
Speckle-Tracking Global Longitudinal and Regional Strain Analysis in Neonates with Coarctation of Aorta: A Case-Control Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
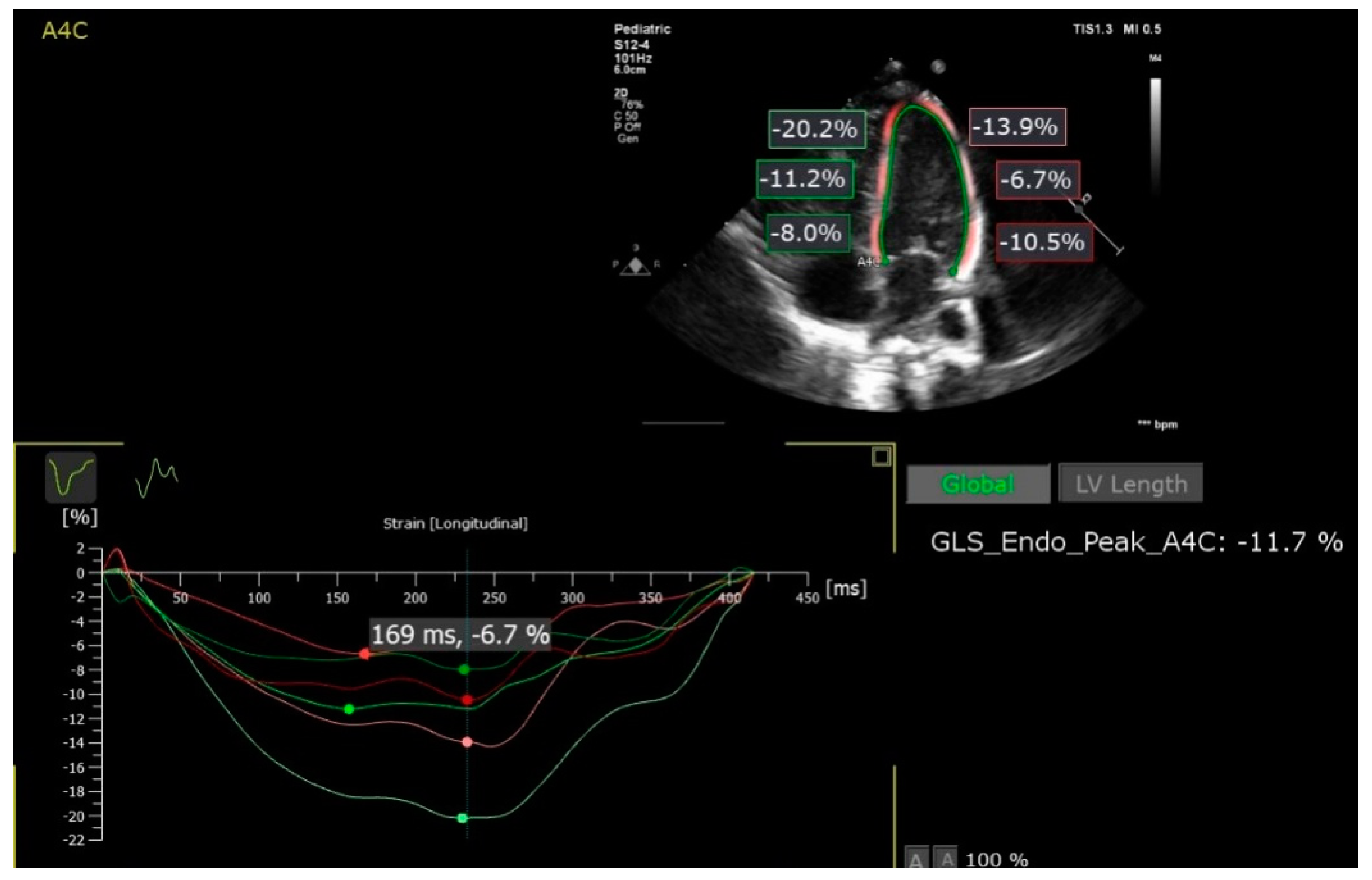
2.1. Speckle-Tracking Analysis
2.2. Ethics
2.3. Statistical Analysis
3. Results
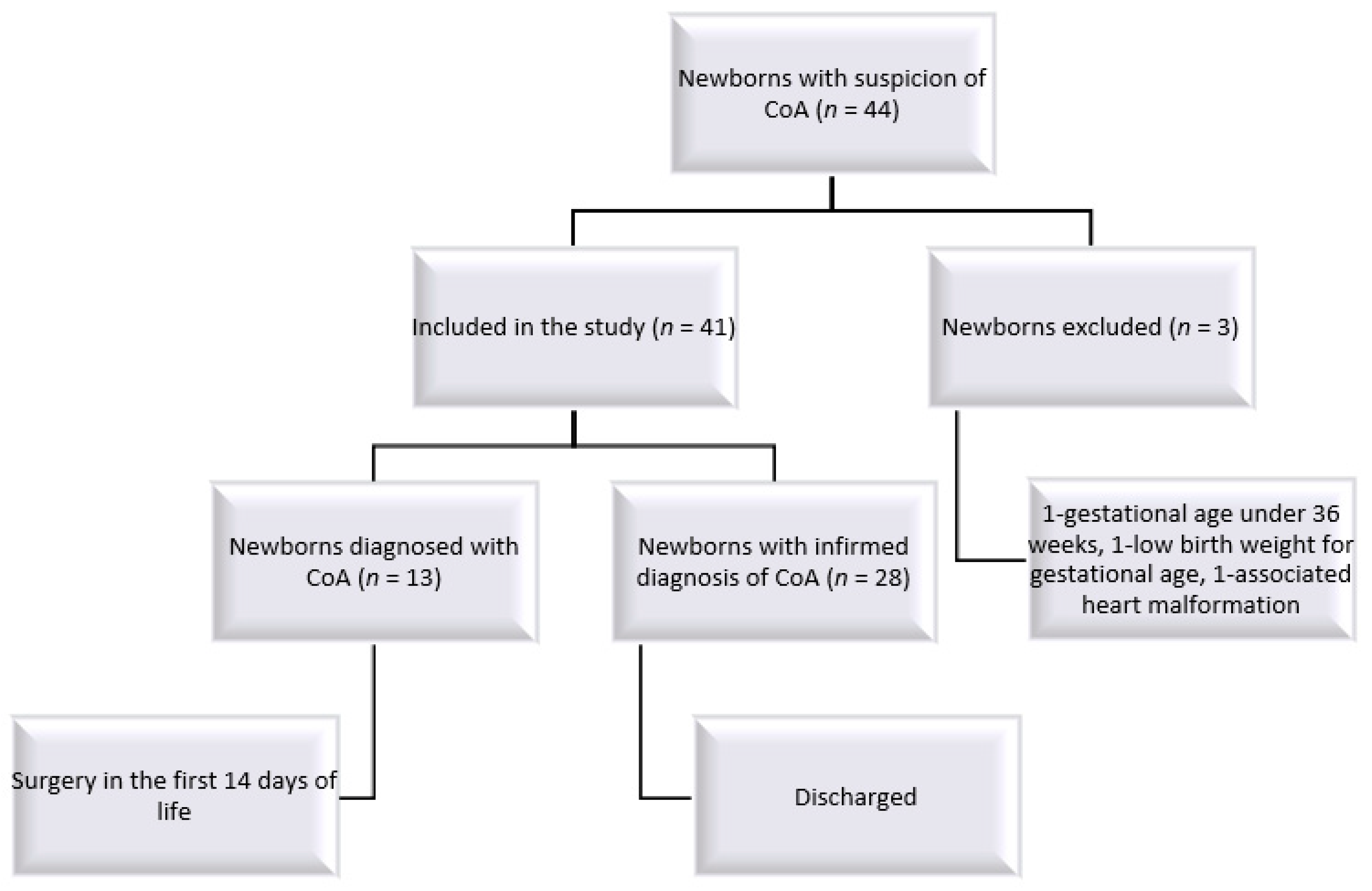
3.1. Description of the Studied Groups
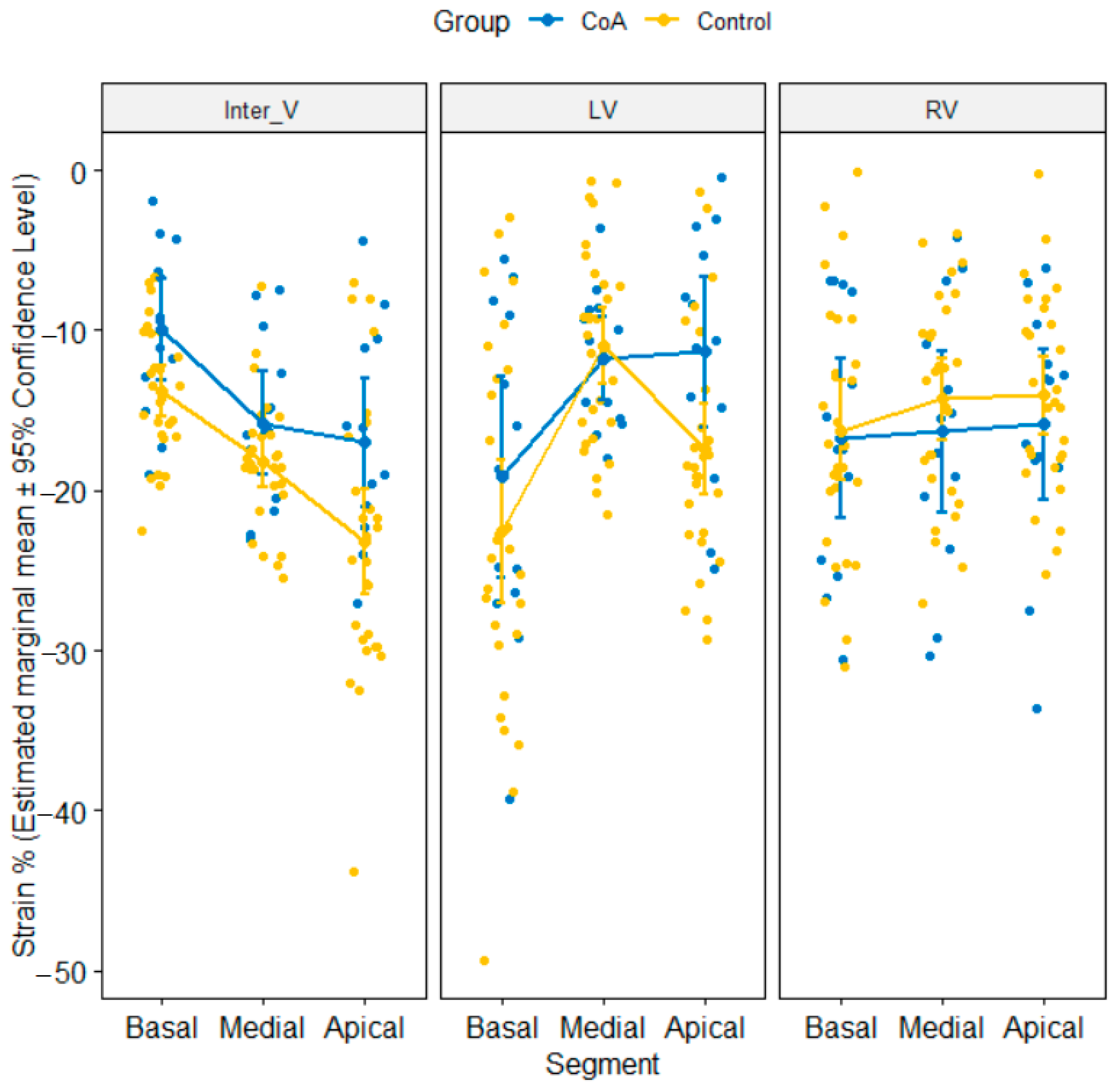
3.2. Comparison of Segmental Strain Values between CoA and Control Groups
3.3. Comparison of Longitudinal Strain Values between CoA and Control Groups
3.4. ROC (Receiver-Operating Characteristic Curve) Analysis
3.5. Reliability Analysis of Speckle-Tracking Parameters in the Whole Sample (n = 41)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenthal, E. Coarctation of the aorta from fetus to adult: Curable condition or life long disease process? Heart 2005, 91, 1495–1502. [Google Scholar] [CrossRef] [Green Version]
- Lannering, K.; Bartos, M.; Mellander, M. Late Diagnosis of Coarctation Despite Prenatal Ultrasound and Postnatal Pulse Oximetry. Pediatrics 2015, 136, e406–e412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, O.; Burch, M.; Manning, N.; Sleeman, K.; Gould, S.; Archer, N. Prenatal diagnosis of coarctation of the aorta improves survival and reduces morbididity. Heart 2002, 87, 67–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez-Montes, E.; Herraiz, I.; Mendoza, A.; Escribano, D.; Galindo, A. Prediction of coarctation of the aorta in the second half of pregnancy. Ultrasound. Obstet. Gynecol. 2013, 41, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Matsui, H.; Mellander, M.; Roughton, M.; Jicinska, H.; Gardiner, H.M. Morphological and physiological predictors of fetal aortic coarcation. Circulation 2008, 118, 1793–1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slodki, M.; Rychik, J.; Moszura, T.; Janiak, K.; Respondek-Liberska, M. Measurment of great vessels in the mediastinum could help distinguish. Ultrasound. Med. 2009, 28, 1313–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anuwutnavin, S.; Satou, G.; Chang, R.