
Sports Obstetrics: Implications of Pregnancy in Elite Sportswomen, a Narrative Review

 ,
,
Abstract
:1. Introduction
2. First Trimester
Miscarriage
3. Second and Third Trimesters
3.1. Fetal Growth and Birth Weight
3.2. Fetal Heart Rate, Umbilical and Uterine Blood Flood
3.3. Pre-Eclampsia and Gestational Hypertension
3.4. Placental Abruption
4. Intrapartum Considerations
4.1. Preterm Birth
4.2. Labour and Mode of Delivery
5. Postnatal Implications
5.1. Pelvic Floor Dysfunction and Incontinence
5.2. Breastfeeding
5.3. Injury
5.4. Postnatal Depression
6. Neonatal Outcomes
7. Impact of Pregnancy on Performance
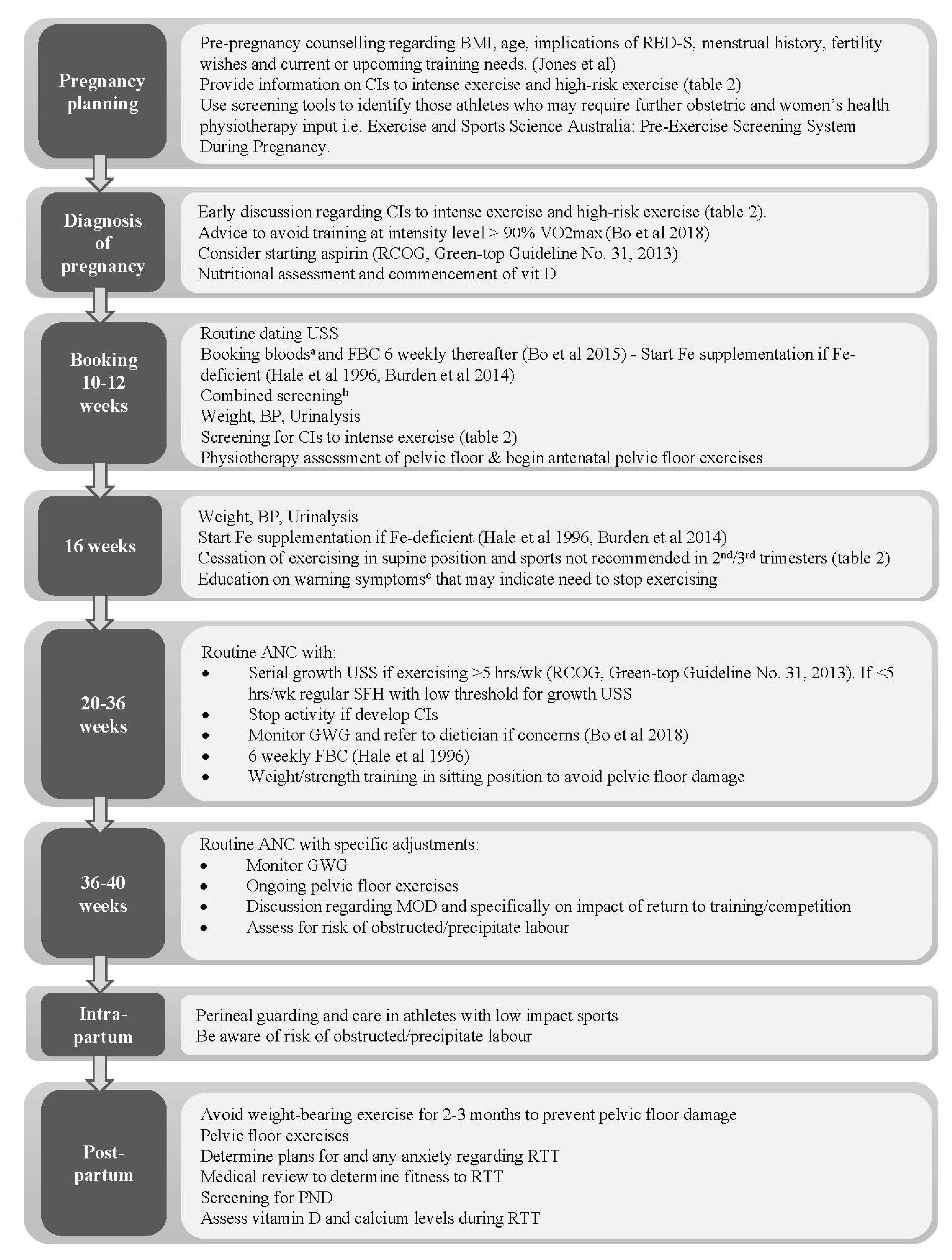
8. Assessment and Management of the Elite Athlete during Pregnancy and Postpartum
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Evenson, K.R.; Barakat, R.; Brown, W.J.; Dargent-Molina, P.; Haruna, M.; Mikkelsen, E.M.; Mottola, M.F.; Owe, K.M.; Rousham, E.K.; Yeo, S. Guidelines for Physical Activity during Pregnancy: Comparisons from Around the World. Am. J. Lifestyle Med. 2014, 8, 102–121. [Google Scholar] [CrossRef]
- Department of Health and Social Care. UK Chief Medical Officers’ Physical Activity Guidelines; Department of Health and Social Care: London, UK, 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832868/uk-chief-medical-officers-physical-activity-guidelines.pdf (accessed on 18 March 2020).
