
MicroRNAs in Colon Tissue of Pediatric Ulcerative Pancolitis Patients Allow Detection and Prognostic Stratification

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Candidate miRNAs Selection
2.3. Nucleic Acid Isolation and miRNA Expression Analysis
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients
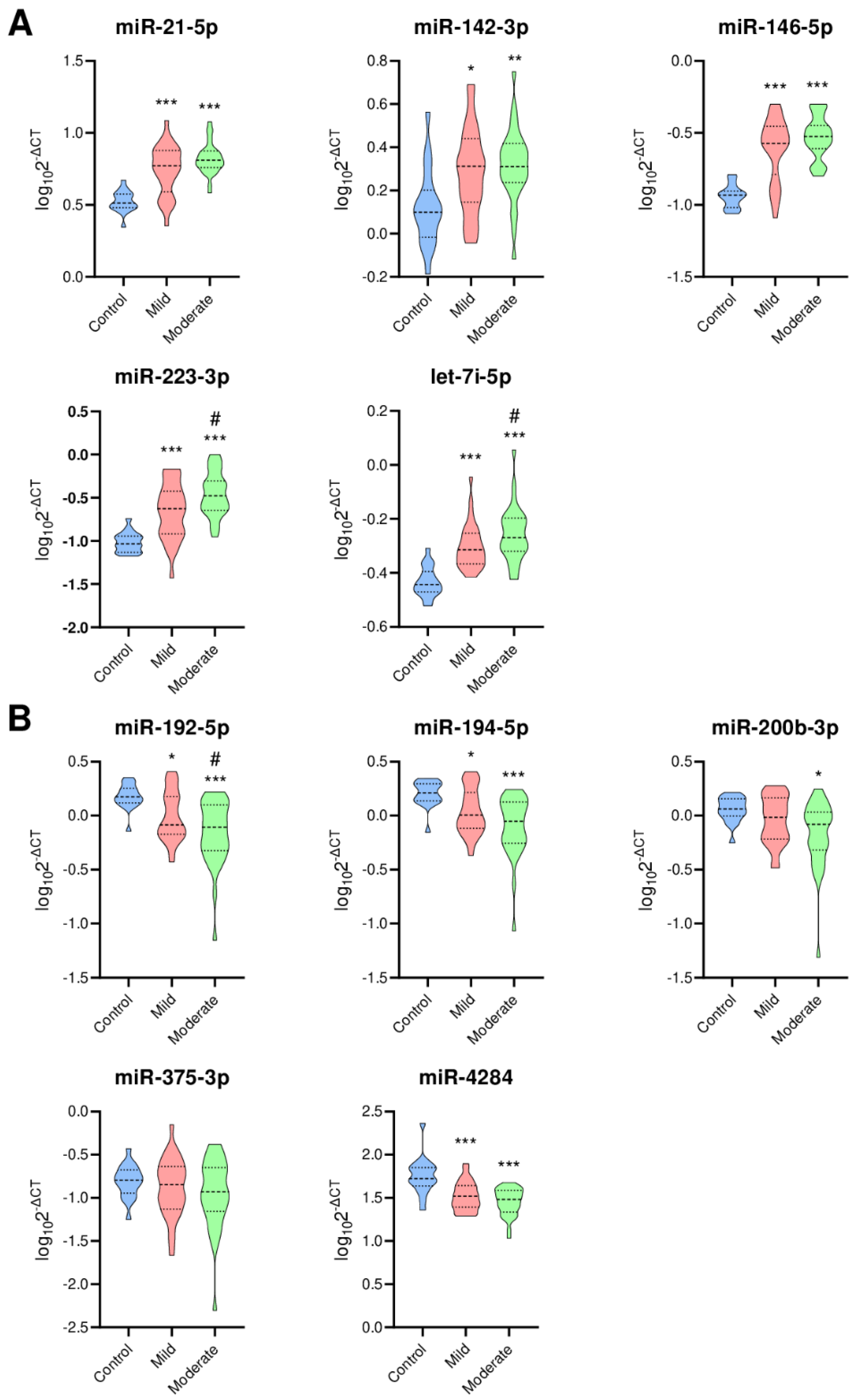
3.2. Expression of 10 Selected miRNAs
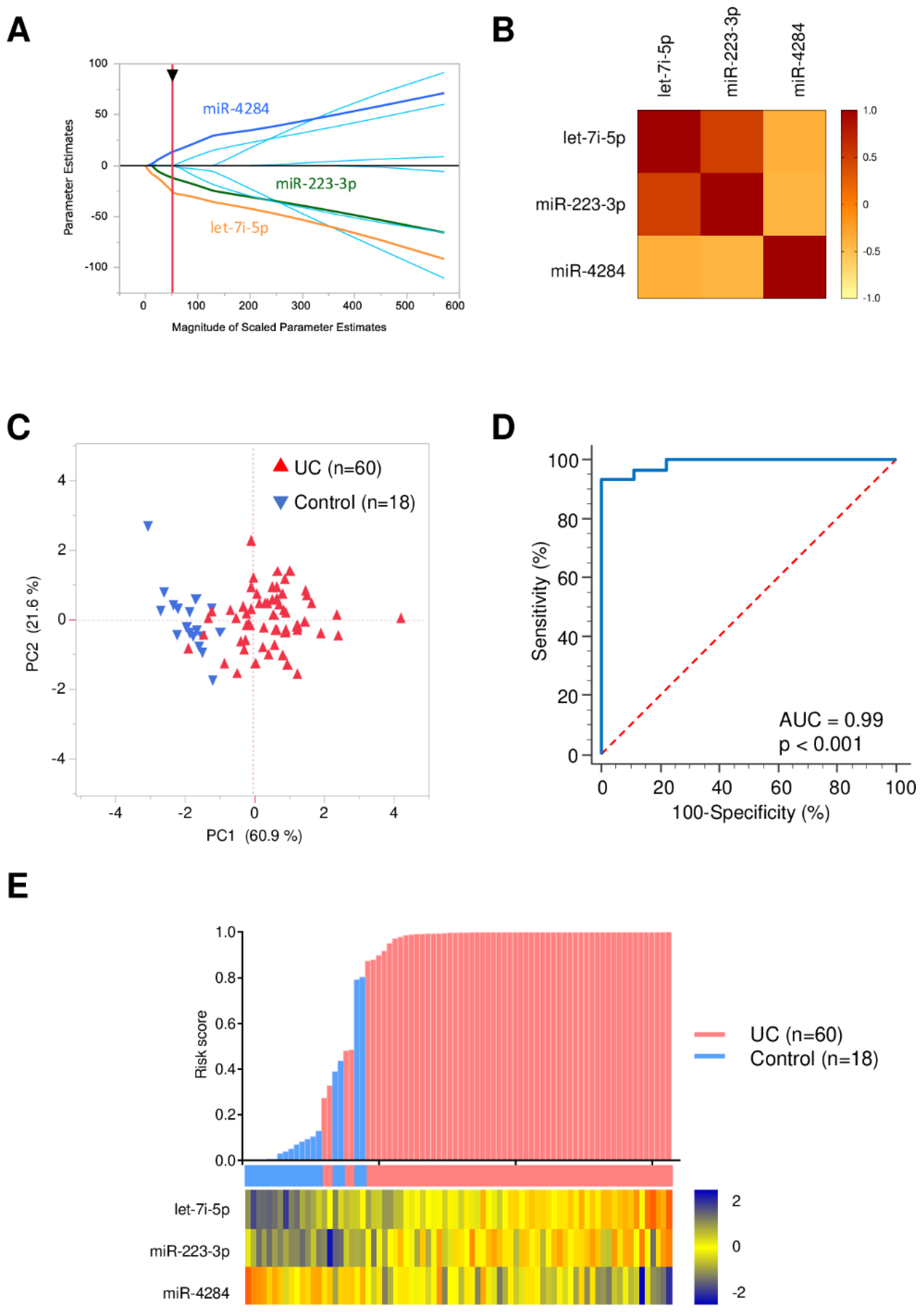
3.3. Identification of Robust miRNA Panel for UC Diagnosis
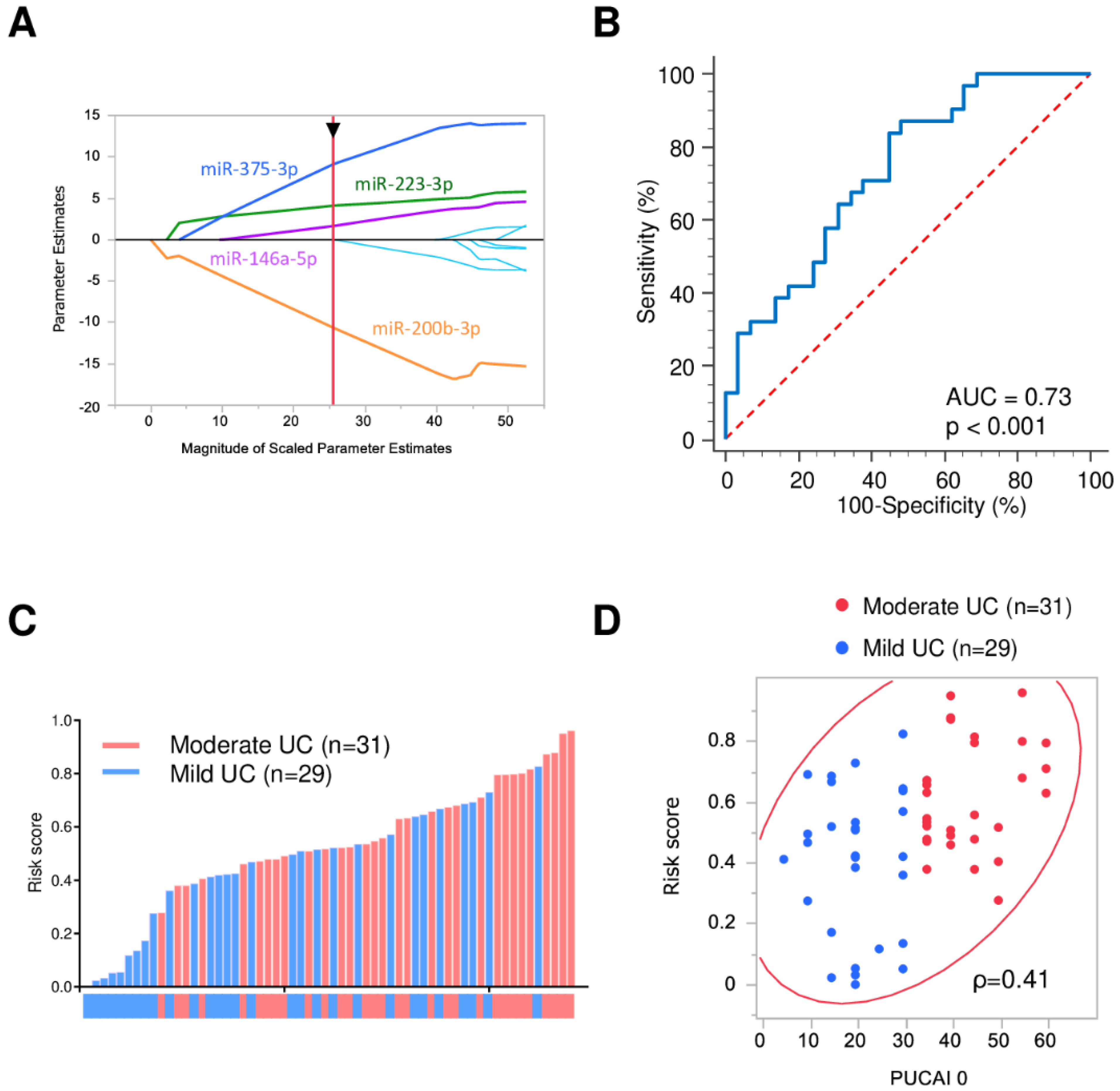
3.4. Severity Stratification Panel
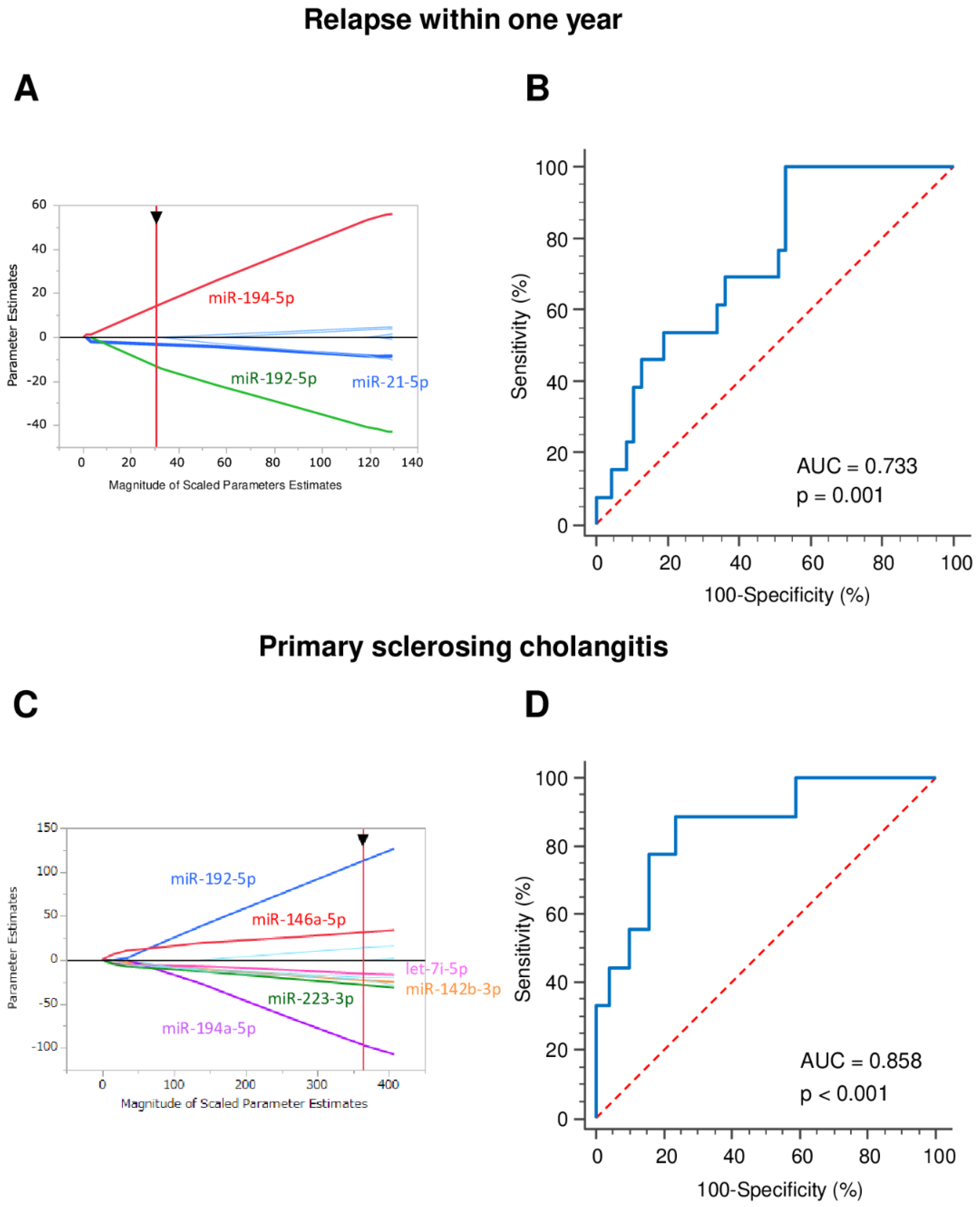
3.5. Early Relapse Prediction
3.6. Primary Sclerosing Cholangitis Identification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sartor, R.B. Mechanisms of disease: Pathogenesis of Crohn’s disease and ulcerative colitis. Nat. Clin. Pract. Gastroenterol. Hepatol. 2006, 3, 390–407. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Zhou, X.; Ma, J.; Zhou, W.; Yang, W.; Fan, D.; Hong, L. Role of MiRNAs in inflammatory bowel disease. Dig. Dis. Sci. 2017, 62, 1426–1438. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.P.; Bi, Y.J.; Liu, D.-M.; Wang, L.-Y. Hsa-miR-375 promotes the progression of inflammatory bowel disease by upregulating TLR4. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 7543–7549. [Google Scholar]
- Rosen, M.J.; Karns, R.; Vallance, J.E.; Bezold, R.; Waddell, A.; Collins, M.H.; Haberman, Y.; Minar, P.; Baldassano, R.N.; Hyams, J.S.; et al. Mucosal expression of type 2 and Type 17 immune response genes distinguishes ulcerative colitis from colon-only Crohn’s disease in treatment-naive pediatric patients. Gastroenterology 2017, 152, 1345–1357.e7. [Google Scholar] [CrossRef] [Green Version]