-K.; DeVore, G.R. Prenatal sonographic predictors of neonatal coarcation of the aorta. J. Ultrasound. Med. 2016, 35, 2353–2364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, T.P.; Dimaano, V.L.; Liang, H.Y. Role of tissue Doppler and strain echocardiography in current clinical practice. Circulation 2007, 116, 2597–2609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nestaas, E.; Stoylen, A.; Sandvik, L.; Brunvand, L.; Fugelseth, D. Feasibility and reliability of strainand strain rate measuremnent in neonates by optimizing the analysis parameters settings. Ultrasound. Med. Biol. 2007, 33, 270–278. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Jain, A.; El-Khuffash, A.F.; Kuipers, B.C.; Mohamed, A.; Connelly, K.A.; McNamara, P.J.; Jankov, R.P.; Mertens, L. Left ventricular function in healthy term neonates during the transitional period. J. Pediatr. 2017, 182, 197–203. [Google Scholar] [CrossRef]
- Schubert, U.; Matthias, M.; Norman, M.; Abdul-Khaliq, H. Transition from fetal to neonatal life: Change in cardiac function assessed by speckle-tracking echocardiography. Earlhumdev 2013, 89, 803–808. [Google Scholar] [CrossRef] [Green Version]
- Pena Jl da Silva, M.G.; AlvesJrJm Salemi, V.M.; Mady, C.; Baltabaeva, A.; Sutherland, G.R. Sequential changes of longitudinal and radial myocardial deformation indices in the healthy neonate heart. J. Am. Soc. Echocardiogr. 2010, 23, 294–300. [Google Scholar] [CrossRef]
- Petitjean, C.; Rougon, N.; Cluzel, P. Assessment of myocardial function: A review of quantification methods and results using tagged MRI. J. Cardiovasc. Magn. Reson. 2005, 7, 501–516. [Google Scholar] [CrossRef] [PubMed]
