
Correlation between Biomarkers of Pain in Saliva and PAINAD Scale in Elderly People with Cognitive Impairment and Inability to Communicate

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Objectives
3. Materials and Methods
3.1. Study Design
3.2. Study Setting
3.3. Participants and Selection Criteria
- Being 65 or older.
- Having a medical diagnosis of dementia or Alzheimer’s disease-like dementia (AD) with a global deterioration scale (GDS) score between 5 and 7. Those patients who met DSM-V clinical criteria were diagnosed with dementia, and those who met the NINCDS/ADRDA (National Institute of Neurological and Communicative Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association) criteria were classified as probable or possible AD patients.
- Being unable to communicate verbally.
- Having received health care at the community level for at least three months because of the dementia process. In the center dedicated to the care of patients suffering from AD, the included patients were those who have used this service for at least three months.
- Having an informed consent signed by a relative or legal representative for the patient’s inclusion in the study.
3.4. Study Measures and Data Collection
- Subjects were not allowed to practice physical exercise or to eat, ingest any drinks (except for water), chew gum, brush their teeth, or consume caffeine during the previous hour preceding the sample collection process.
- Five minutes before the collection of the sample, as a way to reduce the contamination of saliva with food debris, the subjects were asked to rinse their mouth with clean water.
- Right before starting the sample collection, any saliva present in the mouth at that time should be swallowed.
- Afterwards, the saliva accumulated in their mouths for 5 min was deposited in a collection tube, 1 mL being the minimum volume required. In the case of the 5 mL collection tube being filled before those 5 min, the corresponding amount of time elapsed was recorded.
3.5. Determination of sTNF-RII and IgA
3.6. Data Analysis
3.7. Ethical Aspects
4. Results
4.1. Sample Characteristics
4.2. Correlation between PAINAD Scale and Sample Characteristics
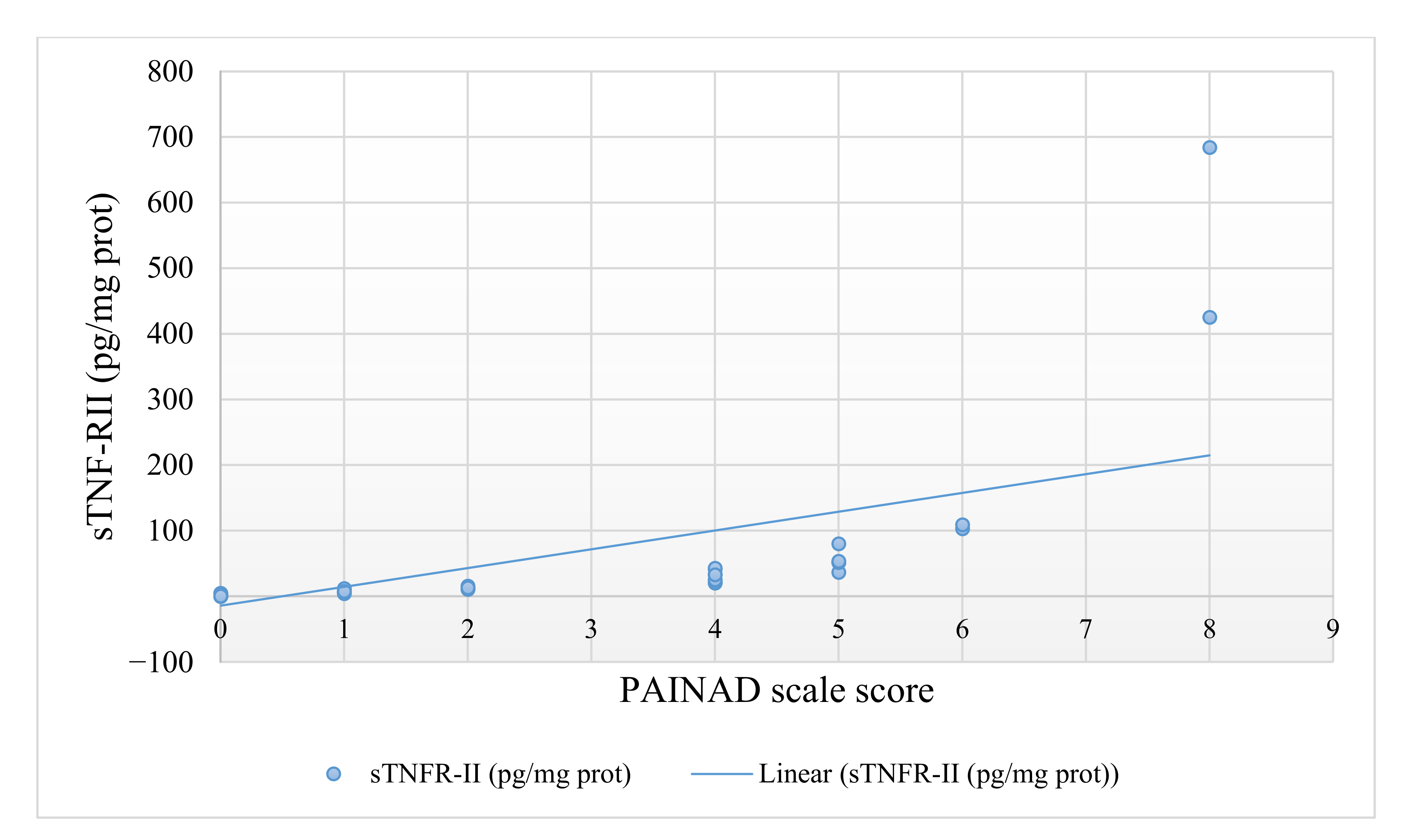
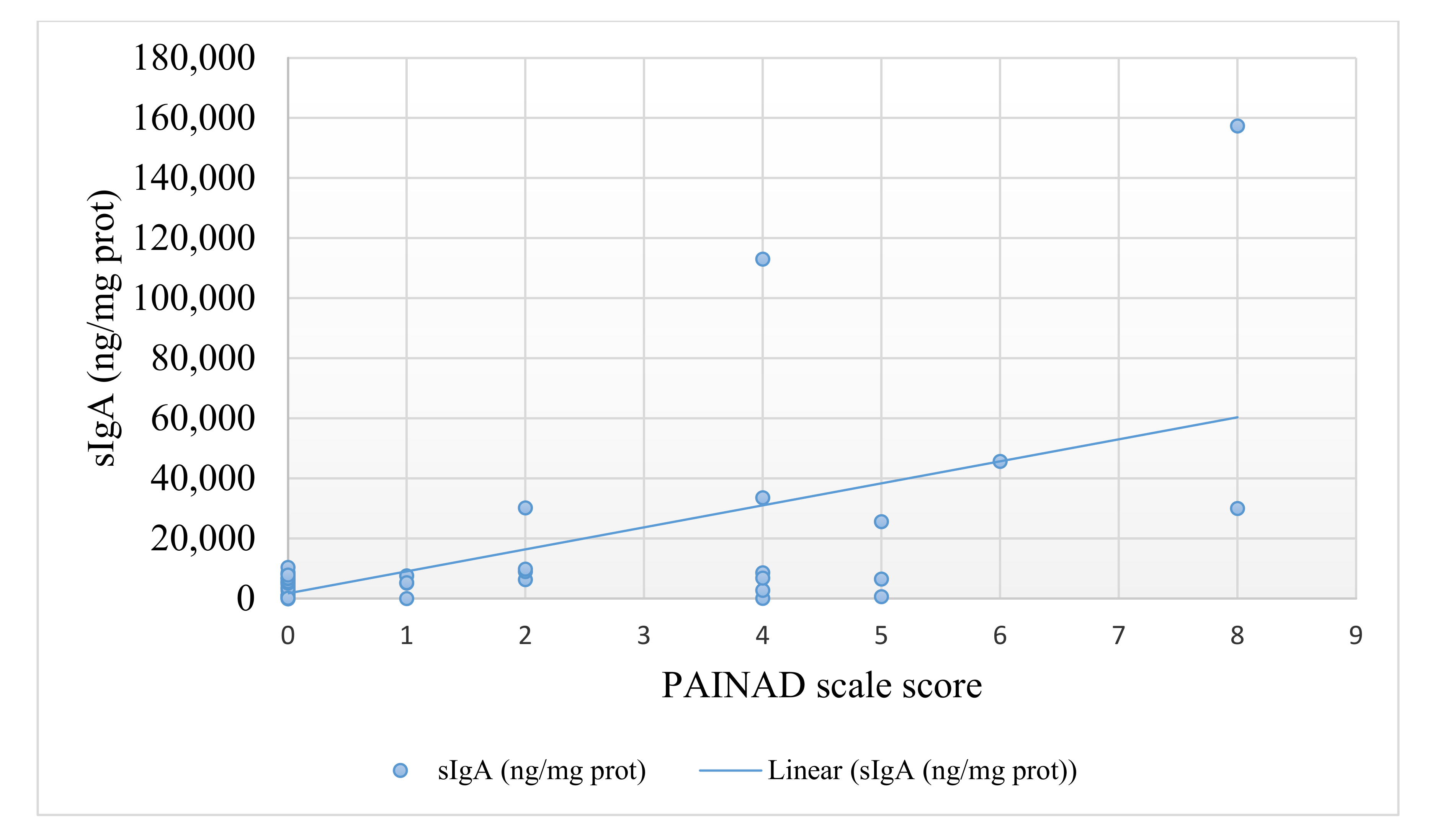
4.3. Correlation between PAINAD Scale and Saliva Biomarkers
4.4. Regression Models
5. Discussion
Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The Revised International Association for the Study of Pain Definition of Pain: Concepts, Challenges, and Compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Quintner, J.; van Rysewyk, S. Reconsidering the International Association for the Study of Pain Definition of Pain. Pain Rep. 2018, 3, e634. [Google Scholar] [CrossRef] [PubMed]
- Aydede, M. Does the IASP Definition of Pain Need Updating? Pain Rep. 2019, 4, e777. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.C.; Craig, K.D. Updating the Definition of Pain. Pain 2016, 157, 2420–2423. [Google Scholar] [CrossRef] [PubMed]
- Domenichiello, A.F.; Ramsden, C.E. The Silent Epidemic of Chronic Pain in Older Adults. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 93, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Makino, K.; Lee, S.; Bae, S.; Jung, S.; Shinkai, Y.; Chiba, I.; Shimada, H. Pain Characteristics and Incidence of Functional Disability among Community-Dwelling Older Adults. PLoS ONE 2019, 14, e0215467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, K.V.; Guralnik, J.M.; Dansie, E.J.; Turk, D.C. Prevalence and Impact of Pain among Older Adults in the United States: Findings from the 2011 National Health and Aging Trends Study. Pain 2013, 154, 2649–2657. [Google Scholar] [CrossRef] [Green Version]
- Sjölund, B.; Mamhidir, A.; Engström, M. Pain Prevalence among Residents Living in Nursing Homes and Its Association with Quality of Life and Well-being. Scand. J. Caring Sci. 2021, scs.12955, [published online ahead of print, 6 January 2021]. [Google Scholar] [CrossRef]
- Hemmingsson, E.-S.; Gustafsson, M.; Isaksson, U.; Karlsson, S.; Gustafson, Y.; Sandman, P.-O.; Lövheim, H. Prevalence of Pain and Pharmacological Pain Treatment among Old People in Nursing Homes in 2007 and 2013. Eur. J. Clin. Pharm. 2018, 74, 483–488. [Google Scholar] [CrossRef] [Green Version]
- Nunziata, V.; Proietti, M.; Saporiti, E.; Calcaterra, L.; Rolland, Y.; Vellas, B.; Cesari, M. Pain Management in Nursing Home Residents: Results from the Incur Study. J. Nutr. Health Aging 2020, 24, 1019–1022. [Google Scholar] [CrossRef]
- Hadjistavropoulos, T.; Herr, K.; Prkachin, K.M.; Craig, K.D.; Gibson, S.J.; Lukas, A.; Smith, J.H. Pain Assessment in Elderly Adults with Dementia. Lancet Neurol. 2014, 13, 1216–1227. [Google Scholar] [CrossRef]