- Laborda, T.J.; Jensen, M.K.; Kavan, M.; Deneau, M. Treatment of primary sclerosing cholangitis in children. World J. Hepatol. 2019, 11, 19–36. [Google Scholar] [CrossRef] [PubMed]
- Jabandziev, P.; Pinkasova, T.; Kunovsky, L.; Papez, J.; Jouza, M.; Karlinova, B.; Novackova, M.; Urik, M.; Aulicka, S.; Slaby, O.; et al. Regional incidence of inflammatory bowel disease in a Czech pediatric population: 16 years of experience (2002–2017). J. Pediatr. Gastroenterol. Nutr. 2020, 70, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Sýkora, J.; Pomahačová, R.; Kreslová, M.; Cvalínová, D.; Štych, P.; Schwarz, J. Current global trends in the incidence of pediatric-onset inflammatory bowel disease. World J. Gastroenterol. 2018, 24, 2741–2763. [Google Scholar] [CrossRef]
- Kelsen, J.; Baldassano, R.N. Inflammatory bowel disease: The difference between children and adults. Inflamm. Bowel Dis. 2008, 14, S9–S11. [Google Scholar] [CrossRef]
- Turunen, P.; Ashorn, M.; Auvinen, A.; Iltanen, S.; Huhtala, H.; Kolho, K.-L. Long-term health outcomes in pediatric inflammatory bowel disease: A population-based study. Inflamm. Bowel Dis. 2009, 15, 56–62. [Google Scholar] [CrossRef]
- Guariso, G.; Gasparetto, M. Treating children with inflammatory bowel disease: Current and new perspectives. World J. Gastroenterol. 2017, 23, 5469–5485. [Google Scholar] [CrossRef]
- Naviglio, S.; Lacorte, D.; Lucafò, M.; Cifù, A.; Favretto, D.; Cuzzoni, E.; Silvestri, T.; Mucelli, M.P.; Radillo, O.; Decorti, G.; et al. Causes of treatment failure in children with inflammatory bowel disease treated with infliximab: A pharmacokinetic study. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Jabandziev, P.; Bohosova, J.; Pinkasova, T.; Kunovsky, L.; Slaby, O.; Goel, A. The emerging role of noncoding RNAs in pediatric inflammatory bowel disease. Inflamm. Bowel Dis. 2020, 26, 985–993. [Google Scholar] [CrossRef] [Green Version]
