
Neoadjuvant Chemo-Immunotherapy for Locally Advanced Non-Small-Cell Lung Cancer: A Review of the Literature



Abstract
:1. Introduction
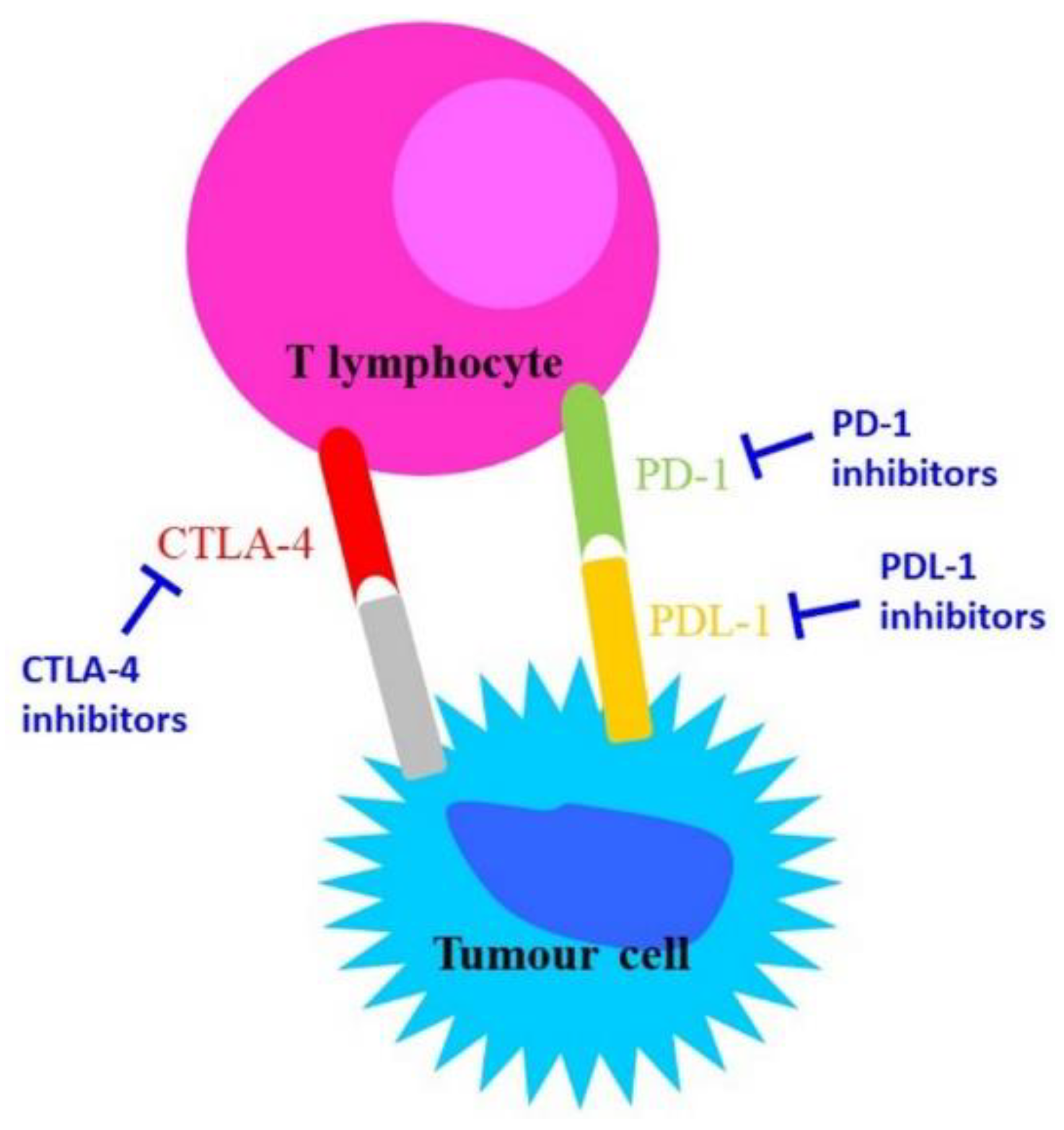
2. Immune Check-Points on Immunotherapy
Immune Checkpoints Inhibitors in Cancer
3. Histopathological Aspects
Biomarkers
4. Immunochemotherapy in Oncology
4.1. Phase II Clinical Trials of Neoadjuvant Immunochemotherapy

{kind=link}
{kind=link}
| Trial | Patients (M/F) | Age (Median) | Stage | Treatment | Primary Endpoint | Results |
|---|---|---|---|---|---|---|
| NCT03081689 (NADIM) [35] | 46 (34/12) | 63 | IIIA (N2) | Nivolumab + paclitaxel and carboplatin | PFS (at 24 months) | PFS: 77.1% MPR: 83% pCR: 63% |
| NCT03366766 [36] | 13 (8/5) | 69 | IB (≥4 cm)–IIIA | Nivolumab + cisplatin and pemetrexed or cisplatin and gemcitabine | MPR | MPR: 85% pCR: 38% |
| NCT02716038 [37] | 30(15/15) | 67 | IB–IIIA | Atezolizumab + carboplatin and nab-paclitaxel | MPR | MPR: 57% pCR: 33% |
| NCT02572843 (SAKK 16/14) [38] | 67 (35/32) | 61 | IIIA (N2) | Durvalumab + cisplatin and docetaxel | EFS (at 12 months) | EFS: 73.3% MPR: 60% pCR: 18.2% |
| NCT04304248 (neoTPD01) [39] | 33 (27/6) | 61 | IIIA–IIIB–(T3-4 N2) | Toripalimab + carboplatin and pemetrexed or carboplatin and nab-paclitaxel | MPR | MPR: 60.6% pCR: 45.5% |
4.2. Phase III Clinical Trials of Neoadjuvant Immunochemotherapy
| Trial | Stage | Neoadjuvant Treatment | Adjuvant Treatment | Primary Endpoint | Status |
|---|---|---|---|---|---|
| NCT02998528 Checkmate816 [41,42] | IIB–IIIA | Platinum + vinorelbine/pemetrexed/gemcitabine/docetaxel/paclitaxel + nivolumab vs. Platinum + vinorelbine/pemetrexed/gemcitabine/docetaxel/paclitaxel | NA | pCR; EFS | Active, not recruiting |
| NCT04025879 Checkmate77T [43] | IIA–IIIB (T3N2) | Platinum + pemetrexed/docetaxel/paclitaxel + nivolumab vs. Platinum + pemetrexed/docetaxel/paclitaxel | Nivolumab for 1year vs. placebo | EFS | Recruiting |
