
Accuracy of Computer-Assisted Dynamic Navigation in Implant Placement with a Fully Digital Approach: A Prospective Clinical Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- Submission of written informed consent;
- Restoration of at least one missing tooth using an implant;
- At least six residual teeth in the affected jaw.
- People under 18 years of age or people without legal capacity;
- The use of a reference marker for implant placement is not possible (restricted mouth opening);
- Necessary additional augmentation requirements;
- Heavy smoker (>10 cigarettes/day);
- Immediate implant placements;
- Intake of bisphosphonates;
- Pregnant women;
- Alcohol and/or drug abuse;
- Patients with infectious diseases, such as hepatitis or AIDS;
- Poorly controlled diabetes mellitus.
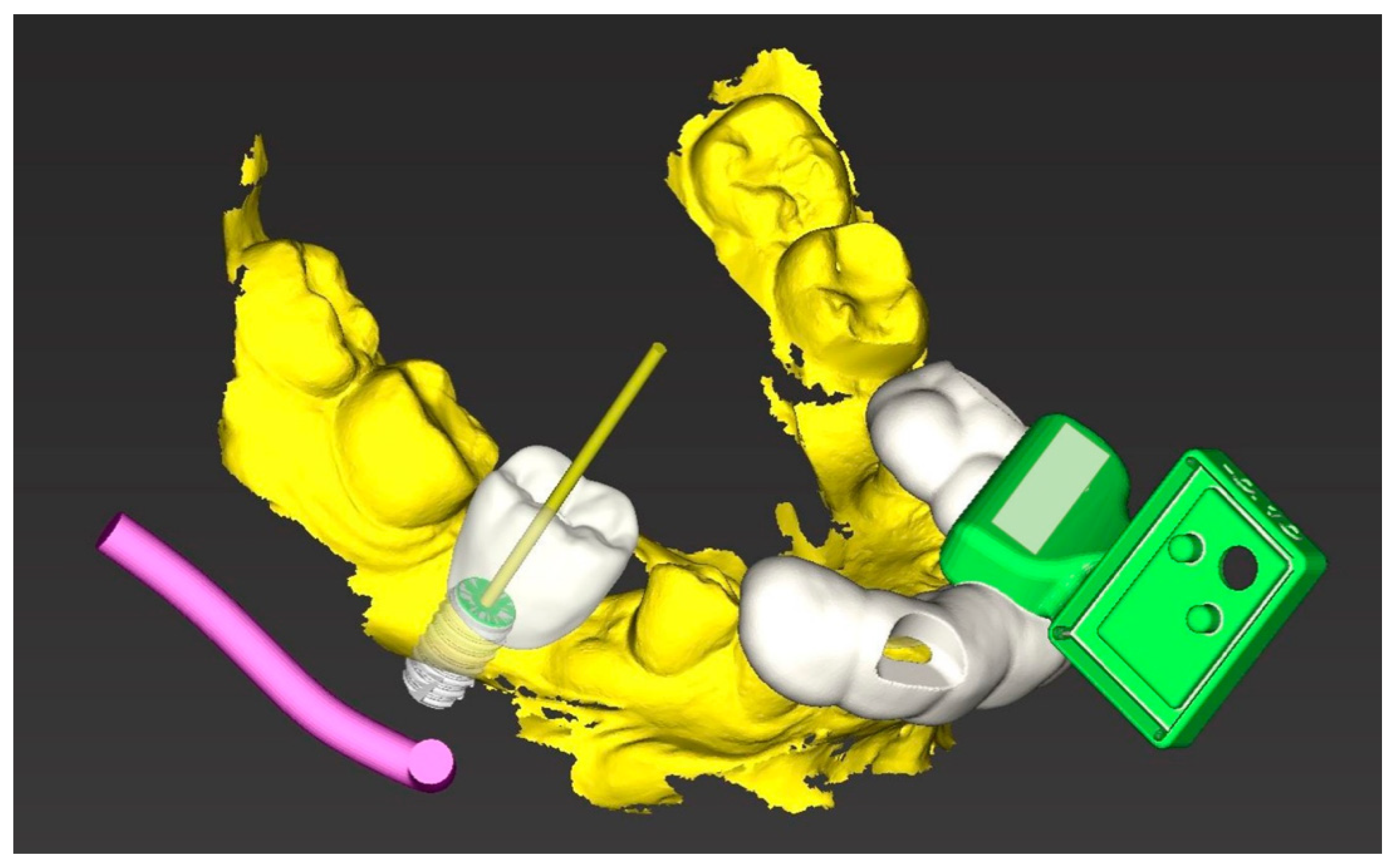
2.2. Implant Planning
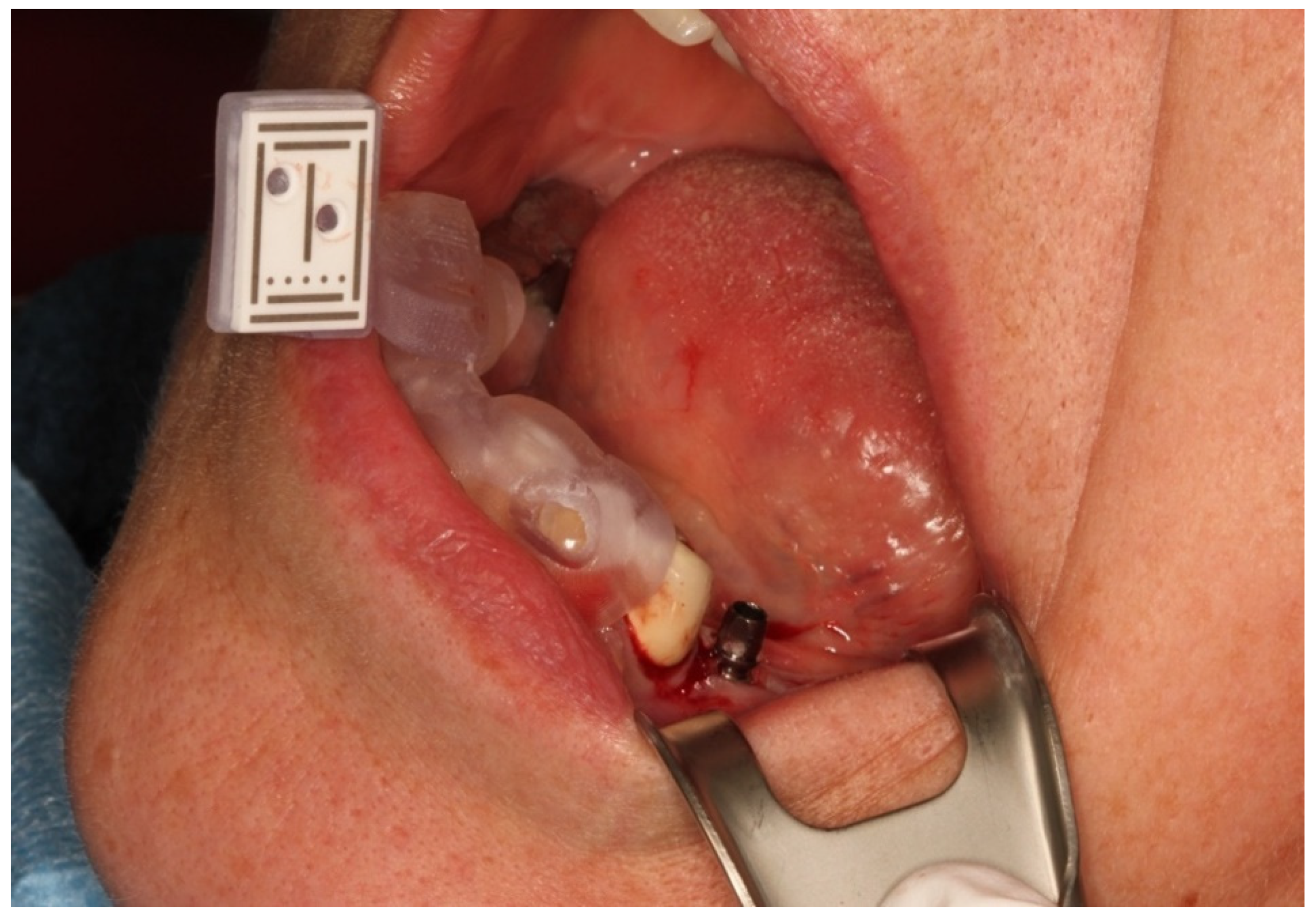
2.3. Reference Marker
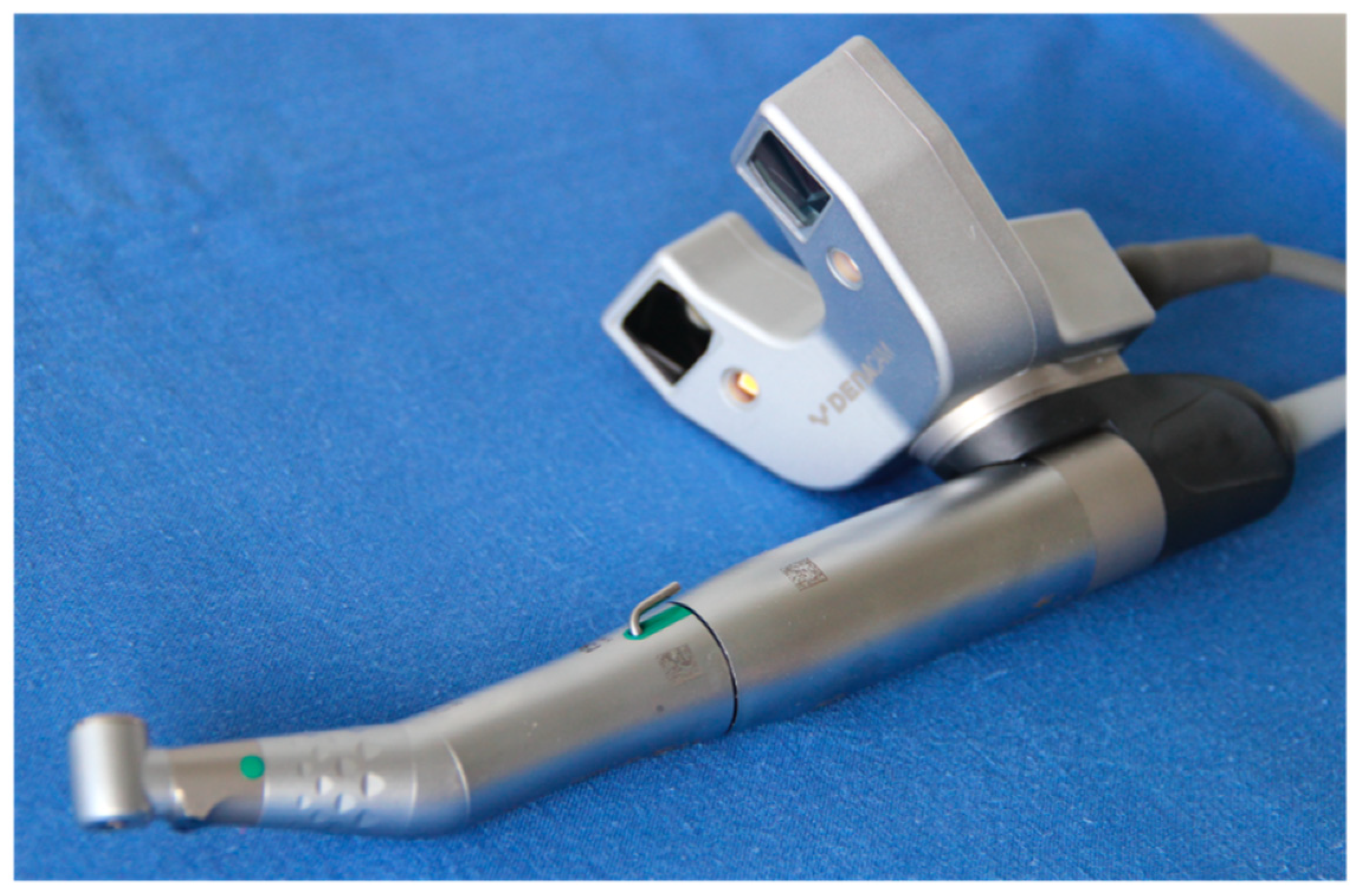
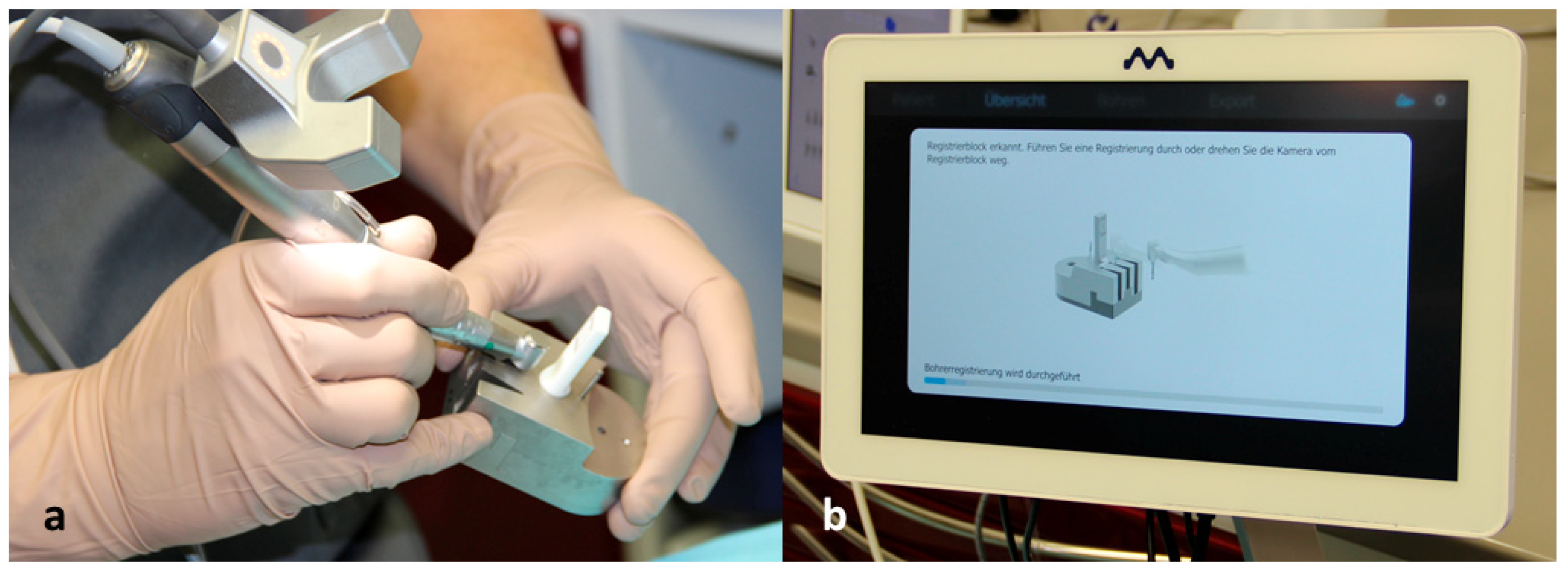
2.4. Registration of the Implant Position
2.5. Analysis of the Implant Position
2.6. Statistical Analysis
3. Results
3.1. Description of the Study Population
3.2. Evaluation of the Implantations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- D’Haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontol. 2000 2017, 73, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of titanium, titanium alloy and zirconia dental implants: Current knowledge and open questions. Periodontol. 2000 2017, 73, 22–40. [Google Scholar] [CrossRef]
- Albrektsson, T.; Chrcanovic, B.; Ostman, P.O.; Sennerby, L. Initial and long-term crestal bone responses to modern dental implants. Periodontol. 2000 2017, 73, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Al Amri, M.D. Influence of interimplant distance on the crestal bone height around dental implants: A systematic review and meta-analysis. J. Prosthet. Dent. 2016, 115, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.E.; Delgado-Ruiz, R.; Sculean, A. Concepts for prevention of complications in implant therapy. Periodontol. 2000 2019, 81, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Staubli, N.; Walter, C.; Schmidt, J.C.; Weiger, R.; Zitzmann, N.U. Excess cement and the risk of peri-implant disease-a systematic review. Clin. Oral Implant. Res. 2017, 28, 1278–1290. [Google Scholar] [CrossRef]