- IBD Working Group of the European Society for Paediatric Gastroenterology HpaN. Inflammatory bowel disease in children and adolescents: Recommendations for diagnosis—The Porto criteria. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Levine, A.; Koletzko, S.; Turner, D.; Escher, J.C.; Cucchiara, S.; de Ridder, L.; Kolho, K.-L.; Veres, G.; Russell, R.K.; Paerregaard, A.; et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 795–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, A.; Griffiths, A.; Markowitz, J.; Wilson, D.C.; Turner, D.; Russell, R.K.; Fell, J.; Ruemmele, F.M.; Walters, T.; Sherlock, M.; et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: The Paris classification. Inflamm. Bowel Dis. 2011, 17, 1314–1321. [Google Scholar] [CrossRef]
- Turner, D.; Hyams, J.; Markowitz, J.; Lerer, T.; Mack, D.R.; Evans, J.; Pfefferkorn, M.; Rosh, J.; Kay, M.; Crandall, W.; et al. Appraisal of the pediatric ulcerative colitis activity index (PUCAI). Inflamm. Bowel Dis. 2009, 15, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Bronský, J.; Beránková, K.; Černá, Z.; Čopová, I.; Durilová, M.; Hradský, O.; Karásková, E.; Mitrová, K.; Nevoral, J.; Poš, L.; et al. Czech Working Group for Paediatric Gastroenterology and Nutrition guidelines for diagnostics and treatment of inflammatory bowel diseases in children—1st edition update. Gastroenterol. Hepatol. 2017, 71, 11–18. [Google Scholar] [CrossRef]
