
Prospective Evaluation of a Standardized Screening for Atrial Fibrillation after Ablation of Cavotricuspid Isthmus Dependent Atrial Flutter

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
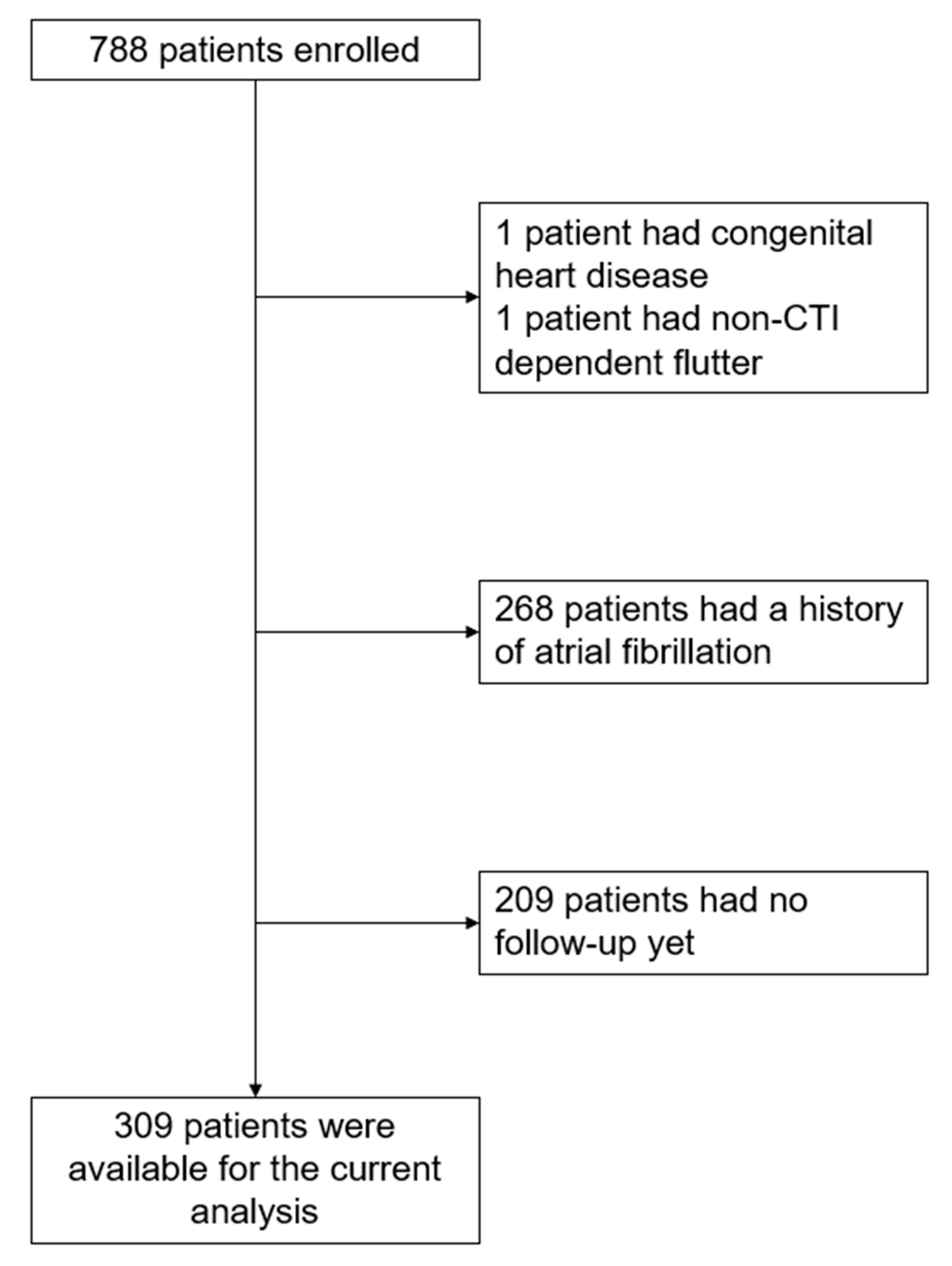
2.1. Patient Population
2.2. Assessment of Study Variables
2.3. Ablation Procedure
2.4. Study Outcomes
2.5. Statistical Analysis
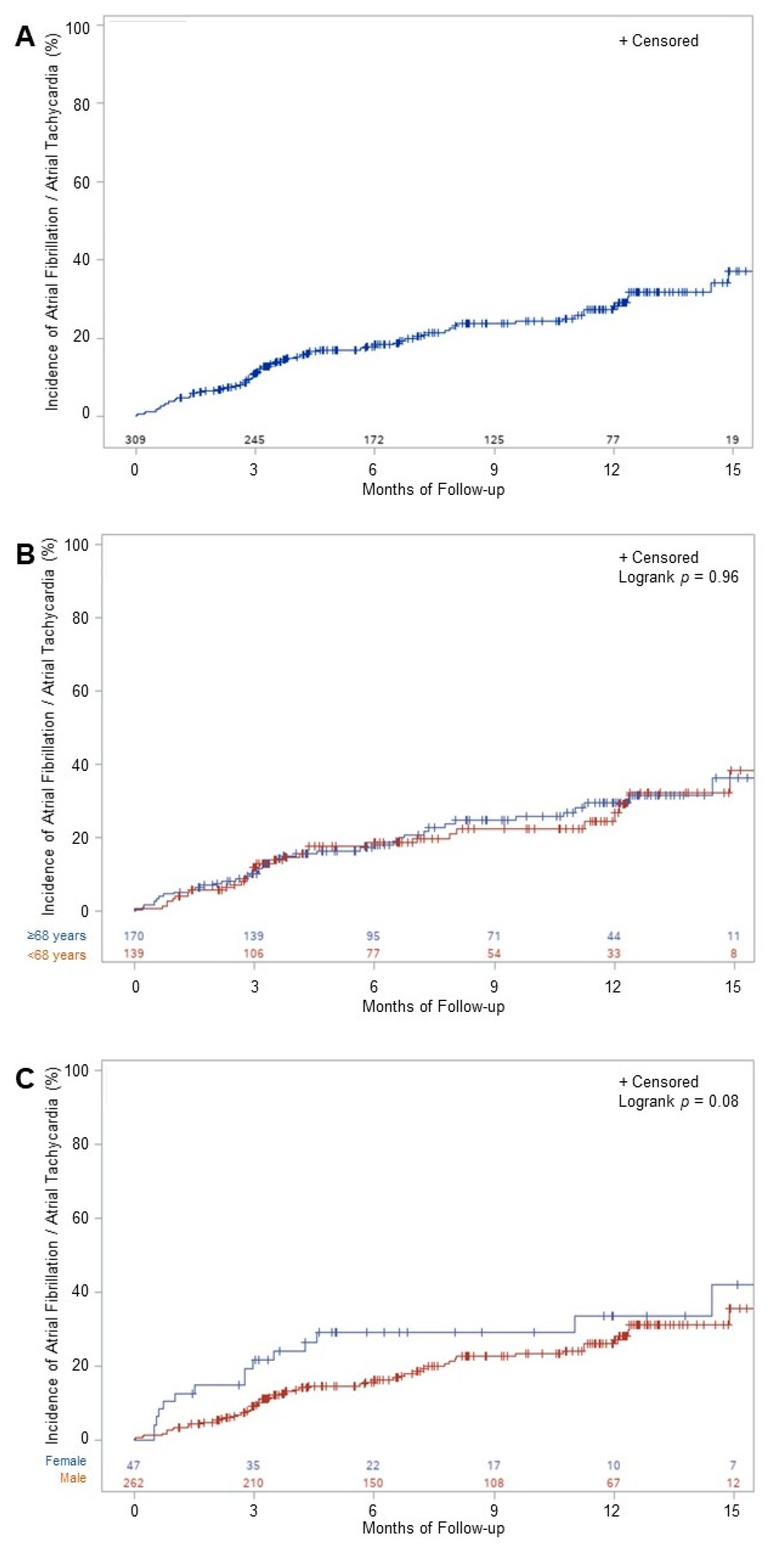
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maskoun, W.; Pino, M.I.; Ayoub, K.; Llanos, O.L.; Almomani, A.; Nairooz, R.; Hakeem, A.; Miller, J. Incidence of Atrial Fibrillation After Atrial Flutter Ablation. JACC Clin. Electrophysiol. 2016, 2, 682–690. [Google Scholar] [CrossRef]
- Celikyurt, U.; Knecht, S.; Kuehne, M.; Reichlin, T.; Muehl, A.; Spies, F.; Osswald, S.; Sticherling, C. Incidence of New-Onset Atrial Fibrillation after Cavotricuspid Isthmus Ablation for Atrial Flutter. Europace 2017, 19, 1776–1780. [Google Scholar] [CrossRef] [PubMed]
- Waldo, A.L.; Feld, G.K. Inter-Relationships of Atrial Fibrillation and Atrial Flutter Mechanisms and Clinical Implications. J. Am. Coll. Cardiol. 2008, 51, 779–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldo, A.L.; Cooper, T.B. Spontaneous Onset of Type I Atrial Flutter in Patients. J. Am. Coll. Cardiol. 1996, 28, 707–712. [Google Scholar] [CrossRef] [Green Version]
- Watson, R.M.; Josephson, M.E. Atrial Flutter. I. Electrophysiologic Substrates and Modes of Initiation and Termination. Am. J. Cardiol. 1980, 45, 732–741. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association of Cardio-Thoracic Surgery (EACTS)The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed with the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef]
- Tada, H.; Oral, H.; Sticherling, C.; Chough, S.P.; Baker, R.L.; Wasmer, K.; Pelosi, F.; Knight, B.P.; Strickberger, S.A.; Morady, F. Double Potentials along the Ablation Line as a Guide to Radiofrequency Ablation of Typical Atrial Flutter. J. Am. Coll. Cardiol. 2001, 38, 750–755. [Google Scholar] [CrossRef] [Green Version]