- Garber, D.A.; Belser, U.C. Restoration-driven implant placement with restoration-generated site development. Compend. Contin. Educ. Dent. 1995, 16, 796, 798–802, 804. [Google Scholar]
- Vercruyssen, M.; van de Wiele, G.; Teughels, W.; Naert, I.; Jacobs, R.; Quirynen, M. Implant- and patient-centred outcomes of guided surgery, a 1-year follow-up: An RCT comparing guided surgery with conventional implant placement. J. Clin. Periodontol. 2014, 41, 1154–1160. [Google Scholar] [CrossRef]
- Greenstein, G.; Tarnow, D. The mental foramen and nerve: Clinical and anatomical factors related to dental implant placement: A literature review. J. Periodontol. 2006, 77, 1933–1943. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Derksen, W.; Wittneben, J.G.; Kuehl, S. Static computer-aided implant surgery (s-CAIS) analysing patient-reported outcome measures (PROMs), economics and surgical complications: A systematic review. Clin. Oral. Implant. Res. 2018, 29 (Suppl. 16), 359–373. [Google Scholar] [CrossRef] [Green Version]
- Gargallo-Albiol, J.; Barootchi, S.; Salomo-Coll, O.; Wang, H.L. Advantages and disadvantages of implant navigation surgery. A systematic review. Ann. Anat. 2019, 225, 1–10. [Google Scholar] [CrossRef]
- Wismeijer, D.; Joda, T.; Flugge, T.; Fokas, G.; Tahmaseb, A.; Bechelli, D.; Bohner, L.; Bornstein, M.; Burgoyne, A.; Caram, S.; et al. Group 5 ITI Consensus Report: Digital technologies. Clin. Oral Implant. Res. 2018, 29 (Suppl. 16), 436–442. [Google Scholar] [CrossRef] [PubMed]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. 16), 416–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Yafi, F.; Camenisch, B.; Al-Sabbagh, M. Is Digital Guided Implant Surgery Accurate and Reliable? Dent. Clin. N. Am. 2019, 63, 381–397. [Google Scholar] [CrossRef] [PubMed]
- Gjelvold, B.; Mahmood, D.J.H.; Wennerberg, A. Accuracy of surgical guides from 2 different desktop 3D printers for computed tomography-guided surgery. J. Prosthet. Dent. 2019, 121, 498–503. [Google Scholar] [CrossRef]