| NCT03456063 Impower030 [44] | II–IIIA–IIIB (T3N2) | Platinum + pemetrexed/gemcitabine/nab-paclitaxel + atezolizumab vs. Platinum + pemetrexed/gemcitabine/nab-paclitaxel | Atezolizumab for 48weeks vs. placebo | EFS | Active, not recruiting |
| NCT03425643 KEYNOTE671 [45] | IIA–IIIA–IIIB (N2) | Cisplatin + pemetrexed/gemcitabine + pembrolizumab vs. Cisplatin + pemetrexed/gemcitabine | Pembrolizumab for 39weeks vs. placebo | EFS; OS | Recruiting |
| NCT03800134 AEGEAN [46] | IIA–IIIA -IIIB(N2) | Platinum + pemetrexed/gemcitabine/paclitaxel + durvalumab vs. Platinum + pemetrexed/gemcitabine/paclitaxel | Durvalumab for 1 year vs. placebo | pCR; EFS | Recruiting |
5. Surgery after Immunochemotherapy
- Effect on surgery timing and delay for adverse effects;
- Effect on cardiopulmonary function and performance status;
- Technical difficulty of surgical resection and potential complications;
- Necessity of surgery reconsideration in case of disease progression.
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kryczka, J.; Kryczka, J.; Czarnecka-Chrebelska, K.H.; Brzeziańska-Lasota, E. Molecular Mechanisms of Chemoresistance Induced by Cisplatin in NSCLC Cancer Therapy. Int. J. Mol. Sci. 2021, 22, 8885. [Google Scholar] [CrossRef]
- Linee Guida NEOPLASIE DEL POLMONE Edizione. 2020. Available online: https://www.aiom.it/linee-guida-aiom-2020-neoplasie-del-polmone/ (accessed on 10 January 2021).
- Ulas, E.B.; Dickhoff, C.; Schneiders, F.L.; Senan, S.; Bahce, I. Neoadjuvant Immune Checkpoint Inhibitors in Resectable Non-small-Cell Lung Cancer: A Systematic Review. ESMO Open 2021, 6, 100244. [Google Scholar] [CrossRef] [PubMed]
- FDA. FDA Approves Neoadjuvant Nivolumab and Platinum-Doublet Chemotherapy for Early-Stage Non-Small Cell Lung Cancer; FDA: Silver Spring, MD, USA, 2022.
