
Corneal Nerve Changes Observed by In Vivo Confocal Microscopy in Patients Receiving Oxaliplatin for Colorectal Cancer: The COCO Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Paice, J.A. Clinical challenges: Chemotherapy-induced peripheral neuropathy. Semin. Oncol. Nurs. 2009, 25, S8–S19. [Google Scholar] [CrossRef] [PubMed]
- Beijers, A.J.; Mols, F.; Tjan-Heijnen, V.C.; Faber, C.G.; van de Poll-Franse, L.V.; Vreugdenhil, G. Peripheral neuropathy in colorectal cancer survivors: The influence of oxaliplatin administration. Results from the population-based PROFILES registry. Acta Oncol. 2015, 54, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Haller, D.G.; Tabernero, J.; Maroun, J.; De Braud, F.; Price, T.; Van Cutsem, E.; Hill, M.; Gilberg, F.; Rittweger, K.; Schmoll, H.-J. Capecitabine plus oxaliplatin compared with fluorouracil and folinic acid as adjuvant therapy for stage III colon cancer. J. Clin. Oncol. 2011, 29, 1465–1471. [Google Scholar] [CrossRef]
- Osti, M.F.; Agolli, L.; Bracci, S.; Masoni, L.; Valeriani, M.; Falco, T.; De Sanctis, V.; Maurizi Enrici, R. Neoadjuvant chemoradiation with concomitant boost radiotherapy associated to capecitabine in rectal cancer patients. Int. J. Colorectal Dis. 2014, 29, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Kyritsis, A.P.; Makatsoris, T.; Kalofonos, H.P. Chemotherapy-induced peripheral neuropathy in adults: A comprehensive update of the literature. Cancer Manag. Res. 2014, 6, 135. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.L.; Craig, J.P.; Patel, D.V.; McGhee, C.N.; Pradhan, M.; Ellyett, K.; Kilfoyle, D.; Braatvedt, G.D. In Vivo Confocal Microscopy of Corneal Nerves: An Ocular Biomarker for Peripheral and Cardiac Autonomic Neuropathy in Type 1 Diabetes Mellitus. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5060–5065. [Google Scholar] [CrossRef]
