
The Effect of Intraoperative Fluid Management According to Stroke Volume Variation on Postoperative Bowel Function Recovery in Colorectal Cancer Surgery

 , ,
, ,
Abstract
:1. Introduction
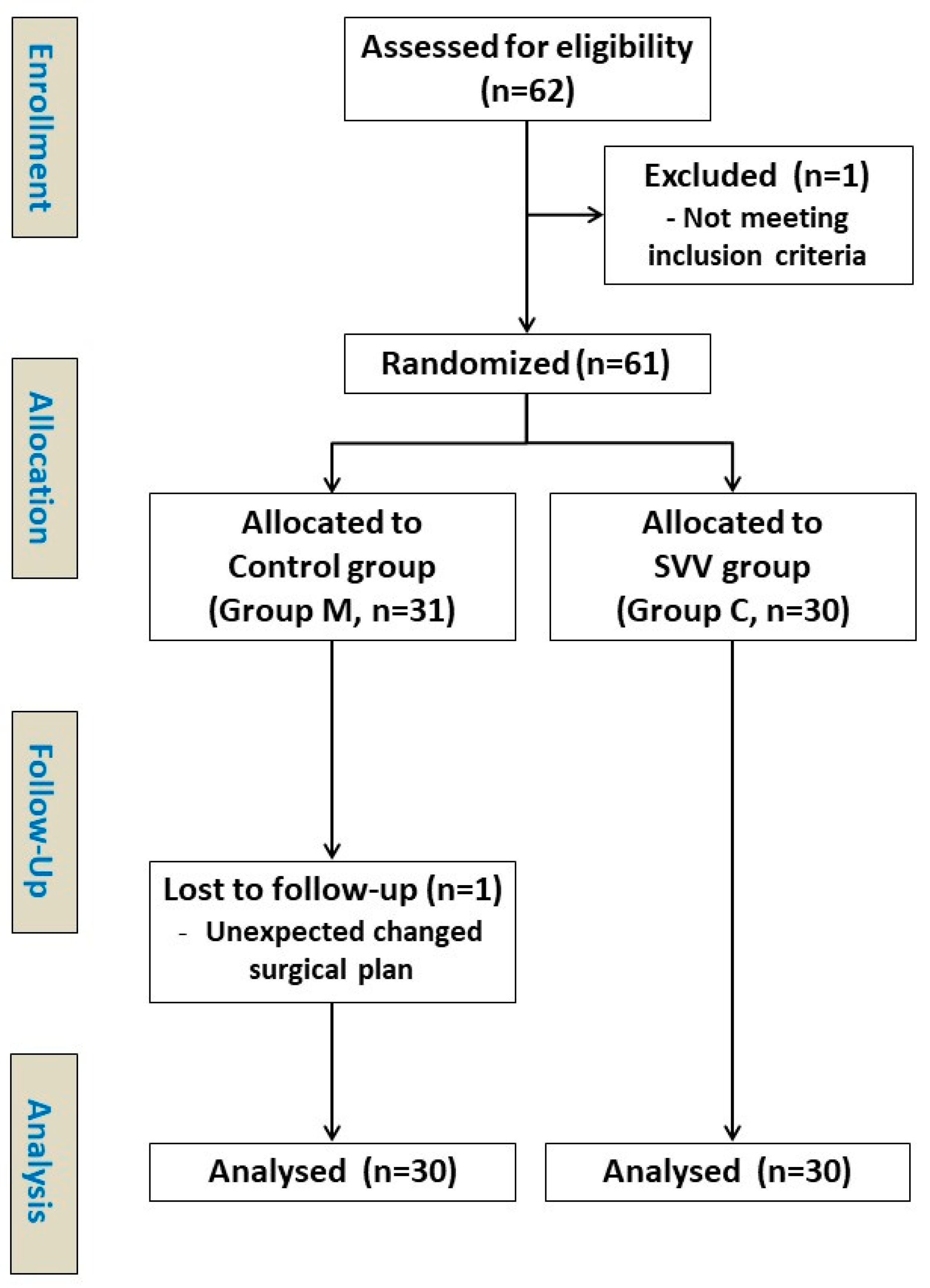
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bamboat, Z.M.; Bordeianou, L. Perioperative fluid management. Clin. Colon Rectal Surg. 2009, 22, 28–33. [Google Scholar] [CrossRef]
- Bleier, J.I.; Aarons, C.B. Perioperative fluid restriction. Clin. Colon Rectal. Surg. 2013, 26, 197–202. [Google Scholar]
- Patel, S.; Lutz, J.M.; Panchagnula, U.; Bansal, S. Anesthesia and perioperative management of colorectal surgical patients—Specific issues (part 2). J. Anaesthesiol. Clin. Pharmacol. 2012, 28, 304–313. [Google Scholar] [CrossRef]
- Feissel, M.; Mangin, I.; Ruyer, O.; Faller, J.-P.; Michard, F.; Teboul, J.-L. Respiratory changes in aortic blood velocity as an indicator of fluid responsiveness in ventilated patients with septic shock. Chest 2001, 119, 867–873. [Google Scholar] [CrossRef]
- Bendjelid, K.; Romand, J.-A. Fluid responsiveness in mechanically ventilated patients: A review of indices used in intensive care. Intensive Care Med. 2003, 29, 352–360. [Google Scholar] [CrossRef]
- Michard, F.; Teboul, J.L. Predicting fluid responsiveness in icu patients: A critical analysis of the evidence. Chest 2002, 121, 2000–2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahner, D.; Kabon, B.; Marschalek, C.; Chiari, A.; Pestel, G.; Kaider, A.; Fleischmann, E.; Hetz, H. Evaluation of stroke volume variation obtained by arterial pulse contour analysis to predict fluid responsiveness intraoperatively. Br. J. Anaesthesiol. 2009, 103, 346–351. [Google Scholar] [CrossRef] [Green Version]
- Derichard, A.; Robin, E.; Tavernier, B.; Costecalde, M.; Fleyfel, M.; Onimus, J.; Lebuffe, G.; Chambon, J.-P.; Vallet, B. Automated pulse pressure and stroke volume variations from radial artery: Evaluation during major abdominal surgery. Br. J. Anaesthesiol. 2009, 103, 678–684. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Lu, B.; Sheng, X.; Jin, N. Accuracy of stroke volume variation in predicting fluid responsiveness: A systematic review and meta-analysis. J. Anesth. 2011, 25, 904–916. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Lin, F.-Q.; Fu, S.-K.; Chen, G.-Q.; Yang, X.-H.; Zhu, C.-Y.; Zhang, L.-J.; Li, Q. Stroke volume variation for prediction of fluid responsiveness in patients undergoing gastrointestinal surgery. Int. J. Med. Sci. 2013, 10, 148–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asklid, D.; Segelman, J.; Gedda, C.; Hjern, F.; Pekkari, K.; Gustafsson, U. The impact of perioperative fluid therapy on short-term outcomes and 5-year survival among patients undergoing colorectal cancer surgery—A prospective cohort study within an ERAS protocol. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 1433–1439. [Google Scholar] [CrossRef]