- Levy, P.T.; Holland, M.R.; Sekarski, T.J.; Hamvas, A.; Singh, G.K. Feasibility and reproducibility of systolic right ventricular strain measurement by speckle –tracking echocardiography in premature infants. J. Am. Soc. Echocardiogr. 2013, 26, 1201–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sequela, P.E.; Thomas-Chabaneix, J.; Jalal, Z.; Rouertie, F.; Faydi, L.; Mouton, J.-B.; Dumas-de-la-Roque, E.; Tandonnet, O.; Pillois, X.; Thambo, J.-B.; et al. Toward the integration of global longitudinal strain analysis in the assessment of neonatal aortic coarctation? A preliminary study. Arch. Cardiovasc. Dis. 2018, 111, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Morton, S.U.; Brodsky, D. Fetal physiology and the transition to extrauterine life. Clin. Perinatol. 2016, 43, 395–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, Y.; Weidong, R.; Xiao, Y.; Qiao, W.; Song, G.; Sun, L. Changes in the interventricuarseptal curvature in healthy full-term neonates during the first 14 days of life. J. Ultrasound. Med. 2020, 39, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Arya, B.; Bhat, A.; Vernon, M.; Conwell, J.; Lewin, M. Utility of novel fetal echocardiographic morphometric measures of the aortic arch in the diagnosis of neonatal coarcation of the aorta. Prenat. Diagn. 2016, 36, 127–134, Erratum in: Prenat. Diagn. 2018, 38, 798. [Google Scholar] [CrossRef] [PubMed]
- Durand, I.; Deverriere, G.; Thill, C.; Lety, A.S.; Parrod, C.; David, N.; Barre, E.; Hazelzet, T. Prenatal detection of coarctation of the aorta in a non-selected population: A prospective analysis of 10 years of experience. Pediatr. Cardiol. 2015, 36, 1248–1254. [Google Scholar] [CrossRef] [PubMed]
