
| 2 | RCA | 61 | M | 14.43 | 1.69 | 1.46 | 49.0 | 73.8 | 2.78 | 2.94 | 0.86 | 0.62 |
| 3 | LAD | 58 | M | 16.96 | 1.76 | 1.49 | 50.4 | 75.2 | 2.95 | 3.06 | 0.87 | 0.49 |
| 4 | LAD | 65 | F | 25.82 | 1.63 | 1.42 | 46.2 | 70.7 | 2.42 | 2.86 | 0.80 | 0.82 |
| 5 | LAD | 61 | M | 22.35 | 1.48 | 1.37 | 40.2 | 64.2 | 2.28 | 2.30 | 0.61 | 0.91 |
| 6 | LAD | 57 | M | 20.35 | 1.02 | 1.14 | 44.7 | 70.2 | 1.75 | 2.37 | 0.58 | 0.90 |
| 7 | LAD | 44 | M | 7.81 | 1.11 | 1.19 | 62.6 | 86.1 | 3.18 | 3.19 | 0.80 | 0.81 |
| QFR ≤ 0.80 and OFR ≤ 0.80 (n = 38) | QFR > 0.80 and OFR > 0.80 (n = 29) | p | AUC (95%CI) | Cut off Value | |
|---|---|---|---|---|---|
| QCA-based characteristics | |||||
| Lesion length (mm) | 27.24 ± 8.99 | 12.20 ± 5.24 | <0.001 | 0.93(0.87–0.99) | 19.19 |
| DS (%) | 58.52 ± 10.38 | 47.38 ± 10.19 | <0.001 | 0.78(0.67–0.90) | 57.52 |
| OCT-based characteristics | |||||
| MLA (mm2) | 1.26 ± 0.45 | 2.52 ± 1.04 | <0.001 | 0.92(0.85–0.98) | 1.55 |
| MLD (mm) | 1.25 ± 0.19 | 1.75 ± 0.34 | <0.001 | 0.93(0.86–0.98) | 1.40 |
| DS% (%) | 51.02 ± 9.35 | 42.01 ± 8.91 | <0.001 | 0.77(0.65–0.89) | 51.65 |
| AS% (%) | 75.02 ± 10.18 | 65.63 ± 10.14 | <0.001 | 0.76(0.64–0.88) | 70.45 |
| Distal reference diameter (mm) | 2.40 ± 0.37 | 2.95 ± 0.45 | <0.001 | 0.83(0.74–0.93) | 2.70 |
| Proximal reference diameter (mm) | 2.77 ± 0.37 | 3.13 ± 0.50 | 0.002 | 0.71(0.59–0.83) | 3.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.; Lin, Z.; Wu, Q.; Chen, L.; Yang, J.; Deng, H.; Liu, Y.; Xie, N. Morphometric Assessment for Functional Evaluation of Coronary Stenosis with Optical Coherence Tomography and the Optical Flow Ratio in a Vessel with Single Stenosis. J. Clin. Med. 2022, 11, 5198. https://doi.org/10.3390/jcm11175198
Huang Y, Lin Z, Wu Q, Chen L, Yang J, Deng H, Liu Y, Xie N. Morphometric Assessment for Functional Evaluation of Coronary Stenosis with Optical Coherence Tomography and the Optical Flow Ratio in a Vessel with Single Stenosis. Journal of Clinical Medicine. 2022; 11(17):5198. https://doi.org/10.3390/jcm11175198
Chicago/Turabian StyleHuang, Yuming, Zehuo Lin, Quanmin Wu, Liansheng Chen, Junqing Yang, Huiliang Deng, Yuanhui Liu, and Nianjin Xie. 2022. "Morphometric Assessment for Functional Evaluation of Coronary Stenosis with Optical Coherence Tomography and the Optical Flow Ratio in a Vessel with Single Stenosis" Journal of Clinical Medicine 11, no. 17: 5198. https://doi.org/10.3390/jcm11175198