
Quality of Life in European Older Adults of SHARE Wave 7: Comparing the Old and the Oldest-Old

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Sample and Procedure
2.2. Instruments
2.3. Statistical Analyses
3. Results
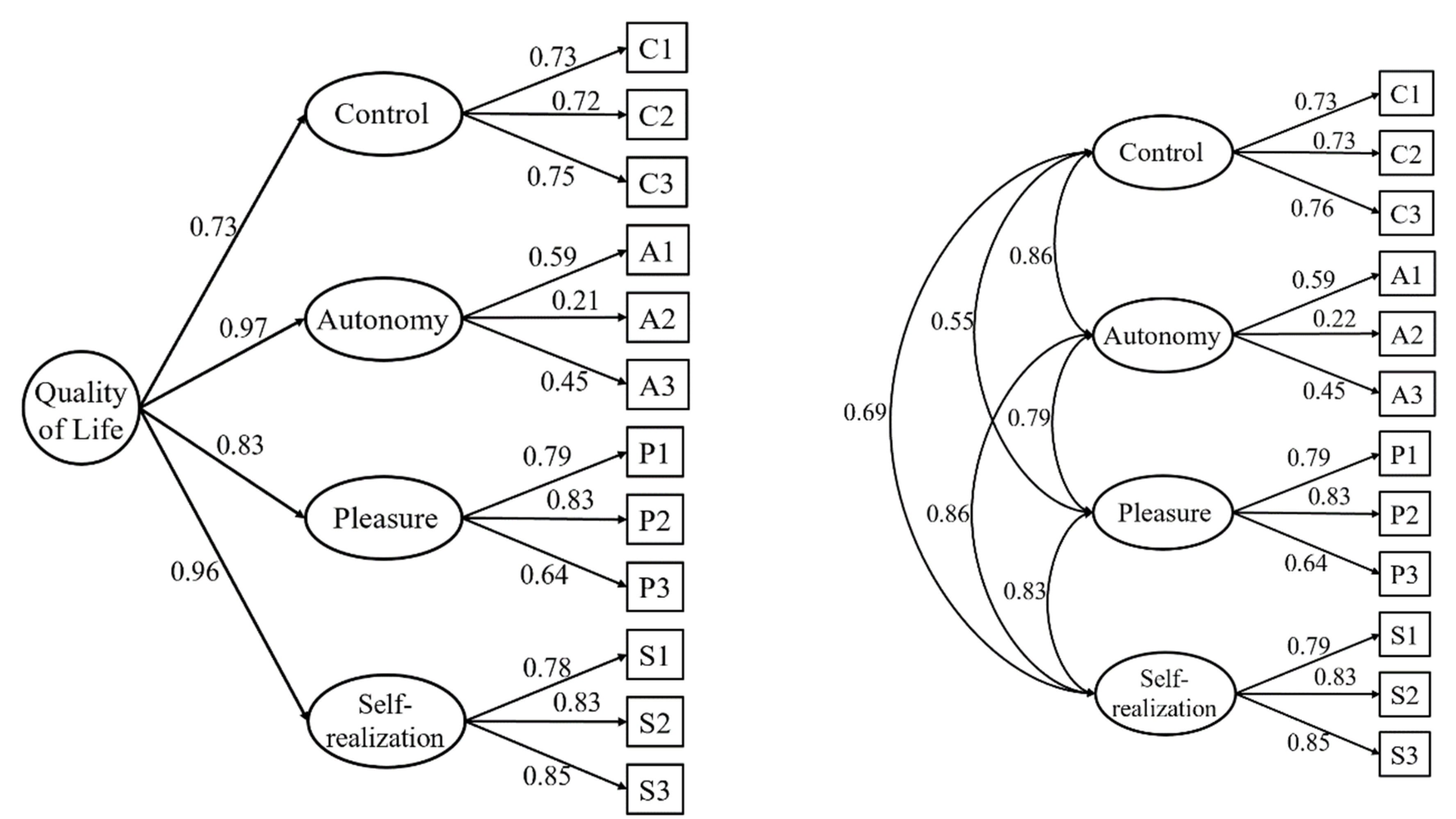
3.1. Factor Structure
- (1)
- One-factor model, found in Kerry [18].
- (2)
- Two-factor model (control/autonomy and self-realization/pleasure), supported, for example, by Borrat-Besson et al. [16].