- Familiari, A.; Morlando, M.; Khalil, A.; Sonesson, S.A.; Scala, C.; Rizzo, G.; Del Sordo, G.; Vassallo, C.; Flacco, M.E.; Manzoli, L.; et al. Risk Fact Factors for Coarcation of the Aorta on Prenatal Ultrasound. Circulation 2017, 135, 772–785. [Google Scholar] [CrossRef] [PubMed]
- Meister, M.; Axt-Fliedner, R.; Grapner, O.; Kuhn, V.; Wolter, A.; Gotte, M.; Enzensberger, C. Atrial and ventricular deformation analysis in normal fetal hearts using two-dimensional speckle tracking echocardiography. Fetal. Diagn. Ther. 2020, 47, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Germanakis, I.; Matsiu, H.; Gardiner, H.M. Myocardial strain abnormalities in fetal congenital heart disease assessed by speckle tracking echocardiography. Fetal. Diagn. Ther. 2021, 32, 123–130. [Google Scholar] [CrossRef]
- Simpson, J. Speckle tracking for the assessment of fetal cardiac function. Ultrasound. Obstet. Ginecol. 2011, 37, 133–134, Erratum in: Ultrasound. Obstet. Gynecol. 2011, 37, 500. [Google Scholar] [CrossRef] [PubMed]
- Miranda, J.O.; Hunter, L.; Tibby, S.; Sharland, G.; Miller, O.; Simpson, J.M. Myocardial deformation in fetus with coarctation of the aorta: A case-control study. Ultrasound. Obstet. Gynecol. 2017, 49, 623–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeVore, G.R.; Haxel, C.; Satou, G.; Sklansky, M.; Pelka, M.J.; Jone, P.N.; Cuneo, B.F. Improved detection of coarcation of the aorta using speckle-tracking analysis of fetal heart on last examination prior to delivery. Ultrasound. Obstet. Gynecol. 2021, 57, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Vigneswaran, T.V.; Bellsham-Revell, H.R.; Chubb, H.; Simpson, J.M. Early postnatal echocardiography in neonates with a prenatal suspicion of coarcation of the aorta. Pediatr. Cardiol. 2020, 41, 772–778. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Measured Variable | Abbreviation | Description |
|---|---|---|