- Wherry, E.J.; Kurachi, M. Molecular and Cellular Insights into T Cell Exhaustion. Nat. Rev. Immunol. 2015, 15, 486–499. [Google Scholar] [CrossRef] [PubMed]
- Pietrobon, V.; Todd, L.A.; Goswami, A.; Stefanson, O.; Yang, Z.; Marincola, F. Improving CAR T-Cell Persistence. Int. J. Mol. Sci. 2021, 22, 10828. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Ito, M.; Srirat, T.; Kondo, T.; Yoshimura, A. Memory T Cell, Exhaustion, and Tumor Immunity. Immunol. Med. 2020, 43, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Waldman, A.D.; Fritz, J.M.; Lenardo, M.J. A Guide to Cancer Immunotherapy: From T Cell Basic Science to Clinical Practice. Nat. Rev. Immunol. 2020, 20, 651–668. [Google Scholar] [CrossRef]
- Philip, M.; Schietinger, A. Heterogeneity and Fate Choice: T Cell Exhaustion in Cancer and Chronic Infections. Curr. Opin. Immunol. 2019, 58, 98–103. [Google Scholar] [CrossRef]
- De Mello, R.A.; Veloso, A.F.; Catarina, P.E.; Nadine, S.; Antoniou, G. Potential Role of Immunotherapy in Advanced Non-small-Cell Lung Cancer. OncoTargets Ther. 2016, 10, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Whiteside, T.L. The Tumor Microenvironment and Its Role in Promoting Tumor Growth. Oncogene 2008, 27, 5904–5912. [Google Scholar] [CrossRef] [Green Version]
- Remon, J.; Soria, J.-C.; Peters, S. Early and Locally Advanced Non-small-Cell Lung Cancer: An Update of the ESMO Clinical Practice Guidelines Focusing on Diagnosis, Staging, Systemic and Local Therapy. Ann. Oncol. 2021, 32, 1637–1642. [Google Scholar] [CrossRef]
- Kalemkerian, G.P.; Narula, N.; Kennedy, E.B.; Biermann, W.A.; Donington, J.; Leighl, N.B.; Lew, M.; Pantelas, J.; Ramalingam, S.S.; Reck, M.; et al. Molecular Testing Guideline for the Selection of Patients with Lung Cancer for Treatment with Targeted Tyrosine Kinase Inhibitors: American Society of Clinical Oncology Endorsement of the College of American Pathologists/International Association for the Study of Lung Cancer/Association for Molecular Pathology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic Non-Small Cell Lung Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef] [PubMed]
- Haratake, N.; Seto, T. NTRK Fusion-positive Non–small-cell Lung Cancer: The Diagnosis and Targeted Therapy. Clin. Lung Cancer 2021, 22, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Wistuba, I.I. Molecular Testing of Non–Small Cell Lung Carcinoma Biopsy and Cytology Specimens. Am. Soc. Clin. Oncol. Educ. Book 2012, 32, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Cooper, W.A.; Russell, P.A.; Cherian, M.; Duhig, E.E.; Godbolt, D.; Jessup, P.J.; Khoo, C.; Leslie, C.; Mahar, A.; Moffat, D.F.; et al. Intra- and Interobserver Reproducibility Assessment of PD-L1 Biomarker in Non–Small Cell Lung Cancer. Clin. Cancer Res. 2017, 23, 4569–4577. [Google Scholar] [CrossRef] [Green Version]
- Rimm, D.L.; Han, G.; Taube, J.M.; Yi, E.S.; Bridge, J.A.; Flieder, D.B.; Homer, R.; West, W.W.; Wu, H.; Roden, A.C. A Prospective, Multi-Institutional, Pathologist-Based Assessment of 4 Immunohistochemistry Assays for PD-L1 Expression in Non–Small Cell Lung Cancer. JAMA Oncol. 2017, 3, 1051–1058. [Google Scholar] [CrossRef]