- Hunt, L.J.; Covinsky, K.E.; Yaffe, K.; Stephens, C.E.; Miao, Y.; Boscardin, W.J.; Smith, A.K. Pain in Community-Dwelling Older Adults with Dementia: Results from the National Health and Aging Trends Study. J. Am. Geriatr. Soc. 2015, 63, 1503–1511. [Google Scholar] [CrossRef] [Green Version]
- Zwakhalen, S.; Docking, R.E.; Gnass, I.; Sirsch, E.; Stewart, C.; Allcock, N.; Schofield, P. Pain in Older Adults with Dementia. Der Schmerz 2018, 32, 364–373. [Google Scholar] [CrossRef] [Green Version]
- Hadjistavropoulos, T.; Herr, K.; Turk, D.C.; Fine, P.G.; Dworkin, R.H.; Helme, R.; Jackson, K.; Parmelee, P.A.; Rudy, T.E.; Lynn Beattie, B.; et al. An Interdisciplinary Expert Consensus Statement on Assessment of Pain in Older Persons. Clin. J. Pain 2007, 23, S1–S43. [Google Scholar] [CrossRef]
- Lukas, A.; Schuler, M.; Fischer, T.W.; Gibson, S.J.; Savvas, S.M.; Nikolaus, T.; Denkinger, M. Pain and Dementia: A Diagnostic Challenge. Z. Gerontol. Geriatr. 2012, 45, 45–49. [Google Scholar] [CrossRef]
- Herr, K.; Zwakhalen, S.; Swafford, K. Observation of Pain in Dementia. Curr. Alzheimer Res. 2017, 14, 486–500. [Google Scholar] [CrossRef]
- Horgas, A.L.; Elliott, A.F.; Marsiske, M. Pain Assessment in Persons with Dementia: Relationship Between Self-Report and Behavioral Observation. J. Am. Geriatr. Soc. 2009, 57, 126–132. [Google Scholar] [CrossRef]
- Lichtner, V.; Dowding, D.; Esterhuizen, P.; Closs, S.J.; Long, A.F.; Corbett, A.; Briggs, M. Pain Assessment for People with Dementia: A Systematic Review of Systematic Reviews of Pain Assessment Tools. BMC Geriatr. 2014, 14, 138. [Google Scholar] [CrossRef]
- Herr, K.; Bursch, H.; Ersek, M.; Miller, L.L.; Swafford, K. Use of Pain-Behavioral Assessment Tools in the Nursing Home. J. Gerontol. Nurs. 2010, 36, 18–29. [Google Scholar] [CrossRef]
- Warden, V.; Hurley, A.C.; Volicer, L. Development and Psychometric Evaluation of the Pain Assessment in Advanced Dementia (PAINAD) Scale. J. Am. Med. Dir. Assoc. 2003, 4, 9–15. [Google Scholar] [CrossRef]
- Choi, J.C.; Chung, M.I.; Lee, Y.D. Modulation of Pain Sensation by Stress-Related Testosterone and Cortisol. Anaesthesia 2012, 67, 1146–1151. [Google Scholar] [CrossRef]
- Da Silva Campos, M.J.; Souza Alves, C.C.; Barbosa Raposo, N.R.; Ferreira, A.P.; Farinazzo Vitral, R.W. Influence of Salivary Secretory Immunoglobulin A Level on the Pain Experienced by Orthodontic Patients. Med. Sci. Monit. 2010, 16, CR405–CR409. [Google Scholar]
