
Surgical Applications of Lymphatic Vessel Visualization Using Photoacoustic Imaging and Augmented Reality

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
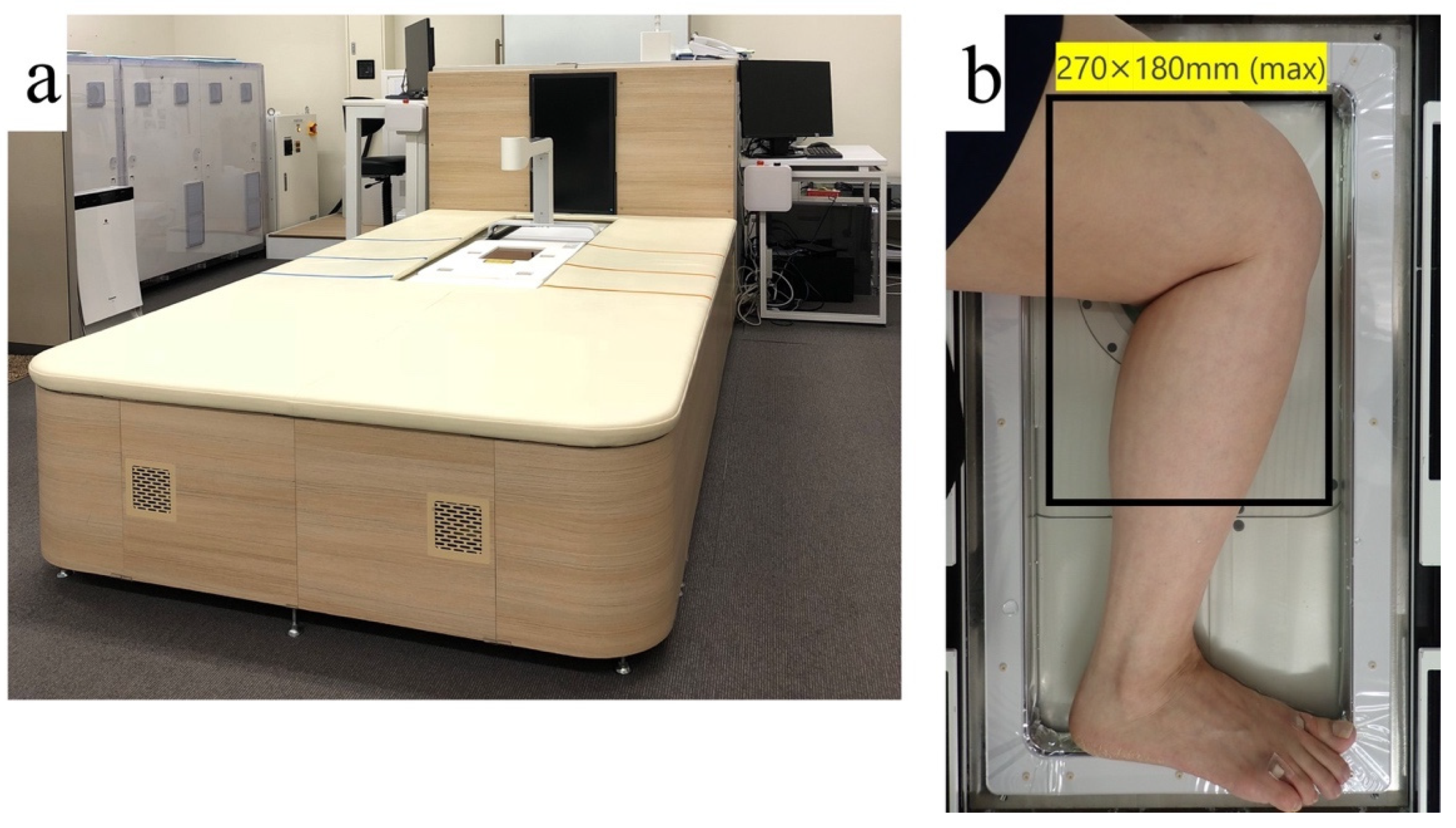
2.1. Principles of Photoacoustic Imaging
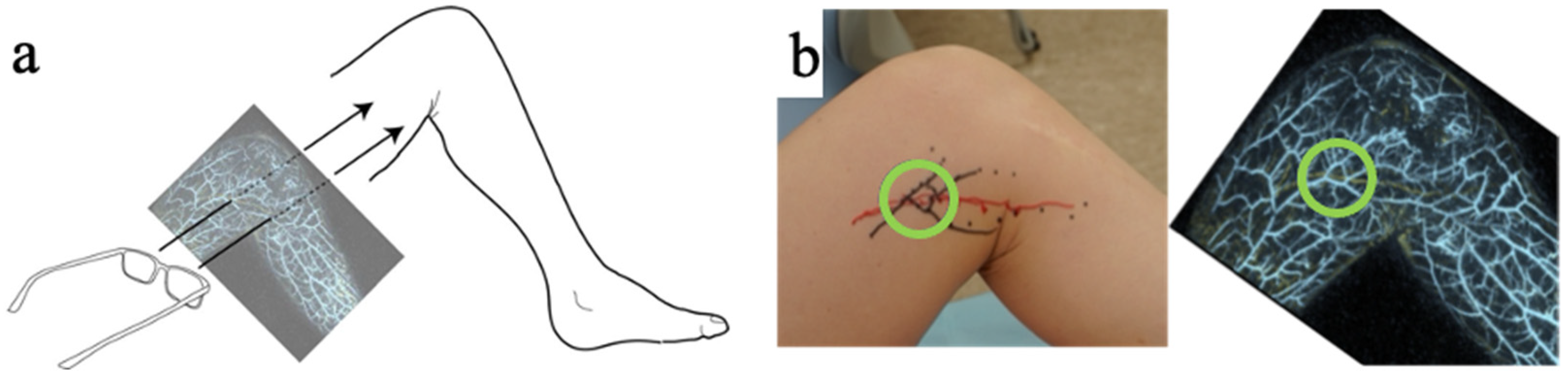
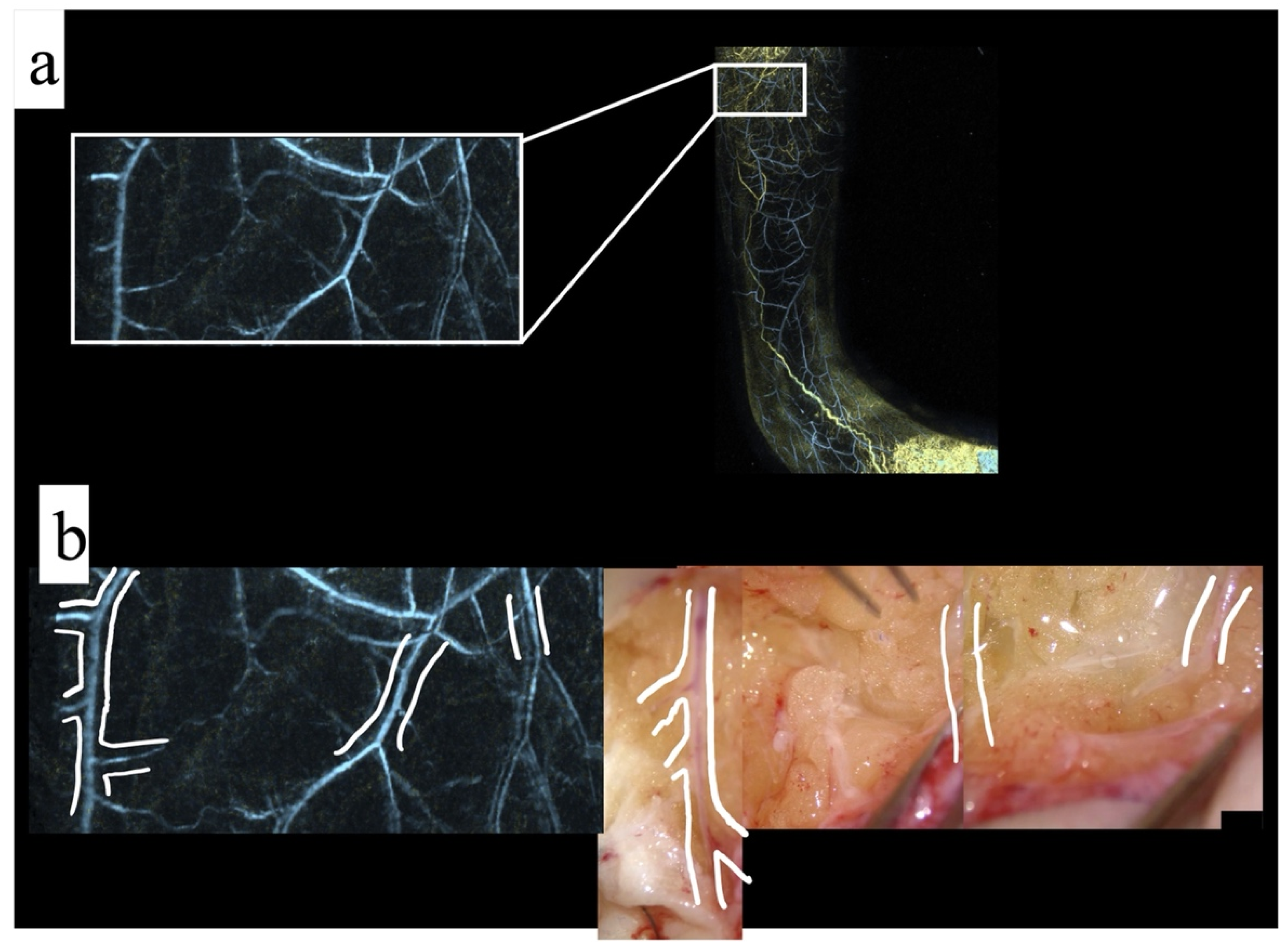
2.1.1. Method: Photoacoustic Imaging Match with Surgical Findings
2.1.2. Method: Transfer of Photoacoustic Image to the Actual Surgical Field
3. Results
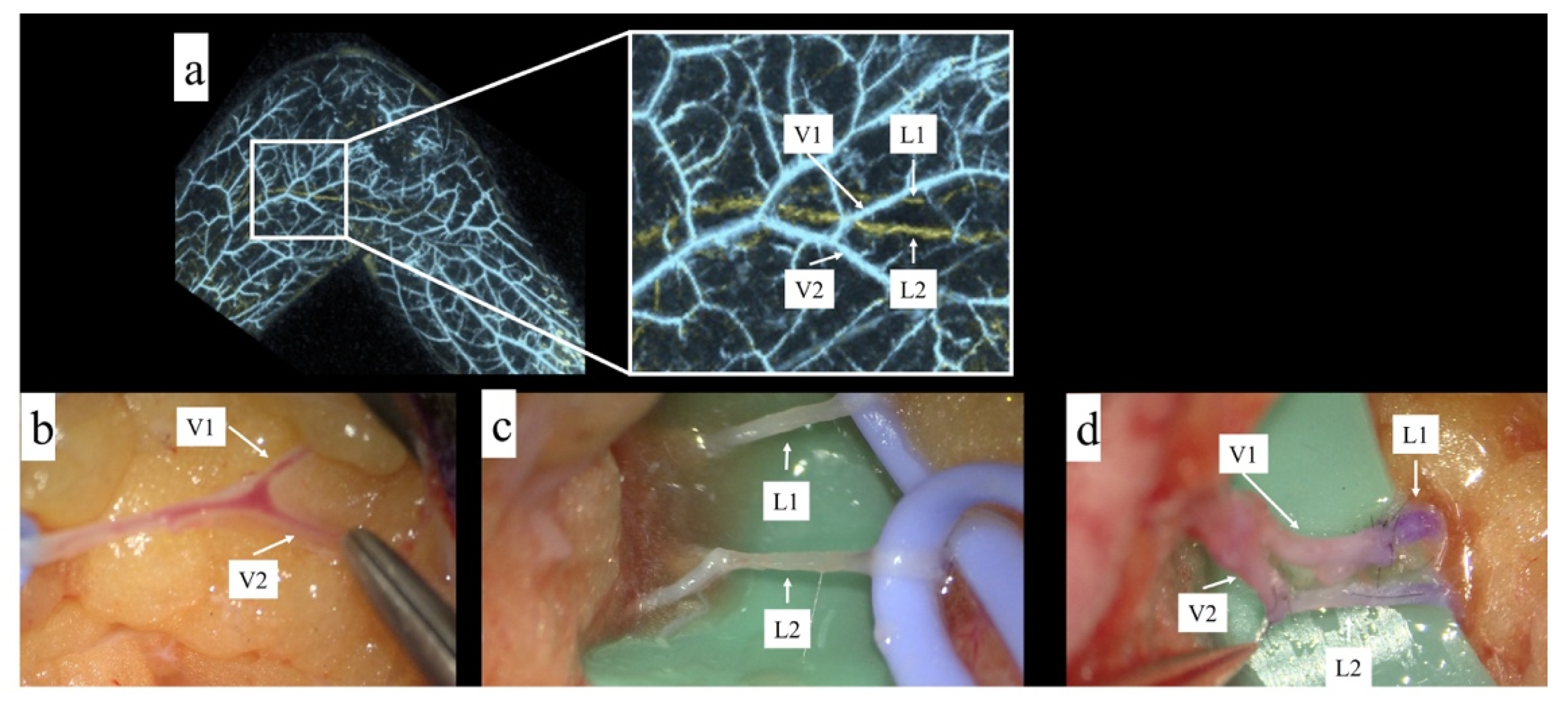
3.1. Result: Photoacoustic Imaging Match with Surgical Findings
3.2. Result: Transfer the Photoacoustic Image to the Actual Surgical Field
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Koshima, I.; Inagawa, K.; Urushibara, K.; Moriguchi, T. Supermicrosurgical Lymphaticovenular Anastomosis for the Treatment of Lymphedema in the Upper Extremities. J. Reconstr. Microsurg. 2000, 16, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Koshima, I.; Nanba, Y.; Tsutsui, T.; Takahashi, Y.; Itoh, S. Long-Term Follow-Up After Lymphaticovenular Anastomosis for Lymphedema in the Leg. J. Reconstr. Microsurg. 2003, 19, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.W. Lymphaticovenular Bypass for Lymphedema Management in Breast Cancer Patients: A Prospective Study. Plast. Reconstr. Surg. 2010, 126, 752–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaciulyte, J.; Garutti, L.; Spadoni, D.; Velazquez-Mujica, J.; Losco, L.; Ciudad, P.; Marcasciano, M.; Torto, F.L.; Casella, D.; Ribuffo, D.; et