- Zahm, A.M.; Hand, N.J.; Tsoucas, D.M.; Le Guen, C.L.; Baldassano, R.N.; Friedman, J.R. Rectal microRNAs are perturbed in pediatric inflammatory bowel disease of the colon. J. Crohns Colitis 2014, 8, 1108–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Béres, N.J.; Szabó, D.; Kocsis, D.; Szűcs, D.; Kiss, Z.; Müller, K.E.; Lendvai, G.A.; Kiss, A.; Arató, A.; Sziksz, E.; et al. Role of altered expression of miR-146a, miR-155, and miR-122 in pediatric patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2016, 22, 327–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Béres, N.J.; Kiss, Z.; Sztupinszki, Z.; Lendvai, G.; Arató, A.; Sziksz, E.; Vannay, Á.; Szabó, A.J.; Müller, K.E.; Cseh, Á.; et al. Altered mucosal expression of microRNAs in pediatric patients with inflammatory bowel disease. Dig. Liver Dis. 2017, 49, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Leon-Cabrera, S.; Vázquez-Sandoval, A.; Molina-Guzman, E.; Delgado-Ramirez, Y.; Delgado-Buenrostro, N.L.; Callejas, B.E.; Chirino, Y.I.; Pérez-Plasencia, C.; Rodríguez-Sosa, M.; Olguín, J.E.; et al. Deficiency in STAT1 signaling predisposes gut inflammation and prompts colorectal cancer development. Cancers 2018, 10, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles, E.M.; Sanders, T.J.; McCarthy, N.E.; Lung, J.; Pathak, M.; Macdonald, T.T.; Lindsay, J.O.; Stagg, A.J. Regulation of human intestinal T-cell responses by type 1 interferon-STAT1 signaling is disrupted in inflammatory bowel disease. Mucosal Immunol. 2017, 10, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giroud, M.; Karbiener, M.; Pisani, D.F.; Ghandour, R.A.; Beranger, G.E.; Niemi, T.; Taittonen, M.; Nuutila, P.; Virtanen, K.A.; Langin, D.; et al. Let-7i-5p represses brite adipocyte function in mice and humans. Sci. Rep. 2016, 6, 28613. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Zhang, L. Members of the microRNA-200 family are promising therapeutic targets in cancer. Exp. Ther. Med. 2017, 14, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Lewis, A.; Felice, C.; Kumagai, T.; Lai, C.; Singh, K.; Jeffery, R.R.; Feakins, R.; Giannoulatou, E.; Armuzzi, A.; Jawad, N.; et al. The miR-200 family is increased in dysplastic lesions in ulcerative colitis patients. PLoS ONE 2017, 12, e0173664. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Huang, Y.; Zhou, C.; Wu, H.; Zhao, J.; Wu, L.; Zhao, M.; Zhang, F.; Liu, H. The role of autophagy and related MicroRNAs in inflammatory bowel disease. Gastroenterol. Res. Pract. 2018, 2018, 1–10. [Google Scholar] [CrossRef]
- Duijvis, N.W.; Moerland, P.D.; Kunne, C.; Slaman, M.M.W.; Van Dooren, F.H.; Vogels, E.W.; De Jonge, W.J.; Meijer, S.L.; Fluiter, K.; Velde, A.A.T. Inhibition of miR-142-5P ameliorates disease in mouse models of experimental colitis. PLoS ONE 2017, 12, e0185097. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Gao, J.; Zhang, S.; Gu, J.; Lu, H.; Xia, Y.; Zhu, Q.; Qian, X.; Zhang, F.; Zhang, C.; et al. miR-142-3p regulates autophagy by targeting ATG16L1 in thymic-derived regulatory T cell (tTreg). Cell Death Dis. 2018, 9, 1–10. [Google Scholar] [CrossRef]
- Qian, M.; Fang, X.; Wang, X. Autophagy and inflammation. Clin. Transl. Med. 2017, 6, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonkoly, E.; Ståhle, M.; Pivarcsi, A. MicroRNAs and immunity: Novel players in the regulation of normal immune function and inflammation. Semin. Cancer Biol. 2008, 18, 131–140. [Google Scholar] [CrossRef]