- Xu, C.; Peng, J.; Liu, S.; Huang, Y.; Guo, X.; Xiao, H.; Qi, D. Goal-directed fluid therapy versus conventional fluid therapy in colorectal surgery: A meta analysis of randomized controlled trials. Int. J. Surg. 2018, 56, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.H.; Lee, K.Y.; Lee, K.Y.; Min, B.S.; Yoo, Y.C. Maintaining optimal surgical conditions with low insufflation pressures is possible with deep neuromuscular blockade during laparoscopic colorectal surgery: A prospective, randomized, double-blind, parallel-group clinical trial. Medicine (Baltimore) 2016, 95, e2920. [Google Scholar] [CrossRef]
- Rex, S.; Brose, S.; Metzelder, S.; Hüneke, R.; Schälte, G.; Autschbach, R.; Rossaint, R.; Buhre, W. Prediction of fluid responsiveness in patients during cardiac surgery. Br. J. Anaesthesiol. 2004, 93, 782–788. [Google Scholar] [CrossRef] [Green Version]
- Marx, G.; Cope, T.; McCrossan, L.; Swaraj, S.; Cowan, C.; Mostafa, S.M.; Wenstone, R.; Leuwer, M. Assessing fluid responsiveness by stroke volume variation in mechanically ventilated patients with severe sepsis. Eur. J. Anaesthesiol. 2004, 21, 132–138. [Google Scholar] [CrossRef]
- Opdam, H.I.; Wan, L.; Bellomo, R. A pilot assessment of the flotrac cardiac output monitoring system. Intensive Care Med. 2007, 33, 344–349. [Google Scholar] [CrossRef]
- Penttilä, J.; Snapir, A.; Kentala, E.; Koskenvuo, J.; Posti, J.; Scheinin, M.; Scheinin, H.; Kuusela, T. Estimation of cardiac output in a pharmacological trial using a simple method based on arterial blood pressure signal waveform: A comparison with pulmonary thermodilution and echocardiographic methods. Eur. J. Clin. Pharmacol. 2006, 62, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Michard, F. Changes in arterial pressure during mechanical ventilation. Anesthesiology 2005, 103, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Campbell, I.T.; Baxter, J.N.; Tweedie, I.E.; Taylor, G.T.; Keens, S.J. Iv fluids during surgery. Br. J. Anaesthesiol. 1990, 65, 726–729. [Google Scholar] [CrossRef]
- Joosten, A.; Delaporte, A.; Ickx, B.; Touihri, K.; Stany, I.; Barvais, L.; Van Obbergh, L.; Loi, P.; Rinehart, J.; Cannesson, M.; et al. Crystalloid versus colloid for intraoperative goal-directed fluid therapy using a closed-loop system: A randomized, double-blinded, controlled trial in major abdominal surgery. Anesthesiology 2018, 128, 55–66. [Google Scholar] [CrossRef]
- Myburgh, J.A. Fluid resuscitation in acute medicine: What is the current situation? J. Intern. Med. 2014, 277, 58–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandstrup, B.; Tønnesen, H.; Beier-Holgersen, R.; Hjortsø, E.; Ørding, H.; Lindorff-Larsen, K.; Rasmussen, M.S.; Lanng, C.; Wallin, L.; Iversen, L.H.; et al. Effects of intravenous fluid restriction on postoperative complications: Comparison of two perioperative fluid regimens: A randomized assessor-blinded multicenter trial. Ann. Surg. 2003, 238, 641–648. [Google Scholar] [CrossRef]