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Erdener, U.; Budgett, R. Exercise and pregnancy: Focus on advice for the competitive and elite athlete. Br. J. Sports Med. 2016, 50, 567. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.J.; Hayman, M.; Haakstad, L.A.H.; Lamerton, T.; Mena, G.P.; Green, A.; Keating, S.E.; Gomes, G.A.O.; Coombes, J.S.; Mielke, G.I. Australian guidelines for physical activity in pregnancy and postpartum. J. Sci. Med. Sport 2022, 25, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Wowdzia, J.B.; McHugh, T.L.; Thornton, J.; Sivak, A.; Mottola, M.F.; Davenport, M.H. Elite Athletes and Pregnancy Outcomes: A Systematic Review and Meta-analysis. Med. Sci. Sports Exerc. 2021, 53, 534–542. [Google Scholar] [CrossRef]
- International Olympic Committee. Women at the Olympic Games. Available online: https://www.olympic.org/women-in-sport/background/statistics (accessed on 2 March 2021).
- Statista.com. Available online: https://www.statista.com/statistics/1090581/olympics-number-athletes-by-gender-since-1896/ (accessed on 11 February 2022).
- Kardel, K.R. Effects of intense training during and after pregnancy in top-level athletes. Scand. J. Med. Sci. Sports 2005, 15, 79–86. [Google Scholar] [CrossRef]
- Hale, R.W.; Milne, L. The elite athlete and exercise in pregnancy. Semin. Perinatol. 1996, 20, 277–284. [Google Scholar] [CrossRef]
- Salvesen, K.Å.; Hem, E.; Sundgot-Borgen, J. Fetal wellbeing may be compromised during strenuous exercise among pregnant elite athletes. Br. J. Sports Med. 2012, 46, 279–283. [Google Scholar] [CrossRef]
- Bø, K.; Artal, R.; Barakat, R.; Brown, W.J.; Davies, G.A.L.; Dooley, M.; Evenson, K.R.; Haakstad, L.A.H.; Kayser, B.; Kinnunen, T.I.; et al. Exercise and pregnancy in recreational and elite athletes: 2016 evidence summary from the IOC expert group meeting, Lausanne. Part 1—Exercise in women planning pregnancy and those who are pregnant. Br. J. Sports Med. 2016, 50, 571–589. [Google Scholar] [CrossRef] [Green Version]
- Kuhrt, K.; Hezelgrave, N.L.; Shennan, A.H. Exercise in pregnancy. Obstet. Gynaecol. 2015, 17, 281–287. [Google Scholar] [CrossRef]
- Bø, K.; Artal, R.; Barakat, R.; Brown, W.; Dooley, M.; Evenson, K.R.; Haakstad, L.A.H.; Larsen, K.; Kayser, B.; Kinnunen, T.I.; et al. Exercise and pregnancy in recreational and elite athletes: 2016 evidence summary from the IOC expert group meeting, Lausanne. Part 2-The effect of exercise on the fetus, labour and birth. Br. J. Sports. Med. 2016, 50, 1297–1305. [Google Scholar] [CrossRef] [PubMed]
- Pivarnik, J.M.; Szymanski, L.M.; Conway, M.R. The Elite Athlete and Strenuous Exercise in Pregnancy. Clin. Obstet. Gynecol. 2016, 59, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Bauer, P.W.; Broman, C.L.; Pivarnik, J.M. Exercise and pregnancy knowledge among healthcare providers. J. Womens Health 2010, 19, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Norton, K.; Norton, L.; Sadgrove, D. Position statement on physical activity and exercise intensity terminology. J. Sci. Med. Sport 2010, 13, 496–502. [Google Scholar] [CrossRef]
- Kimber, M.L.; Meyer, S.; McHugh, T.L.; Thornton, J.; Khurana, R.; Sivak, A.; Davenport, M.H. Health Outcomes after Pregnancy in Elite Athletes: A Systematic Review and Meta-analysis. Med. Sci. Sport. Exerc. 2021, 53, 1739–1747. [Google Scholar] [CrossRef]
- Melzer, K.; Schutz, Y.; Boulvain, M.; Kayser, B. Physical Activity and Pregnancy. Sport Med. 2010, 40, 493–507. [Google Scholar] [CrossRef]
- Soma-Pillay, P.; Nelson-Piercy, C.; Tolppanen, H.; Mebazaa, A. Physiological changes in pregnancy. Cardiovasc. J. Afr. 2016, 27, 89–94. [Google Scholar] [CrossRef]
- Silversides, C.K.; Colam, J.M. Chapter 2, Physiological Changes in Pregnancy. In Heart Disease in Pregnancy, 2nd ed.; Oakley, A., Warnes, C.A., Eds.; Blackwell Publishing: Hoboken, NJ, USA, 2007; pp. 6–17. [Google Scholar]
