
Neuropsychological Predictors of Fatigue in Post-COVID Syndrome

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
- (1)
- To train several machine-learning algorithms using a dataset comprising a wide range of traditional “paper and pencil” and computerized neuropsychological assessments administered to a cohort of patients with PCS.
- (2)
- These models were trained to predict the presence of fatigue, several levels of fatigue severity, and the fatigue score of a perceived fatigue questionnaire.
- (3)
- We used a data-driven approach to evaluate the existence of linear and non-linear relationships between cognitive assessment results and subjective fatigue.
2. Materials and Methods
2.1. Participants
2.2. Fatigue Assessment
2.3. Neuropsychological Assessment
- Forward and backward digit span
- Corsi block-tapping test
- Symbol Digit Modalities Test
- Boston Naming Test
- Judgment of Line Orientation
- Rey–Osterrieth Complex Figure (copy, recall at 3 and 30 min, and recognition)
- Free and Cued Selective Reminding Test
- Verbal fluencies (animals and words beginning with “p” and “m”; 1 min for each)
- Stroop Color–Word Interference Test
- Visual Object and Space Perception Battery.
- Trail Making Test (Langensteinbach version), parts A and B (S1 form).
- Figural Memory Test (S11 form)
- Response inhibition (S13 form)
- N-Back verbal (S1 form)
- Tower of London (Freiburg version) (TOL, S1 form).
2.4. Statistical and Machine Learning Analysis
3. Results
3.1. Sample Description
3.2. Correlations between MFIS and Neuropsychological Tests
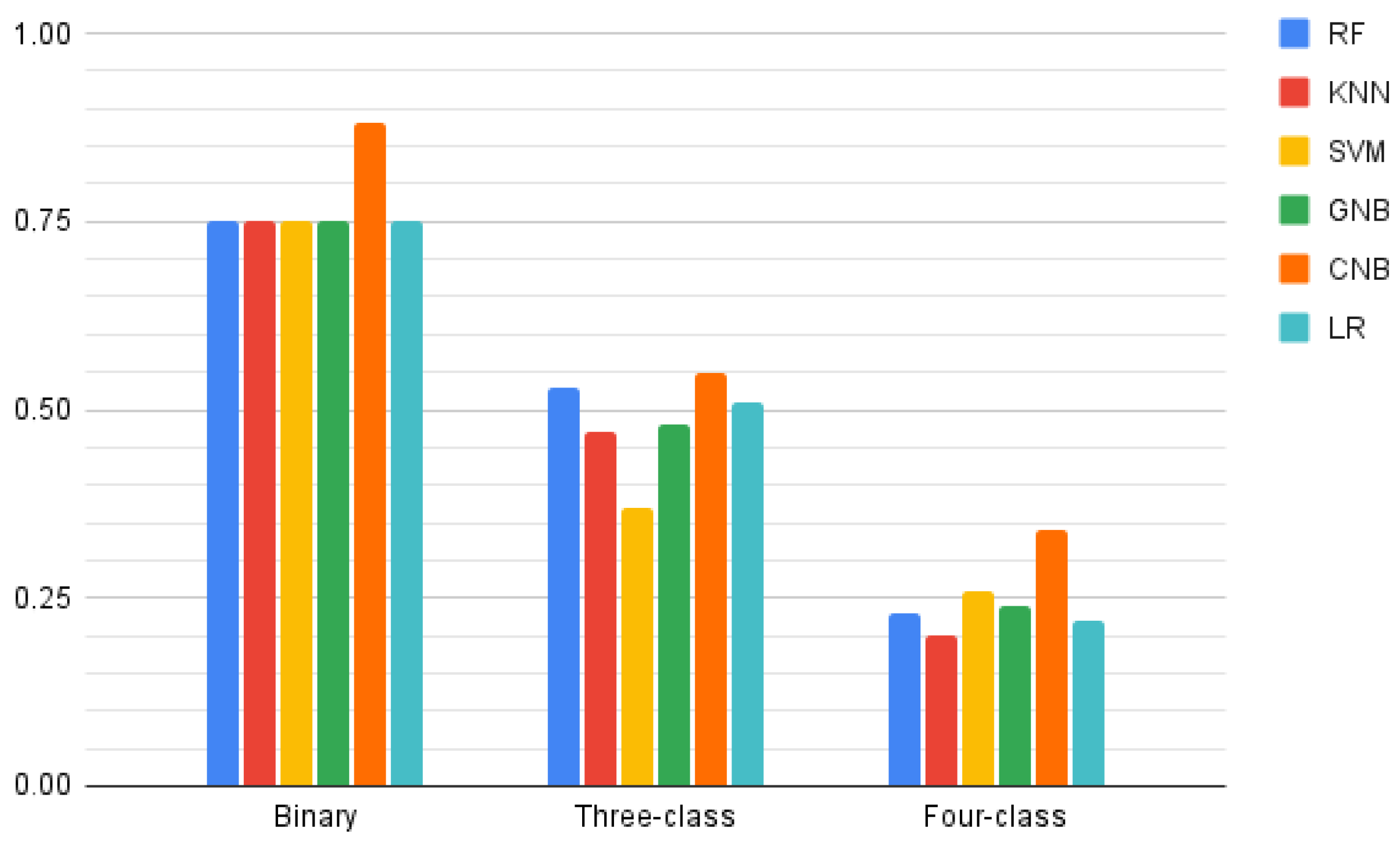
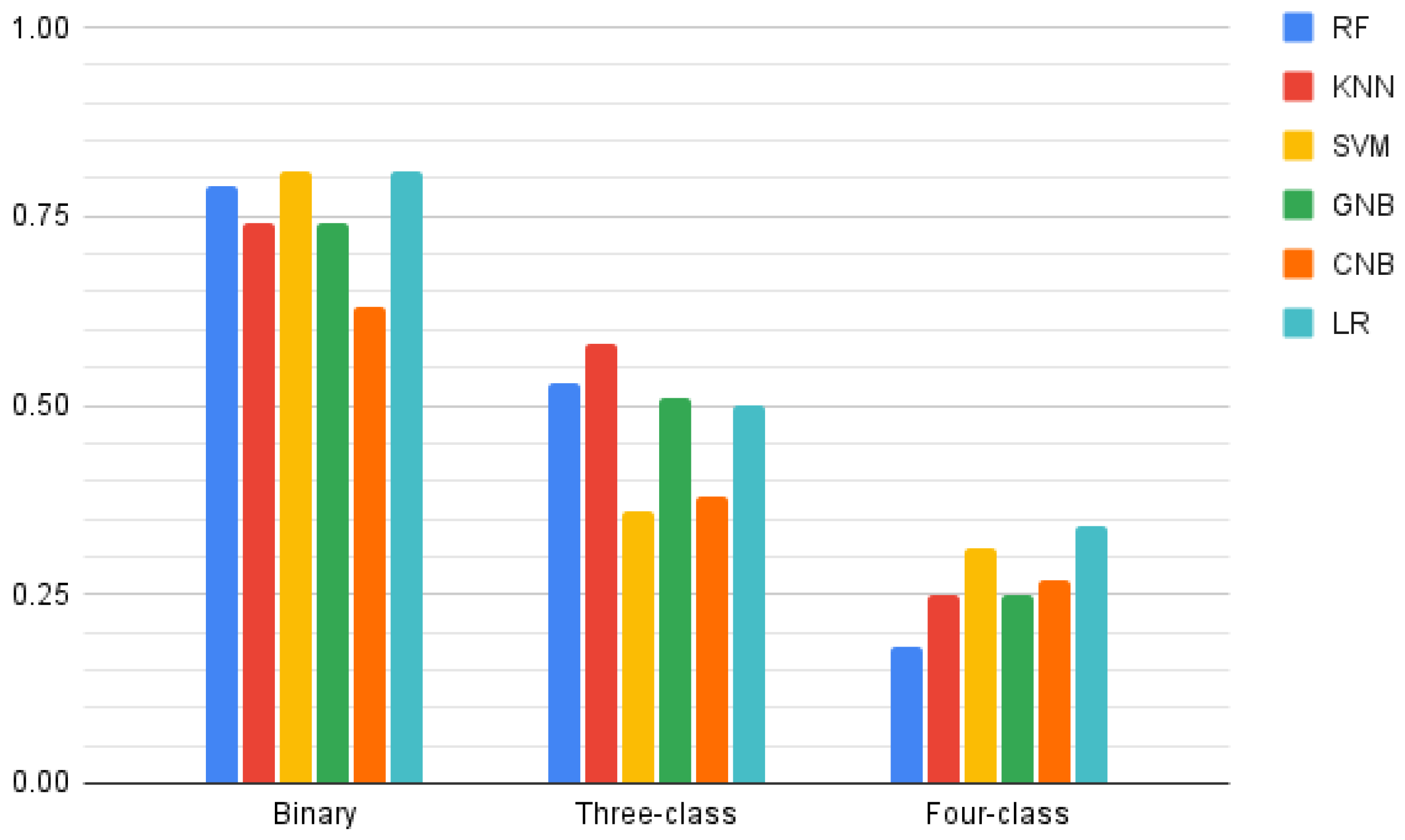
3.3. Classification Models
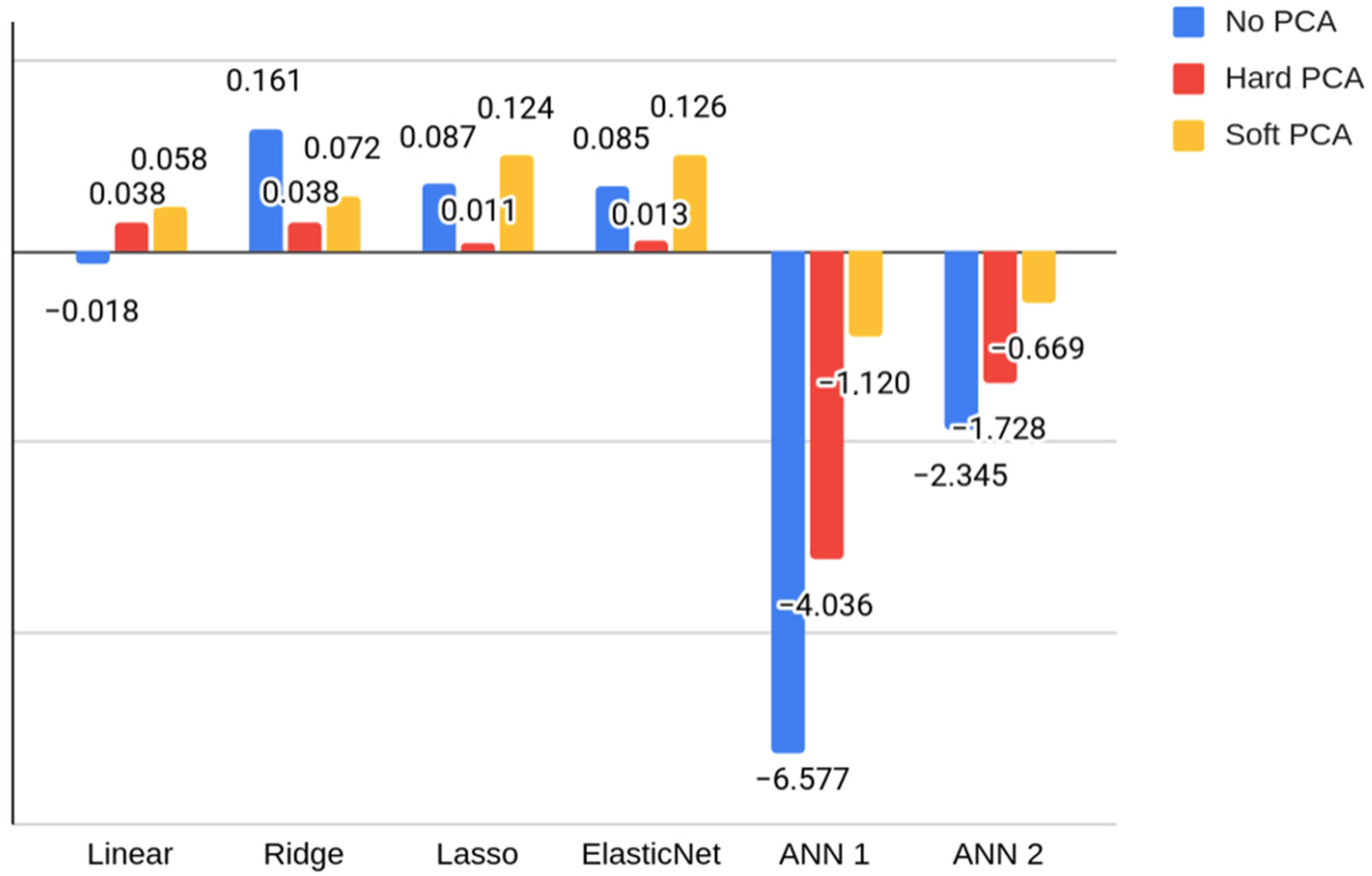
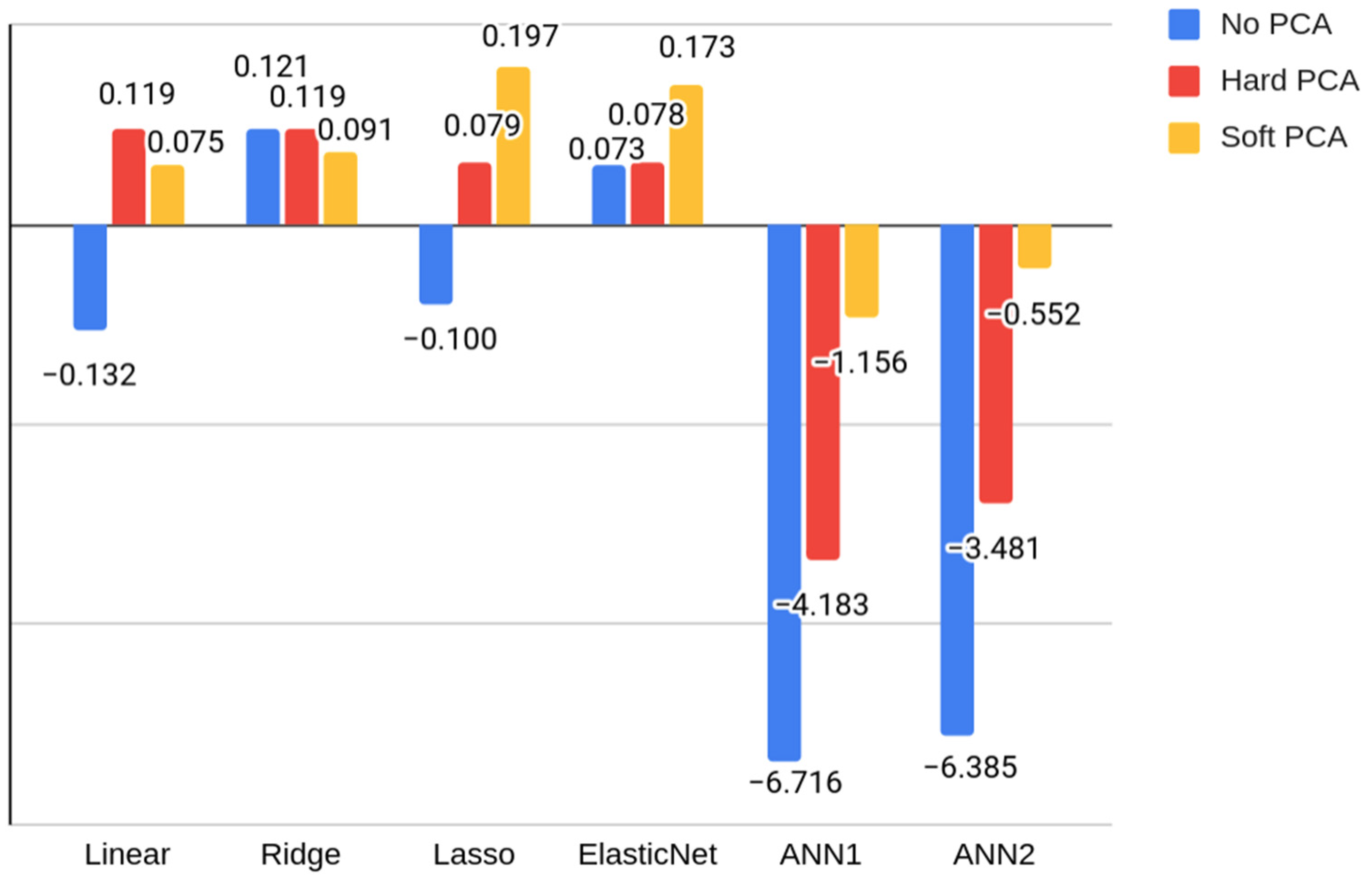
3.4. Regression Models
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chaudhuri, A.; Behan, P.O. Fatigue in neurological disorders. Lancet 2004, 363, 978–988. [Google Scholar] [CrossRef]
- Palotai, M.; Guttmann, C.R. Brain anatomical correlates of fatigue in multiple sclerosis. Mult. Scler. J. 2019, 26, 751–764. [Google Scholar] [CrossRef] [PubMed]