- Henprasert, P.; Dawson, D.V.; El-Kerdani, T.; Song, X.; Couso-Queiruga, E.; Holloway, J.A. Comparison of the Accuracy of Implant Position Using Surgical Guides Fabricated by Additive and Subtractive Techniques. J. Prosthodont. 2020, 29, 534–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieralli, S.; Spies, B.C.; Hromadnik, V.; Nicic, R.; Beuer, F.; Wesemann, C. How Accurate Is Oral Implant Installation Using Surgical Guides Printed from a Degradable and Steam-Sterilized Biopolymer? J. Clin. Med. 2020, 9, 2322. [Google Scholar] [CrossRef]
- Liang, Y.; Yuan, S.; Huan, J.; Zhang, Y.; Fang, C.; Li, J. In Vitro Experimental Study of the Effect of Adjusting the Guide Sleeve Height and Using a Visual Direction-Indicating Guide on Implantation Accuracy. J. Oral Maxillofac. Surg. 2019, 77, 2259–2268. [Google Scholar] [CrossRef]
- Tallarico, M.; Martinolli, M.; Kim, Y.; Cocchi, F.; Meloni, S.M.; Alushi, A.; Xhanari, E. Accuracy of Computer-Assisted Template-Based Implant Placement Using Two Different Surgical Templates Designed with or without Metallic Sleeves: A Randomized Controlled Trial. Dent. J. 2019, 7, 41. [Google Scholar] [CrossRef] [Green Version]
- Kuhl, S.; Payer, M.; Zitzmann, N.U.; Lambrecht, J.T.; Filippi, A. Technical accuracy of printed surgical templates for guided implant surgery with the coDiagnostiX software. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. 1), e177–e182. [Google Scholar] [CrossRef] [PubMed]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implants 2014, 29, 25–42. [Google Scholar] [CrossRef] [Green Version]
- Schnutenhaus, S.; Edelmann, C.; Rudolph, H.; Luthardt, R.G. Retrospective study to determine the accuracy of template-guided implant placement using a novel nonradiologic evaluation method. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, e72–e79. [Google Scholar] [CrossRef] [PubMed]