- Lip, G.Y.H.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J.G.M. Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in Atrial Fibrillation Using a Novel Risk Factor-Based Approach: The Euro Heart Survey on Atrial Fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Mittal, S.; Pokushalov, E.; Romanov, A.; Ferrara, M.; Arshad, A.; Musat, D.; Preminger, M.; Sichrovsky, T.; Steinberg, J.S. Long-Term ECG Monitoring Using an Implantable Loop Recorder for the Detection of Atrial Fibrillation after Cavotricuspid Isthmus Ablation in Patients with Atrial Flutter. Heart Rhythm 2013, 10, 1598–1604. [Google Scholar] [CrossRef]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.V.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [Green Version]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertaglia, E.; Zoppo, F.; Bonso, A.; Proclemer, A.; Verlato, R.; Corò, L.; Mantovan, R.; D’Este, D.; Zerbo, F.; Pascotto, P.; et al. Long Term Follow up of Radiofrequency Catheter Ablation of Atrial Flutter: Clinical Course and Predictors of Atrial Fibrillation Occurrence. Heart Br. Card. Soc. 2004, 90, 59–63. [Google Scholar] [CrossRef] [Green Version]
- Zambito, P.E.; Talreja, A.; Gundewar, S.; Fisher, J.; Ferrick, K.; Gross, J.; Kim, S.; Palma, E.C. Severe Left Ventricular Systolic Dysfunction Increases Atrial Fibrillation After Ablation of Atrial Flutter. Pacing Clin. Electrophysiol. 2005, 28, 1055–1059. [Google Scholar] [CrossRef] [PubMed]
- Paydak, H.; Kall, J.G.; Burke, M.C.; Rubenstein, D.; Kopp, D.E.; Verdino, R.J.; Wilber, D.J. Atrial Fibrillation after Radiofrequency Ablation of Type I Atrial Flutter: Time to Onset, Determinants, and Clinical Course. Circulation 1998, 98, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.; Bai, R.; Deng, W.; Gao, C.; Zhang, J.; Wang, X.; Wang, S.; Fu, H.; Zhao, Y.; Zhang, J.; et al. HATCH Score in the Prediction of New-Onset Atrial Fibrillation after Catheter Ablation of Typical Atrial Flutter. Heart Rhythm 2015, 12, 1483–1489. [Google Scholar] [CrossRef]