- Tsao, M.S.; Kerr, K.M.; Kockx, M.; Beasley, M.-B.; Borczuk, A.C.; Botling, J.; Bubendorf, L.; Chirieac, L.; Chen, G.; Chou, T.-Y.; et al. PD-L1 Immunohistochemistry Comparability Study in Real-Life Clinical Samples: Results of Blueprint Phase 2 Project. J. Thorac. Oncol. 2018, 13, 1302–1311. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, J.; Han, G.; Schalper, K.A.; Carvajal-Hausdorf, D.; Pelekanou, V.; Rehman, J.; Velcheti, V.; Herbst, R.; Lorusso, P.; Rimm, D.L. Quantitative Assessment of the Heterogeneity of PD-L1 Expression in Non-Small-Cell Lung Cancer. JAMA Oncol. 2016, 2, 46–54. [Google Scholar] [CrossRef]
- Munari, E.; Zamboni, G.; Lunardi, G.; Marchionni, L.; Marconi, M.; Sommaggio, M.; Brunelli, M.; Martignoni, G.; Netto, G.J.; Hoque, M.O.; et al. PD-L1 Expression Heterogeneity in Non–Small Cell Lung Cancer: Defining Criteria for Harmonization between Biopsy Specimens and Whole Sections. J. Thorac. Oncol. 2018, 13, 1113–1120. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.J.; Herbst, R.S.; Goldberg, S.B. Selecting the Optimal Immunotherapy Regimen in Driver-Negative Metastatic NSCLC. Nat. Rev. Clin. Oncol. 2021, 18, 625–644. [Google Scholar] [CrossRef]
- Mao, Z.; Jiang, P.; Zhang, Y.; Li, Y.; Jia, X.; Wang, Q.; Jiao, M.; Jiang, L.; Shen, Y.; Guo, H.; et al. First-line Immune-based Combination Therapies for Advanced Non-small Cell Lung Cancer: A Bayesian Network Meta-analysis. Cancer Med. 2021, 10, 9139–9155. [Google Scholar] [CrossRef] [PubMed]
- Pagni, F.; Guerini-Rocco, E.; Schultheis, A.M.; Grazia, G.; Rijavec, E.; Ghidini, M.; Lopez, G.; Venetis, K.; Croci, G.A.; Malapelle, U.; et al. Targeting Immune-Related Biological Processes in Solid Tumors: We do Need Biomarkers. Int. J. Mol. Sci. 2019, 20, 5452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, T.A.; Yarchoan, M.; Jaffee, E.; Swanton, C.; Quezada, S.A.; Stenzinger, A.; Peters, S. Development of Tumor Mutation Burden as an Immunotherapy Biomarker: Utility for the Oncology Clinic. Ann. Oncol. 2019, 30, 44–56. [Google Scholar] [CrossRef]
- Jardim, D.L.; Goodman, A.; de Melo Gagliato, D.; Kurzrock, R. The Challenges of Tumor Mutational Burden as an Immunotherapy Biomarker. Cancer Cell 2021, 39, 154–173. [Google Scholar] [CrossRef] [PubMed]
- Heydt, C.; Rehker, J.; Pappesch, R.; Buhl, T.; Ball, M.; Siebolts, U.; Haak, A.; Lohneis, P.; Büttner, R.; Hillmer, A.M.; et al. Analysis of Tumor Mutational Burden: Correlation of Five Large Gene Panels with Whole Exome Sequencing. Sci. Rep. 2020, 10, 11387. [Google Scholar] [CrossRef] [PubMed]
- Pepe, F.; Pisapia, P.; Gristina, V.; Rocco, D.; Bs, M.M.; Micheli, P.; Iaccarino, A.; Tufano, R.; Bs, G.G.; De Luca, C.; et al. Tumor Mutational Burden on Cytological Samples: A Pilot Study. Cancer Cytopathol. 2020, 129, 460–467. [Google Scholar] [CrossRef]
- Wang, Z.; Duan, J.; Cai, S.; Han, M.; Dong, H.; Zhao, J.; Zhu, B.; Wang, S.; Zhuo, M.; Sun, J.; et al. Assessment of Blood Tumor Mutational Burden as a Potential Biomarker for Immunotherapy in Patients with Non–Small Cell Lung Cancer with Use of a Next-Generation Sequencing Cancer Gene Panel. JAMA Oncol. 2019, 5, 696–702. [Google Scholar] [CrossRef]