- (3)
- Three-factor model (control/autonomy, self-realization, and pleasure), found, for example, in Stoner et al. [15].
- (4)
- Four-factor model (control, autonomy, self-realization, and pleasure), theoretically proposed during the scale development.
- (5)
- Four-factor model with a second-order factor (QoL), also based on the theory underlying the scale development.
3.2. Internal Consistency
3.3. External Validity
3.4. Measurement Invariance
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Higgs, P.; Hyde, M.; Wiggins, R.; Blane, D. Researching quality of life in early old age: The importance of the sociological dimension. Soc. Policy Adm. 2003, 37, 239–252. [Google Scholar] [CrossRef]
- WHOQOL Group. The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Hyde, M.; Wiggins, R.D.; Higgs, P.; Blane, D.B. A measure of quality of life in early old age: The theory, development and properties of a needs satisfaction model (CASP-19). Aging Ment. Health 2003, 7, 186–194. [Google Scholar] [CrossRef]
- Bowling, A. Measuring Health. A Review of Quality of Life Measurement Scales, 2nd ed.; Open University Press: Milton Keynes, UK, 1997. [Google Scholar]
- De Leval, N. Quality of life and depression: Symmetry concepts? Qual. Life Res. 1999, 8, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Mozes, B.; Maor, Y.; Shnueli, A. Do we know what global ratings of health related quality of life measure? Qual. Life Res. 1999, 8, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.E. Quality of life: A review. Educ. Ageing 2000, 15, 419–435. [Google Scholar]
- Maslow, A.H. Toward a Psychology of Being, 2nd ed.; Van Nostrand Reinhold: New York, NY, USA, 1968. [Google Scholar]
- Wiggins, R.D.; Netuveli, G.; Hyde, M.; Higgs, P.; Blane, D. The evaluation of a self-enumerated scale of quality of life (CASP-19) in the context of research on ageing: A combination of exploratory and confirmatory. Soc. Indic. Res. 2008, 89, 61–77. [Google Scholar] [CrossRef]
- Eid, M.; Diener, E. Global judgements of subjective well-being: Situational variability and long term stability. Soc. Indic. Res. 2004, 65, 245–277. [Google Scholar] [CrossRef]
- Pérez-Rojo, G.; Martín, N.; Noriega, C.; López, J. Psychometric properties of the CASP-12 in a Spanish older community dwelling sample. Aging Ment. Health 2018, 22, 700–708. [Google Scholar] [CrossRef]
- Heravi-Karimooi, M.; Rejeh, N.; Garshasbi, A.; Montazeri, A.; Bandari, R. Psychometric properties of the Persian version of the quality of life in early old age (CASP-19). Iran. J. Psychiatry Behav. Sci. 2018, 12, e8378. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.R.; Netuveli, G.; Blane, D.; Peasy, A.; Malyutina, S.; Simonova, G.; Kubinova, R.; Pajak, A.; Croezen, S.; Bobak, M.; et al. Psychometric properties and confirmatory factor analysis of the CASP-19, a measure of quality of life in early old age: The HAPIEE study. Aging Ment. Health 2015, 19, 595–609. [Google Scholar] [CrossRef] [PubMed]
- Neri, A.L.; Borin, F.S.A.; Batistoni, A.A.T.; Cachioni, M.; Rabelo, D.F.; Fontes, A.P.; Yassuda, M.S. New semantic-cultural validation and psychometric study of the CASP-19 scale in adult and elderly Brazilians. Cad. Saude Publica 2018, 34, e00181417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoner, C.R.; Orrell, M.; Spector, A. The psychometric properties of the Control, Autonomy, Self-realisation and Pleasure Scale (CASP-19) for older adults with dementia. Aging Ment. Health 2019, 23, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Borrat-Besson, C.; Ryser, V.A.; Gonçalves, J. An Evaluation of the CASP-12 Scale Used in the Survey of Ageing and Retirement in Europe (SHARE) to Measure Quality of Life Among People Aged 50+; FORS Working Paper Series: Paper 2015–4; FORS: Lausanne, Switzerland, 2015. [Google Scholar]