- Ren, P.; Anderson, A.J.; McDermott, K.; Baran, T.M.; Lin, F. Cognitive fatigue and cortico-striatal network in old age. Aging 2019, 11, 2312–2326. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Álvarez, A.; Matías-Guiu, J.A.; Delgado-Alonso, C.; Cuevas, C.; Palacios-Sarmiento, M.; Vidorreta-Ballesteros, L.; Montero-Escribano, P.; Matías-Guiu, J. Validation of two new scales for the assessment of fatigue in Multiple Sclerosis: F-2-MS and FACIT-F. Mult. Scler. Relat. Disord. 2022, 63, 103826. [Google Scholar] [CrossRef]
- Kos, D.; Kerckhofs, E.; Carrea, I.; Verza, R.; Ramos, M.; Jansa, J. Evaluation of the Modified Fatigue Impact Scale in four different European countries. Mult. Scler. J. 2005, 11, 76–80. [Google Scholar] [CrossRef]
- Hanken, K.; Eling, P.; Hildebrandt, H. Is there a cognitive signature for MS-related fatigue? Mult. Scler. 2015, 21, 376–381. [Google Scholar] [CrossRef]
- Linnhoff, S.; Fiene, M.; Heinze, H.-J.; Zaehle, T. Cognitive Fatigue in Multiple Sclerosis: An Objective Approach to Diagnosis and Treatment by Transcranial Electrical Stimulation. Brain Sci. 2019, 9, 100. [Google Scholar] [CrossRef] [Green Version]
- Berard, J.A.; Smith, A.M.; Walker, L. Predictive Models of Cognitive Fatigue in Multiple Sclerosis. Arch. Clin. Neuropsychol. 2019, 34, 31–38. [Google Scholar] [CrossRef]
- Mackay, L.; Johnson, A.M.; Moodie, S.T.; Rosehart, H.; Morrow, S.A. Predictors of cognitive fatigue and fatigability in multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 56, 103316. [Google Scholar] [CrossRef]
- Mehandru, S.; Merad, M. Pathological sequelae of long-haul COVID. Nat. Immunol. 2022, 23, 194–202. [Google Scholar] [CrossRef]
- Vanichkachorn, G.; Newcomb, R.; Cowl, C.T.; Murad, M.H.; Breeher, L.; Miller, S.; Trenary, M.; Neveau, D.; Higgins, S. Post–COVID-19 Syndrome (long haul syndrome): Description of a multidisciplinary clinic at mayo clinic and characteristics of the initial patient cohort. Mayo Clin. Proc. 2021, 96, 1782–1791. [Google Scholar] [CrossRef] [PubMed]
