
Gait Kinetic and Kinematic Changes in Chronic Low Back Pain Patients and the Effect of Manual Therapy: A Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
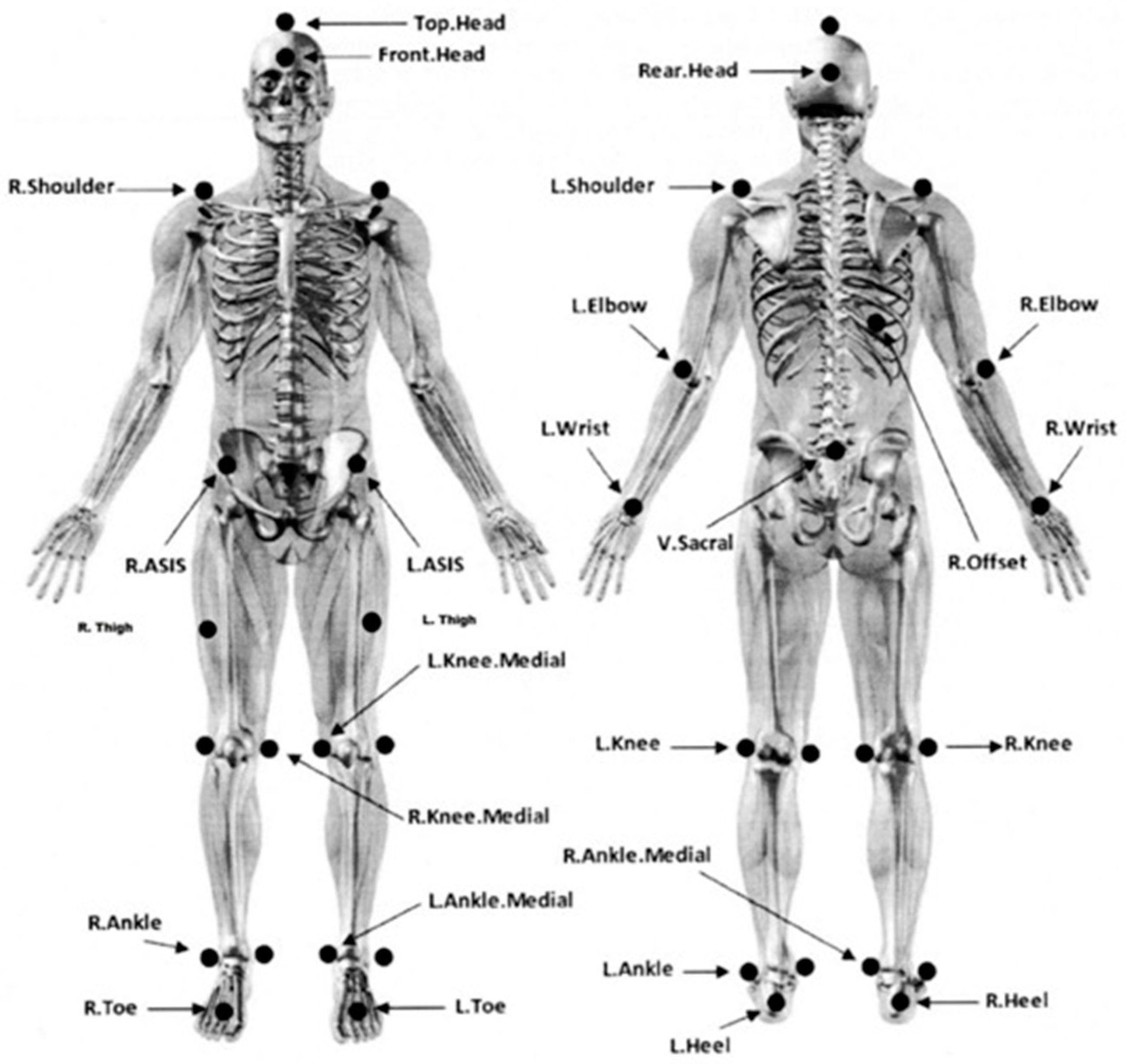
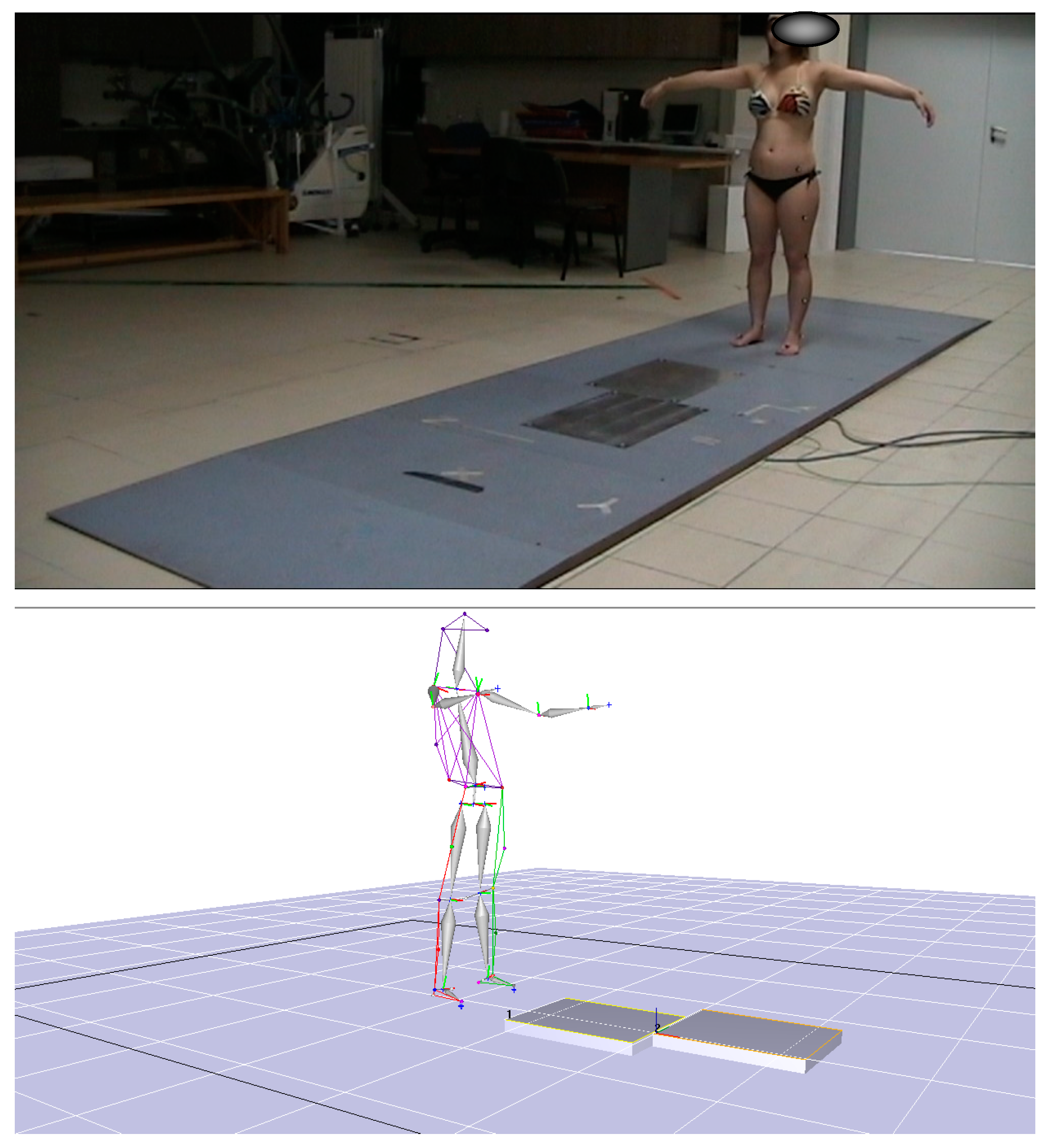
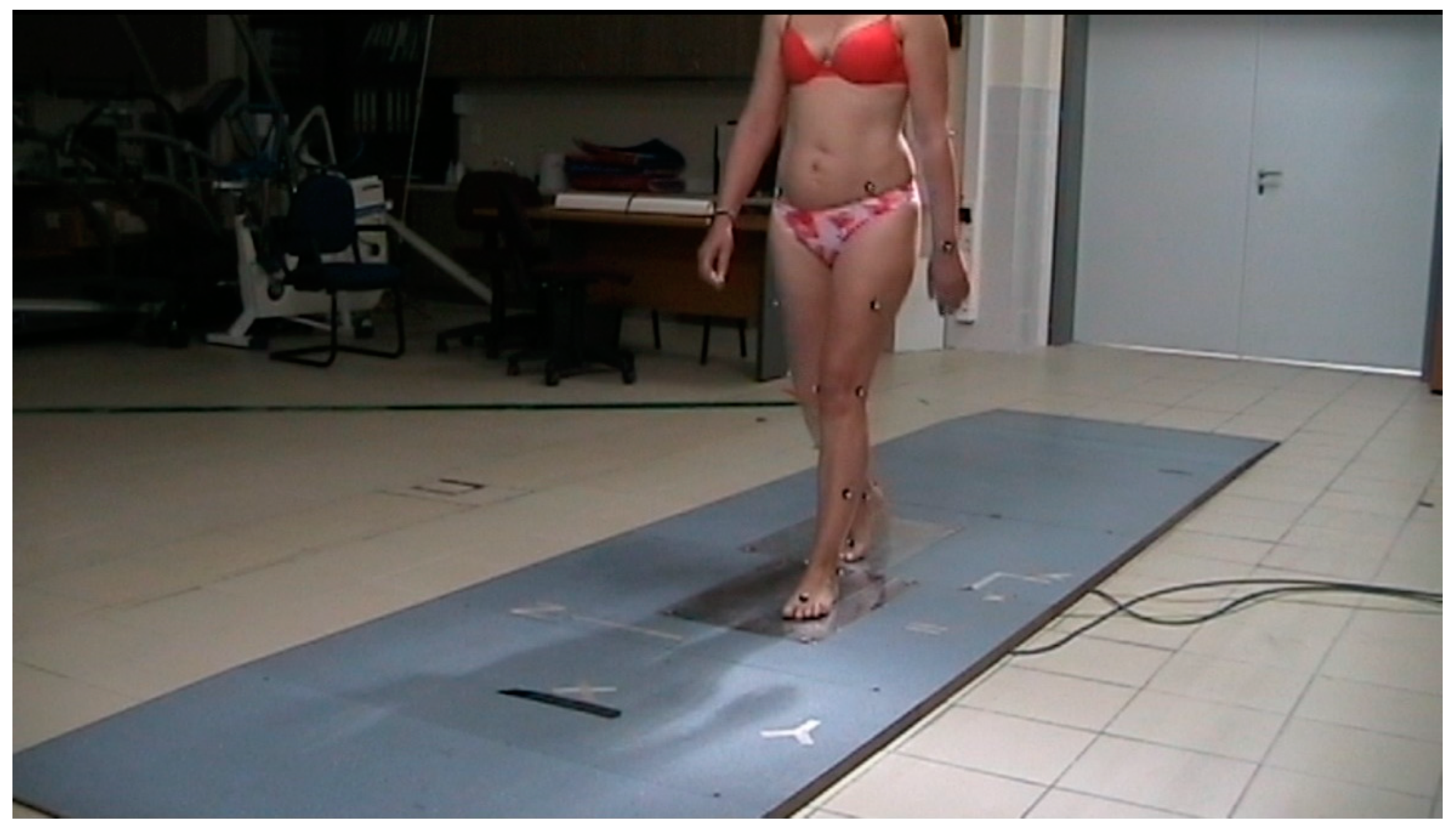
2.1. Equipment
2.2. Procedures
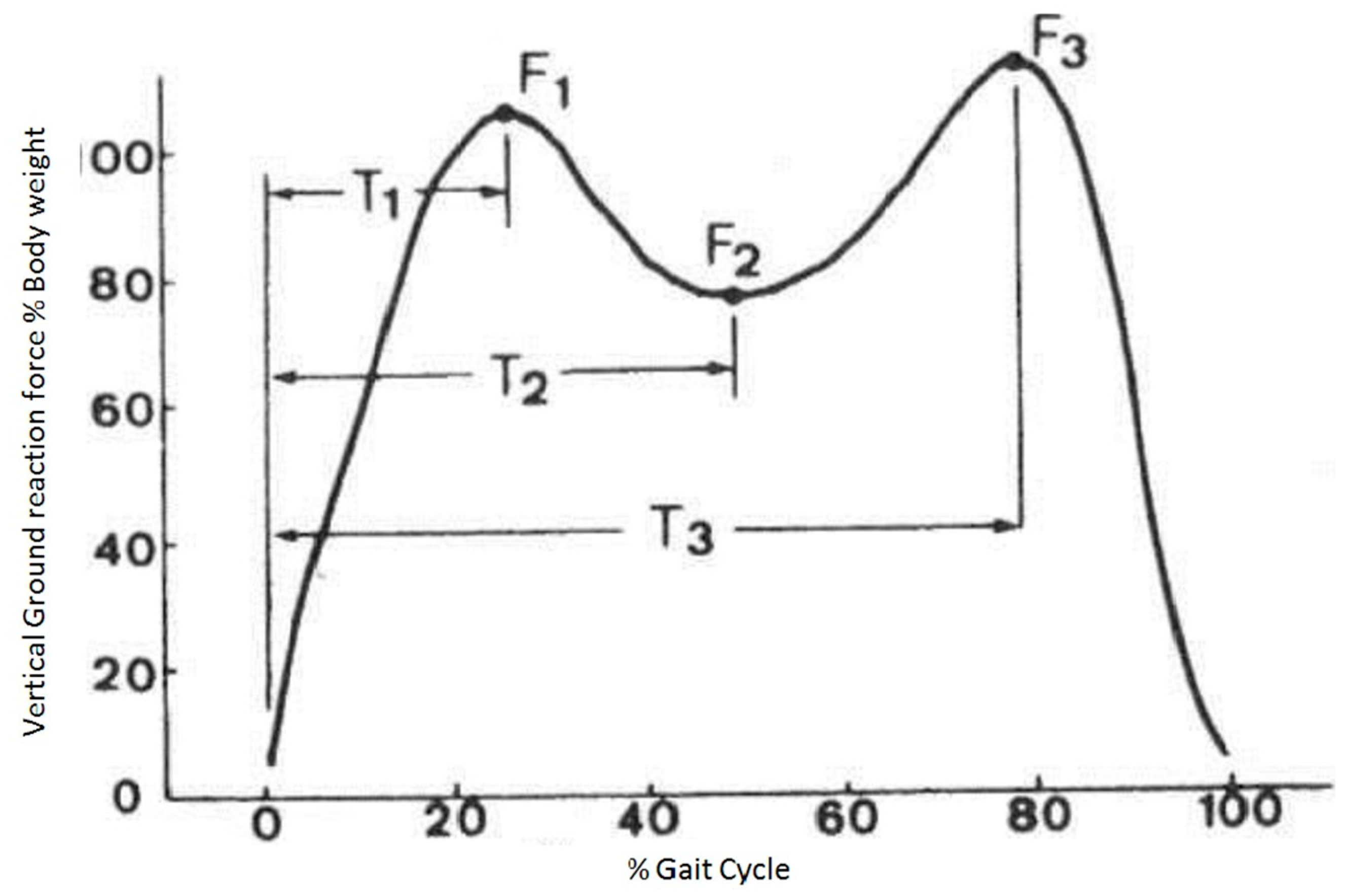
- (1)
- Τ1: moment of peak value of ground reacting force (F1) during heel strike;
- (2)
- Τ2: moment of minimum value of ground reacting force (F2) during mid stance;
- (3)
- Τ3: moment of peak value of ground reacting force (F3) during acceleration [51].
2.3. Interventions
2.4. Statistical Analysis
3. Results
3.1. Comparison between Groups
3.2. Gait Symmetry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Kinetic Values | Manual Therapy | Sham Therapy | Classic Physiotherapy | ANCOVA | |
|---|---|---|---|---|---|
| GRF Right Τ1 (%BW) | Before M(SD) | 106.27 (6.97) | 106.99 (7.33) | 107.02 (6.97) | p = 0.001 * |
| After Ma | 104.3 | 107.81 | 107.82 | ||
| GRF Right Τ2 (%BW) | Before M(SD) | 80.86 (6.12) | 79.18 (7.83) | 77.97 (7.7) | p = 0.89 |
| After Ma | 78.45 | 78.21 | 78.05 | ||
| GRF Right Τ3 (%BW) | Before M(SD) | 114.82 (8.21) | 114.28 (8) | 113.53 (7.93) | p = 0.001 * |
| After Ma | 108.75 | 115.85 | 117.2 | ||
| GRF Left Τ1 (%BW) | Before M(SD) | 109.03 (8.88) | 106.12 (6.92) | 107.28 (8.44) | p = 0.001 * |
| After Ma | 102.95 | 108.31 | 109.03 | ||
| GRF Left Τ2 (%BW) | Before M(SD) | 82.5 (9.88) | 78.47 (10.1) | 78.65 (9.97) | p = 0.89 |
| After Ma | 78.22 | 77.75 | 77.56 | ||
| GRF Left Τ3 (%BW) | Before M(SD) | 116.5 (10.08) | 112.1 (7.86) | 114.37 (9.43) | p = 0.001 * |
| After Ma | 108.22 | 115.88 | 116.55 | ||
| Trunk Kinematic Values | Manual Therapy | Sham Therapy | Classic Physiotherapy | ANCOVA p | |
|---|---|---|---|---|---|
| Trunk frontal plane Τ1 right (degrees) | Before M(SD) | −0.22 (2.1) | −1.18 (1.64) | 0.39 (1.96) | 0.001 *** |
| After Ma | −1.38 | −0.26 | −0.99 | ||
| Trunk frontal plane Τ2 right (degrees) | Before M(SD) | 0.2 (1.94) | −1.69 (1.56) | −0.82 (1.86) | 0.001 ** |
| After Ma | −0.64 | −0.91 | 1.33 | ||
| Trunk frontal plane Τ3 right (degrees) | Before M(SD) | 0.58 (1.63) | −0.09 (1.29) | 0.357 (1.33) | 0.011 *** |
| After Ma | −1.32 | −0.28 | −0.37 | ||
| Trunk sagittal plane Τ1 right (degrees) | Before M(SD) | −4.19 (5.16) | −1.34 (4.05) | 2.77 (4.1) | 0.06 |
| After Ma | −2.76 | −2.87 | −4.11 | ||
| Trunk sagittal plane Τ2 right (degrees) | Before M(SD) | −3.46 (4.56) | −1.53 (3.63) | −2.7 (3.79) | 0.2 |
| After Ma | −1.33 | −2.17 | −1.85 | ||
| Trunk sagittal plane Τ3 right (degrees) | Before M(SD) | −3.19 (4.09) | −2.58 (4.42) | −2.91 (3.43) | 0.008 * |
| After Ma | −3.2 | −2.07 | −3.49 | ||
| Trunk transverse plane Τ1 right (degrees) | Before M(SD) | 2.06 (4.5) | 5.54 (4.44) | 4.44 (4.52) | 0.001 * |
| After Ma | 1.8 | −2.28 | 3.61 | ||
| Trunk transverse plane Τ2 right (degrees) | Before M(SD) | 3.12 (3.64) | 7.14 (4.47) | 5.83 (4.21) | 0.001 *** |