- Alborelli, I.; Leonards, K.; Rothschild, S.I.; Leuenberger, L.P.; Prince, S.S.; Mertz, K.; Poechtrager, S.; Buess, M.; Zippelius, A.; Läubli, H.; et al. Tumor Mutational Burden Assessed by Targeted NGS Predicts Clinical Benefit from Immune Checkpoint Inhibitors in Non-Small Cell Lung Cancer. J. Pathol. 2019, 250, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Mooradian, M.J.; Piotrowska, Z.; Drapkin, B.J.; Dias-Santagata, D.; Marcoux, N.; Arnaoutakis, K.; Nagy, R.J.; Lanman, R.; Iafrate, A.J.; Farago, A.F.; et al. Clonal Evolution and the Role of Serial Liquid Biopsies in a Case of Small-Cell Lung Cancer–Transformed EGFR Mutant Non–Small-Cell Lung Cancer. JCO Precis. Oncol. 2017, 1, 1–7. [Google Scholar] [CrossRef]
- Wu, F.; Fan, J.; He, Y.; Xiong, A.; Yu, J.; Li, Y.; Zhang, Y.; Zhao, W.; Zhou, F.; Li, W.; et al. Single-Cell Profiling of Tumor Heterogeneity and the Microenvironment in Advanced Non-small Cell Lung Cancer. Nat. Commun. 2021, 12, 2540. [Google Scholar] [CrossRef]
- Zito Marino, F.; Bianco, R.; Accardo, M.; Ronchi, A.; Cozzolino, I.; Morgillo, F.; Rossi, G.; Franco, R. Molecular Heterogeneity in Lung Cancer: From Mechanisms of Origin to Clinical Implications. Int. J. Med. Sci. 2019, 16, 981–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, A.; Incorvaia, L.; Del Re, M.; Malapelle, U.; Capoluongo, E.; Gristina, V.; Castiglia, M.; Danesi, R.; Fassan, M.; Giuffrè, G.; et al. The Molecular Profiling of Solid Tumors by Liquid Biopsy: A Position Paper of the AIOM–SIAPEC-IAP–SIBioC–SIC–SIF Italian Scientific Societies. ESMO Open 2021, 6, 100164–100176. [Google Scholar] [CrossRef]
- Provencio, M.; Nadal, E.; Insa, A.; García-Campelo, M.R.; Casal-Rubio, J.; Dómine, M.; Majem, M.; Rodríguez-Abreu, D.; Martínez-Martí, A.; de Castro Carpeño, J.; et al. Neoadjuvant Chemotherapy and Nivolumab in Resectable Non-small-Cell Lung Cancer (NADIM): An Open-Label, Multicentre, Single-Arm, Phase 2 Trial. Lancet Oncol. 2020, 21, 1413–1422. [Google Scholar] [CrossRef]
- Zinner, R.; Axelrod, R.; Solomides, C.C.; Cowan, S.; Leiby, B.; Bhatia, A.K.; Sundermeyer, M.L.; Hooper, D.C.; Harshyne, L.; Lu-Yao, G.L.; et al. Neoadjuvant Nivolumab (N) Plus Cisplatin (C)/Pemetrexed (P) or Cisplatin /Gemcitabine (G) in Resectable NSCLC. J. Clin. Oncol. 2020, 38, 9051. [Google Scholar] [CrossRef]
- Shu, C.A.; Gainor, J.F.; Awad, M.M.; Chiuzan, C.; Grigg, C.M.; Pabani, A.; Garofano, R.F.; Stoopler, M.B.; Cheng, S.K.; White, A.; et al. Neoadjuvant Atezolizumab and Chemotherapy in Patients with Resectable Non-small-Cell Lung Cancer: An Open-Label, Multicentre, Single-Arm, Phase 2 Trial. Lancet Oncol. 2020, 21, 786–795. [Google Scholar] [CrossRef]
- Rothschild, S.I.; Zippelius, A.; Eboulet, E.I.; Savic Prince, S.; Betticher, D.; Bettini, A.; Früh, M.; Joerger, M.; Lardinois, D.; Gelpke, H.; et al. SAKK 16/14: Durvalumab in Addition to Neoadjuvant Chemotherapy in Patients with Stage IIIA(N2) Non–Small-Cell Lung Cancer—A Multicenter Single-Arm Phase II Trial. J. Clin. Oncol. 2021, 39, 2872–2880. [Google Scholar] [CrossRef]
- Zhao, Z.-R.; Yang, C.-P.; Chen, S.; Yu, H.; Lin, Y.-B.; Lin, Y.-B.; Qi, H.; Jin, J.-T.; Lian, S.-S.; Wang, Y.-Z.; et al. Phase 2 Trial of Neoadjuvant Toripalimab with Chemotherapy for Resectable Stage III Non-small-Cell Lung Cancer. OncoImmunology 2021, 10, 1996000. [Google Scholar] [CrossRef]
- NCT04245514. Multimodality Treatment in Stage III Non-Small Cell Lung Cancer (NSCLC). Available online: https://clinicaltrials.gov/ct2/show/NCT04245514?cond=NCT04245514&draw=2&rank=1 (accessed on 16 February 2022).