- Lin, J.; Zhang, X.; Zhao, Z.; Welker, N.C.; Li, Y.; Liu, Y.; Bronner, M.B. Novel MicroRNA signature to differentiate ulcerative colitis from Crohn disease: A genome-wide study using next generation sequencing. Microrna 2016, 5, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Sheedy, F.J. Turning 21: Induction of miR-21 as a key switch in the inflammatory response. Front. Immunol. 2015, 6, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludwig, K.; Fassan, M.; Mescoli, C.; Pizzi, M.; Balistreri, M.; Albertoni, L.; Pucciarelli, S.; Scarpa, M.; Sturniolo, G.C.; Angriman, I.; et al. PDCD4/miR-21 dysregulation in inflammatory bowel disease-associated carcinogenesis. Virchows Arch. Pathol. Anat. Physiol. Klin. Med. 2013, 462, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Persson, T.; Monsef, N.; Andersson, P.; Bjartell, A.; Malm, J.; Calafat, J.; Egesten, A. Expression of the neutrophil-activating CXC chemokine ENA-78/CXCL5 by human eosinophils. Clin. Exp. Allergy 2003, 33, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Koukos, G.; Polytarchou, C.; Kaplan, J.L.; Oikonomopoulos, A.; Ziring, D.; Hommes, D.W.; Wahed, R.; Kokkotou, E.; Pothoulakis, C.; Winter, H.S.; et al. A microRNA signature in pediatric ulcerative colitis: Deregulation of the miR-4284/CXCL5 pathway in the intestinal epithelium. Inflamm. Bowel Dis. 2015, 21, 996–1005. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Liu, Q.; Peng, J.; Wang, M.; Li, T.; Liu, J.; Cui, M.; Zhang, X.; Gao, X.; Liao, Q.; et al. CXCL5 overexpression predicts a poor prognosis in pancreatic ductal adenocarcinoma and is correlated with immune cell infiltration. J. Cancer 2020, 11, 2371–2381. [Google Scholar] [CrossRef]