al. Genital Lymphedema and How to Deal with It: Pearls and Pitfalls from over 38 Years of Experience with Unusual Lymphatic System Impairment. Medicina 2021, 57, 1175. [Google Scholar] [CrossRef] [PubMed]
- Ciudad, P.; Sabbagh, M.D.; Agko, M.; Huang, T.C.; Manrique, O.J.; Román, C.; Reynaga, C.; Delgado, R.; Maruccia, M.; Chen, H.-C. Surgical Management of Lower Extremity Lymphedema: A Comprehensive Review. Indian J. Plast. Surg. 2019, 52, 81–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forte, A.J.; Sisti, A.; Huayllani, M.T.; Boczar, D.; Cinotto, G.; Ciudad, P.; Manrique, O.J.; Lu, X.; McLaughlin, S. Lymphaticovenular anastomosis for breast cancer-related upper extremity lymphedema: A literature review. Gland. Surg. 2020, 9, 539–544. [Google Scholar] [CrossRef]
- Mihara, M.; Hara, H.; Tange, S.; Zhou, H.P.; Kawahara, M.; Shimizu, Y.; Murai, N. Multisite Lymphaticovenular Bypass Using Supermicrosurgery Technique for Lymphedema Management in Lower Lymphedema Cases. Plast. Reconstr. Surg. 2016, 138, 262–272. [Google Scholar] [CrossRef] [PubMed]
- Maegawa, J.; Mikami, T.; Yamamoto, Y.; Satake, T.; Kobayashi, S. Types of Lymphoscintigraphy and Indications for Lymphaticovenous Anastomosis. Microsurgery 2010, 30, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Unno, N.; Inuzuka, K.; Suzuki, M.; Yamamoto, N.; Sagara, D.; Nishiyama, M.; Konno, H. Preliminary experience with a novel fluorescence