- Goodin, B.R.; Quinn, N.B.; King, C.D.; Page, G.G.; Haythornthwaite, J.A.; Edwards, R.R.; Stapleton, L.; McGuire, L. Salivary Cortisol and Soluble Tumor Necrosis Factor-α Receptor II Responses to Multiple Experimental Modalities of Acute Pain. Psychophysiology 2012, 49, 118–127. [Google Scholar] [CrossRef] [Green Version]
- McLean, S.A.; Williams, D.A.; Harris, R.E.; Kop, W.J.; Groner, K.H.; Ambrose, K.; Lyden, A.K.; Gracely, R.H.; Crofford, L.J.; Geisser, M.E.; et al. Momentary Relationship between Cortisol Secretion and Symptoms in Patients with Fibromyalgia. Arthritis Rheum. 2005, 52, 3660–3669. [Google Scholar] [CrossRef]
- Robles, T.F.; Sharma, R.; Park, K.-S.; Harrell, L.; Yamaguchi, M.; Shetty, V. Utility of a Salivary Biosensor for Objective Assessment of Surgery-Related Stress. J. Oral Maxillofac. Surg. 2012, 70, 2256–2263. [Google Scholar] [CrossRef] [Green Version]
- Sobas, E.M.; Reinoso, R.; Cuadrado-Asensio, R.; Fernández, I.; Maldonado, M.J.; Pastor, J.C. Reliability of Potential Pain Biomarkers in the Saliva of Healthy Subjects: Inter-Individual Differences and Intersession Variability. PLoS ONE 2016, 11, e0166976. [Google Scholar] [CrossRef]
- Sobas, E.M.; Vázquez, A.; Videla, S.; Reinoso, R.; Fernández, I.; Garcia-Vazquez, C.; Maldonado, M.J.; Pastor, J.C. Evaluation of Potential Pain Biomarkers in Saliva and Pain Perception After Corneal Advanced Surface Ablation Surgery. Clin. Ophthalmol. 2020, 14, 613–623. [Google Scholar] [CrossRef] [Green Version]
- Golatowski, C.; Gesell Salazar, M.; Dhople, V.M.; Hammer, E.; Kocher, T.; Jehmlich, N.; Völker, U. Comparative Evaluation of Saliva Collection Methods for Proteome Analysis. Clin. Chim. Acta 2013, 419, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Boltz, M.; Resnick, B.; Kuzmik, A.; Mogle, J.; Jones, J.R.; Arendacs, R.; BeLue, R.; Cacchione, P.; Galvin, J.E. Pain Incidence, Treatment, and Associated Symptoms in Hospitalized Persons with Dementia. Pain Manag. Nurs. 2020. [Google Scholar] [CrossRef] [PubMed]
- Malotte, K.L.; McPherson, M.L. Identification, Assessment, and Management of Pain in Patients with Advanced Dementia. Mental Health Clin. 2016, 6, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Narbona, L.; Roldán-Merino, J.; Lluch-Canut, T.; Juvé-Udina, E.; Llorca, M.B.; Cabrera-Jaime, S. Impact of a Training Intervention on the Pain Assessment in Advanced Dementia (PAINAD) Scale in Noncommunicative Inpatients. Pain Manag. Nurs. 2019, 20, 468–474. [Google Scholar] [CrossRef]