- de las Peñas, C.F.; Martín-Guerrero, J.D.; Cancela-Cilleruelo, I.; Moro-López-Menchero, P.; Pellicer-Valero, O. Exploring the recovery curve for long-term post-COVID dyspnea and fatigue. Eur. J. Intern. Med. 2022, 117, 201–203. [Google Scholar] [CrossRef]
- Delgado-Alonso, C.; Valles-Salgado, M.; Delgado-Álvarez, A.; Yus, M.; Gómez-Ruiz, N.; Jorquera, M.; Polidura, C.; Gil, M.J.; Marcos, A.; Matías-Guiu, J.; et al. Cognitive dysfunction associated with COVID-19: A comprehensive neuropsychological study. J. Psychiatr. Res. 2022, 150, 40–46. [Google Scholar] [CrossRef] [PubMed]
- García-Sánchez, C.; Calabria, M.; Grunden, N.; Pons, C.; Arroyo, J.A.; Gómez-Anson, B.; Lleó, A.; Alcolea, D.; Belvís, R.; Morollón, N.; et al. Neuropsychological deficits in patients with cognitive complaints after COVID-19. Brain Behav. 2022, 12, e2508. [Google Scholar] [CrossRef] [PubMed]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; McCarthy, P.; Lange, F.; Andersson, J.L.R.; Griffanti, L.; Duff, E.; et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Yus, M.; Matias-Guiu, J.A.; Gil-Martínez, L.; Gómez-Ruiz, N.; Polidura, C.; Jorquera, M.; Delgado-Alonso, C.; Díez-Cirarda, M.; Matías-Guiu, J.; Arrazola, J. Persistent olfactory dysfunction after COVID-19 is associated with reduced perfusion in the frontal lobe. Acta Neurol. Scand. 2022, in press. [Google Scholar] [CrossRef]
- Huang, S.; Zhou, Z.; Yang, D.; Zhao, W.; Zeng, M.; Xie, X.; Du, Y.; Jiang, Y.; Zhou, X.; Yang, W.; et al. Persistent white matter changes in recovered COVID-19 patients at the 1-year follow-up. Brain 2022, 145, 1830–1838. [Google Scholar] [CrossRef]
- Huang, Y.; Ling, Q.; Manyande, A.; Wu, D.; Xiang, B. Brain imaging changes in patients recovered from COVID-19: A Narrative Review. Front. Neurosci. 2022, 16, 5868. [Google Scholar] [CrossRef]
- Ortelli, P.; Ferrazzoli, D.; Sebastianelli, L.; Engl, M.; Romanello, R.; Nardone, R.; Bonini, I.; Koch, G.; Saltuari, L.; Quartarone, A.; et al. Neuropsychological and neurophysiological correlates of fatigue in post-acute patients with neurological manifestations of COVID-19: Insights into a challenging symptom. J. Neurol. Sci. 2021, 420, 117271. [Google Scholar] [CrossRef]