| After Ma | 6.86 | 3.55 | 5.06 | ||
| Trunk transverse plane Τ3 right (degrees) | Before M(SD) | 4.4 (5.83) | 4.42 (3.88) | 6.2 (5.56) | 0.001 ** |
| After Ma | 8.14 | 7.39 | 3.09 | ||
| Trunk frontal plane Τ1 left (degrees) | Before M(SD) | 0.06 (1.12) | 0.12 (1.57) | 0.97 (1.19) | 0.001 *** |
| After Ma | 1.58 | 0.55 | 0.33 | ||
| Trunk frontal plane Τ2 left (degrees) | Before M(SD) | −0.29 (1.45) | −0.56 (2.03) | 0.62 (1.47) | 0.27 |
| After Ma | 0.39 | −0.25 | 0.33 | ||
| Trunk frontal plane Τ3 left (degrees) | Before M(SD) | −1.59 (2) | −2.34 (1.82) | −0.98 (1.96) | 0.001 *** |
| After Ma | 1.57 | −1.21 | −2.03 | ||
| Trunk sagittal plane Τ1 left (degrees) | Before M(SD) | −4.46 (4.78) | −3.29 (4.04) | −3.5 (4.14) | 0.81 |
| After Ma | −3.26 | −3.27 | −3.63 | ||
| Trunk sagittal plane Τ2 left (degrees) | Before M(SD) | −4.23 (4.36) | −3.85 (3.74) | −4.52 (3.97) | 0.001 ** |
| After Ma | −2.15 | −3.3 | −4.16 | ||
| Trunk sagittal plane Τ3 left (degrees) | Before M(SD) | −4.09 (3.76) | −4.2 (3.57) | −4.89 (3.26) | 0.27 |
| After Ma | −3.82 | −3.72 | −4.44 | ||
| Trunk transverse plane Τ1 left (degrees) | Before M(SD) | 2.44 (4.44) | 2.11 (4.88) | 3.96 (5.51) | 0.001 *** |
| After Ma | −0.33 | 4.18 | 4.24 | ||
| Trunk transverse plane Τ2 left (degrees) | Before M(SD) | 0.21 (3.8) | −2.58 (6.26) | 1.58 (5.83) | 0.001 *** |
| After Ma | −4.41 | 1.75 | 0.64 | ||
| Trunk transverse plane Τ3 left (degrees) | Before M(SD) | −0.55 (4.31) | −1.87 (5.25) | −1.29 (4.34) | 0.001 *** |
| After Ma | −7.83 | −1.62 | −1.55 | ||
| Pelvic Kinematic Values | Manual Therapy | Sham Therapy | Classic Physiotherapy | ANCOVA p | |
|---|---|---|---|---|---|
| Pelvis frontal plane Τ1 right (degrees) | Before M(SD) | 1.94 (5.76) | 1.15 (2.82) | 0.75 (5.12) | 0.02 ** |
| After Ma | 3.81 | 2.95 | 1.5 | ||
| Pelvis frontal plane Τ2 right (degrees) | Before M(SD) | 1.26 (3.65) | −1.23 (2.26) | 0.59 (3.71) | 0.31 |
| After Ma | 0.15 | 1.03 | 0.67 | ||
| Pelvis frontal plane Τ3 right (degrees) | Before M(SD) | −0.67 (2.2) | −3.79 (3.67) | −2.18 (2.88) | 0.001 *** |
| After Ma | −3.13 | −1.04 | −0.84 | ||
| Pelvis sagittal plane Τ1 right (degrees) | Before M(SD) | 12.84 (5.09) | 13.67 (5.33) | 12.98 (4.56) | 0.167 |
| After Ma | 12.12 | 13.63 | 13.42 | ||
| Pelvis sagittal plane Τ2 right (degrees) | Before M(SD) | 13.26 (4.24) | 14.85 (4.07) | 12.74 (3.44) | 0.013 ** |
| After Ma | 12.65 | 12.3 | 14.34 | ||
| Pelvis sagittal plane Τ3 right (degrees) | Before M(SD) | 14.42 (4.43) | 11.44 (8.64) | 12.94 (4.54) | 0.001 *** |
| After Ma | 12.87 | 15.3 | 16.27 | ||
| Pelvis transverse plane Τ1 right (degrees) | Before M(SD) | 3.14 (6.03) | 2.9 (4.96) | 2.14 (5.83) | 0.12 |
| After Ma | 4.11 | 4.53 | 2.73 | ||
| Pelvis transverse plane Τ2 right (degrees) | Before M(SD) | 3.56 (5.64) | 2.06 (6.73) | 1.07 (5.81) | 0.07 |
| After Ma | 2.55 | 4 | 4.7 | ||
| Pelvis transverse plane Τ3 right (degrees) | Before M(SD) | 1.76 (6.55) | −0.34 (5.89) | 1.73 (6.84) | 0.001 *** |