- Misra, S.L.; Goh, Y.W.; Patel, D.V.; Riley, A.F.; McGhee, C.N. Corneal microstructural changes in nerve fiber, endothelial and epithelial density after cataract surgery in patients with diabetes mellitus. Cornea 2015, 34, 177–181. [Google Scholar] [CrossRef]
- Petropoulos, I.N.; Green, P.; Chan, A.W.; Alam, U.; Fadavi, H.; Marshall, A.; Asghar, O.; Efron, N.; Tavakoli, M.; Malik, R.A. Corneal confocal microscopy detects neuropathy in patients with type 1 diabetes without retinopathy or microalbuminuria. PLoS ONE 2015, 10, e0123517. [Google Scholar] [CrossRef]
- Quattrini, C.; Tavakoli, M.; Jeziorska, M.; Kallinikos, P.; Tesfaye, S.; Finnigan, J.; Marshall, A.; Boulton, A.J.; Efron, N.; Malik, R.A. Surrogate markers of small fiber damage in human diabetic neuropathy. Diabetes 2007, 56, 2148–2154. [Google Scholar] [CrossRef]
- Tavakoli, M.; Petropoulos, I.N.; Malik, R.A. Corneal confocal microscopy to assess diabetic neuropathy: An eye on the foot. J. Diabetes Sci. Technol. 2013, 7, 1179–1189. [Google Scholar] [CrossRef] [PubMed]
- Campagnolo, M.; Lazzarini, D.; Fregona, I.; Cacciavillani, M.; Bergamo, F.; Parrozzani, R.; Midena, E.; Briani, C. Corneal confocal microscopy in patients with oxaliplatin-induced peripheral neuropathy. J. Peripher. Nerv. Syst. 2013, 18, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Ferdousi, M.; Azmi, S.; Petropoulos, I.N.; Fadavi, H.; Ponirakis, G.; Marshall, A.; Tavakoli, M.; Malik, I.; Mansoor, W.; Malik, R.A. Corneal confocal microscopy detects small fibre neuropathy in patients with upper gastrointestinal cancer and nerve regeneration in chemotherapy induced peripheral neuropathy. PLoS ONE 2015, 10, e0139394. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.C.B.; Goldstein, D.; Trinh, T.; Au, K.; Park, S.B.; Krishnan, A.V.; Markoulli, M. A cross-sectional study of ocular surface discomfort and corneal nerve dysfunction after paclitaxel treatment for cancer. Sci. Rep. 2021, 11, 1786. [Google Scholar] [CrossRef]