- Ortelli, P.; Ferrazzoli, D.; Sebastianelli, L.; Maestri, R.; Dezi, S.; Spampinato, D.; Saltuari, L.; Alibardi, A.; Engl, M.; Kofler, M.; et al. Altered motor cortex physiology and dysexecutive syndrome in patients with fatigue and cognitive difficulties after mild COVID-19. Eur. J. Neurol. 2022, 29, 1652–1662. [Google Scholar] [CrossRef]
- Kurki, S.N.; Kantonen, J.; Kaivola, K.; Hokkanen, L.; Mäyränpää, M.I.; Puttonen, H.; Martola, J.; Pöyhönen, M.; Kero, M.; Tuimala, J.; et al. APOE ε4 associates with increased risk of severe COVID-19, cerebral microhaemorrhages and post-COVID mental fatigue: A Finnish biobank, autopsy and clinical study. Acta Neuropathol. Commun. 2021, 9, 199. [Google Scholar] [CrossRef] [PubMed]
- Ruz-Caracuel, I.; Pian-Arias, H.; Corral, I.; Carretero-Barrio, I.; Bueno-Sacristán, D.; Pérez-Mies, B.; García-Cosío, M.; Caniego-Casas, T.; Pizarro, D.; García-Narros, M.I.; et al. Neuropathological findings in fatal COVID-19 and their associated neurological clinical manifestations. Pathology 2022. [Google Scholar] [CrossRef] [PubMed]
- Maiese, A.; Manetti, A.C.; Bosetti, C.; Del Duca, F.; La Russa, R.; Frati, P.; Di Paolo, M.; Turillazzi, E.; Fineschi, V. SARS-CoV-2 and the brain: A review of the current knowledge on neuropathology in COVID-19. Brain Pathol. 2021, 31, e13013. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; Wang, Y.; Zheng, J. COVID-19 and Alzheimer’s disease: How one crisis worsens the other. Transl. Neurodegener. 2021, 10, 15. [Google Scholar] [CrossRef]
- Frontera, J.A.; Simon, N.M. Bridging knowledge gaps in the diagnosis and management of neuropsychiatric sequelae of COVID-19. JAMA Psychiatry 2022, in press. [Google Scholar] [CrossRef]
- Becker, R.C. Autonomic dysfunction in SARS-COV-2 infection acute and long-term implications COVID-19 editor’s page series. J. Thromb. Thrombolysis 2021, 52, 692–707. [Google Scholar] [CrossRef]
- Paul, B.D.; Lemle, M.D.; Komaroff, A.L.; Snyder, S.H. Redox imbalance links COVID-19 and myalgic encephalomyelitis/chronic fatigue syndrome. Proc. Natl. Acad. Sci. USA 2021, 118, e2024358118. [Google Scholar] [CrossRef]