- Artal, R.; O’Toole, M. Guidelines of the American College of Obstetricians and Gynecologists for exercise during pregnancy and the postpartum period. Br. J. Sports Med. 2003, 37, 6–12. [Google Scholar] [CrossRef]
- Barakat, R.; Ruiz, J.R.; Lucia, A. Exercise during pregnancy and risk of maternal anaemia: A randomised controlled trial. Br. J. Sports Med. 2009, 43, 954–956. [Google Scholar] [CrossRef]
- Chidi-Ogbolu, N.; Baar, K. Effect of Estrogen on Musculoskeletal Performance and Injury Risk. Front. Physiol. 2019, 9, 1834. [Google Scholar] [CrossRef] [PubMed]
- Skow, R.J.; Davenport, M.H.; Mottola, M.F.; Davies, G.A.; Poitras, V.J.; Gray, C.; Garcia, A.J.; Barrowman, N.; Meah, V.L.; Slater, L.G.; et al. Effects of prenatal exercise on fetal heart rate, umbilical and uterine blood flow: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Myer, G.D.; Ford, K.R.; Paterno, M.V.; Nick, T.G.; Hewett, T.E. The effects of generalized joint laxity on risk of anterior cruciate ligament injury in young female athletes. Am. J. Sports Med. 2008, 36, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Milunsky, A.; Ulcickas, M.; Rothman, K.J.; Willett, W.; Jick, S.S.; Jick, H. Maternal heat exposure and neural tube defects. JAMA 1992, 268, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.J. Hyperthermia as a teratogen: A review of experimental studies and their clinical significance. Teratog. Carcinog. Mutagen. 1986, 6, 563–582. [Google Scholar] [CrossRef]
- Moretti, M.E.; Bar-Oz, B.; Fried, S.; Koren, G. Maternal hyperthermia and the risk for neural tube defects in offspring: Systematic review and meta-analysis. Epidemiology 2005, 16, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Yoo, C.; Mottola, M.F.; Poitras, V.J.; Garcia, A.J.; Gray, C.; Barrowman, N.; Davies, G.A.; Kathol, A.; Skow, R.J.; et al. Effects of prenatal exercise on incidence of congenital anomalies and hyperthermia: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 116–123. [Google Scholar] [CrossRef]
- Ravanelli, N.; Casasola, W.; English, T.; Edwards, K.; Jay, O. Heat stress and fetal risk. Environmental limits for exercise and passive heat stress during pregnancy: A systematic review with best evidence synthesis. Br. J. Sports Med. 2019, 53, 799–805. [Google Scholar] [CrossRef]
- Smallcombe, J.W.; Puhenthirar, A.; Casasola, W.; Inoue, D.S.; Chaseling, G.K.; Ravanelli, N.; Edwards, K.M.; Jay, O. Thermoregulation During Pregnancy: A Controlled Trial Investigating the Risk of Maternal Hyperthermia During Exercise in the Heat. Sports Med. 2021, 51, 2655–2664. [Google Scholar] [CrossRef]
- Morris, S.N.; Missmer, S.A.; Cramer, D.W.; Powers, R.D.; McShane, P.M.; Hornstein, M.D. Effects of lifetime exercise on the outcome of in vitro fertilization. Obstet Gynecol. 2006, 108, 938–945. [Google Scholar] [CrossRef] [Green Version]
- Madsen, M.; Jorgensen, T.; Jensen, M.L.; Juhl, M.; Olsen, J.; Andersen, P.K.; Nybo Andersen, A.M. Leisure time physical exercise during pregnancy and the risk of miscarriage: A study within the Danish National Birth Cohort. BJOG 2007, 114, 1419–1426. [Google Scholar] [CrossRef] [PubMed]
- Feodor Nilsson, S.; Andersen, P.K.; Strandberg-Larsen, K.; Nybo Andersen, A.M. Risk factors for miscarriage from a prevention perspective: A nationwide follow-up study. BJOG 2014, 121, 1375–1384. [Google Scholar] [CrossRef] [PubMed]
- Sundgot-Borgen, J.; Sundgot-Borgen, C.; Myklebust, G.; Sølvberg, N.; Torstveit, M.K. Elite athletes get pregnant, have healthy babies and return to sport early postpartum. BMJ Open Sport Exerc. Med. 2019, 5, e000652. [Google Scholar] [CrossRef]
- Davenport, M.H.; Kathol, A.J.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Riske, L.; et al. Prenatal exercise is not associated with fetal mortality: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 108–115. [Google Scholar] [CrossRef]