- Towers, A.; Yeung, P.; Stevenson, B.; Stephens, C.; Alpass, F. Quality of life in indigenous and non-indigenous older adults: Assessing the CASP-12 factor structure and identifying a brief CASP-3. Qual. Life Res. 2015, 24, 193–203. [Google Scholar] [CrossRef]
- Kerry, M.J. Bifactor model of the CASP-12’s general factor for measuring quality of life in older patients. J. Patient Rep. Outcomes 2018, 2, 1–57. [Google Scholar] [CrossRef]
- Hamren, K.; Chungkham, H.S.; Hyde, M. Religion, spirituality, social support and quality of life: Measurement and predictors CASP-12(v2) amongst other Ethiopians living in Addis Ababa. Aging Ment. Health 2015, 19, 610–621. [Google Scholar] [CrossRef]
- Rodríguez-Blázquez, C.; Ribeiro, O.; Ayala, A.; Teixeira, L.; Araujo, L.; Forjaz, M.J. Psychometric properties of the CASP-12 scale in Portugal: An analysis using SHARE data. Int. J. Environ. Res. Public Health 2020, 17, 6610. [Google Scholar] [CrossRef]
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE). Wave 7, Release version 7.1.1; SHARE-ERIC: Munich, Germany, 2020. [Google Scholar] [CrossRef]
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S.; SHARE Central Coordination Team. Data Resource Profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef]
- Bergmann, M.; Scherpenzeel, A.; Börsch-Supan, A. (Eds.) SHARE Wave 7 Methodology: Panel Innovations and Life Histories; MEA, Max Planck Institute for Social Law and Social Policy: Munich, Germany, 2019. [Google Scholar]
- Prince, M.J.; Reischies, F.; Beekman, A.T.F.; Fuhrer, R.; Jonker, C.; Kivela, S.L.; Lawlor, B.A.; Lobo, A.; Magnusson, H.; Fichter, M.; et al. Development of the EURO-D scale—A European Union initiative to compare symptoms of depression in 14 European centres. Br. J. Psychiatry 1999, 174, 330–338. [Google Scholar] [CrossRef]
- Mehrbrodt, T.; Gruber, S.; Wagner, M. Scales and Multi-Item Indicators; Center for the Economics of Aging (MEA): Munich, Germany, 2019. [Google Scholar]
- Ware, J.E.; Gandek, B. Overview of the SF-36 health survey and the international quality of life assessment (IQOLA) project. J. Clin. Epidemiol. 1998, 51, 903–912. [Google Scholar] [CrossRef]
- Diedenhofen, B.; Musch, S. Cocron: A web interface and R package for the statistical comparison of Cronbach’s alpha coefficients. Int. J. Internet Sci. 2016, 11, 51–60. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Finney, S.J.; DiStefano, C. Nonnormal and categorical data in structural equation modeling. In Structural Equation Modeling: A Second Course; Hancock, G.R., Mueller, R.O., Eds.; IAP Information Age Publishing: Charlotte, NC, USA, 2013; pp. 439–492. [Google Scholar]
- Li, C.H. Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behav. Res. Methods 2016, 48, 936–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Marsh, H.W.; Hau, K.T.; Wen, Z. In search of golden rules: Comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) findings. Struct Equ. Model. 2004, 11, 320–341. [Google Scholar] [CrossRef]
- Van de Schoot, R.; Lugtig, P.; Hox, J. A checklist for testing measurement invariance. Eur. J. Dev. Psychol. 2012, 9, 486–492. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equ. Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Little, T.D. Mean and covariance structures (MACS) analyses of cross-cultural data: Practical and theoretical issues. Multivar. Behav. Res. 1997, 32, 53–76. [Google Scholar] [CrossRef]