- Gómez-Pinedo, U.; Matias-Guiu, J.; Sanclemente-Alaman, I.; Moreno-Jimenez, L.; Montero-Escribano, P.; Matias-Guiu, J.A. Is the brain a reservoir organ for SARS-CoV2? J. Med. Virol. 2020, 92, 2354–2355. [Google Scholar] [CrossRef]
- Zollner, A.; Koch, R.; Jukic, A.; Pfister, A.; Meyer, M.; Rössler, A.; Kimpel, J.; Adolph, T.E.; Tilg, H. Postacute COVID-19 is Characterized by Gut Viral Antigen Persistence in Inflammatory Bowel Diseases. Gastroenterology 2022, in press. [Google Scholar] [CrossRef]
- Ramakrishnan, R.K.; Kashour, T.; Hamid, Q.; Halwani, R.; Tleyjeh, I.M. Unraveling the Mystery Surrounding Post-Acute Sequelae of COVID-19. Front. Immunol. 2021, 12, 686029. [Google Scholar] [CrossRef]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Fisk, J.D.; Ritvo, P.G.; Ross, L.; Haase, D.A.; Marrie, T.J.; Schlech, W.F. Measuring the functional impact of fatigue: Initial validation of the Fatigue Impact Scale. Clin. Infect. Dis. 1994, 18 (Suppl. S1), S79–S83. [Google Scholar] [CrossRef] [PubMed]
- Larson, R.D. Psychometric Properties of the Modified Fatigue Impact Scale. Int. J. MS Care 2013, 15, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peña-Casanova, J.; Blesa, R.; Aguilar, M.; Gramunt, N.; Gómez-Ansón, B.; Oliva, R.; Molinuevo, J.L.; Robles, A.; Barquero, M.S.; Antúnez, C.; et al. Spanish Multicenter Normative Studies (NEURONORMA Project): Methods and Sample Characteristics. Arch. Clin. Neuropsychol. 2009, 24, 307–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peña-Casanova, J.; Casals-Coll, M.; Quintana, M.; Sánchez-Benavides, G.; Rognoni, T.; Calvo, L.; Palomo, R.; Aranciva, F.; Tamayo, F.; Manero, R. Spanish normative studies in a young adult population (NEURONORMA young adults project): Methods and characteristics of the sample. Neurologia 2012, 27, 253–260. [Google Scholar] [CrossRef]
- Aschenbrenner, S.; Kaiser, S.; Pfüller, U.; Roesch-Ely, D.; Weisbrod, M. Testset COGBAT; Schuhfried GmbH: Mödling, Austria, 2012. [Google Scholar]
- Ceban, F.; Ling, S.; Lui, L.M.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav. Immun. 2021, 101, 93–135. [Google Scholar] [CrossRef]