- Vercruyssen, M.; Fortin, T.; Widmann, G.; Jacobs, R.; Quirynen, M. Different techniques of static/dynamic guided implant surgery: Modalities and indications. Periodontol. 2000 2014, 66, 214–227. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Wangrao, K.; Liu, L.; Liu, L.; Yao, Y. Quantification of image artifacts from navigation markers in dynamic guided implant surgery and the effect on registration performance in different clinical scenarios. Int. J. Oral Maxillofac. Implant. 2019, 34, 726–736. [Google Scholar] [CrossRef] [PubMed]
- Brief, J.; Edinger, D.; Hassfeld, S.; Eggers, G. Accuracy of image-guided implantology. Clin. Oral Implant. Res. 2005, 16, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Westendorff, C.; Gomez-Roman, G.; Reinert, S. Accuracy of navigation-guided socket drilling before implant installation compared to the conventional free-hand method in a synthetic edentulous lower jaw model. Clin. Oral Implant. Res. 2005, 16, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Kramer, F.J.; Baethge, C.; Swennen, G.; Rosahl, S. Navigated vs. conventional implant insertion for maxillary single tooth replacement. Clin. Oral Implant. Res. 2005, 16, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.H.; Cao, C.R.; Lin, W.C.; Shu, C.M. Experimental and numerical simulation study of the thermal hazards of four azo compounds. J. Hazard. Mater. 2019, 365, 164–177. [Google Scholar] [CrossRef]
- Chen, J.T. A Novel Application of Dynamic Navigation System in Socket Shield Technique. J. Oral Implant. 2019, 45, 409–415. [Google Scholar] [CrossRef] [Green Version]
- Block, M.S.; Emery, R.W. Static or Dynamic Navigation for Implant Placement-Choosing the Method of Guidance. J. Oral Maxillofac. Surg. 2016, 74, 269–277. [Google Scholar] [CrossRef]
- Schnutenhaus, S.; Edelmann, C.; Knipper, A.; Luthardt, R.G. Accuracy of Dynamic Computer-Assisted Implant Placement: A Systematic Review and Meta-Analysis of Clinical and In Vitro Studies. J. Clin. Med. 2021, 10, 704. [Google Scholar] [CrossRef]
- Ayoub, A.; Pulijala, Y. The application of virtual reality and augmented reality in Oral & Maxillofacial Surgery. BMC Oral Health 2019, 19, 238. [Google Scholar] [CrossRef] [Green Version]
- Schnutenhaus, S.; Groller, S.; Luthardt, R.G.; Rudolph, H. Accuracy of the match between cone beam computed tomography and model scan data in template-guided implant planning: A prospective controlled clinical study. Clin. Implant. Dent. Relat. Res. 2018, 20, 541–549. [Google Scholar] [CrossRef]