- Jasim, H.; Carlsson, A.; Hedenberg-Magnusson, B.; Ghafouri, B.; Ernberg, M. Saliva as a Medium to Detect and Measure Biomarkers Related to Pain. Sci. Rep. 2018, 8, 3220. [Google Scholar] [CrossRef] [Green Version]
- Delwel, S.; Binnekade, T.T.; Perez, R.S.G.M.; Hertogh, C.M.P.M.; Scherder, E.J.A.; Lobbezoo, F. Oral Hygiene and Oral Health in Older People with Dementia: A Comprehensive Review with Focus on Oral Soft Tissues. Clin. Oral Investig. 2018, 22, 93–108. [Google Scholar] [CrossRef] [Green Version]
- Gil-Montoya, J.A.; Barrios, R.; Sánchez-Lara, I.; Carnero-Pardo, C.; Fornieles-Rubio, F.; Montes, J.; Gonzalez-Moles, M.A.; Bravo, M. Prevalence of Drug-Induced Xerostomia in Older Adults with Cognitive Impairment or Dementia: An Observational Study. Drugs Aging 2016, 33, 611–618. [Google Scholar] [CrossRef]
- Zhang, J.-M.; An, J. Cytokines, Inflammation, and Pain. Int. Anesthesiol. Clin. 2007, 45, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, S.L.; Bowers, W.J. Tumor Necrosis Factor-Alpha and the Roles It Plays in Homeostatic and Degenerative Processes Within the Central Nervous System. J. Neuroimmune Pharm. 2012, 7, 42–59. [Google Scholar] [CrossRef]
- Bradburn, S.; Murgatroyd, C.; Ray, N. Neuroinflammation in Mild Cognitive Impairment and Alzheimer’s Disease: A Meta-Analysis. Ageing Res. Rev. 2019, 50, 1–8. [Google Scholar] [CrossRef]
- Calsolaro, V.; Edison, P. Neuroinflammation in Alzheimer’s Disease: Current Evidence and Future Directions. Alzheimer’s Dement. 2016, 12, 719–732. [Google Scholar] [CrossRef]
- Pasqualetti, G.; Brooks, D.J.; Edison, P. The Role of Neuroinflammation in Dementias. Curr. Neurol. Neurosci. Rep. 2015, 15, 17. [Google Scholar] [CrossRef]
- Stefaniak, J.; O’Brien, J. Imaging of Neuroinflammation in Dementia: A Review. J. Neurol. Neurosurg. Psychiatry 2015, 87, 21–28. [Google Scholar] [CrossRef]
- De Oliveira Martinez, K.; Mendes, L.L.; Alves, J.B. Secretory A Immunoglobulin, Total Proteins and Salivary Flow in Recurrent Aphthous Ulceration. Braz. J. Otorhinolaryngol. 2007, 73, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Dioguardi, M.; Crincoli, V.; Laino, L.; Alovisi, M.; Sovereto, D.; Mastrangelo, F.; Lo Russo, L.; Lo Muzio, L. The Role of Periodontitis and Periodontal Bacteria in the Onset and Progression of Alzheimer’s Disease: A Systematic Review. J. Clin. Med. 2020, 9, 495. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-T.; Lee, H.-C.; Hu, C.-J.; Huang, L.-K.; Chao, S.-P.; Lin, C.-P.; Su, E.C.-Y.; Lee, Y.-C.; Chen, C.-C. Periodontitis as a Modifiable Risk Factor for Dementia: A Nationwide Population-Based Cohort Study. J. Am. Geriatr. Soc. 2017, 65, 301–305. [Google Scholar] [CrossRef]
- Nadim, R.; Tang, J.; Dilmohamed, A.; Yuan, S.; Wu, C.; Bakre, A.T.; Partridge, M.; Ni, J.; Copeland, J.R.; Anstey, K.J.; et al. Influence of Periodontal Disease on Risk of Dementia: A Systematic Literature Review and a Meta-Analysis. Eur. J. Epidemiol. 2020, 35, 821–833. [Google Scholar] [CrossRef]
- Bjørnnes, A.K.; Parry, M.; Lie, I.; Falk, R.; Leegaard, M.; Rustøen, T. The Association between Hope, Marital Status, Depression and Persistent Pain in Men and Women Following Cardiac Surgery. BMC Women’s Health 2018, 18, 2. [Google Scholar] [CrossRef] [Green Version]
- Sorge, R.E.; Totsch, S.K. Sex Differences in Pain. J. Neurosci. Res. 2017, 95, 1271–1281. [Google Scholar] [CrossRef]
- Nowak, T.; Neumann-Podczaska, A.; Tobis, S.; Wieczorowska-Tobis, K. Characteristics of Pharmacological Pain Treatment in Older Nursing Home Residents. J. Pain Res. 2019, 12, 1083–1089. [Google Scholar] [CrossRef] [Green Version]
- Tan, E.C.K.; Jokanovic, N.; Koponen, M.P.H.; Thomas, D.; Hilmer, S.N.; Bell, J.S. Prevalence of Analgesic Use and Pain in People with and without Dementia or Cognitive Impairment in Aged Care Facilities: A Systematic Review and Meta-Analysis. Curr. Clin. Pharm. 2015, 10, 194–203. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total n = 75 |
|---|---|
| Sociodemographic variables | |
| Age x (SD) | 84.41 (7.44) |
| Sex n (%) | |
| Woman | 59 (78.7%) |
| Man | 16 (21.3%) |
| Marital status n (%) | |
| Single | 6 (8%) |
| Married | 16 (21.3%) |
| Widowed | 51 (68%) |
| Divorced | 2 (2.7%) |
| Institutionalized n (%) | |
| Yes | 52 (69.3%) |
| No | 23 (30.7%) |
| Area of residence of the sample n (%) | |
| Rural | 11 (14.7%) |
| Urban | 64 (85.3%) |
| Clinical variables | |
| Type of dementia n (%) | |
| Alzheimer’s disease | 52 (69.33%) |
| Vascular dementia | 8 (10.67%) |
| Primary degenerative dementia | 2 (2.67%) |
| Mixed dementia | 13 (17.33%) |
| Level of cognitive impairment b n (%) | |
| GDS 5 | 13 (17.33%) |
| GDS 6 | 28 (37.33%) |
| GDS 7 | 34 (45.33%) |