- Sim, J.; Bartlam, B.; Bernard, M. The CASP-19 as a measure of quality of life in old age: Evaluation of its use in a retirement community. Qual. Life Res. 2011, 20, 997–1004. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The support of autonomy and the control of behavior. J. Pers Soc. Psychol. 1987, 57, 1024–1037. [Google Scholar] [CrossRef]
- Baltes, P.B.; Smith, J. New frontiers in the future of aging: From successful aging of the young old to the dilemmas of the fourth age. Gerontology 2003, 49, 123–135. [Google Scholar] [CrossRef]
- United Nations Population Division. World Population Ageing 1950–2050; United Nations, Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2002. [Google Scholar]
- Angelini, V.; Cavapozzi, D.; Corazzini, L.; Paccagnella, O. Age, health and life satisfaction among older Europeans. Soc. Indic. Res. 2012, 105, 293–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez, M.; Tomás, J.M.; Sancho, P.; Galiana, L.; Francisco, E. Perception of quality of life in an elderly Angolan sample. Rev. Psicol. Soc. 2014, 29, 346–370. [Google Scholar] [CrossRef]
- Gwozdz, W.; Sousa-Poza, A. Ageing, health and life satisfaction of the oldest old: An analysis for Germany. Soc. Indic. Res. 2010, 97, 397–417. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.; Borchelt, M.; Maier, H.; Jopp, D. Health and well-being in the young old and oldest old. J. Soc. Issues 2002, 58, 715–732. [Google Scholar] [CrossRef]
- Berg, A.I.; Hoffman, L.; Hassing, L.B.; McClearn, G.E.; Johansson, B. What matters, and what matters most, for change in life satisfaction in the oldest-old? A study over 6 years among individuals 80+. Aging Ment. Health 2009, 13, 191–201. [Google Scholar] [CrossRef] [Green Version]
- Enkvist, Å.; Ekström, H.; Elmståhl, S. What factors affect life satisfaction (LS) among the oldest-old? Arch. Gerontol. Geriatr. 2012, 54, 140–145. [Google Scholar] [CrossRef]
- McCrory, C.; Leahy, S.; Mcgarrigle, C. What factors are associated with change in older people’s quality of life? In The over 50s in a Changing Ireland. Economic Circumstances, Health and Well-Being; Nolan, A., O’Regan, C., Dooley, C., Wallace, D., Hever, A., Cronin, H., Hudson, E., Kenny, R.A., Eds.; The Irish Longitudinal Study on Ageing: Dublin, Ireland, 2014; pp. 153–186. Available online: https://tilda.tcd.ie/publications/reports/pdf/w2-key-findings-report/Wave2-Key-Findings-Report.pdf (accessed on 23 May 2021).
- Tampubolon, G. Delineating the third age: Joint models of older people’s quality of life and attrition in Britain 2002–2010. Aging Ment. Health 2015, 19, 576–583. [Google Scholar] [CrossRef] [Green Version]
- Zaninotto, P.; Falaschetti, E.; Sacker, A. Age trajectories of quality of life among older adults: Results from the English longitudinal study of Ageing. Qual. Life Res. 2009, 18, 1301–1309. [Google Scholar] [CrossRef]
- Ward, M.; McGarridge, C.A.; Kenny, R.A. More than health: Quality of life trajectories among older adults—Findings from The Irish Longitudinal Study of Ageing (TILDA). Qual. Life Res. 2019, 28, 429–439. [Google Scholar] [CrossRef]
- Ponte, C.; Almeida, V.; Fernandes, L. Suicidal ideation, depression and quality of life in the elderly: Study in a gerontopsychiatric consultation. Span. J. Psychol. 2014, 17, E14. [Google Scholar] [CrossRef] [PubMed]
- Unalan, D.; Gocer, S.; Basturk, M.; Baydur, H.; Ozturk, A. Coincidence of low social support and high depressive score on quality of life in elderly. Eur. Geriatr. Med. 2015, 6, 319–324. [Google Scholar] [CrossRef]