- Aydemir, C.A.; Arisan, V. Accuracy of dental implant placement via dynamic navigation or the freehand method: A split-mouth randomized controlled clinical trial. Clin. Oral Implant. Res. 2020, 31, 255–263. [Google Scholar] [CrossRef]
- Block, M.S.; Emery, R.W.; Cullum, D.R.; Sheikh, A. Implant Placement Is More Accurate Using Dynamic Navigation. J. Oral Maxillofac. Surg. 2017, 75, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Emery, R.W.; Lank, K.; Ryan, J. Implant Placement Accuracy Using Dynamic Navigation. Int. J. Oral Maxillofac. Implants 2017, 32, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Kaewsiri, D.; Panmekiate, S.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. The accuracy of static vs. dynamic computer-assisted implant surgery in single tooth space: A randomized controlled trial. Clin. Oral Implant. Res. 2019, 30, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, G.; Taraschi, V.; Andrea, Z.; Ferri, A.; Marchetti, C. Dynamic navigation: A prospective clinical trial to evaluate the accuracy of implant placement. Int. J. Comput. Dent. 2019, 22, 139–147. [Google Scholar] [PubMed]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a Dynamic Dental Implant Navigation System in a Private Practice. Int. J. Oral Maxillofac. Implants 2019, 34, 205–213. [Google Scholar] [CrossRef]
- Stefanelli, L.V.; Mandelaris, G.A.; DeGroot, B.S.; Gambarini, G.; De Angelis, F.; Di Carlo, S. Accuracy of a Novel Trace-Registration Method for Dynamic Navigation Surgery. Int. J. Periodontics Restor. Dent. 2020, 40, 427–435. [Google Scholar] [CrossRef]
- Wu, D.; Zhou, L.; Yang, J.; Zhang, B.; Lin, Y.; Chen, J.; Huang, W.; Chen, Y. Accuracy of dynamic navigation compared to static surgical guide for dental implant placement. Int. J. Implant. Dent. 2020, 6, 78. [Google Scholar] [CrossRef]
- Yimarj, P.; Subbalekha, K.; Dhanesuan, K.; Siriwatana, K.; Mattheos, N.; Pimkhaokham, A. Comparison of the accuracy of implant position for two-implants supported fixed dental prosthesis using static and dynamic computer-assisted implant surgery: A randomized controlled clinical trial. Clin. Implant. Dent. Relat. Res. 2020, 22, 672–678. [Google Scholar] [CrossRef]