lymphography using indocyanine green in patients with secondary lymphedema. J. Vasc. Surg. 2007, 45, 1016–1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T.; Narushima, M.; Doi, K.; Oshima, A.; Ogata, F.; Mihara, M.; Koshima, I.; Mundinger, G.S. Characteristic Indocyanine Green Lymphography Findings in Lower Extremity Lymphedema: The Generation of a Novel Lymphedema Severity Staging System Using Dermal Backflow Patterns. Plast. Reconstr. Surg. 2011, 127, 1979–1986. [Google Scholar] [CrossRef] [PubMed]
- Mihara, M.; Hara, H.; Kawakami, Y. Ultrasonography for Classifying Lymphatic Sclerosis Types and Deciding Optimal Sites for Lymphatic-Venous Anastomosis in Patients with Lymphoedema. J. Plast. Reconstr. Aesthet. Surg. 2018, 71, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, A.; Hayashi, N.; Yoshimatsu, H.; Yamamoto, T. Effective and efficient lymphaticovenular anastomosis using preoperative ultrasound detection technique of lymphatic vessels in lower extremity lymphedema. J. Surg. Oncol. 2018, 117, 290–298. [Google Scholar] [CrossRef]
- Yasunaga, Y.; Nakajima, Y.; Mimura, S.; Yuzuriha, S.; Kondoh, S. Magnetic resonance lymphography as three-dimensional navigation for lymphaticovenular anastomosis in patients with leg lymphedema. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 1253–1260. [Google Scholar] [CrossRef]
- Kajita, H.; Kishi, K. High-Resolution Imaging of Lymphatic Vessels with Photoacoustic Lymphangiography. Radiology 2019, 292, 35. [Google Scholar] [CrossRef]