- Nisanevich, V.; Felsenstein, I.; Almogy, G.; Weissman, C.; Einav, S.; Matot, I. Effect of intraoperative fluid management on outcome after intraabdominal surgery. Anesthesiology 2005, 103, 25–32. [Google Scholar] [CrossRef]
- Kumar, L.; Rajan, S.; Baalachandran, R. Outcomes associated with stroke volume variation versus central venous pressure guided fluid replacements during major abdominal surgery. J. Anaesthesiol. Clin. Pharmacol. 2016, 32, 182–186. [Google Scholar] [CrossRef]
- Lilot, M.; Ehrenfeld, J.M.; Lee, C.; Harrington, B.; Cannesson, M.; Rinehart, J. Variability in practice and factors predictive of total crystalloid administration during abdominal surgery: Retrospective two-centre analysis †. Br. J. Anaesthesiol. 2015, 114, 767–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thacker, J.K.; Mountford, W.K.; Ernst, F.R.; Krukas, M.R.; Mythen, M.M. Perioperative fluid utilization variability and association with outcomes: Considerations for enhanced recovery efforts in sample us surgical populations. Ann. Surg. 2016, 263, 502–510. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M.A.; Cecconi, M.; Rhodes, A. A systematic review and meta-analysis on the use of preemptive hemodynamic intervention to improve postoperative outcomes in moderate and high-risk surgical patients. Anesth. Analg. 2011, 112, 1392–1402. [Google Scholar] [CrossRef]
- Pearse, R.M.; Harrison, D.A.; MacDonald, N.; Gillies, M.A.; Blunt, M.; Ackland, G.; Grocott, M.P.; Ahern, A.; Griggs, K.; Scott, R.; et al. Effect of a perioperative, cardiac output-guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: A randomized clinical trial and systematic review. JAMA 2014, 311, 2181–2190. [Google Scholar] [CrossRef]
- Miller, T.E.; Roche, A.M.; Gan, T.J. Poor adoption of hemodynamic optimization during major surgery: Are we practicing substandard care? Anesth. Analg. 2011, 112, 1274–1276. [Google Scholar] [CrossRef] [PubMed]
- Joosten, A.; Alexander, B.; Delaporte, A.; Lilot, M.; Rinehart, J.; Cannesson, M. Perioperative goal directed therapy using automated closed-loop fluid management: The future? Anestezjol. Intensive Ter. 2015, 47, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Goepfert, M.S.; Richter, H.P.; Eulenburg, C.Z.; Gruetzmacher, J.; Rafflenbeul, E.; Roeher, K.; von Sandersleben, A.; Diedrichs, S.; Reichenspurner, H.; Goetz, A.E.; et al. Individually optimized hemodynamic therapy reduces complications and length of stay in the intensive care unit: A prospective, randomized controlled trial. Anesthesiology 2013, 119, 824–836. [Google Scholar] [CrossRef] [Green Version]