- Jorba-García, A.; González-Barnadas, A.; Camps-Font, O.; Figueiredo, R.; Valmaseda-Castellón, E. Accuracy assessment of dynamic computer-aided implant placement: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 1–16. [Google Scholar] [CrossRef]
- Wei, S.M.; Zhu, Y.; Wei, J.X.; Zhang, C.N.; Shi, J.Y.; Lai, H.C. Accuracy of dynamic navigation in implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2021, 32, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Forna, N.; Agop-Forna, D. Esthetic aspects in implant-prosthetic rehabilitation. Med. Pharm. Rep. 2019, 92 (Suppl. No 3), S6–S13. [Google Scholar] [CrossRef]
- Schnutenhaus, S.; Edelmann, C.; Rudolph, H. Does the macro design of an implant affect the accuracy of template-guided implantation? A prospective clinical study. Int. J. Implant. Dent. 2021, accepted. [Google Scholar]
- Zhou, W.; Liu, Z.; Song, L.; Kuo, C.L.; Shafer, D.M. Clinical Factors Affecting the Accuracy of Guided Implant Surgery-A Systematic Review and Meta-analysis. J. Evid. Based Dent. Pract. 2018, 18, 28–40. [Google Scholar] [CrossRef]
- Yeung, M.; Abdulmajeed, A.; Carrico, C.K.; Deeb, G.R.; Bencharit, S. Accuracy and precision of 3D-printed implant surgical guides with different implant systems: An in vitro study. J. Prosthet. Dent. 2020, 123, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Guzman, A.M.; Deglow, E.R.; Zubizarreta-Macho, A.; Agustin-Panadero, R.; Montero, S.H. Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Navigation for Dental Implant Placement: An In Vitro Study. J. Clin. Med. 2019, 8, 2123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.H.; Lee, J.W.; Lim, S.H.; Kim, Y.H.; Kim, M.K. Verification of the usability of a navigation method in dental implant surgery: In vitro comparison with the stereolithographic surgical guide template method. J. Craniomaxillofac. Surg. 2014, 42, 1530–1535. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Schneider, D.; Ganeles, J.; Wismeijer, D.; Zwahlen, M.; Hammerle, C.H.; Tahmaseb, A. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2009, 24, 92–109. [Google Scholar] [PubMed]