- Sterenczak, K.A.; Stache, N.; Bohn, S.; Allgeier, S.; Köhler, B.; Bartschat, A.; George, C.; Guthoff, R.F.; Stachs, O.; Stachs, A. Burst of corneal dendritic cells during trastuzumab and paclitaxel treatment. Diagnostics 2021, 11, 838. [Google Scholar] [CrossRef] [PubMed]
- Koschmieder, A.; Stachs, O.; Kragl, B.; Stahnke, T.; Sterenczak, K.A.; Henze, L.; Jünemann, A.G.; Junghanss, C.; Guthoff, R.F.; Murua Escobar, H. Non-invasive detection of corneal sub-basal nerve plexus changes in multiple myeloma patients by confocal laser scanning microscopy. Biosci. Rep. 2020, 40, BSR20193563. [Google Scholar] [CrossRef] [PubMed]
- Mols, F.; Beijers, T.; Lemmens, V.; van den Hurk, C.J.; Vreugdenhil, G.; van de Poll-Franse, L.V. Chemotherapy-induced neuropathy and its association with quality of life among 2-to 11-year colorectal cancer survivors: Results from the population-based PROFILES registry. J. Clin. Oncol. 2013, 31, 2699–2707. [Google Scholar] [CrossRef]
- Chiang, J.C.B.; Goldstein, D.; Trinh, T.; Au, K.; Mizrahi, D.; Muhlmann, M.; Crowe, P.; O’Neill, S.; Edwards, K.; Park, S.B. A cross-sectional study of sub-basal corneal nerve reduction following neurotoxic chemotherapy. Transl. Vis. Sci. Technol. 2021, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; McKeage, M. Neuropathies associated with oxaliplatin therapy. Asia-Pac. J. Clin. Oncol. 2012, 8, 107–110. [Google Scholar] [CrossRef]
- Swanevelder, S.K.; Misra, S.L.; Tyler, E.F.; McGhee, C.N. Precision, agreement and utility of a contemporary non-contact corneal aesthesiometer. Clin. Exp. Optom. 2020, 103, 798–803. [Google Scholar] [CrossRef]
- Patel, D.V.; McGhee, C.N. Mapping of the normal human corneal sub-basal nerve plexus by in vivo laser scanning confocal microscopy. Investig. Ophthalmol. Vis. Sci. 2005, 46, 4485–4488. [Google Scholar] [CrossRef]
- Hertz, P.; Bril, V.; Orszag, A.; Ahmed, A.; Ng, E.; Nwe, P.; Ngo, M.; Perkins, B. Reproducibility of in vivo corneal confocal microscopy as a novel screening test for early diabetic sensorimotor polyneuropathy. Diabet. Med. 2011, 28, 1253–1260. [Google Scholar] [CrossRef] [PubMed]