| Left ventricle lateral wall basal | LV Basal | Strain measured on the basal portion of the left ventricle lateral wall |
| Left ventricle lateral wall medial | LV Medial | Strain measured on the medial portion of the left ventricle lateral wall |
| Left ventricle lateral wall apical | LV Apical | Strain measured on the apical portion of the left ventricle lateral wall |
| Inter-ventricular septum basal | Inter V Basal | Strain measured on the basal portion of the inter-ventricular septum |
| Inter-ventricular septum medial | Inter V Medial | Strain measured on the medial portion of the inter-ventricular septum |
| Inter-ventricular septum apical | Inter V Apical | Strain measured on the apical portion of the inter-ventricular septum |
| Left ventricle peak global strain | LV pGLS | Peak Global longitudinal strain of the left ventricle |
| Right ventricle lateral wall basal | RV Basal | Strain measured on the basal portion of the right ventricle lateral wall |
| Right ventricle lateral wall medial | RV Medial | Strain measured on the medial portion of the right ventricle lateral wall |
| Right ventricle lateral wall apical | RV Apical | Strain measured on the apical portion of the right ventricle lateral wall |
| Right ventricle free wall | RV free wall | Longitudinal strain of the right ventricle free wall |
| Right ventricle global4-chamber longitudinal strain | RV4C | Global longitudinal strain of the right ventricle from 4-chamber view |
| Control Group (n1 = 28) | CoA Group (n2 = 13) | p-Value | |
|---|---|---|---|
| Gestational Age (weeks), mean ± SD | 39.18 ± 0.98 | 39.77 ± 0.83 | 0.056 |
| Age (days), median (Q1, Q3) | 2 (2.00, 3.25) | 1 (1.00, 6.00) | 0.362 |
| Sex (male), n (%) | 15 (53.57) | 7 (53.85) | 1.000 |
| Weight (g), mean ± SD | 3474 ± 257.85 | 3725 ± 145.01 | 0.0003 * |
| Systolic blood pressure, mean ± SD | 83.8 ± 2.6 | 83.8 ± 2.7 | 0.954 |