- Forde, P.M.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Felip, E.; Broderick, S.; Brahmer, J.; Swanson, S.J.; et al. Abstract CT003: Nivolumab (NIVO) + Platinum-Doublet Chemotherapy (Chemo) vs Chemo as Neoadjuvant Treatment (tx) for Resectable (IB-IIIA) Non-Small Cell Lung Cancer (NSCLC) in the Phase 3 CheckMate 816 Trial. Cancer Res. 2021, 81, CT003. [Google Scholar] [CrossRef]
- Spicer, J.; Wang, C.; Tanaka, F.; Saylors, G.B.; Chen, K.N.; Liberman, M.; Vokes, E.E.; Girard, N.; Lu, S.; Provencio, M.; et al. Surgical Outcomes from the Phase 3 CheckMate 816 Trial: Nivolumab (NIVO) + Platinum-Doublet Chemotherapy (Chemo) vs Chemo Alone as Neoadjuvant Treatment for Patients with Resectable Non-small Cell Lung Cancer (NSCLC). J. Clin. Oncol. 2021, 39, 8503. [Google Scholar] [CrossRef]
- Cascone, T.; Provencio, M.; Sepesi, B.; Lu, S.; Aanur, N.; Li, S.; Spicer, J. Checkmate 77T: A phase III Trial of Neoadjuvant Nivolumab (NIVO) Plus Chemotherapy (Chemo) Followed by Adjuvant Nivo in Resectable Early-Stage NSCLC. J. Clin. Oncol. 2020, 38, TPS9076. [Google Scholar] [CrossRef]
- Peters, S.; Kim, A.W.; Solomon, B.; Gandara, D.R.; Dziadziuszko, R.; Brunelli, A.; Garassino, M.C.; Reck, M.; Wang, L.; To, I.; et al. IMpower030: Phase III Study Evaluating Neoadjuvant Treatment of Resectable Stage II-IiiB Non-small Cell Lung Cancer (NSCLC) with Atezolizumab (Atezo) + Chemotherapy. Ann. Oncol. 2019, 30, ii30. [Google Scholar] [CrossRef]
- Tsuboi, M.; Luft, A.; Ursol, G.; Kato, T.; Levchenko, E.; Eigendorff, E.; Berard, H.; Zurawski, B.; Demedts, I.; Garassino, M.C.; et al. 1235TiP Perioperative Pembrolizumab + Platinum-Based Chemotherapy for Resectable Locally Advanced Non-small Cell Lung Cancer: The Phase III KEYNOTE-671 study. Ann. Oncol. 2020, 31, S801–S802. [Google Scholar] [CrossRef]
- Heymach, J.V.; Mitsudomi, T.; Harpole, D.; Aperghis, M.; Jones, S.; Mann, H.; Fouad, T.M.; Reck, M. Design and Rationale for a Phase III, Double-Blind, Placebo-Controlled Study of Neoadjuvant Durvalumab+Chemotherapy Followed by Adjuvant Durvalumab for the Treatment of Patients with Resectable Stages II and III Non-Small-Cell Lung Cancer: The AEGEAN Tr. Clin. Lung Cancer 2021. [Google Scholar] [CrossRef] [PubMed]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; ESMO Guidelines Committee. Early and Locally Advanced Non-Small-Cell Lung Cancer (NSCLC): ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up. Ann. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. Version 2.2021. JNCCN 2021. Available online: https://www.nccn.org/ (accessed on 10 January 2021).
- Maconachie, R.; Mercer, T.; Navani, N.; McVeigh, G. Lung Cancer: Diagnosis and Management: Summary of Updated NICE Guidance. BMJ 2019, 364, l1049. [Google Scholar] [CrossRef]
- Wood, L.S.; Moldawer, N.P.; Lewis, C. Immune Checkpoint Inhibitor Therapy: Key Principles When Educating Patients. Clin. J. Oncol. Nurs. 2019, 23, 271–280. [Google Scholar] [CrossRef]
- Yang, C.-F.J.; McSherry, F.; Mayne, N.R.; Wang, X.; Berry, M.F.; Tong, B.; Harpole, D.H.; D’Amico, T.A.; Christensen, J.D.; Ready, N.E.; et al. Surgical Outcomes After Neoadjuvant Chemotherapy and Ipilimumab for Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2018, 105, 924–929. [Google Scholar] [CrossRef] [Green Version]
- Romero Román, A.; Campo-Cañaveral de la Cruz, J.L.; Macía, I.; Escobar Campuzano, I.; Figueroa Almánzar, S.; Delgado Roel, M.; Gálvez Muñoz, C.; García Fontán, E.M.; Muguruza Trueba, I.; Romero Vielva, L.; et al. Outcomes of Surgical Resection after Neoadjuvant Chemoimmunotherapy in Locally Advanced Stage IIIA Non-Small-Cell Lung Cancer. Eur. J. Cardio-Thoracic Surg. 2021, 60, 81–88. [Google Scholar] [CrossRef]
- Edge, S.B.; Byrd, D.R.; Compton, C.C. AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2010. [Google Scholar]