| After Ma | −5.55 | 0.86 | 1.89 | ||
| Pelvis frontal plane Τ1 left (degrees) | Before M(SD) | −2.1 (3.84) | −0.61 (2.76) | −2.5 (3.72) | 0.23 |
| After Ma | −3.91 | −4.18 | −2.86 | ||
| Pelvis frontal plane Τ2 left (degrees) | Before M(SD) | 0.46 (2.12) | 1.59 (3.48) | 0.59 (2.3) | 0.1 |
| After Ma | −0.11 | −0.7 | 0.43 | ||
| Pelvis frontal plane Τ3 left (degrees) | Before M(SD) | 1.54 (2.5) | 2.04 (3.6) | 1.94 (2.8) | 0.059 |
| After Ma | 2.43 | 1.3 | 1.64 | ||
| Pelvis sagittal plane Τ1 left (degrees) | Before M(SD) | 11.09 (7.28) | 11.41 (9.78) | 7.7 (10) | 0.19 |
| After Ma | 10.93 | 8.87 | 9.1 | ||
| Pelvis sagittal plane Τ2 left (degrees) | Before M(SD) | 12.27 (7.2) | 10.63 (10.17) | 9.8 (10.44) | 0.8 |
| After Ma | 11.37 | 11.68 | 10.89 | ||
| Pelvis sagittal plane Τ3 left (degrees) | Before M(SD) | 13.07 (10.21) | 11.98 (10.26) | 8.19 (11.12) | 0.38 |
| After Ma | 12.12 | 10.05 | 11.15 | ||
| Pelvis transverse plane Τ1 left (degrees) | Before M(SD) | −0.86 (3.24) | 2.15 (5.77) | −1.75 (3.76) | 0.05 |
| After Ma | −3.77 | −1.66 | −1.74 | ||
| Pelvis transverse plane Τ2 left (degrees) | Before M(SD) | 1.71 (4.15) | 7.29 (7.21) | 4.42 (4.5) | 0.15 |
| After Ma | 3.7 | 4.1 | 4.7 | ||
| Pelvis transverse plane Τ3 left (degrees) | Before M(SD) | 5.41 (7.61) | 7.86 (7.33) | 6.62 (6.94) | 0.69 |
| After Ma | 5.87 | 6.86 | 6.54 | ||
| Manual Therapy | Sham Treatment | Classic Physiotherapy | p | |
|---|---|---|---|---|
| GRF Τ1 | 1.012 | 1.001 | 0.995 | 0.96 |
| GRF Τ2 | 1.003 | 1.018 | 1.011 | 0.42 |
| GRF Τ3 | 1.008 | 1.006 | 1.009 | 0.965 |
| Pelvis frontal planeΤ1 | 0.419 | 0.295 | 0.427 | 0.994 |
| Trunk sagittal planeΤ1 | 0.978 | 0.953 | 1.05 | 0.877 |
| Pelvis sagittal planeΤ1 | 1.032 | 0.031 | 0.784 | 0.157 |
| Trunk transverse planeΤ1 | 1.585 | 0.914 | 1.145 | 0.071 |
| Pelvis transverse planeΤ1 | 1.162 | 4.727 | 3.716 | 0.495 |
| Pelvis sagittal planeΤ2 | 1.122 | 1.025 | 0.716 | 0.14 |
| Trunk transverse planeΤ2 | 1.788 | 7.62 | 0.828 | 0.293 |
| Pelvis transverse planeΤ2 | 1.124 | 0.635 | 9.146 | 0.184 |
| Trunk frontal planeΤ3 | 0.973 | 1.023 | 0.776 | 0.255 |
| Pelvis frontal planeΤ3 | 1.236 | 0.16 | 0.679 | 0.515 |
| Trunk sagittal planeΤ3 | 1.114 | 0.383 | 2.022 | 0.467 |
| Pelvis sagittal planeΤ3 | 0.155 | 2.01 | 0.67 | 0.35 |
| Trunk transverse planeΤ3 | 1.343 | 0.878 | 10.714 | 0.069 |
| Pelvis transverse planeΤ3 | 0.965 | 0.45 | 0.285 | 0.078 |
| Trunk frontal plane Τ1 | 1.147 | 0.852 | 0.4 | 0.028 |
| Trunk frontal plane Τ2 | 1.307 | 0.172 | 0.429 | 0.009 |
| Pelvis frontal plane Τ2 | 0.844 | 1.295 | 1.044 | 0.003 |
| Trunk sagittal plane Τ2 | 0.272 | 1.645 | 1.819 | 0.017 |
References