- Peña-Casanova, J.; Quiñones-Úbeda, S.; Gramunt-Fombuena, N.; Quintana, M.; Aguilar, M.; Molinuevo, J.L.; Serradell, M.; Robles, A.; Barquero, M.S.; Payno, M.; et al. Spanish Multicenter Normative Studies (NEURONORMA Project): Norms for the Stroop Color-Word Interference Test and the Tower of London-Drexel. Arch. Clin. Neuropsychol. 2009, 24, 413–429. [Google Scholar] [CrossRef]
- Kok, A. Cognitive control, motivation and fatigue: A cognitive neuroscience perspective. Brain Cogn. 2022, 160, 105880. [Google Scholar] [CrossRef]
- Calabria, M.; García-Sánchez, C.; Grunden, N.; Pons, C.; Arroyo, J.A.; Gómez-Anson, B.; García, M.d.C.E.; Belvís, R.; Morollón, N.; Igual, J.V.; et al. Post-COVID-19 fatigue: The contribution of cognitive and neuropsychiatric symptoms. J. Neurol. 2022. [Google Scholar] [CrossRef]
- Wylie, G.R.; Yao, B.; Genova, H.M.; Chen, M.H.; DeLuca, J. Using functional connectivity changes associated with cognitive fatigue to delineate a fatigue network. Sci. Rep. 2020, 10, 21927. [Google Scholar] [CrossRef]
- Pessiglione, M.; Vinckier, F.; Bouret, S.; Daunizeau, J.; Le Bouc, R. Why not try harder? Computational approach to motivation deficits in neuro-psychiatric diseases. Brain 2017, 141, 629–650. [Google Scholar] [CrossRef] [Green Version]
- Matias-Guiu, J.A.; Cabrera-Martin, M.N.; Valles-Salgado, M.; Rognoni, T.; Galán, L.; Moreno-Ramos, T.; Carreras, J.L.; Matías-Guiu, J. Inhibition impairment in frontotemporal dementia, amyotrophic lateral sclerosis, and Alzheimer’s disease: Clinical assessment and metabolic correlates. Brain Imaging Behav. 2019, 13, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, R.; Grach, S.L.; Ghosh, A.K.; Bierle, D.M.; Salonen, B.R.; Collins, N.M.; Joshi, A.Y.; Boeder, N.D.; Anstine, C.V.; Mueller, M.R.; et al. The Female-Predominant Persistent Immune Dysregulation of the Post-COVID Syndrome. Mayo Clin. Proc. 2022, 97, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Bafna, T.; Bækgaard, P.; Hansen, J.P. Mental fatigue prediction during eye-typing. PLoS ONE 2021, 16, e0246739. [Google Scholar] [CrossRef] [PubMed]