| Level of dependency for basic activities of daily living c n (%) | |
| Moderate dependence | 7 (9.3%) |
| Severe dependence | 18(24%) |
| Total dependence | 50 (66.7%) |
| Prescription of analgesics n (%) | |
| Yes | 34 (45.33%) |
| No | 41 (54.67%) |
| Time consuming analgesics (days) Me (maximum-minimum) a | 471 (4321–5) |
| PAINAD x (SD) | 1.45 (2.15) |
| sTNF-RII (pg/mg protein) Me (maximum-minimum) a | 2.56 (684.28–0.0162) |
| sIgA (ng/mg protein) (n = 54) Me (maximum-minimum) a | 5285.60 (157440.83–6.49) |
| Variables in the Equation | ||||||
|---|---|---|---|---|---|---|
| Dependent Variable: Binary_PAINAD | B | Standard Error | Wald | df | Sig. | Exp(B) |
| sTNF-RII (pg/mg prot) Constant | 2.177 | 1.301 | 2.801 | 1 | 0.094 | 8.817 |
| −10.469 | 6.118 | 2.928 | 1 | 0.087 | 0.000 | |
| Parameter Estimates | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Recoded PAINAD a | B | Standard Error | Wald | df | Sig. | Exp(B) | 95% Confidence Interval for Exp(B) | ||
| Lower Limit | Upper Limit | ||||||||
| Possible pain | Interception | −68.332 | 2827.925 | 0.001 | 1 | 0.981 | |||
| sTNF-RII | 10.264 | 0.702 | 213.580 | 1 | 0.000 | 28667.235 | 7237.641 | 113546.716 | |
| sIgA | 0.001 | 1.530 | 0.000 | 1 | 0.999 | 1.001 | 0.050 | 20.072 | |
| With pain | Interception | −77.191 | 2827.924 | 0.001 | 1 | 0.978 | |||
| sTNF-RII | 10.915 | 0.000 | 1 | 0.000 | 54977.698 | 54977.698 | 54977.698 | ||
| sIgA | 0.002 | 1.530 | 0.000 | 1 | 0.999 | 1.002 | 0.050 | 20.077 | |
| Likelihood Ratio Comparison | ||||
|---|---|---|---|---|
| Effect | Model Fit Criteria | Likelihood Ratio Comparison | ||
| -2Log Likelihood of the Reduced Model | Chi-Square | df | Sig. | |
| Interception | 79.552 | 75.041 | 2 | 0.000 |
| sTNF-RII (pg/mg prot) | 66.945 | 62.433 | 2 | 0.000 |
| sIgA (ng/mg prot) | 5.343 | 0.831 | 2 | 0.660 |
| Parameter Estimates | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| PAINAD a (0–10 Points) c | B | Standard Error | Wald | df | Sig. | Exp(B) | 95% Confidence Interval for Exp(B) | ||
| Lower Limit | Upper Limit | ||||||||
| 1 | Interception | −61.291 | 3968.797 | 0.000 | 1 | 0.988 | |||
| sTNF-RII | 9.203 | 595.872 | 0.000 | 1 | 0.988 | 9923.542 | 0.000 | b | |
| sIgA | 0.001 | 0.738 | 0.000 | 1 | 0.999 | 1.001 | 0.236 | 04.255 | |
| 2 | Interception | −69.780 | 3968.804 | 0.000 | 1 | 0.986 | |||
| sTNF-RII | 9.801 | 595.872 | 0.000 | 1 | 0.987 | 18055.531 | 0.000 | b | |