- Huang, Y.P.; Bruijn, S.M.; Lin, J.H.; Meijer, O.G.; Wu, W.H.; Abbasi-Bafghi, H.; Lin, X.C.; van Dieën, J.H. Gait adaptations in low back pain patients with lumbar disc herniation: Trunk coordination and arm swing. Eur. Spine J. 2011, 20, 491–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamoth, C.J.; Daffertshofer, A.; Meijer, O.G.; Beek, P.J. How do persons with chronic low back pain speed up and slow down? Trunk-pelvis coordination and lumbar erector spinae activity during gait. Gait. Posture 2006, 23, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Taylor, N.F.; Evans, O.M.; Goldie, P.A. The effect of walking faster on people with acute low back pain. Eur. Spine J. 2003, 12, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, R.; Kamruzzaman, J. A machine learning approach for automated recognition of movement patterns using basic, kinetic and kinematic gait data. J. Biomech. 2005, 38, 401–408. [Google Scholar] [CrossRef]
- Bianchi, L.; Angelini, D.; Orani, G.P.; Lacquaniti, F. Kinematic coordination in human gait: Relation to mechanical energy cost. J. Neurophysiol. 1998, 79, 2155–2170. [Google Scholar] [CrossRef]
- Conti, S.; Lalonde, K.A.; Martin, R. Kinematic analysis of the agility total ankle during gait. Foot Ankle Int. 2006, 27, 980–984. [Google Scholar] [CrossRef]
- Desailly, E.; Daniel, Y.; Sardain, P.; Lacouture, P. Foot contact event detection using kinematic data in cerebral palsy children and normal adults gait. Gait Posture 2009, 29, 76–80. [Google Scholar] [CrossRef]
- Clouet, J.; Vinatier, C.; Merceron, C.; Pot-Vauce, M.; Hamel, O.; Weiss, P.; Grimandi, G.; Guicheux, J. The intervertebral disc: From pathophysiology to tissue engineering. Jt. Bone Spine 2009, 76, 614–618. [Google Scholar] [CrossRef]
- Brinjikji, W.; Diehn, F.E.; Jarvik, J.G.; Carr, C.M.; Kallmes, D.F.; Murad, M.H.; Luetmer, P.H. MRI Findings of Disc Degeneration are More Prevalent in Adults with Low Back Pain than in Asymptomatic Controls: A Systematic Review and Meta-Analysis. AJNR Am. J. Neuroradiol. 2015, 36, 2394–2399. [Google Scholar] [CrossRef] [Green Version]
- Benner, B.; Ehni, G. Degenerative lumbar scoliosis. Spine 1979, 4, 548–552. [Google Scholar] [CrossRef]
- Cho, K.J.; Suk, S.I.; Park, S.R.; Kim, J.H.; Kim, S.S.; Lee, T.J.; Lee, J.J.; Lee, J.M. Short fusion versus long fusion for degenerative lumbar scoliosis. Eur. Spine J. 2008, 17, 650–656. [Google Scholar] [CrossRef] [Green Version]
- Crawford, C.H., 3rd; Glassman, S.D. Surgical treatment of lumbar spinal stenosis associated with adult scoliosis. Instr. Course Lect. 2009, 58, 669–676. [Google Scholar]
- Danielsson, A.J.; Cederlund, C.G.; Ekholm, S.; Nachemson, A.L. The prevalence of disc aging and back pain after fusion extending into the lower lumbar spine. A matched MR study twenty-five years after surgery for adolescent idiopathic scoliosis. Acta Radiol. 2001, 42, 187–197. [Google Scholar]
- Mitchell, T.; O’Sullivan, P.B.; Burnett. A.F.; Straker, L.; Smith, A. Regional differences in lumbar spinal posture and the influence of low back pain. BMC Musculoskelet Disord. 2008, 9, 152. [Google Scholar] [CrossRef] [Green Version]
- Al-Eisa, E.; Egan, D.; Deluzio, K.; Wassersug, R. Effects of pelvic skeletal asymmetry on trunk movement: Three-dimensional analysis in healthy individuals versus patients with mechanical low back pain. Spine 2006, 1, E71–E79. [Google Scholar] [CrossRef] [PubMed]