- Hooda, R.; Joshi, V.; Shah, M. A comprehensive review of approaches to detect fatigue using machine learning techniques. Chronic Dis. Transl. Med. 2021, 8, 26–35. [Google Scholar] [CrossRef] [PubMed]
- De la Vega, R.; Anabalón, H.; Jara, C.; Villamil-Cabello, E.; Chervellino, M.; Calvo-Rodríguez, A. Effectiveness of mobile technology in managing fatigue: Balert App. Front. Psychol. 2021, 12, 704955. [Google Scholar] [CrossRef]
- Matias-Guiu, J.A.; Cortés-Martínez, A.; Montero, P.; Pytel, V.; Moreno-Ramos, T.; Jorquera, M.; Yus, M.; Arrazola, J.; Matías-Guiu, J. Structural MRI correlates of PASAT performance in multiple sclerosis. BMC Neurol. 2018, 18, 214. [Google Scholar] [CrossRef] [Green Version]
- Pitteri, M.; Dapor, C.; DeLuca, J.; Chiaravalloti, N.D.; Marastoni, D.; Calabrese, M. Slowing processing speed is associated with cognitive fatigue in newly diagnosed multiple sclerosis patients. J. Int. Neuropsychol. Soc. 2022, in press. [Google Scholar] [CrossRef]
- Cortés-Martínez, A.; Matías-Guiu, J.A.; Pytel, V.; Montero, P.; Moreno-Ramos, T.; Matías-Guiu, J. What is the meaning of PASAT rejection in multiple sclerosis? Acta Neurol. Scand. 2019, 139, 559–562. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Age (years), mean ± SD | 50.94 ± 11.90 |
| Sex (women) | 73 (64.60%) |
| Months from acute onset to assessment, mean ± SD | 11.14 ± 4.67 |
| Years of education, mean ± SD | 14.12 ± 3.84 |
| Hypertension | 32 (28.32%) |
| Diabetes | 15 (13.27%) |
| Dyslipidemia | 35 (30.97%) |
| Smokers | 18 (15.93%) |
| SARS-CoV-2 reinfection | 10 (8.8%) |
| Hospital admission | 33 (29.20%) |
| Days of hospitalization, mean ± SD | 19.25 ± 14.12 |
| ICU admission | 10 (8.85%) |
| Ventilatory support | 11 (9.73%) |
| Classification Type | RF | KNN | SVM | GNB | CNB | LR | |
|---|---|---|---|---|---|---|---|
| MFIS-total score | Binary | 0.75 | 0.75 | 0.75 | 0.75 | 0.88 | 0.75 |
| Three-classes | 0.53 | 0.47 | 0.37 | 0.48 | 0.55 | 0.51 | |
| Four-classes | 0.23 | 0.20 | 0.26 | 0.24 | 0.34 | 0.22 | |
| MFIS-cognitive score | Binary | 0.79 | 0.74 | 0.81 | 0.74 | 0.63 | 0.81 |