| sIgA | 0.002 | 0.738 | 0.000 | 1 | 0.998 | 1.002 | 0.236 | 4.256 | |
| 4 | Interception | −164.123 | 8885.031 | 0.000 | 1 | 0.985 | |||
| sTNF-RII | 15.207 | 737.434 | 0.000 | 1 | 0.984 | 4020202.510 | 0.000 | b | |
| sIgA | 0.001 | 0.752 | 0.000 | 1 | 0.999 | 1.001 | 0.229 | 4.368 | |
| 5 | Interception | −333.143 | 20651.032 | 0.000 | 1 | 0.987 | |||
| sTNF-RII | 18.817 | 788.261 | 0.001 | 1 | 0.981 | 148569218.102 | 0.000 | b | |
| sIgA | 0.001 | 1.035 | 0.000 | 1 | 0.999 | 1.001 | 0.132 | 7.617 | |
| 6 | Interception | −393.108 | 20877.084 | 0.000 | 1 | 0.985 | |||
| sTNF-RII | 19.192 | 847.243 | 0.001 | 1 | 0.982 | 216275110.473 | 0.000 | b | |
| sIgA | 0.002 | 0.805 | 0.000 | 1 | 0.998 | 1.002 | 0.207 | 4.852 | |
| 8 | Interception | −414.142 | 0.000 | 1 | |||||
| sTNF-RII | 19.308 | 852.322 | 0.001 | 1 | 0.982 | 242920504.208 | 0.000 | b | |
| sIgA | 0.001 | 0.964 | 0.000 | 1 | 0.999 | 1.001 | 0.151 | 6.622 | |
| Likelihood Ratio Comparison | ||||
|---|---|---|---|---|
| Effect | Model Fit Criteria | Likelihood Ratio Comparison | ||
| -2Log Likelihood of the Reduced Model | Chi-Square | df | Sig. | |
| Interception | 178.552 | 174.056 | 6 | 0.000 |
| sTNF-RII | 110.324 | 105.827 | 6 | 0.000 |
| sIgA | 5.343 | 0.846 | 6 | 0.991 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantón-Habas, V.; Rich-Ruiz, M.; Moreno-Casbas, M.T.; Ramírez-Expósito, M.J.; Martínez-Martos, J.M.; Carrera-González, M.D.P. Correlation between Biomarkers of Pain in Saliva and PAINAD Scale in Elderly People with Cognitive Impairment and Inability to Communicate. J. Clin. Med. 2021, 10, 1424. https://doi.org/10.3390/jcm10071424
Cantón-Habas V, Rich-Ruiz M, Moreno-Casbas MT, Ramírez-Expósito MJ, Martínez-Martos JM, Carrera-González MDP. Correlation between Biomarkers of Pain in Saliva and PAINAD Scale in Elderly People with Cognitive Impairment and Inability to Communicate. Journal of Clinical Medicine. 2021; 10(7):1424. https://doi.org/10.3390/jcm10071424
Chicago/Turabian StyleCantón-Habas, Vanesa, Manuel Rich-Ruiz, María Teresa Moreno-Casbas, María Jesús Ramírez-Expósito, Jose Manuel Martínez-Martos, and María Del Pilar Carrera-González. 2021. "Correlation between Biomarkers of Pain in Saliva and PAINAD Scale in Elderly People with Cognitive Impairment and Inability to Communicate" Journal of Clinical Medicine 10, no. 7: 1424. https://doi.org/10.3390/jcm10071424