- Bott, M.J.; Yang, S.C.; Park, B.J.; Adusumilli, P.S.; Rusch, V.W.; Isbell, J.M.; Downey, R.J.; Brahmer, J.R.; Battafarano, R.; Bush, E.; et al. Initial Results of Pulmonary Resection after Neoadjuvant Nivolumab in Patients with Resectable Non–Small Cell Lung Cancer. J. Thorac. Cardiovasc. Surg. 2019, 158, 269–276. [Google Scholar] [CrossRef]
- Remark, R.; Lupo, A.; Alifano, M.; Biton, J.; Ouakrim, H.; Stefani, A.; Cremer, I.; Goc, J.; Régnard, J.-F.; Dieu-Nosjean, M.-C.; et al. Immune Contexture and Histological Response after Neoadjuvant Chemotherapy Predict Clinical Outcome of Lung Cancer Patients. OncoImmunology 2016, 5, e1255394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, H.; Yang, C.; Gonzalez-Rivas, D.; Zhong, Y.; He, P.; Deng, H.; Liu, J.; Liang, W.; He, J.; Li, S. Sleeve Lobectomy after Neoadjuvant Chemoimmunotherapy/Chemotherapy for Local Advanced Non-small Cell Lung Cancer. Transl. Lung Cancer Res. 2021, 10, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.; Liu, J.; Cai, X.; Chen, J.; Rocco, G.; Petersen, R.H.; Brunelli, A.; Ng, C.S.H.; D’Amico, T.A.; Liang, W.; et al. Radical Minimally invasive surgery following immuno-chemotherapy in Initially-unresectable stage IIIB Non-small cell lung cancer. Ann. Surg. 2022, 275, e600–e602. [Google Scholar] [CrossRef] [PubMed]
- Lazzari, C.; Karachaliou, N.; Bulotta, A.; Viganó, M.; Mirabile, A.; Brioschi, E.; Santarpia, M.; Gianni, L.; Rosell, R.; Gregorc, V.; et al. Combination of Immunotherapy with Chemotherapy and Radiotherapy in Lung Cancer: Is This the Beginning of the End for Cancer? Ther. Adv. Med. Oncol. 2018, 10, 1758835918762094. [Google Scholar] [CrossRef]
- Paez, J.G.; Jänne, P.A.; Lee, J.C.; Tracy, S.; Greulich, H.; Gabriel, S.; Herman, P.; Kaye, F.J.; Lindeman, N.; Boggon, T.J.; et al. EGFR Mutations in Lung Cancer: Correlation with Clinical Response to Gefitinib Therapy. Science 2004, 304, 1497–1500. [Google Scholar] [CrossRef] [Green Version]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, Activity, and Immune Correlates of Anti–PD-1 Antibody in Cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Carbone, D.; Lee, J.; Kris, M.; Wistuba, I.; Kwiatkowski, D.; Owen, D.; Bunn, P.; Johnson, B.; Oezkan, F.; Tang, Y.; et al. OA06.06 Clinical/Biomarker Data for Neoadjuvant Atezolizumab in Resectable Stage IB-IIIB NSCLC: Primary Analysis in the LCMC3 Study. J. Thorac. Oncol. 2021, 16, S115–S116. [Google Scholar] [CrossRef]
- Besse, B.; Adam, J.; Cozic, N.; Chaput-Gras, N.; Planchard, D.; Mezquita, I.; Remon, J.; Masip, P.; Lavaud, P.; Naltet, C.; et al. Neoadjuvant Atezolizumab (A) for Resectable Non-Small Cell Lung Cancer (SCLC): Results from the Phase II PRINCEPS Trial. Ann. Onco. 2020, 31, S794–S795. [Google Scholar] [CrossRef]
- Eichhorn, F.; Klotz, L.V.; Bischoff, H.; Thomas, M.; Lasitschka, F.; Winter, H.; Hoffmann, H.; Eichhorn, M.E. Neoadjuvant Anti-programmed Death-1 Immunotherapy by Pembrolizumab in Resectable Nodal Positive Stage II/Iiia Non-small-Cell Lung Cancer (NSCLC): The NEOMUN Trial. BMC Cancer 2019, 19, 413. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Li, N.; Gao, S.; Xue, Q.; Ying, J.; Wang, S.; Tao, X.; Zhao, J.; Mao, Y.; Wang, B.; et al. Neoadjuvant PD-1 Inhibitor (Sintilimab) in NSCLC. J. Thorac. Oncol. 2020, 15, 816–826. [Google Scholar] [CrossRef] [Green Version]
- Wislez, M.; Mazieres, J.; Lavole, A.; Zalcman, G.; Carre, O.; Egenod, T.; Caliandro, R.; Gervais, R.; Jeannin, G.; Molinier, O.; et al. 1214O Neoadjuvant Durvalumab in Resectable Non-Small Cell Lung Cancer (NSCLC): Preliminary Results from a Multicenter Study (IFCT-1601 IONESCO). Ann. Oncol. 2020, 31, S794. [Google Scholar] [CrossRef]