- Messmer, E.M.; Schmid-Tannwald, C.; Zapp, D.; Kampik, A. In vivo confocal microscopy of corneal small fiber damage in diabetes mellitus. Graefes. Arch. Clin. Exp. Ophthalmol. 2010, 248, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, M.; Kallinikos, P.; Iqbal, A.; Herbert, A.; Fadavi, H.; Efron, N.; Boulton, A.J.; Malik, R.A. Corneal confocal microscopy detects improvement in corneal nerve morphology with an improvement in risk factors for diabetic neuropathy. Diabet. Med. 2011, 28, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Zhivov, A.; Winter, K.; Hovakimyan, M.; Peschel, S.; Harder, V.; Schober, H.-C.; Kundt, G.; Baltrusch, S.; Guthoff, R.F.; Stachs, O. Imaging and Quantification of Subbasal Nerve Plexus in Healthy Volunteers and Diabetic Patients with or without Retinopathy. PLoS ONE 2013, 8, e52157. [Google Scholar] [CrossRef]
- Oakley, J.D.; Russakoff, D.B.; McCarron, M.E.; Weinberg, R.L.; Izzi, J.M.; Misra, S.L.; McGhee, C.N.; Mankowski, J.L. Deep learning-based analysis of macaque corneal sub-basal nerve fibers in confocal microscopy images. Eye Vis. 2020, 7, 27. [Google Scholar] [CrossRef]
- McCarron, M.E.; Weinberg, R.L.; Izzi, J.M.; Queen, S.E.; Tarwater, P.M.; Misra, S.L.; Russakoff, D.B.; Oakley, J.D.; Mankowski, J.L. Combining In Vivo Corneal Confocal Microscopy with Deep Learning–Based Analysis Reveals Sensory Nerve Fiber Loss in Acute Simian Immunodeficiency Virus Infection. Cornea 2021, 40, 635–642. [Google Scholar] [CrossRef]
- Cornblath, D.; Chaudhry, V.; Carter, K.; Lee, D.; Seysedadr, M.; Miernicki, M.; Joh, T. Total neuropathy score: Validation and reliability study. Neurology 1999, 53, 1660. [Google Scholar] [CrossRef]
- Sterne, J.A.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef]
- Beijers, A.; Mols, F.; Vreugdenhil, G. A systematic review on chronic oxaliplatin-induced peripheral neuropathy and the relation with oxaliplatin administration. Supportive Care Cancer 2014, 22, 1999–2007. [Google Scholar] [CrossRef]