- Chinitz, J.S.; Gerstenfeld, E.P.; Marchlinski, F.E.; Callans, D.J. Atrial Fibrillation Is Common after Ablation of Isolated Atrial Flutter during Long-Term Follow-Up. Heart Rhythm 2007, 4, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Dewland, T.A.; Vittinghoff, E.; Mandyam, M.C.; Heckbert, S.R.; Siscovick, D.S.; Stein, P.K.; Psaty, B.M.; Sotoodehnia, N.; Gottdiener, J.S.; Marcus, G.M. Atrial Ectopy as a Predictor of Incident Atrial Fibrillation: A Cohort Study. Ann. Intern. Med. 2013, 159, 721–728. [Google Scholar] [CrossRef] [Green Version]
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomström-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.-P.; et al. 2019 ESC Guidelines for the Management of Patients with Supraventricular TachycardiaThe Task Force for the Management of Patients with Supraventricular Tachycardia of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 655–720. [Google Scholar] [CrossRef] [Green Version]
- Vadmann, H.; Nielsen, P.B.; Hjortshøj, S.P.; Riahi, S.; Rasmussen, L.H.; Lip, G.Y.H.; Larsen, T.B. Atrial Flutter and Thromboembolic Risk: A Systematic Review. Heart Br. Card. Soc. 2015, 101, 1446–1455. [Google Scholar] [CrossRef]
- Chen, Y.-L.; Lin, Y.-S.; Wang, H.-T.; Liu, W.-H.; Chen, H.-C.; Chen, M.-C. Clinical Outcomes of Solitary Atrial Flutter Patients Using Anticoagulation Therapy: A National Cohort Study. Europace 2019, 21, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Giehm-Reese, M.; Johansen, M.N.; Kronborg, M.B.; Jensen, H.K.; Gerdes, C.; Kristensen, J.; Johannessen, A.; Jacobsen, P.K.; Djurhuus, M.S.; Hansen, P.S.; et al. Discontinuation of Oral Anticoagulation and Risk of Stroke and Death after Ablation for Typical Atrial Flutter: A Nation-Wide Danish Cohort Study. Int. J. Cardiol. 