- Meah, V.L.; Davies, G.A.; Davenport, M.H. Why can’t I exercise during pregnancy? Time to revisit medical ‘absolute’ and ‘relative’ contraindications: Systematic review of evidence of harm and a call to action. Br. J. Sports Med. 2020, 54, 1395–1404. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.S.; McDonald, S.W. Aerobic exercise for women during pregnancy. Cochrane Database Syst. Rev. 2006, CD000180. [Google Scholar] [CrossRef]
- McCowan, L.; Roberts, C.; Dekker, G.; Taylor, R.; Chan, E.; Kenny, L.; Baker, P.; Moss-Morris, R.; Chappell, L.; North, R.A.; et al. Risk factors for small-for-gestational-age infants by customised birthweight centiles: Data from an international prospective cohort study. BJOG 2010, 117, 1599–1607. [Google Scholar] [CrossRef]
- Bø, K.; Backe-Hansen, K.L. Do elite athletes experience low back, pelvic girdle and pelvic floor complaints during and after pregnancy? Scand. J. Med. Sci. Sports 2007, 17, 480–487. [Google Scholar] [CrossRef]
- Beetham, K.S.; Giles, C.; Noetel, M.; Clifton, V.; Jones, J.C.; Naughton, G. The effects of vigorous intensity exercise in the third trimester of pregnancy: A systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019, 19, 281. [Google Scholar] [CrossRef]
- Royal College of Obstetricians and Gynaecologists. Small-for-Gestational-Age Fetus, Investigation and Management (Green-Top Guideline No. 31), 2nd ed.; Royal College of Obstetricians and Gynaecologists: London, UK, 2013; Available online: https://www.rcog.org.uk/globalassets/documents/guidelines/gtg_31.pdf (accessed on 2 March 2021).
- Rafla, N.M.; Cook, J.R. The effect of maternal exercise on fetal heart rate. J. Obstet. Gynaecol. 1999, 19, 381–384. [Google Scholar]
- Rafla, N.M. The effect of maternal exercise on umbilical artery velocimetry waveforms in intrauterine growth retardation. J. Obstet. Gynaecol. 1999, 19, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Magro-malosso, E.R.; Saccone, G.; di Tommaso, M.; Roman, A.; Berghella, V. Exercise during pregnancy and risk of gestational hypertensive disorders: A systematic review and meta-analysis. AOGS 2017, 96, 921–931. [Google Scholar] [CrossRef] [PubMed]
- Østerdal, M.L.; Strøm, M.; Klemmensen, A.K.; Knudsen, V.K.; Juhl, M.; Halldorsson, T.I.; Nybo Andersen, A.M.; Magnus, P.; Olsen, S.F. Does leisure time physical activity in early pregnancy protect against pre-eclampsia? Prospective cohort in Danish women. BJOG 2009, 116, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Wolf, H.T.; Owe, K.M.; Juhl, M.; Hegaard, H.K. Leisure time physical activity and the risk of pre-eclampsia: A systematic review. Matern. Child Health J. 2014, 18, 899–910. [Google Scholar] [CrossRef]
- Aune, D.; Saugstad, O.D.; Henriksen, T.; Tonstad, S. Physical Activity and the Risk of Preeclampsia. Epidemiology 2014, 25, 331–343. [Google Scholar] [CrossRef]
- Rauramo, I.; Forss, M. Effect of exercise on placental blood flow in pregnancies complicated by hypertension, diabetes or intrahepatic cholestasis. Acta Obstet. Gynecol. Scand. 1988, 67, 15–20. [Google Scholar] [CrossRef]
- Rauramo, I. Effect of short-term physical exercise on foetal heart rate and uterine activity in normal and abnormal pregnancies. Ann. Chir. Gynaecol. 1987, 76, 274–279. [Google Scholar]
- Chahal, H.S.; Gelaye, B.; Mostofsky, E.; Sanchez, S.E.; Mittleman, M.A.; Maclure, M.; Pacora, P.; Torres, J.A.; Romero, R.; Ananth, C.V.; et al. Physical exertion immediately prior to placental abruption: A case-crossover study. Am. J. Epidemiol. 2018, 187, 2073–2079. [Google Scholar] [CrossRef]
- Davenport, M.H.; Meah, V.L.; Ruchat, S.M.; Davies, G.A.; Skow, R.J.; Barrowman, N.; Adamo, K.B.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; et al. Impact of prenatal exercise on neonatal and childhood outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1386–1396. [Google Scholar] [CrossRef]