- Portellano-Ortiz, C.; Garre-Olmo, J.; Calvó-Perxas, L.; Conde-Sala, J.L. Depression and variables associated with quality of life in people over 65 in Spain and Europe. Data from SHARE 2013. Eur. J. Psychiatry 2018, 32, 122–131. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Model | χ2 | df | p | RMSEA | 90%CI | CFI | SRMR | Δχ2 | df | p | ΔCFI |
|---|---|---|---|---|---|---|---|---|---|---|---|
| One-factor model | 48,906.4 | 54 | <0.001 | 0.123 | 0.123–0.124 | 0.903 | 0.062 | - | - | - | - |
| Two-factor model | 28,867.4 | 53 | <0.001 | 0.096 | 0.095–0.097 | 0.943 | 0.048 | - | - | - | - |
| Three-factor model | 21,564.1 | 51 | <0.001 | 0.084 | 0.083–0.085 | 0.957 | 0.044 | - | - | - | - |
| Four-factor model | 16,443.1 | 48 | <0.001 | 0.076 | 0.075–0.077 | 0.968 | 0.038 | - | - | - | - |
| Second-order model | 19,963.1 | 50 | <0.001 | 0.082 | 0.081–0.083 | 0.961 | 0.043 | - | - | - | - |
| Measurement invariance | |||||||||||
| Configural | 14,656.3 | 144 | <0.001 | 0.071 | 0.070–0.072 | 0.969 | 0.037 | - | - | - | - |
| Metric | 13,461.7 | 160 | <0.001 | 0.065 | 0.064–0.066 | 0.972 | 0.038 | 887.2 | 16 | <0.001 | 0.003 |
| Scalar | 19,973.2 | 200 | <0.001 | 0.071 | 0.070–0.072 | 0.958 | 0.041 | 7233.4 | 40 | <0.001 | 0.014 |
| Modified scalar | 17,266.5 | 198 | <0.001 | 0.066 | 0.065–0.067 | 0.964 | 0.040 | 4607.9 | 38 | <0.001 | 0.008 |
| Item | Mean | SD | rit |
|---|---|---|---|
| Control 1 | 2.53 | 1.04 | 0.48 |
| Control 2 | 2.79 | 0.99 | 0.58 |
| Control 3 | 3.14 | 0.95 | 0.52 |
| Autonomy 1 | 3.18 | 0.89 | 0.13 |
| Autonomy 2 | 3.09 | 0.96 | 0.20 |
| Autonomy 3 | 2.61 | 1.10 | 0.28 |
| Pleasure 1 | 3.47 | 0.77 | 0.29 |
| Pleasure 2 | 3.47 | 0.79 | 0.32 |
| Pleasure 3 | 3.37 | 0.76 | 0.20 |
| Self-realization 1 | 3.06 | 0.87 | 0.39 |
| Self-realization 2 | 3.03 | 0.89 | 0.48 |
| Self-realization 3 | 2.98 | 0.91 | 0.48 |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | |
|---|---|---|---|---|---|---|---|
| (1) Control | 1 | ||||||
| (2) Autonomy | 0.442 | 1 | |||||
| (3) Self-realization | 0.365 | 0.334 | 1 | ||||
| (4) Pleasure | 0.528 | 0.391 | 0.609 | 1 | |||
| (5) CASP-12 | 0.789 | 0.694 | 0.732 | 0.836 | 1 | ||
| (6) Life satisfaction | 0.406 | 0.366 | 0.472 | 0.510 | 0.573 | 1 | |
| (7) Depression | −0.442 | −0.257 | −0.422 | −0.498 | −0.524 | −0.416 | 1 |
| (8) Self-perceived health | 0.405 | 0.233 | 0.304 | 0.494 | 0.479 | 0.361 | −0.439 |
| Group 2 vs. 1 | Group 3 vs. 1 | |||||
|---|---|---|---|---|---|---|
| Factor | Difference | p | Cohen’s d | Difference | p | Cohen’s d |
| Control | −0.514 | <0.001 | 0.471 | −0.950 | <0.001 | 0.811 |
| Autonomy | 0.196 | <0.001 | 0.234 | 0.668 | <0.001 | 0.655 |
| Self-realization | −0.628 | <0.001 | 0.498 | −1.111 | <0.001 | 0.478 |
| Pleasure | −0.365 | <0.001 | 0.290 | −0.598 | <0.001 | 0.857 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliver, A.; Sentandreu-Mañó, T.; Tomás, J.M.; Fernández, I.; Sancho, P. Quality of Life in European Older Adults of SHARE Wave 7: Comparing the Old and the Oldest-Old. J. Clin. Med. 2021, 10, 2850. https://doi.org/10.3390/jcm10132850
Oliver A, Sentandreu-Mañó T, Tomás JM, Fernández I, Sancho P. Quality of Life in European Older Adults of SHARE Wave 7: Comparing the Old and the Oldest-Old. Journal of Clinical Medicine. 2021; 10(13):2850. https://doi.org/10.3390/jcm10132850
Chicago/Turabian StyleOliver, Amparo, Trinidad Sentandreu-Mañó, José M. Tomás, Irene Fernández, and Patricia Sancho. 2021. "Quality of Life in European Older Adults of SHARE Wave 7: Comparing the Old and the Oldest-Old" Journal of Clinical Medicine 10, no. 13: 2850. https://doi.org/10.3390/jcm10132850