- Park, S.B.; Goldstein, D.; Lin, C.S.-Y.; Krishnan, A.V.; Friedlander, M.L.; Kiernan, M.C. Acute abnormalities of sensory nerve function associated with oxaliplatin-induced neurotoxicity. J. Clin. Oncol. 2009, 27, 1243–1249. [Google Scholar] [CrossRef]
- Schmid, K.E.; Kornek, G.V.; Scheithauer, W.; Binder, S. Update on ocular complications of systemic cancer chemotherapy. Surv. Ophthalmol. 2006, 51, 19–40. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Moreno, A.; Liang, H.; Moreau, N.; Luzu, J.; Rabut, G.; Melik Parsadaniantz, S.; Labbé, A.; Baudouin, C.; Réaux-Le Goazigo, A. Corneal Nerve Abnormalities in Painful Dry Eye Disease Patients. Biomedicines 2021, 9, 1424. [Google Scholar] [CrossRef] [PubMed]
- Petropoulos, I.N.; Fitzgerald, K.C.; Oakley, J.; Ponirakis, G.; Khan, A.; Gad, H.; George, P.; Deleu, D.; Canibano, B.G.; Akhtar, N.; et al. Corneal confocal microscopy demonstrates axonal loss in different courses of multiple sclerosis. Sci. Rep. 2021, 11, 21688. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.L.; Kersten, H.M.; Roxburgh, R.H.; Danesh-Meyer, H.V.; McGhee, C.N. Corneal nerve microstructure in Parkinson’s disease. J. Clin. Neurosci. 2017, 39, 53–58. [Google Scholar] [CrossRef]
- Mesquida, M.; Sanchez-Dalmau, B.; Ortiz-Perez, S.; Pelegrín, L.; Molina-Fernandez, J.J.; Figueras-Roca, M.; Casaroli-Marano, R.; Adán, A. Oxaliplatin-related ocular toxicity. Case Rep. Oncol. 2010, 3, 423–427. [Google Scholar] [CrossRef]
- Marsovszky, L.; Nemeth, J.; Resch, M.D.; Toldi, G.; Legány, N.; Kovács, L.; Balog, A. Corneal Langerhans cell and dry eye examinations in ankylosing spondylitis. Innate Immun. 2014, 20, 471–477. [Google Scholar] [CrossRef]
- Wang, E.F.; Misra, S.L.; Patel, D.V. In vivo confocal microscopy of the human cornea in the assessment of peripheral neuropathy and systemic diseases. BioMed Res. Int. 2015, 2015, 951081. [Google Scholar] [CrossRef]