- Harris-Hayes, M.; Van Dillen, L.R. The inter-tester reliability of physical therapists classifying low back pain problems based on the movement system impairment classification system. PM R 2009, 1, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.U.; Lee, J.I.; Butts, K.; Carragee, E.; Fredericson, M. Changes in posterior lumbar disk contour abnormality with flexion-extension movement in subjects with low back pain and degenerative disk disease. PM R 2009, 1, 541–546. [Google Scholar] [CrossRef]
- Luomajoki, H.; Kool, J.; de Bruin, E.D.; Airaksinen, O. Movement control tests of the low back; evaluation of the difference between patients with low back pain and healthy controls. BMC Musculoskelet Disord. 2008, 9, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbott, J.H.; Fritz, J.M.; McCane, B.; Shultz, B.; Herbison, P.; Lyons, B.; Stefanko, G.; Walsh, R.M. Lumbar segmental mobility disorders: Comparison of two methods of defining abnormal displacement kinematics in a cohort of patients with non-specific mechanical low back pain. BMC Musculoskelet Disord. 2006, 7, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett, A.F.; Cornelius, M.W.; Dankaerts, W.; O’sullivan, P.B. Spinal kinematics and trunk muscle activity in cyclists: A comparison between healthy controls and non-specific chronic low back pain subjects-a pilot investigation. Man. Ther. 2004, 9, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Dankaerts, W.; O’Sullivan, P.; Burnett, A.; Straker, L.; Davey, P.; Gupta, R. Discriminating healthy controls and two clinical subgroups of nonspecific chronic low back pain patients using trunk muscle activation and lumbosacral kinematics of postures and movements: A statistical classification model. Spine 2009, 34, 1610–1618. [Google Scholar] [CrossRef]
- Engsberg, J.R.; Bridwell, K.H.; Wagner, J.M.; Uhrich, M.L.; Blanke, K.; Lenke, L.G. Gait changes as the result of deformity reconstruction surgery in a group of adults with lumbar scoliosis. Spine 2003, 15, 1836–1843. [Google Scholar] [CrossRef] [PubMed]
- Gombatto, S.P.; Collins, D.R.; Sahrmann, S.A.; Engsberg, J.R.; Van Dillen, L.R. Patterns of lumbar region movement during trunk lateral bending in 2 subgroups of people with low back pain. Phys. Ther. 2007, 87, 441–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shum, G.L.; Crosbie, J.; Lee, R.Y. Effect of low back pain on the kinematics and joint coordination of the lumbar spine and hip during sit-to-stand and stand-to-sit. Spine 2005, 30, 1998–2004. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.E.; Simmonds, M.J.; Etnyre, B.R.; Morris, G.S. Influence of pain distribution on gait characteristics in patients with low back pain: Part 1: Vertical ground reaction force. Spine 2007, 32, 1329–1336. [Google Scholar] [CrossRef]
- Keller, T.S.; Weisberger, A.M.; Ray, J.L.; Hasan, S.S.; Shiavi, R.G.; Spengler, D.M. Relationship between vertical ground reaction force and speed during walking, slow jogging, and running. Clin. Biomech. 1996, 11, 253–259. [Google Scholar] [CrossRef]