- Suzuki, Y.; Kajita, H.; Konishi, N.; Oh, A.; Urano, M.; Watanabe, S.; Asao, Y.; Imanishi, N.; Tsuji, T.; Jinzaki, M.; et al. Subcutaneous Lymphatic Vessels in the Lower Extremities: Comparison between Photoacoustic Lymphangiography and Near-Infrared Fluorescence Lymphangiography. Radiology 2020, 295, 469–474. [Google Scholar] [CrossRef]
- Suzuki, Y.; Kajita, H.; Oh, A.; Urano, M.; Watanabe, S.; Sakuma, H.; Imanishi, N.; Tsuji, T.; Jinzaki, M.; Kishi, K. Photoacoustic Lymphangiography Exhibits Advantages over Near-Infrared Fluorescence Lymphangiography as a Diagnostic Tool in Patients with Lymphedema. J. Vasc. Surg. Venous Lymph. Disord. in press. [CrossRef]
- Yoshimatsu, H.; Yamamoto, T.; Narushima, M.; Iida, T.; Koshima, I. Perforator-bridged lymphaticovenular anastomosis. J. Plast. Reconstr. Aesthetic Surg. 2012, 65, 1438–1439. [Google Scholar] [CrossRef] [PubMed]
- Vles, M.; Terng, N.; Zijlstra, K.; Mureau, M.; Corten, E. Virtual and augmented reality for preoperative planning in plastic surgical procedures: A systematic review. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1951–1959. [Google Scholar] [CrossRef] [PubMed]
- Pereira, N.; Kufeke, M.; Parada, L.; Troncoso, E.; Bahamondes, J.; Sanchez, L.; Roa, R. Augmented Reality Microsurgical Planning with a Smartphone (ARM-PS): A dissection route map in your pocket. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Nishimoto, S.; Tonooka, M.; Fujita, K.; Sotsuka, Y.; Fujiwara, T.; Kawai, K.; Kakibuchi, M. An augmented reality system in lymphatico-venous anastomosis surgery. J. Surg. Case Rep. 2016, 2016, rjw047. [Google Scholar] [CrossRef] [PubMed]