- Aggarwal, S.; Kheirkhah, A.; Cavalcanti, B.M.; Cruzat, A.; Colon, C.; Brown, E.; Borsook, D.; Prüss, H.; Hamrah, P. Autologous serum tears for treatment of photoallodynia in patients with corneal neuropathy: Efficacy and evaluation with in vivo confocal microscopy. Ocul. Surf. 2015, 13, 250–262. [Google Scholar] [CrossRef]
- Giannaccare, G.; Buzzi, M.; Fresina, M.; Velati, C.; Versura, P. Efficacy of 2-month treatment with cord blood serum eye drops in ocular surface disease: An in vivo confocal microscopy study. Cornea 2017, 36, 915–921. [Google Scholar] [CrossRef]
- Chinnery, H.R.; Rajan, R.; Jiao, H.; Wu, M.; Zhang, A.C.; De Silva, M.E.H.; Makrai, E.; Stepp, M.A.; Di Girolamo, N.; Downie, L.E. Identification of presumed corneal neuromas and microneuromas using laser-scanning in vivo confocal microscopy: A systematic review. Br. J. Ophthalmol. 2021, 10, 1136. [Google Scholar] [CrossRef]
- Pulvers, J.N.; Marx, G. Factors associated with the development and severity of oxaliplatin-induced peripheral neuropathy: A systematic review. Asia-Pac. J. Clin. Oncol. 2017, 13, 345–355. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | 6 Weeks | 12 Weeks | 20 Weeks | 36 Weeks | 52 Weeks | ||
|---|---|---|---|---|---|---|---|
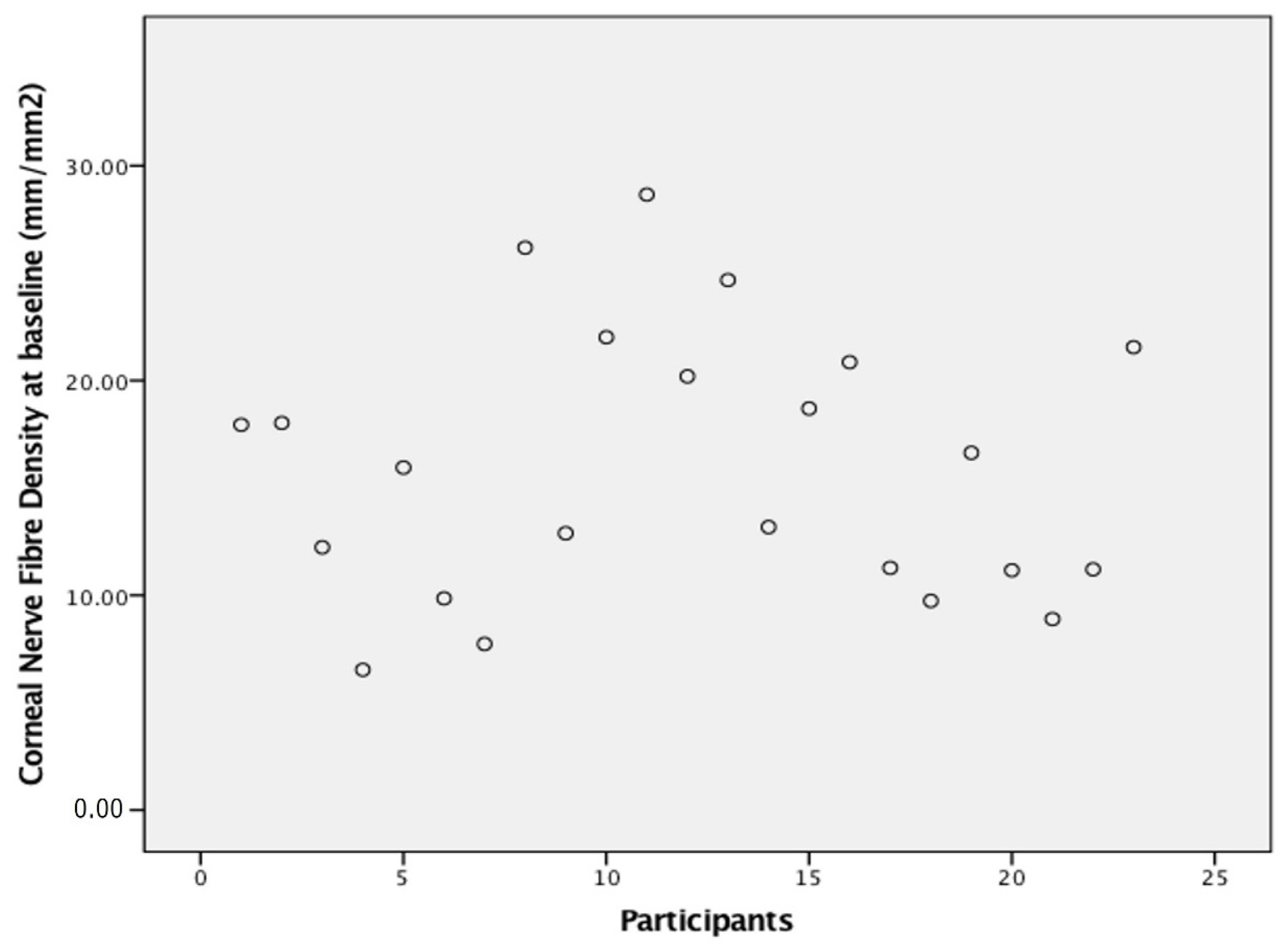
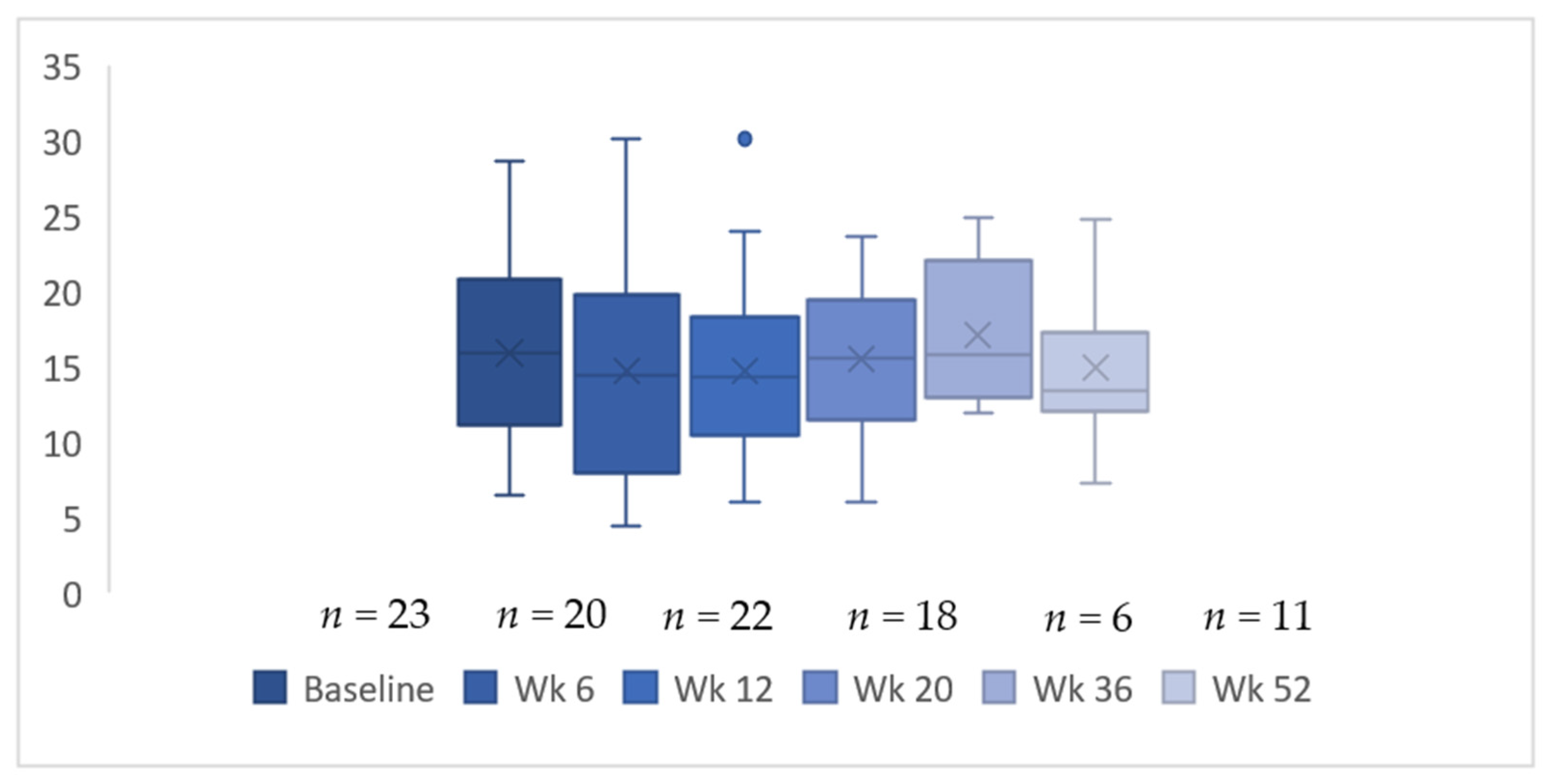
| n = 23 | n = 20 | n = 22 | n = 18 | n = 6 | n = 11 | ||
| Corneal sub-basal nerve density | 15.91 ± 6.2 | 14.73 ± 6.8 | 14.74 ± 5.8 | 15.51 ± 4.8 | 17.51 ± 4.9 | 14.91 ± 4.9 | |
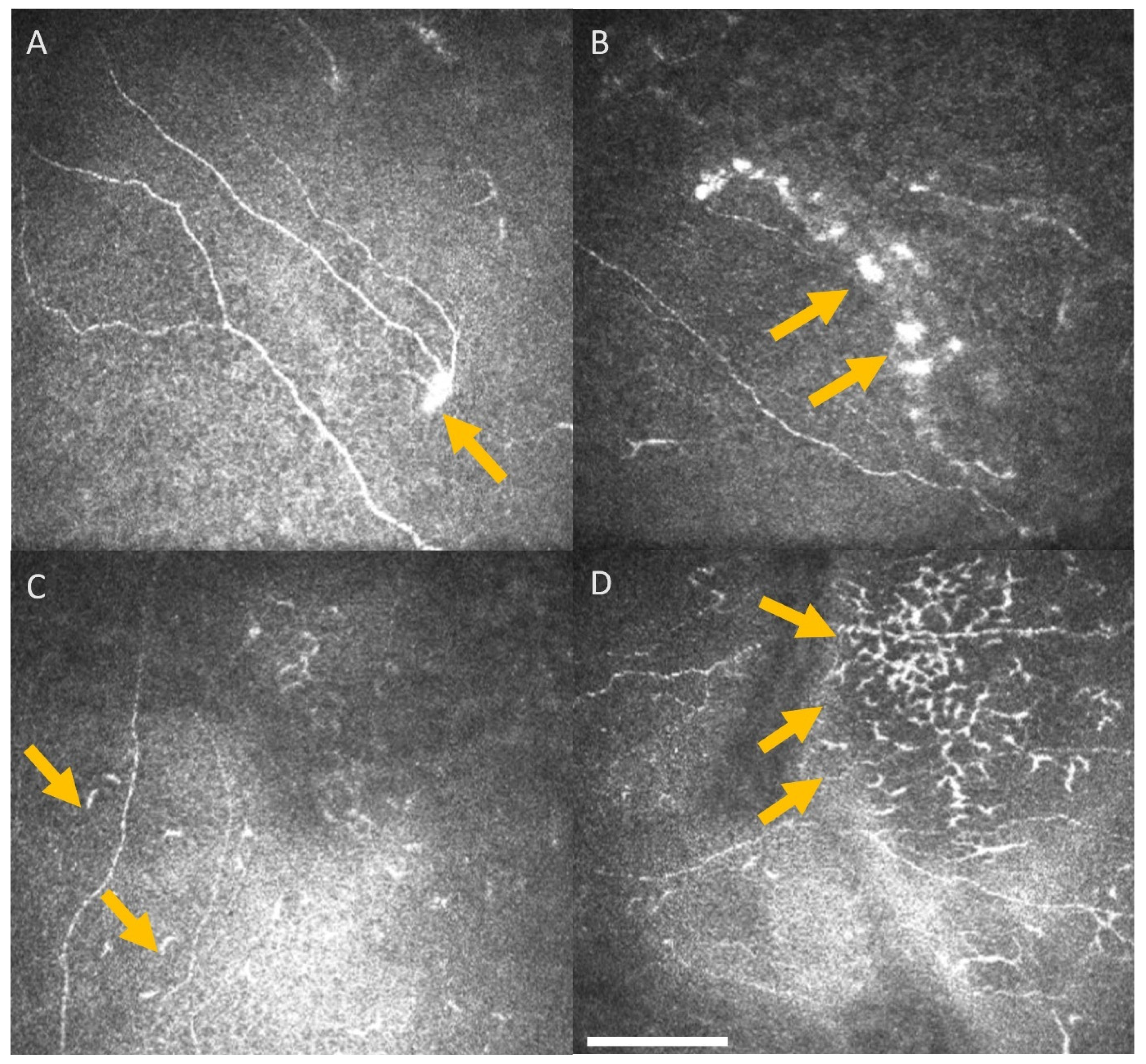
| Presence of dendritic cells (n) | 11 | 3 | 7 | 4 | 1 | 4 | |
| Presence of neuromas (n) | 9 | 10 | 6 | 8 | 3 | 3 | |
| Corneal sensitivity threshold | 0.39 ± 0.1 | 0.38 ± 0.2 | 0.49 ± 0.3 | 0.47 ± 0.3 | 0.25 ± 0.3 | 0.19 ± 0.3 | |
| Presence of peripheral neuropathy (n) (NCS or TNS) | 6 | 16 | 17 | 16 | 3 | 3 | |
| TNS score (0–30) | Median | 0 | 1 | 3 | 5 | 3.5 | 0 |
| Range | 0 | 0–7 | 0–7 | 0–13 | 0–13 | 0–14 | |