- Nilsson, J.; Thorstensson, A. Ground reaction forces at different speeds of human walking and running. Acta Physiol. Scand. 1989, 136, 217–227. [Google Scholar] [CrossRef] [PubMed]
- van der Hulst, M.; Vollenbroek-Hutten, M.M.; Rietman, J.S.; Hermens, H.J. Lumbar and abdominal muscle activity during walking in subjects with chronic low back pain: Support of the "guarding" hypothesis? J. Electromyogr. Kinesiol. 2010, 20, 31–38. [Google Scholar] [CrossRef]
- van den Hoorn, W.; Bruijn, S.M.; Meijer, O.G.; Hodges, P.W.; van Dieën, J.H. Mechanical coupling between transverse plane pelvis and thorax rotations during gait is higher in people with low back pain. J. Biomech. 2012, 45, 342–347. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.S.; Shakoor, M.A.; Khan, A.A. Evaluation of the effects of shortwave diathermy in patients with chronic low back pain. Bangladesh Med. Res. Counc. Bull. 2009, 35, 18–20. [Google Scholar] [CrossRef]
- Khadilkar, A.; Odebiyi, D.O.; Brosseau, L.; Wells, G.A. Transcutaneous electrical nerve stimulation (TENS) versus placebo for chronic low-back pain. Cochrane Database Syst. Rev. 2008, 4, CD003008. [Google Scholar] [CrossRef]
- Adamczyk, A.; Kiebzak, W.; Wilk-Frańczuk, M.; Sliwiński, Z. Effectiveness of holistic physiotherapy for low back pain. Ortop. Traumatol. Rehabil. 2009, 11, 562–576. [Google Scholar]
- Ansari, N.N.; Ebadi, S.; Talebian, S.; Naghdi, S.; Mazaheri, H.; Olyaei, G.; Jalaie, S. A randomized, single blind placebo controlled clinical trial on the effect of continuous ultrasound on low back pain. Electromyogr. Clin. Neurophysiol. 2006, 46, 329–336. [Google Scholar]
- Bunzli, S.; Gillham, D.; Esterman, A. Physiotherapy-provided operant conditioning in the management of low back pain disability: A systematic review. Physiother. Res. Int. 2011, 16, 4–19. [Google Scholar] [CrossRef] [PubMed]
- French, S.D.; Cameron, M.; Walker, B.F.; Reggars, J.W.; Esterman, A.J. A Cochrane review of superficial heat or cold for low back pain. Spine 2006, 31, 998–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aure, O.F.; Nilsen, J.H.; Vasseljen, O. Manual therapy and exercise therapy in patients with chronic low back pain: A randomized, controlled trial with 1-year follow-up. Spine 2003, 28, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Byrne, K.; Doody, C.; Hurley, D.A. Exercise therapy for low back pain: A small-scale exploratory survey of current physiotherapy practice in the Republic of Ireland acute hospital setting. Man. Ther. 2006, 11, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Cairns, M.C.; Foster, N.E.; Wright, C. Randomized controlled trial of specific spinal stabilization exercises and conventional physiotherapy for recurrent low back pain. Spine 2006, 31, E670–E681. [Google Scholar] [CrossRef] [Green Version]