| Three-classes | 0.53 | 0.58 | 0.36 | 0.51 | 0.38 | 0.50 | |
| Four-classes | 0.18 | 0.25 | 0.31 | 0.25 | 0.27 | 0.34 |
| Test Scores | Linear Regression | Ridge Regression | Lasso Regression | Elastic Net Regression | |
|---|---|---|---|---|---|
| MFIS-total score | Raw | −0.857 | 0.005 | −0.149 | −0.052 |
| Scaled | −0.018 | 0.161 | 0.087 | 0.085 | |
| Computerized | −0.940 | −0.490 | −0.208 | −0.237 | |
| MFIS-cognitive | Raw | −0.383 | 0.104 | −0.100 | −0.020 |
| Scaled | −0.132 | 0.121 | −0.100 | 0.073 | |
| Computerized | −0.683 | −0.185 | −0.062 | −0.014 |
| Feature Reduction | Linear | Ridge | Lasso | Elastic Net | ANN 1 | ANN 2 | |
|---|---|---|---|---|---|---|---|
| MFIS-total score | None | −0.018 | 0.161 | 0.087 | 0.085 | −6.577 | −2.345 |
| Hard PCA | 0.038 | 0.038 | 0.011 | 0.013 | −4.036 | −1.728 | |
| Soft PCA | 0.058 | 0.072 | 0.124 | 0.126 | −1.120 | −0.669 | |
| MFIS-cognitive score | None | −0.132 | 0.121 | −0.100 | 0.073 | −6.716 | −6.385 |
| Hard PCA | 0.119 | 0.119 | 0.079 | 0.078 | −4.183 | −3.481 | |
| Soft PCA | 0.075 | 0.091 | 0.197 | 0.173 | −1.156 | −0.552 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matias-Guiu, J.A.; Delgado-Alonso, C.; Díez-Cirarda, M.; Martínez-Petit, Á.; Oliver-Mas, S.; Delgado-Álvarez, A.; Cuevas, C.; Valles-Salgado, M.; Gil, M.J.; Yus, M.; et al. Neuropsychological Predictors of Fatigue in Post-COVID Syndrome. J. Clin. Med. 2022, 11, 3886. https://doi.org/10.3390/jcm11133886
Matias-Guiu JA, Delgado-Alonso C, Díez-Cirarda M, Martínez-Petit Á, Oliver-Mas S, Delgado-Álvarez A, Cuevas C, Valles-Salgado M, Gil MJ, Yus M, et al. Neuropsychological Predictors of Fatigue in Post-COVID Syndrome. Journal of Clinical Medicine. 2022; 11(13):3886. https://doi.org/10.3390/jcm11133886
Chicago/Turabian StyleMatias-Guiu, Jordi A., Cristina Delgado-Alonso, María Díez-Cirarda, Álvaro Martínez-Petit, Silvia Oliver-Mas, Alfonso Delgado-Álvarez, Constanza Cuevas, María Valles-Salgado, María José Gil, Miguel Yus, and et al. 2022. "Neuropsychological Predictors of Fatigue in Post-COVID Syndrome" Journal of Clinical Medicine 11, no. 13: 3886. https://doi.org/10.3390/jcm11133886