- Di Mascio, D.; Magro-Malosso, E.R.; Saccone, G.; Marhefka, G.D.; Berghella, V. Exercise during pregnancy in normal-weight women and risk of preterm birth: A systematic review and meta-analysis of randomized controlled trials. Am. J. Obstet Gynecol. 2016, 215, 561–571. [Google Scholar] [CrossRef]
- Penttinen, J.; Erkkola, R. Pregnancy in endurance athletes. Scand. J. Med. Sci. Sports. 1997, 7, 226–228. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Fan, L.; Ding, P.; He, Y.-H.; Xie, C.; Niu, Z.; Tian, F.-Y.; Yuan, S.-X.; Jia, D.-Q.; Chen, W.-Q. Maternal Exercise During Pregnancy Reduces the Risk of Preterm Birth Through the Mediating Role of Placenta. J. Matern. Fetal. Neonatal Med. 2019, 32, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Runge, S.B.; Pedersen, J.K.; Svendsen, S.W.; Juhl, M.; Bonde, J.P.; Andersen, A.-M.N. Occupational lifting of heavy loads and preterm birth: A study within the Danish National Birth Cohort. Occup. Environ. Med. 2013, 70, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Vandermeer, B.; Khurana, R.; Nerenberg, K.; Featherstone, R.; Sebastianski, M.; Davenport, M.H. The impact of occupational activities during pregnancy on pregnancy outcomes: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2020, 222, 224–238. [Google Scholar] [CrossRef] [PubMed]
- Poyatos-León, R.; García-Hermoso, A.; Sanabria-Martínez, G.; Álvarez-Bueno, C.; Sánchez-López, M.; Martínez-Vizcaíno, V. Effects of exercise during pregnancy on mode of delivery: A meta-analysis. Acta Obstet. Gynecol. 2015, 94, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Ruchat, S.-M.; Sobierajski, F.; Poitras, V.J.; Gray, C.; Yoo, C.; Skow, R.J.; Garcia, A.J.; Barrowman, N.; Meah, V.L.; et al. Impact of prenatal exercise on maternal harms, labour and delivery outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 99–107. [Google Scholar] [CrossRef]
- Kruger, J.A.; Dietz, H.P.; Murphy, B.A. Pelvic floor function in elite nulliparous athletes. Ultrasound Obstet. Gynecol. 2007, 30, 81–85. [Google Scholar] [CrossRef]
- Sigurdardottir, T.; Steingrimsdottir, T.; Geirsson, R.T.; Halldorsson, T.I.; Aspelund, T.; Bø, K. Do female elite athletes experience more complicated childbirth than non-athletes? A case-control study What are the findings? Br. J. Sport Med. 2019, 53, 354–358. [Google Scholar] [CrossRef]
- Bø, K.; Artal, R.; Barakat, R.; Brown, W.J.; Davies, G.A.L.; Dooley, M.; Evenson, K.R.; Haakstad, L.A.H.; Kayser, B.; Kinnunen, T.I.; et al. Exercise and pregnancy in recreational and elite athletes: 2016/17 evidence summary from the IOC Expert Group Meeting, Lausanne. Part 3-Exercise in the postpartum period. Br. J. Sports Med. 2017, 51, 1516–1525. [Google Scholar] [CrossRef]
- Milsom, I.; Coyne, K.S.; Nicholson, S.; Kvasz, M.; Chen, C.-I.; Wein, A.J. Global Prevalence and Economic Burden of Urgency Urinary Incontinence: A Systematic Review. Eur. Urol. 2014, 65, 79–95. [Google Scholar] [CrossRef]
- Jones, B.P.; L’Heveder, A.; Saso, S.; Yazbek, J.; Smith, J.R.; Dooley, M. Sports gynaecology. Obstet. Gynaecol. 2019, 21, 85–94. [Google Scholar] [CrossRef]
- de Mattos Lourenco, T.R.; Matsuoka, P.K.; Baracat, E.C.; Haddad, J.M. Urinary incontinence in female athletes: A systematic review. Int. Urogynecol. J. 2018, 29, 1757–1763. [Google Scholar] [CrossRef] [PubMed]
- Moore, I.S.; James, M.L.; Brockwell, E.; Perkins, J.; Jones, A.L.; Donnelly, G.M. Multidisciplinary, biopsychosocial factors contributing to return to running and running related stress urinary incontinence in postpartum women. Br. J. Sports Med. 2021, 55, 1286–1292. [Google Scholar] [CrossRef] [PubMed]
- Bo, K. Urinary incontinence, pelvic floor dysfunction, exercise and sport. Sports Med. 2004, 34, 451–464. [Google Scholar]