- Cannesson, M.; Ramsingh, D.; Rinehart, J.; Demirjian, A.; Vu, T.; Vakharia, S.; Imagawa, D.; Yu, Z.; Greenfield, S.; Kain, Z. Perioperative goal-directed therapy and postoperative outcomes in patients undergoing high-risk abdominal surgery: A historical-prospective, comparative effectiveness study. Crit. Care 2015, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallet, B.; Blanloeil, Y.; Cholley, B.; Orliaguet, G.; Pierre, S.; Tavernier, B. Guidelines for perioperative haemodynamic optimization. Ann. Fr. Anesth. Reanim. 2013, 32, e151–e158. [Google Scholar] [CrossRef] [PubMed]
- Cannesson, M.; Pestel, G.; Ricks, C.; Hoeft, A.; Perel, A. Hemodynamic monitoring and management in patients undergoing high risk surgery: A survey among North American and European anesthesiologists. Crit. Care 2011, 15, R197. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Control Group (N = 30) | SVV Group (N = 30) | p-Value | |
|---|---|---|---|
| Age (year) | 57.9 (6.1) | 60.3 (8.9) | 0.077 |
| Gender (M/F) | 17 (13) | 24 (6) | 0.095 |
| Height (cm) | 163.0 (9.3) | 164.6 (6.7) | 0.722 |
| Weight (kg) | 63.6 (15.5) | 65.5 (12.8) | 0.829 |
| ASA physical status | 0.713 | ||
| 1 | 12 | 9 | |
| 2 | 12 | 15 | |
| 3 | 6 | 6 | |
| Comorbidity | |||
| Hypertension | 12 | 14 | 0.795 |
| Diabetes Mellitus | 3 | 4 | >0.999 |
| Cardiovascular | 4 | 1 | 0.353 |
| Respiratory | 5 | 5 | >0.999 |
| Neurologic | 1 | 0 | >0.999 |
| Liver | 0 | 1 | >0.999 |
| Kidney | 1 | 4 | 0.353 |
| Anesthetic duration (min) | 285 (66.5) | 261.2 (88.9) | 0.074 |
| Surgical duration (min) | 239.3 (59.1) | 218.2 (83.3) | 0.056 |
| Surgical types | 0.360 | ||
| Laparoscopic | 21 | 25 | |
| Open | 9 | 5 | |
| Surgical procedures | 0.691 | ||
| Right hemicolectomy | 7 | 8 | |
| Anterior resection | 9 | 12 | |
| Low anterior resection | 13 | 8 | |
| Left hemicolectomy | 0 | 1 | |
| Total colectomy | 1 | 1 | |
| Patient-controlled analgesia (via) | >0.999 | ||
| Intravenous | 27 | 27 | |
| Epidural | 3 | 3 |
| Control Group (N = 30) | SVV Group (N = 30) | p-Value | |
|---|---|---|---|
| Initial vital signs | |||
| HR (BPM) | 71.6 (11.8) | 70.3 (11.3) | 0.834 |
| MBP (mmHg) | 82.4 (13.7) | 86.5 (12.8) | 0.181 |
| SpO2 (%) | 100 (0) | 100 (0) | >0.999 |
| Vasopressor administration | 15 | 15 | >0.999 |
| Ephedrine | 7 | 8 | |
| Phenylephrine | 7 | 7 | |
| Norepinephrine | 1 | 0 | |
| Bradycardia event | 1 | 0 | >0.999 |
| Laboratory values at baseline | |||
| PH | 7.443 (0.03) | 7.435 (0.04) | 0.315 |
| PO2 | 194.0 (43.4) | 194.1 (54.3) | 0.806 |
| PCO2 | 33.3 (4.8) | 34.6 (4.0) | 0.126 |
| Hematocrit | 11.3 (1.6) | 11.6 (1.5) | 0.246 |
| Lactate | 0.83 (0.2) | 0.80 (0.2) | 0.414 |
| Laboratory values at surgery end | |||
| PH | 7.428 (0.10) | 7.401 (0.04) | 0.305 |
| PO2 | 175 (31.5) | 184.1 (31.1) | 0.265 |
| PCO2 | 34.9 (3.8) | 37.1 (4.4) | 0.054 |
| Hematocrit | 11.3 (1.4) | 11.4 (1.4) | 0.777 |
| Lactate | 0.90 (0.3) | 0.85 (0.2) | 0.419 |
| Input | |||
| Crystalloid (mL) | 1615.8 (814.8) | 806.0 (898.6) | 0.033 |
| Colloid (mL) | 616.7 (313.0) | 851.2 (461.8) | <0.001 |
| RBC (mL) | 41.7 (160.9) | 16.7 (57.7) | 0.901 |
| Output | |||