- Casserley-Feeney, S.N.; Bury, G.; Daly, L.; Hurley, D.A. Physiotherapy for low back pain: Differences between public and private healthcare sectors in Ireland--a retrospective survey. Man. Ther. 2008, 13, 441–449. [Google Scholar] [CrossRef]
- Blomberg, S.; Hallin, G.; Grann, K.; Berg, E.; Sennerby, U. Manual therapy with steroid injections-A new approach to treatment of low back pain. Spine 1994, 19, 569–577. [Google Scholar] [CrossRef]
- Geisser, M.E.; Wiggert, E.A.; Haig, A.J.; Colwell, M.O. A randomized, controlled trial of manual therapy and specific adjuvant exercise for chronic low back pain. Clin. J. Pain. 2005, 21, 463–470. [Google Scholar] [CrossRef] [Green Version]
- Harvey, E.; Burton, A.K.; Moffett, J.K.; Breen, A. Spinal manipulation for low-back pain: A treatment package agreed to by the UK chiropractic, osteopathy and physiotherapy professional associations. Man. Ther. 2003, 8, 46–51. [Google Scholar] [CrossRef]
- Krekoukias, G.; Gelalis, I.D.; Xenakis, T.; Gioftsos, G.; Dimitriadis, Z.; Sakellari, V. Spinal mobilization vs conventional physiotherapy in the management of chronic low back pain due to spinal disk degeneration: A randomized controlled trial. J. Man. Manip. Ther. 2017, 25, 66–73. [Google Scholar] [CrossRef] [Green Version]
- Carpino, G.; Tran, S.; Currie, S.; Enebo, B.; Davidson, B.S.; Howarth, S.J. Does manual therapy affect functional and biomechanical outcomes of a sit-to-stand task in a population with low back pain? A preliminary analysis. Chiropr. Man. Therap. 2020, 28, 1–9. [Google Scholar] [CrossRef]
- G*Power. Available online: https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower (accessed on 1 October 2012).
- Griffith, J.F.; Wang, Y.X.; Antonio, G.E.; Choi, K.C.; Yu, A.; Ahuja, A.T.; Leung, P.C. Modified Pfirrmann grading system for lumbar intervertebral disc degeneration. Spine 2007, 32, E708–E712. [Google Scholar] [CrossRef] [PubMed]
- Ewins, D.; Collins, T. Clinical Gait Analysis. In Clinical Engineering: A Handbook for Clinical and Biomedical Engineers; Taktak, A., Ganney, P., Long, D., Axel, R., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 389–406. [Google Scholar]
- Egerton, T.; Danoudis, M.; Huxham, F.; Iansek, R. Central gait control mechanisms and the stride length—Cadence relationship. Gait Posture. 2011, 34, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, J.P.; Patla, A.E.; McGill, S.M. Low back three-dimensional joint forces, kinematics, and kinetics during walking. Clin. Biomech. 1999, 14, 203–216. [Google Scholar] [CrossRef]
- Mello, R.G.; Oliveira, L.F.; Nadal, J. Digital Butterworth filter for subtracting noise from low magnitude surface electromyogram. Comput. Methods Programs. Biomed. 2007, 87, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Chao, E.Y.; Laughman, R.K.; Schneider, E.; Stauffer, R.N. Normative data of knee joint motion and ground reaction forces in adult level walking. J. Biomech. 1983, 16, 219–233. [Google Scholar] [CrossRef]
- GraphPad. Available online: https://www.graphpad.com/quickcalcs/randomize1/ (accessed on 1 October 2012).