- Dewey, K.G.; Lovelady, C.A.; Nommsen-Rivers, L.A.; McCrory, M.A.; Lönnerdal, B. A randomized study of the effects of aerobic exercise by lactating women on breast-milk volume and composition. N. Engl. J. Med. 1994, 330, 449–453. [Google Scholar] [CrossRef]
- Lovelady, C.A.; Lonnerdal, B.; Dewey, K.G. Lactation performance of exercising women. Am. J. Clin. Nutr. 1990, 52, 103–109. [Google Scholar] [CrossRef]
- Tenforde, A.S.; Toth, K.E.S.; Langen, E.; Fredericson, M.; Sainani, K.L. Running habits of competitive runners during pregnancy and breastfeeding. Sports Health 2015, 7, 172–176. [Google Scholar] [CrossRef]
- Yeo, U.H.; Choi, C.J.; Choi, W.S.; Kim, K.S. Relationship between breast-feeding and bone mineral density among Korean women in the 2010 Korea National Health and Nutrition Examination Survey. J. Bone Miner. Metab. 2016, 34, 109–117. [Google Scholar] [CrossRef]
- Grizzo, F.M.F.; Alarcão, A.C.J.; Agnolo, C.M.D.; Pedroso, R.B.; Santos, T.S.; Vissoci, J.R.N.; Pinheiro, M.M.; Carvalho, M.D.B.; Pelloso, S.M. How does women’s bone health recover after lactation? A systematic review and meta-analysis. Osteoporos. Int. 2020, 31, 413–427. [Google Scholar] [CrossRef]
- Nose-Ogura, S.; Yoshino, O.; Dohi, M.; Kigawa, M.; Harada, M.; Hiraike, O.; Onda, T.; Osuga, Y.; Fujii, T.; Saito, S. Risk factors of stress fractures due to the female athlete triad: Differences in teens and twenties. Scand. J. Med. Sci. Sports 2019, 29, 1501–1510. [Google Scholar] [CrossRef]
- Solli, G.S.; Sandbakk, Ø. Training Characteristics During Pregnancy and Postpartum in the World’s Most Successful Cross Country Skier. Front. Physiol. 2018, 9, s595. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.; Pollock, N.; Polglass, G.; Clarsen, B. Injury and Illness in Elite Athletics: A Prospective Cohort Study Over Three Seasons. Int. J. Sports Phys. Ther. 2022, 17, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Songoygard, K.M.; Stafne, S.N.; Evensen, K.A.; Salvesen, K.A.; Vik, T.; Morkved, S. Does exercise during pregnancy prevent postnatal depression? A randomized controlled trial. Acta Obs. Gynecol. Scand. 2012, 91, 62–67. [Google Scholar] [CrossRef] [PubMed]
- McCurdy, A.P.; Boulé, N.G.; Sivak, A.; Davenport, M.H. Effects of Exercise on Mild-to-Moderate Depressive Symptoms in the Postpartum Period. Obstet Gynecol. 2017, 129, 1087–1097. [Google Scholar] [CrossRef]
- Poyatos-León, R.; García-Hermoso, A.; Sanabria-Martínez, G.; Álvarez-Bueno, C.; Cavero-Redondo, I.; Martínez-Vizcaíno, V. Effects of exercise-based interventions on postpartum depression: A meta-analysis of randomized controlled trials. Birth 2017, 44, 200–208. [Google Scholar] [CrossRef]
- Pritchett, R.V.; Daley, A.J.; Jolly, K. Does aerobic exercise reduce postpartum depressive symptoms? A systematic review and meta-analysis. Br. J. Gen. Pract. 2017, 67, e684–e691. [Google Scholar] [CrossRef]
- Vargas-Terrones, M.; Barakat, R.; Santacruz, B.; Fernandez-Buhigas, I.; Mottola, M.F. Physical exercise programme during pregnancy decreases perinatal depression risk: A randomised controlled trial. Br. J. Sports Med. 2019, 53, 348–353. [Google Scholar] [CrossRef]
- Bø, K.; Artal, R.; Barakat, R.; Brown, W.J.; Davies, G.A.L.; Dooley, M.; Evenson, K.R.; Haakstad, L.A.H.; Kayser, B.; Kinnunen, T.I.; et al. Exercise and pregnancy in recreational and elite athletes: 2016/2017 evidence summary from the IOC expert group meeting, Lausanne. Part Recommendations for health professionals and active women. Br. J. Sports Med. 2018, 52, 1080–1085. [Google Scholar] [CrossRef]
- Ellingson, M.S.; Petterson, A.; Stafne, S.N.; Morkved, S.; Salvesen, K.A.; Evensen, K.A.I. Neurodevelopmental outcome in 7-year-old children is not affected by exercise during pregnancy: Follow up of a multicentre randomised controlled trial. BJOG 2020, 127, 508–517. [Google Scholar] [CrossRef]