- Bover-Ramos, F.; Vina-Almunia, J.; Cervera-Ballester, J.; Penarrocha-Diago, M.; Garcia-Mira, B. Accuracy of Implant Placement with Computer-Guided Surgery: A Systematic Review and Meta-Analysis Comparing Cadaver, Clinical, and In Vitro Studies. Int. J. Oral Maxillofac. Implant. 2018, 33, 101–115. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | Upper Jaw | Lower Jaw | Flap | Flapless | |
|---|---|---|---|---|---|---|
| Frequencies | 7 | 13 | 4 | 16 | 10 | 10 |
| Percent | 35% | 65% | 20% | 80% | 50% | 50% |
| Lengths/Diameters (mm) | 3.8 | 4.4 | 5.0 |
|---|---|---|---|
| 9 | 2 | 9 | 3 |
| 11 | 1 | 3 | 1 |
| 13 | 1 | 0 | 0 |
| Mean (SD) | 95% CI | Minimum | Maximum | ||
|---|---|---|---|---|---|
| Angle | Deviation | 2.7 (0.26) | 2.2–3.36 | 1.1 | 5.9 |
| Shoulder | 3D Deviation | 1.83 (0.24) | 1.34–2.33 | 0.53 | 4.14 |
| Mesiodistal Deviation | 0.93 (0.17) | 0.58–1.29 | 0.00 | 3.01 | |
| Oro-vestibular Deviation | 0.48 (0.08) | 0.30–0.65 | 0.01 | 1.30 | |
| Apico-coronal Deviation | 1.31 (0.22) | 0.85–1.78 | 0.02 | 3.68 | |
| Apex | 3D Deviation | 1.95 (0.28) | 1.39–2.50 | 0.51 | 4.37 |
| Mesiodistal Deviation | 1.07 (0.22) | 0.62–1.52 | 0.10 | 3.88 | |
| Oro-vestibular Deviation | 0.57 (0.08) | 0.40–0.74 | 0.10 | 1.58 | |
| Apico-coronal Deviation | 1.30 (0.22) | 0.84–1.76 | 0.03 | 3.68 |
| Lower Jaw n = 16 | Upper Jaw n = 4 | p-Value | Open Procedure n = 10 | Flapless n = 10 | p-Value | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | 95% CI | Min.–Max. | Mean (SD) | 95% CI | Min.–Max. | Mean (SD) | 95% CI | Min.–Max. | Mean (SD) | 95% CI | Min.–Max. | ||||
| Shoulder | 3D | 1.77 (0.24) | 1.25–2.29 | 0.53–3.84 | 2.08 (0.74) | 0.28–4.44 | 0.82–4.14 | 0.617 | 1.78 (0.39) | 0.91–2.67 | 0.53–3.84 | 1.88 (0.29) | 1.22–2.54 | 0.82–4.14 | 0.162 |
| Mesiodistal | 0.93 (0.19) | 0.52–1.34 | 0.00–3.01 | 0.95 (0.42) | 0.37–2.27 | 0.13–1.69 | 0.958 | 1.02 (0.30) | 0.34–1.70 | 0.00–3.01 | 0.84 (0.17) | 0.45–1.23 | 0 13–1.69 | 0.179 | |