| NCS (0–10) | Median | 0 | 6 | ||||
| Range | 0 (n = 10) | 0–6 (n = 9) | |||||
| Presence of RAPD (n) | 0 | 0 | 0 | 0 | 0 | 0 | |
| Retinal abnormalities (n) | 0 | 0 | 0 | 0 | 0 | 0 | |
| Baseline CND | 6 Weeks CND | 12 Weeks CND | 20 Weeks CND | 36 Weeks CND | 52 Weeks CND | Patient Outcome | |
|---|---|---|---|---|---|---|---|
| Patient 1 | 17.94 | 11.98 | 12.47 | Deceased prior to 20 weeks | |||
| Patient 2 | 18.02 | 20.62 | 15.36 | 19.84 | Disease progression at 20 weeks and referred to hospice | ||
| Patient 3 | 12.23 | 12.18 | 8.99 | 14.06 | 11.91 | 12.01 | Completed follow up |
| Patient 4 | 6.53 | 4.43 | 6.61 | 10.26 | Disease progression at 20 weeks Rx 2nd line treatment. Lost to follow up | ||
| Patient 5 | 15.95 | 19.83 | 16.59 | 20.05 | 24.91 | 24.82 | Completed follow up |
| Patient 6 | 9.85 | 5.82 | 6.04 | Moved overseas and deceased | |||
| Patient 7 | 7.73 | 14.49 | 14.49 | 15.41 | 13.38 | 13.38 | Completed follow up |
| Patient 8 | 26.19 | 20.78 | 14.16 | 17.31 | 21.1 | 13.33 | Completed follow up |
| Patient 9 | 12.89 | 12.96 | 12.96 | 14.61 | 12.88 | Completed follow up | |
| Patient 10 | 22.02 | 17.82 | 17.06 | 14.82 | 16.37 | 16.37 | Completed follow up |
| Patient 11 | 28.66 | 30.11 | 30.11 | Had a stroke, chemotherapy terminated and too unwell to attend clinics | |||
| Patient 12 | 20.19 | 18.73 | Disease progression at 20 weeks and Rx 2nd line treatment. Lost to follow up | ||||
| Patient 13 | 24.67 | 15.34 | 9.13 | 11.92 | Offered resection of metastases at 20 weeks, no response to contact thereafter | ||
| Patient 14 | 13.18 | 11.68 | Too unwell to attend | ||||
| Patient 15 | 18.7 | 17.52 | 19.8 | 17.28 | 9.9 | Completed follow up | |
| Patient 16 | 20.86 | 23.96 | 23.96 | 22.17 | Lost to follow up after completion of Rx | ||
| Patient 17 | 11.27 | 6.77 | 5.99 | Lost to follow up after completion of Rx | |||
| Patient 18 | 9.74 | 10.94 | 8.99 | 15.25 | 17.3 | Completed follow up | |