2021, 333, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.; Natale, A.; Mohanty, P.; Biase, L.D.; Trivedi, C.; Santangeli, P.; Bai, R.; Burkhardt, J.D.; Gallinghouse, G.J.; Horton, R.; et al. Pulmonary Vein Isolation to Reduce Future Risk of Atrial Fibrillation in Patients Undergoing Typical Flutter Ablation: Results from a Randomized Pilot Study (REDUCE AF). J. Cardiovasc. Electrophysiol. 2015, 26, 819–825. [Google Scholar] [CrossRef]
- Navarrete, A.; Conte, F.; Moran, M.; Ali, I.; Milikan, N. Ablation of Atrial Fibrillation at the Time of Cavotricuspid Isthmus Ablation in Patients With Atrial Flutter Without Documented Atrial Fibrillation Derives a Better Long-Term Benefit. J. Cardiovasc. Electrophysiol. 2011, 22, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, J.S.; Romanov, A.; Musat, D.; Preminger, M.; Bayramova, S.; Artyomenko, S.; Shabanov, V.; Losik, D.; Karaskov, A.; Shaw, R.E.; et al. Prophylactic Pulmonary Vein Isolation during Isthmus Ablation for Atrial Flutter: The PReVENT AF Study I. Heart Rhythm 2014, 11, 1567–1572. [Google Scholar] [CrossRef]
- Ding, W.Y.; Williams, E.; Das, M.; Tovmassian, L.; Tayebjee, M.; Haywood, G.; Martin, C.; Rajappan, K.; Bates, M.; Temple, I.P.; et al. Cryoballoon Pulmonary Vein Isolation as First Line Treatment for Typical Atrial Flutter (CRAFT): Study Protocol for a Randomised Controlled Trial. J. Interv. Card. Electrophysiol. 2020, 60, 427–432. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall n = 309 | |
|---|---|
| Sex (female), n | 47 (15.2) |
| Age, years | 67.9 (10.5) |
| BMI, kg/m2 | 27.7 (5.3) |
| CHA2DS2-VASc score, points | 2.4 (1.5) |
| EHRA score, points | 2.2 (0.7) |
| Prior heart failure, n | 57 (18.5) |
| Tachycardia-induced cardiomyopathy, n | 22 (7.1) |
| Hypertension, n | 193 (62.5) |
| Diabetes, n | 52 (16.8) |
| Coronary heart disease, n | 52 (16.8) |
| LVEF, % | 50.7 (13.5) |
| Left atrial volume, ml | 39.5 (17.8) |
| Treatment, n | |
| Oral anticoagulation, n | 279 (90.3) |
| AAD | 38 (12.3) |