| Heart rate, mean ± SD | 135 ± 7.9 | 134.6 ± 8.2 | 0.743 |
| LV asynchronism, n (%) | 0.541 | ||
| Synchronism | 9 (32.14) | 4 (30.77) | |
| 1 asynchronous segments | 6 (21.43) | 5 (38.46) | |
| 2 asynchronous segments | 6 (21.43) | 3 (23.08) | |
| ≥3 asynchronous segments | 7 (25.00) | 1 (7.69) | |
| RV asynchronism, n (%) | 1.000 | ||
| Synchronism | 22 (78.57) | 10 (76.92) | |
| 1 asynchronous segment | 6 (21.43) | 3 (23.08) |
| Wall | Cardiac Segment | Group | Mean (SD) | p-Value | Adjusted pBH-Value |
|---|---|---|---|---|---|
| Inter V | Apical | CoA | −17.02 (6.70) | 0.018 | 0.093 |
| Control | −23.19 (8.54) | ||||
| Inter V | Basal | CoA | −9.93 (5.28) | 0.031 | 0.093 |
| Control | −13.81 (4.15) | ||||
| Inter V | Medial | CoA | −15.80 (5.32) | 0.157 | 0.353 |
| Control | −18.25 (4.08) | ||||
| LV | Apical | CoA | −11.34 (7.79) | 0.026 | 0.093 |
| Control | −17.46 (7.32) | ||||
| LV | Basal | CoA | −19.15 (10.4) | 0.355 | 0.639 |
| Control | −22.54 (11.5) | ||||
| LV | Medial | CoA | −11.77 (4.30) | 0.636 | 0.818 |
| Control | −10.97 (6.17) | ||||
| RV | Apical | CoA | −15.90 (7.74) | 0.808 | 0.850 |
| Control | −14.10 (6.22) | ||||
| RV | Basal | CoA | −16.79 (8.22) | 0.850 | 0.850 |
| Control | −16.26 (8.03) | ||||
| RV | Medial | CoA | −16.35 (8.27) | 0.441 | 0.662 |
| Control | −14.30 (6.48) |
| Wall | Segment | Rater 1 Mean (SD) | Rater 2 Mean (SD) | p-Value * | ICC [95% CI] | Bias [95% CI] |
|---|---|---|---|---|---|---|
| LV | Basal (%) | −21.47 (11.15) | −21.10 (9.95) | 0.725 | 0.80 [0.66, 0.89] | −0.37 [−2.47, 1.74] |
| Medial (%) | −11.22 (5.61) | −11.28 (6.72) | 0.943 | 0.65 [0.43, 0.79] | 0.06 [−1.58, 1.70] | |
| Apical (%) | −15.52 (7.92) | −15.24 (8.04) | 0.756 | 0.75 [0.57, 0.86] | −0.28 [−2.08, 1.52] | |
| RV | Basal (%) | −16.43 (7.99) | −17.32 (9.05) | 0.240 | 0.84 [0.73, 0.91] | 0.89 [−0.62,2.40] |