- Bronfort, G.; Haas, M.; Evans, R.; Kawchuk, G.; Dagenais, S. Evidence-informed management of chronic low back pain with spinal manipulation and mobilization. Spine J. 2008, 8, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Goodsell, M.; Lee, M.; Latimer, J. Short-term effects of lumbar posteroanterior mobilization in individuals with low-back pain. J. Manip. Physiol. Ther. 2000, 23, 332–342. [Google Scholar] [CrossRef]
- Shum, G.L.; Tsung, B.Y.; Lee, R.Y. The immediate effect of posteroanterior mobilization on reducing back pain and the stiffness of the lumbar spine. Arch. Phys. Med. Rehabil. 2013, 94, 673–679. [Google Scholar] [CrossRef]
- França, F.R.; Burke, T.N.; Caffaro, R.R.; Ramos, L.A.; Marques, A.P. Effects of muscular stretching and segmental stabilization on functional disability and pain in patients with chronic low back pain: A randomized, controlled trial. J. Manip. Physiol. Ther. 2012, 35, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Pivec, R.; Stokes, M.; Chitnis, A.S.; Paulino, C.B.; Harwin, S.F.; Mont, M.A. Clinical and economic impact of TENS in patients with chronic low back pain: Analysis of a nationwide database. Orthopedics 2013, 36, 922–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sritoomma, N.; Moyle, W.; Cooke, M.; O’Dwyer, S. The effectiveness of Swedish massage with aromatic ginger oil in treating chronic low back pain in older adults: A randomized controlled trial. Complement. Ther. Med. 2014, 22, 26–33. [Google Scholar] [CrossRef]
- Norman, G.R.; Streiner, D.L. Measuring Change. Biostatistics the Bare Essentials, 2nd ed.; B.C. Decker INC.: Hamilton, ON, Canada, 2000; pp. 155–162. [Google Scholar]
- Field, A. Comparing several means: ANOVA. In Discovering Statistics Using SPSS, 3rd ed.; Field, A., Ed.; SAGE: London, UK, 2009; pp. 347–394. [Google Scholar]
- Seliktar, R.; Mizrahi, J. Some gait characteristics of below-knee amputees and their reflection on the ground reaction forces. Eng. Med. 1986, 15, 27–34. [Google Scholar] [CrossRef]
- O’Sullivan, K.; Verschueren, S.; Van Hoof, W.; Ertanir, F.; Martens, L.; Dankaerts, W. Lumbar repositioning error in sitting: Healthy controls versus people with sitting-related non-specific chronic low back pain (flexion pattern). Man. Ther. 2013, 18, 526–532. [Google Scholar] [CrossRef]
- Learman, K.E.; Myers, J.B.; Lephart, S.M.; Sell, T.C.; Kerns, G.J.; Cook, C.E. Effects of spinal manipulation on trunk proprioception in subjects with chronic low back pain during symptom remission. J. Manipulative Physiol. Ther. 2009, 32, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Ghamkhar, L.; Kahlaee, A.H. Trunk muscles activation pattern during walking in subjects with and without chronic low back pain: A Systematic Review. PM R 2015, 7, 519–526. [Google Scholar] [CrossRef]
- Arendt-Nielsen, L.; Graven-Nielsen, T.; Svarrer, H.; Svensson, P. The influence of low back pain on muscle activity and coordination during gait: A clinical and experimental study. Pain 1995, 64, 231–240. [Google Scholar] [CrossRef]
- Radebold, A.; Cholewicki, J.; Panjabi, M.M.; Patel, T.C. Muscle response pattern to sudden trunk loading in healthy individuals and in patients with chronic low back pain. Spine 2000, 25, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Radebold, A.; Cholewicki, J.; Polzhofer, G.K.; Greene, H.S. Impaired postural control of the lumbar spine is associated with delayed muscle response times in patients with chronic idiopathic low back pain. Spine 2001, 26, 724–730. [Google Scholar] [CrossRef]
- Krekoukias, G.; Petty, N.J.; Cheek, L. Comparison of surface electromyographic activity of erector spinae before and after the application of central posteroanterior mobilisation on the lumbar spine. J. Electromyogr. Kinesiol. 2009, 19, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Harvey, M.P.; Descarreaux, M. Short term modulation of trunk neuromuscular responses following spinal manipulation: A control group study. BMC Musculoskelet Disord. 2013, 14, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterling, M.; Jull, G.; Wright, A. Cervical mobilisation: Concurent effects on pain, sympathetic nervous system activity and motor activity. Man. Ther. 2001, 6, 72–81. [Google Scholar] [CrossRef]
- Bourne, D.; Choo, A.; Regan, W.; MacIntyre, D.; Oxland, T. The Placement of Skin Surface Markers for Non-Invasive Measurement of Scapular Kinematics Affects Accuracy and Reliability. Ann. Biomed. Eng. 2010, 39, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Kilby, J.; Heneghan, N.R.; Maybury, M. Manual palpation of lumbo-pelvic landmarks: A validity study. Man. Ther. 2012, 17, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.; Robinson, H.S.; Bjørke, G.; Kvale, A. Reliability and validity of a palpation technique for identifying the spinous processes of C7 and L5. Man. Ther. 2009, 14, 409–414. [Google Scholar] [CrossRef]
- Armand, S.; Sangeux, M.; Baker, R. Optimal markers’ placement on the thorax for clinical gait analysis. Gait Posture. 2014, 39, 147–153. [Google Scholar] [CrossRef]






| MT Group | ST Group | CP Group | p | |
|---|---|---|---|---|
| Gender (♂/♀) | 12/13 | 14/11 | 16/9 | 0.52 |
| Age (years) | 46.96 (16.07) | 50.08 (12.61) | 45.48 (14.58) | 0.53 |
| Height (cm) | 170.61 (8.36) | 173.54 (8.71) | 173.87 (7.2) | 0.3 |
| Weight (kg) | 77.37 (15.14) | 76.2 (10.3) | 75.7 (9.82) | 0.88 |
| Pain NPRS | 5.96 (1.37) (pre) 1.22 (1.1) (post) | 6.12 (1.06) (pre) 5.88 (0.92) (post) | 6 (1) (pre) 4.96 (0.89) (post) | 0.85 0.001 |
| GDD | 4.72 (1.31) | 4.88 (0.97) | 4.72 (0.79) | 0.8 |
| Manual Therapy | Sham Treatment | Classic Physiotherapy | p | |
|---|---|---|---|---|
| Trunk frontal plane Τ1 | 1.147 | 0.852 | 0.4 | 0.028 * |
| Trunk frontal plane Τ2 | 1.307 | 0.172 | 0.429 | 0.009 * |
| Pelvis frontal plane Τ2 | 0.844 | 1.295 | 1.044 | 0.003 ** |
| Trunk sagittal plane Τ2 | 0.272 | 1.645 | 1.819 | 0.017 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krekoukias, G.; Sakellari, V.; Anastasiadi, E.; Gioftsos, G.; Dimitriadis, Z.; Soultanis, K.; Gelalis, I.D. Gait Kinetic and Kinematic Changes in Chronic Low Back Pain Patients and the Effect of Manual Therapy: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 3593. https://doi.org/10.3390/jcm10163593
Krekoukias G, Sakellari V, Anastasiadi E, Gioftsos G, Dimitriadis Z, Soultanis K, Gelalis ID. Gait Kinetic and Kinematic Changes in Chronic Low Back Pain Patients and the Effect of Manual Therapy: A Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(16):3593. https://doi.org/10.3390/jcm10163593
Chicago/Turabian StyleKrekoukias, Georgios, Vasiliki Sakellari, Elisavet Anastasiadi, Georgios Gioftsos, Zacharias Dimitriadis, Konstantinos Soultanis, and Ioannis D. Gelalis. 2021. "Gait Kinetic and Kinematic Changes in Chronic Low Back Pain Patients and the Effect of Manual Therapy: A Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 16: 3593. https://doi.org/10.3390/jcm10163593