- Tsuge, I.; Saito, S.; Yamamoto, G.; Sekiguchi, H.; Yoshikawa, A.; Matsumoto, Y.; Suzuki, S.; Toi, M. Preoperative vascular mapping for anterolateral thigh flap surgeries: A clinical trial of photoacoustic tomography imaging. Microsurgery 2020, 40, 324–330. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, Y.; Kajita, H.; Watanabe, S.; Otaki, M.; Okabe, K.; Sakuma, H.; Takatsume, Y.; Imanishi, N.; Aiso, S.; Kishi, K. Surgical Applications of Lymphatic Vessel Visualization Using Photoacoustic Imaging and Augmented Reality. J. Clin. Med. 2022, 11, 194. https://doi.org/10.3390/jcm11010194
Suzuki Y, Kajita H, Watanabe S, Otaki M, Okabe K, Sakuma H, Takatsume Y, Imanishi N, Aiso S, Kishi K. Surgical Applications of Lymphatic Vessel Visualization Using Photoacoustic Imaging and Augmented Reality. Journal of Clinical Medicine. 2022; 11(1):194. https://doi.org/10.3390/jcm11010194
Chicago/Turabian StyleSuzuki, Yushi, Hiroki Kajita, Shiho Watanabe, Marika Otaki, Keisuke Okabe, Hisashi Sakuma, Yoshifumi Takatsume, Nobuaki Imanishi, Sadakazu Aiso, and Kazuo Kishi. 2022. "Surgical Applications of Lymphatic Vessel Visualization Using Photoacoustic Imaging and Augmented Reality" Journal of Clinical Medicine 11, no. 1: 194. https://doi.org/10.3390/jcm11010194