| Urine (mL) | 397.0 (311.1) | 459.8 (403.7) | 0.545 |
| Bleeding (mL) | 159.0 (278.1) | 93.3 (182.7) | 0.078 |
| Control Group (N = 30) | SVV Group (N = 30) | p-Value | |
|---|---|---|---|
| Post-Anesthetic Care Unit | |||
| Numeric Rating Scale (Pain) | 4.3 (1.2) | 3.3 (1.1) | 0.001 |
| Morphine equivalent dose (mg) | 32.2 (38.8) | 16.7 (27.3) | 0.108 |
| Antiemetic requirement | 1 | 0 | 0.483 |
| Stay duration (min) | 45.1 (11.7) | 40.0 (10.5) | 0.077 |
| Postoperative 1–6 h | |||
| Numeric Rating Scale (Pain) | 4.5 (1.1) | 3.8 (1.0) | 0.033 |
| Morphine equivalent dose (mg) | 60.0 (46.8) | 46.7 (41.4) | 0.285 |
| Antiemetic requirement | 14 | 20 | 0.192 |
| Postoperative 6–24 h | |||
| Numeric Rating Scale (Pain) | 5.1 (1.7) | 4.1 (1.5) | 0.018 |
| Morphine equivalent dose (mg) | 101.5 (86.6) | 56.7 (58.3) | 0.025 |
| Antiemetic requirement | 15 | 19 | 0.435 |
| Postoperative 24–48 h | |||
| Numeric Rating Scale (Pain) | 4.2 (1.4) | 3.0 (1.1) | 0.002 |
| Morphine equivalent dose (mg) | 61.7 (71.5) | 28.3 (40.9) | 0.061 |
| Antiemetic requirement | 2 | 1 | >0.999 |
| Control Group (N = 30) | SVV Group (N = 30) | p-Value | |
|---|---|---|---|
| Bowel movement recovery | |||
| Sips of water time (h) | 42.4 (11.6) | 37.3 (11.7) | 0.051 |
| Soft diet time (h) | 85.1 (16.8) | 67.6 (17.1) | <0.001 |
| Gas passing time (h) | 85.3 (18.5) | 77.8 (36.6) | 0.034 |
| Postoperative Complications | |||
| Total cases | 15 | 22 | 0.110 |
| Fever (>38 °C) | 12 | 20 | 0.069 |
| Intra-abdominal infection | 1 | 1 | >0.999 |
| Respiratory | 0 | 2 | >0.999 |
| Cardiovascular | 0 | 1 | >0.999 |
| Ileus | 1 | 1 | >0.999 |
| Wound problem | 1 | 0 | >0.999 |
| Anastomosis leakage | 0 | 1 | >0.999 |
| Dyspepsia | 0 | 1 | >0.999 |
| Kidney injury | 4 | 0 | 0.112 |
| Reoperation | 0 | 1 | >0.999 |
| Postoperative length of stay in hospital | 8.1 (5.7) | 7.9 (3.8) | 0.925 |
| Postoperative intensive care unit transfer | 3 | 0 | 0.237 |
| Death | 1 | 1 | >0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.-Y.; Yoo, Y.-C.; Cho, J.-S.; Lee, W.; Kim, J.-Y.; Kim, M.-H. The Effect of Intraoperative Fluid Management According to Stroke Volume Variation on Postoperative Bowel Function Recovery in Colorectal Cancer Surgery. J. Clin. Med. 2021, 10, 1857. https://doi.org/10.3390/jcm10091857
Lee K-Y, Yoo Y-C, Cho J-S, Lee W, Kim J-Y, Kim M-H. The Effect of Intraoperative Fluid Management According to Stroke Volume Variation on Postoperative Bowel Function Recovery in Colorectal Cancer Surgery. Journal of Clinical Medicine. 2021; 10(9):1857. https://doi.org/10.3390/jcm10091857
Chicago/Turabian StyleLee, Ki-Young, Young-Chul Yoo, Jin-Sun Cho, Wootaek Lee, Ji-Young Kim, and Myoung-Hwa Kim. 2021. "The Effect of Intraoperative Fluid Management According to Stroke Volume Variation on Postoperative Bowel Function Recovery in Colorectal Cancer Surgery" Journal of Clinical Medicine 10, no. 9: 1857. https://doi.org/10.3390/jcm10091857