- Lundby, C.; Montero, D.; Joyner, M. Biology of VO2 max: Looking under the physiology lamp. Acta Physilogica 2017, 220, 218–228. [Google Scholar] [CrossRef]
- Poole, D.C.; Wilkerson, D.P.; Jones, A.M. Validity of criteria for establishing maximal O2 uptake during ramp exercise tests. Eur. J. Appl. Physiol. 2008, 102, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.D. VO2max: What do we know, and what do we still need to know? J. Physiol. 2008, 586, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Capeless, J.F.; Clapp, E. The VO2max of recreational athletes before and after pregnancy. Med. Sci. Sports Exerc. 1991, 23, 1128–1133. [Google Scholar]
- Chakaravertty, B.; Parkavi, K.; Coumary, S.A.; Felix, A.J.W. Antepartum cardiorespiratory fitness (CRF) quantification by estimation of maximal oxygen consumption (Vo2 max) in pregnant South Indian women. J. Indian Med. Assoc. 2012, 110, 214–217. [Google Scholar]
- Treuth, M.S.; Butte, N.F.; Puyau, M. Pregnancy-Related Changes in Physical Activity, Fitness, and Strength. Med. Sci. Sports Exerc 2005, 37, 832–837. [Google Scholar] [CrossRef]
- Sim, M.; Garvican-Lewis, L.A.; Cox, G.R.; Govus, A.; McKay, A.K.A.; Stellingwerff, T.; Peeling, P. Iron considerations for the athlete: A narrative review. Eur. J. Appl. Physiol. 2019, 119, 1463–1478. [Google Scholar] [CrossRef]
- Pivarnik, J.M.; Mauer, M.B.; Ayers, N.A.; Kirshon, B.; Dildy, G.A.; Cotton, D.B. Effects of chronic exercise on blood volume expansion and hematologic indices during pregnancy. Obstet Gynecol. 1994, 83, 265–269. [Google Scholar]
- Burden, R.J.; Morton, K.; Richards, T.; Whyte, G.P.; Pedlar, C.R. Is iron treatment beneficial in, iron-deficient but non-anaemic (IDNA) endurance athletes? A systematic review and meta-analysis. Br. J. Sports Med. 2014, 49, 1389–1397. [Google Scholar] [CrossRef]
- Carpenter, M.W.; Sady, S.P.; Sady, M.A.; Haydon, B.; Coustan, D.R.; Thompson, P.D. Effect of maternal weight gain during pregnancy on exercise performance. J. Appl. Physiol. 1990, 68, 1173–1176. [Google Scholar] [CrossRef]
- Larew, K.; Hunter, G.R.; Larson-Meyer, D.E.; Newcomer, B.R.; McCarthy, J.P.; Weinsier, R.L. Muscle metabolic function, exercise performance, and weight gain. Med. Sci. Sports Exerc. 2003, 35, 230–236. [Google Scholar] [CrossRef]


{kind=link}
| Physiological Adaptation | 1st Trimester | 2nd Trimester | 3rd Trimester | Implication for Exercise |
|---|---|---|---|---|
| Cardiovascular | Increase in CO by 20% Marked fall in PVR Increase in blood volume | Maximum CO (40% increase) at 20–28 week Fall in PVR by 25–30 | Minimal fall in CO at term, with SV declining but raised HR persisting PVR increases from 32 weeks Blood volume increases to 50% of pre-pregnancy level by term In supine position, pressure of gravid uterus on IVC reduces venous return to the heart, with reduced SV and C | Compensation for moderate but not strenuous physical activity or endurance sports Misinterpretation of maximum HR Difficulty exercising in supine position Decline in oxygen carrying capacity of blood due to haemodilution. Improved performance postpartum |
| Throughout: Hypervolaemia due to increased E, which activates renin-angiotensin system, as well as involvement of other hormones | ||||
| Respiratory | Reduced inspiratory reserve volume due to increased tidal volume | 20–30% increase in VO2 max at term Diaphragmatic elevation causes decreased functional residual capacity Inspiratory reserve volume increases due to reduced functional residual capacity | Overall positive impact on exercise due to increase in VO2max At later gestation, subjective feeling of hypoxia at rest, which can improve with mild activity | |
| Throughout: Increase in minute ventilation (40–50%) and VO2max. | ||||