| Patient 19 | 16.63 | 13.8 | 20.28 | 19.34 | 20.34 | Completed follow up | |
| Patient 20 | 11.16 | 17.39 | 15.64 | 15.64 | 16.39 | Completed follow up | |
| Patient 21 | 8.89 | 6.23 | 13.28 | 9.31 | 7.29 | Completed follow up | |
| Patient 22 | 11.21 | 7.92 | 7.92 | 18.63 | Lost to follow up after completion of Rx | ||
| Patient 23 | 21.55 | 18.1 | 23.61 | Lost to follow up after completion of Rx |
| Baseline | 6 Weeks | 12 Weeks | 20 Weeks | 52 Weeks | ||
|---|---|---|---|---|---|---|
| n = 23 | n = 20 | n = 22 | n = 18 | n = 11 | ||
| Corneal nerve density vs. TNS | r | −0.04 | −0.4 | 0.15 | −0.1 | −0.48 |
| p | 0.83 | 0.09 | 0.54 | 0.69 | 0.13 | |
| Corneal sensitivity vs. TNS | r | 0.12 | 0.34 | 0.55 * | 0.64 * | 0.05 |
| p | 0.57 | 0.17 | 0.01 * | 0.006 * | 0.88 | |
| Corneal nerve density vs. | r | 0.08 | 0.1 | 0.61 | 0.12 | |
| Cumulative dose of oxaliplatin | p | 0.74 | 0.69 | 0.01 | 0.72 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tyler, E.F.; McGhee, C.N.J.; Lawrence, B.; Braatvedt, G.D.; Mankowski, J.L.; Oakley, J.D.; Sethi, S.; Misra, S.L. Corneal Nerve Changes Observed by In Vivo Confocal Microscopy in Patients Receiving Oxaliplatin for Colorectal Cancer: The COCO Study. J. Clin. Med. 2022, 11, 4770. https://doi.org/10.3390/jcm11164770
Tyler EF, McGhee CNJ, Lawrence B, Braatvedt GD, Mankowski JL, Oakley JD, Sethi S, Misra SL. Corneal Nerve Changes Observed by In Vivo Confocal Microscopy in Patients Receiving Oxaliplatin for Colorectal Cancer: The COCO Study. Journal of Clinical Medicine. 2022; 11(16):4770. https://doi.org/10.3390/jcm11164770
Chicago/Turabian StyleTyler, Ellen F., Charles N. J. McGhee, Benjamin Lawrence, Geoffrey D. Braatvedt, Joseph L. Mankowski, Jonathan D. Oakley, Sargun Sethi, and Stuti L. Misra. 2022. "Corneal Nerve Changes Observed by In Vivo Confocal Microscopy in Patients Receiving Oxaliplatin for Colorectal Cancer: The COCO Study" Journal of Clinical Medicine 11, no. 16: 4770. https://doi.org/10.3390/jcm11164770