| Beta-blocker | 196 (63.4) |
| RAAS-inhibitor | 114 (36.9) |
| Predictor | Univariate | |
|---|---|---|
| HR (95% CI) | p-Value | |
| Sex, female | 1.63 (0.93; 2.84) | 0.09 |
| Age, per 1 year | 1.00 (0.98; 1.02) | 0.98 |
| BMI, per unit | 0.98 (0.93; 1.03) | 0.17 |
| CHA2DS2-VASc, per point | 1.03 (0.88; 1.20) | 0.72 |
| EHRA score, per point | 0.77 (0.55; 1.07) | 0.11 |
| Prior heart failure | 0.94 (0.52; 1.72) | 0.85 |
| Diabetes | 0.99 (0.54; 1.80) | 0.97 |
| Hypertension | 0.79 (0.50; 1.26) | 0.33 |
| Coronary heart disease | 1.03 (1.01; 1.05) | 0.01 |
| Tachycardia induced cardiomyopathy | 0.77 (0.32; 1.82) | 0.54 |
| LVEF, per 1% | 1.00 (0.98; 1.01) | 0.66 |
| LA volume, per 1 mL | 1.01 (0.99; 1.03) | 0.25 |
| AAD | 0.98 (0.84; 1.14) | 0.77 |
| Beta-blockers | 1.18 (0.72; 1.92) | 0.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krisai, P.; Roten, L.; Zeljkovic, I.; Pavlovic, N.; Ammann, P.; Reichlin, T.; Auf der Maur, E.; Streicher, O.; Knecht, S.; Kühne, M.; et al. Prospective Evaluation of a Standardized Screening for Atrial Fibrillation after Ablation of Cavotricuspid Isthmus Dependent Atrial Flutter. J. Clin. Med. 2021, 10, 4453. https://doi.org/10.3390/jcm10194453
Krisai P, Roten L, Zeljkovic I, Pavlovic N, Ammann P, Reichlin T, Auf der Maur E, Streicher O, Knecht S, Kühne M, et al. Prospective Evaluation of a Standardized Screening for Atrial Fibrillation after Ablation of Cavotricuspid Isthmus Dependent Atrial Flutter. Journal of Clinical Medicine. 2021; 10(19):4453. https://doi.org/10.3390/jcm10194453
Chicago/Turabian StyleKrisai, Philipp, Laurent Roten, Ivan Zeljkovic, Nikola Pavlovic, Peter Ammann, Tobias Reichlin, Eric Auf der Maur, Olivia Streicher, Sven Knecht, Michael Kühne, and et al. 2021. "Prospective Evaluation of a Standardized Screening for Atrial Fibrillation after Ablation of Cavotricuspid Isthmus Dependent Atrial Flutter" Journal of Clinical Medicine 10, no. 19: 4453. https://doi.org/10.3390/jcm10194453