- Cascone, T.; William, W.N., Jr.; Weissferdt, A.; Leung, C.H.; Lin, H.Y.; Pataer, A.; Godoy, M.C.B.; Carter, B.W.; Federico, L.; Reuben, A.; et al. Neoadjuvant Nivolumab or Nivolumab Plus Ipilimumab in Operable Non-small Cell Lung Cancer: The Phase 2 Randomized NEOSTAR Trial. Nat. Med. 2021, 27, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Soh, J.; Hamada, A.; Fujino, T.; Mitsudomi, T. Perioperative Therapy for Non-Small Cell Lung Cancer with Immune Checkpoint Inhibitors. Cancers 2021, 13, 4035. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Wang, Y.; Gao, Y.; Sugimura, H.; Minervini, F.; Uchino, J.; Halmos, B.; Yendamuri, S.; Velotta, J.B.; Li, M. Neoadjuvant Immunotherapy or Chemoimmunotherapy in Non-small Cell Lung Cancer: A Systematic Review and Meta-Analysis. Transl. Lung Cancer Res. 2022, 11, 277–294. [Google Scholar] [CrossRef] [PubMed]
- Spini, A.; Gini, R.; Rosellini, P.; Singier, A.; Bellan, C.; Pascucci, A.; Leoncini, L.; Mathieu, C.; Martellucci, I.; Furiesi, F.; et al. First-Line Pharmacotherapies and Survival among Patients Diagnosed with Non-Resectable NSCLC: A Real-Life Setting Study with Gender Prospective. Cancers 2021, 13, 6129. [Google Scholar] [CrossRef]
- Irelli, A.; Sirufo, M.M.; D’Ugo, C.; Ginaldi, L.; De Martinis, M. Sex and Gender Influences on Cancer Immunotherapy Response. Biomedicines 2020, 8, 232. [Google Scholar] [CrossRef]
- Pradhan, M.; Chocry, M.; Gibbons, D.L.; Sepesi, B.; Cascone, T. Emerging Biomarkers for Neoadjuvant Immune Checkpoint Inhibitors in Operable Non-small Cell Lung Cancer. Transl. Lung Cancer Res. 2021, 10, 590–606. [Google Scholar] [CrossRef]
- Ramnath, N.; Dilling, T.J.; Harris, L.J.; Kim, A.W.; Michaud, G.C.; Balekian, A.A.; Diekember, R.; Detterbeck, F.C.; Arenberg, D.A. Treatment of Stage III Non-Small Cell Lung Cancer: Diagnosis and Management of Lung Cancer, 3rd Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2013, 143, 314–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenthal, G.M.; Bunn, P.A., Jr.; Chaft, J.E.; McCoach, C.E.; Perez, E.A.; Scagliotti, G.V.; Carbone, D.P.; Aerts, H.J.; Aisner, D.L.; Bergh, J.; et al. Current Status and Future Perspectives on Neoadjuvant Therapy in Lung Cancer. J. Thorac. Oncol. 2018, 13, 1818–1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Meerbeeck, J.P.; Kramer, G.W.P.M.; Van Schil, P.E.Y.; Legrand, C.; Smit, E.F.; Schramel, F.; Tjan-Heijnen, V.C.; Biesma, B.; Debruyne, C.; van Zandwijk, N.; et al. Randomized Controlled Trial of Resection Versus Radiotherapy After Induction Chemotherapy in Stage IIIA-N2 Non-Small-Cell Lung Cancer. J. Natl. Cancer Inst. 2007, 99, 442–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef]
- Eichhorn, F.; Klotz, L.V.; Kriegsmann, M.; Bischoff, H.; Schneider, M.A.; Muley, T.; Kriegsmann, K.; Haberkorn, U.; Heussel, C.P.; Savai, R.; et al. Neoadjuvant Anti-programmed Death-1 Immunotherapy by Pembrolizumab in Resectable Non-small Cell Lung Cancer: First Clinical Experience. Lung Cancer 2021, 153, 150–157. [Google Scholar] [CrossRef]
- Kennedy, L.B.; Salama, A.K. A Review of Cancer Immunotherapy Toxicity. CA Cancer J. Clin. 2020, 70, 86–104. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franzi, S.; Mattioni, G.; Rijavec, E.; Croci, G.A.; Tosi, D. Neoadjuvant Chemo-Immunotherapy for Locally Advanced Non-Small-Cell Lung Cancer: A Review of the Literature. J. Clin. Med. 2022, 11, 2629. https://doi.org/10.3390/jcm11092629
Franzi S, Mattioni G, Rijavec E, Croci GA, Tosi D. Neoadjuvant Chemo-Immunotherapy for Locally Advanced Non-Small-Cell Lung Cancer: A Review of the Literature. Journal of Clinical Medicine. 2022; 11(9):2629. https://doi.org/10.3390/jcm11092629
Chicago/Turabian StyleFranzi, Sara, Giovanni Mattioni, Erika Rijavec, Giorgio Alberto Croci, and Davide Tosi. 2022. "Neoadjuvant Chemo-Immunotherapy for Locally Advanced Non-Small-Cell Lung Cancer: A Review of the Literature" Journal of Clinical Medicine 11, no. 9: 2629. https://doi.org/10.3390/jcm11092629