| Medial (%) | −14.95 (7.06) | −15.71 (7.18) | 0.138 | 0.90 [0.82, 0.94] | 0.76 [−0.26,1.78] | |
| Apical (%) | −14.29 (7.42) | −15.50 (7.15) | 0.038 | 0.91 [0.83, 0.95] | 0.86 [−0.07,1.80] | |
| Inter V | Basal (%) | −12.58 (4.83) | −12.41 (4.96) | 0.797 | 0.65 [0.43, 0.80] | −0.17 [−1.46, 1.13] |
| Medial (%) | −17.48 (4.59) | −18.05 (4.38) | 0.204 | 0.80 [0.65, 0.89] | 0.58 [−0.33, 1.48] | |
| Apical (%) | −21.23 (8.43) | −23.84 (8.94) | 0.002 | 0.83 [0.70, 0.90] | 2.61 [0.99, 4.22] | |
| LV | Global | −16.16 (4.15) | −16.56 (4.14) | 0.297 | 0.83 [0.70, 0.90] | 0.40 [−0.37, 1.18] |
| RV free wall | free wall (%) | −15.64 (7.18) | −16.50 (7.64) | 0.102 | 0.90 [0.82, 0.95] | 0.86 [−0.18, 1.89] |
| RV4C | 4C (%) | −13.66 (5.06) | −13.87 (5.31) | 0.574 | 0.90 [0.82, 0.94] | 0.21 [−0.53, 0.97] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gozar, L.; Mărginean, C.; Cerghit Paler, A.; Gabor-Miklosi, D.; Toma, D.; Iancu, M.; Togănel, R.; Făgărășan, A. Speckle-Tracking Global Longitudinal and Regional Strain Analysis in Neonates with Coarctation of Aorta: A Case-Control Study. J. Clin. Med. 2021, 10, 4579. https://doi.org/10.3390/jcm10194579
Gozar L, Mărginean C, Cerghit Paler A, Gabor-Miklosi D, Toma D, Iancu M, Togănel R, Făgărășan A. Speckle-Tracking Global Longitudinal and Regional Strain Analysis in Neonates with Coarctation of Aorta: A Case-Control Study. Journal of Clinical Medicine. 2021; 10(19):4579. https://doi.org/10.3390/jcm10194579
Chicago/Turabian StyleGozar, Liliana, Claudiu Mărginean, Andreea Cerghit Paler, Dorottya Gabor-Miklosi, Daniela Toma, Mihaela Iancu, Rodica Togănel, and Amalia Făgărășan. 2021. "Speckle-Tracking Global Longitudinal and Regional Strain Analysis in Neonates with Coarctation of Aorta: A Case-Control Study" Journal of Clinical Medicine 10, no. 19: 4579. https://doi.org/10.3390/jcm10194579