| Haematological | Increased plasma volume with steady fall in Hb throughout 2nd trimester | Plasma volume increased by 50% by 34 weeks Haemoconcentration towards ter | Altered perception of exertion | |
| Throughout: Physiological hypercoagulable state | ||||
| Musculoskeletal | Exaggerated lordosis of the lower back, forward flexion of the neck and downward movement of the shoulders Increased mobility and widening of sacroiliac joints and pubic symphysis. Increased joint laxity due to increased oestrogen and relaxin levels Gravid uterus can result in shift in centre of gravity | Discomfort or damage to joints Increased risk of injury or falls, but improved recovery following injury Lumbar lordosis causes change in centre of gravity and pelvis to tilt forwards; can cause injury, particularly in stop-and-go training | ||
| Throughout: Increasing E concentrations potentially improves muscle and tendon strength Change in the micro-architectural pattern of bone in pregnancy but not overall bone mass Pregnancy-associated weight gain increases forces across joints | ||||
| Metabolic/endocrine | Total cortisol levels increase at the end of the 1st trimester Increased insulin secretion and increased insulin sensitivity in early pregnancy | Insulin resistance begins | Cortisol level 3x that of non-pregnant values at end of pregnancy Peak insulin resistance | Increased maternal nutritional requirements beyond the extra 300 kcal daily intake required to maintain the metabolic demands of pregnancy |
| Throughout: 15% increase in metabolic rate State of hypercortisolism Insulin-resistant state to allow glucose availability for fetus. | ||||
| Pre-existing Medical Conditions | Pregnancy-Related Conditions | |
|---|---|---|
| Absolute (conditions posing high risk to fetus) | Haemodynamically significant heart disease (acquired/congenital) Uncontrolled arryhthmia Severe respiratory disease Uncontrolled T1DM Ψ Poorly controlled hypertension Δ Severe anaemia Δ | Placental abruption FGR in current pregnancy Vasa praevia Cervical insufficiency/cerclage Severe pre-eclampsia PTL during current pregnancy Severe anaemia Δ Persistent bleeding in 2nd/3rd trimesters Δ Multiple gestation with risk of PTL Δ Severe anaemia Δ |
| Relative (conditions posing moderate risk to fetus) | Mild respiratory disorders Mild congenital or acquired heart disease Well-controlled T1DM Untreated thyroid disease Symptomatic, severe eating disorder Multiple nutrient deficiencies and/or chronic undernutrition Orthopaedic limitations Δ Poorly controlled seizure disorder | Mild pre-eclampsia Preterm prelabour rupture of membranes * Placenta praevia > 28 weeks’ gestation * Previous fetal growth restriction, miscarriage, PTL or preterm birth Δ |
| No longer considered contraindications according to Meah et al. [39]. | Chronic hypertension Recurrent miscarriage Epilepsy Anaemia Hx of spontaneous PTL Hx of previous FGR | Pregnancy-induced hypertension Short cervix Multiple pregnancy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
L’Heveder, A.; Chan, M.; Mitra, A.; Kasaven, L.; Saso, S.; Prior, T.; Pollock, N.; Dooley, M.; Joash, K.; Jones, B.P. Sports Obstetrics: Implications of Pregnancy in Elite Sportswomen, a Narrative Review. J. Clin. Med. 2022, 11, 4977. https://doi.org/10.3390/jcm11174977
L’Heveder A, Chan M, Mitra A, Kasaven L, Saso S, Prior T, Pollock N, Dooley M, Joash K, Jones BP. Sports Obstetrics: Implications of Pregnancy in Elite Sportswomen, a Narrative Review. Journal of Clinical Medicine. 2022; 11(17):4977. https://doi.org/10.3390/jcm11174977
Chicago/Turabian StyleL’Heveder, Ariadne, Maxine Chan, Anita Mitra, Lorraine Kasaven, Srdjan Saso, Tomas Prior, Noel Pollock, Michael Dooley, Karen Joash, and Benjamin P. Jones. 2022. "Sports Obstetrics: Implications of Pregnancy in Elite Sportswomen, a Narrative Review" Journal of Clinical Medicine 11, no. 17: 4977. https://doi.org/10.3390/jcm11174977