| Oro-vestibular | 0.42 (0.06) | 0.29–0.56 | 0.01–0.86 | 0.70 (0.34) | 0.38–1.77 | 0.06–1.30 | 0.195 | 0.39 (0.09) | 0.19–0.58 | 0.01–0.80 | 0.57 (0.14) | 0.25–0.88 | 0.06–1.30 | 0.184 | |
| Apico-coronal | 1.26 (0.23) | 0.77–1.75 | 0.02–3.68 | 1.53 (0.68) | 1.26–2.45 | 0.64–3.55 | 0.641 | 1.17 (0.35) | 0.38–1.96 | 0.02–3.68 | 1.46 (0.69) | 0.83–2.09 | 0.64–3.55 | 0.532 | |
| Apex | 3D | 1.86 (0.28) | 1.26–2.45 | 0.51–4.06 | 2.30 (0.76) | 0.11–4.72 | 1.10–4.37 | 0.512 | 1.89 (0.45) | 0.87–2.90 | 0.51–4.06 | 2.00 (0.30) | 1.32–2.69 | 1.10–4.37 | 0.052 |
| Mesiodistal | 1.03 (0.24) | 0.51–1.55 | 0.03–3.88 | 1.21 (0.53) | 0.48–2.91 | 0.29–2.39 | 0.745 | 1.22 (0.36) | 0.41–2.03 | 0.35–3.88 | 0.92 (0.25) | 0.34–1.49 | 0.03–2.39 | 0.597 | |
| Oro-vestibular | 0.49 (0.07) | 0.35–0.63 | 0.10–0.98 | 0.88 (0.29) | 0.42–0.80 | 0.20–1.58 | 0.769 | 0.45 (0.09) | 0.24–0.65 | 0.10–0.98 | 0.69 (0.13) | 0.40–0.98 | 0.17–1.58 | 0.495 | |
| Apico-coronal | 1.25 (0.23) | 0.76–1.74 | 0.03–3.68 | 1.52 (0.68) | 0.64–3.68 | 0.65–3.53 | 0.635 | 1.16 (0.35) | 0.36–1.95 | 0 03–3 68 | 1.45 (0.28) | 0.82–2.08 | 0.65–3.53 | 0.520 | |
| Angular Deviation (degree) | 2.70 (0.30) | 2.10–3.40 | 1.20–5.90 | 2.70 (0.60) | 0.70–4.60 | 1.10–4.00 | 0.905 | 2.90 (0.50) | 1.9–3.90 | 1.20–5.90 | 2.50 (0.30) | 1.90–3.10 | 1.10–4.00 | 0.273 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edelmann, C.; Wetzel, M.; Knipper, A.; Luthardt, R.G.; Schnutenhaus, S. Accuracy of Computer-Assisted Dynamic Navigation in Implant Placement with a Fully Digital Approach: A Prospective Clinical Trial. J. Clin. Med. 2021, 10, 1808. https://doi.org/10.3390/jcm10091808
Edelmann C, Wetzel M, Knipper A, Luthardt RG, Schnutenhaus S. Accuracy of Computer-Assisted Dynamic Navigation in Implant Placement with a Fully Digital Approach: A Prospective Clinical Trial. Journal of Clinical Medicine. 2021; 10(9):1808. https://doi.org/10.3390/jcm10091808
Chicago/Turabian StyleEdelmann, Cornelia, Martin Wetzel, Anne Knipper, Ralph G. Luthardt, and Sigmar Schnutenhaus. 2021. "Accuracy of Computer-Assisted Dynamic Navigation in Implant Placement with a Fully Digital Approach: A Prospective Clinical Trial" Journal of Clinical Medicine 10, no. 9: 1808. https://doi.org/10.3390/jcm10091808