- Tenca, A.; Jaakkola, T.; Färkkilä, M.; Arola, J.; Kolho, K.-L. Impact of paediatric onset primary sclerosing cholangitis on clinical course and outcome of inflammatory bowel disease: A case-control population-based study in Finland. Scand. J. Gastroenterol. 2019, 54, 984–990. [Google Scholar] [CrossRef]
- Dyson, J.K.; Beuers, U.; Jones, D.E.J.; Lohse, A.W.; Hudson, M. Primary sclerosing cholangitis. Lancet 2018, 391, 2547–2559. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Severity of the Disease (PUCAI Score) | Mild | Moderate | Total |
|---|---|---|---|
| 29 (48.3%) | 31 (51.7%) | 60 (100%) | |
| Sex, N (%) | |||
| Male | 13 (44.8%) | 13 (41.9%) | 26 |
| Female | 16 (55.2%) | 18 (58.1%) | 34 |
| Mean age at diagnosis (years) | 13.7 | 13.9 | 13.7 |
| Mean PUCAI: | |||
| At diagnosis | 20.7 | 43.7 | 32.3 |
| After 3 months | 2.2 | 5.0 | 3.7 |
| Treatment, N (%) | |||
| Mesalazine | 29 (100%) | 31 (100%) | 60 (100%) |
| Corticosteroids | 18 (62%) | 25 (80.6%) | 43 (71.7%) |
| Response rate to initial treatment, N (%) | 26 (89.7%) | 25 (80.6%) | 51 (85%) |
| Early relapse, N (%) | 6 (20.7%) | 7 (22.6%) | 13 (21.7%) |
| Primary sclerosing cholangitis, N (%) | 6 (20.7%) | 3 (9.7%) | 9 (15%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabandziev, P.; Kakisaka, T.; Bohosova, J.; Pinkasova, T.; Kunovsky, L.; Slaby, O.; Goel, A. MicroRNAs in Colon Tissue of Pediatric Ulcerative Pancolitis Patients Allow Detection and Prognostic Stratification. J. Clin. Med. 2021, 10, 1325. https://doi.org/10.3390/jcm10061325
Jabandziev P, Kakisaka T, Bohosova J, Pinkasova T, Kunovsky L, Slaby O, Goel A. MicroRNAs in Colon Tissue of Pediatric Ulcerative Pancolitis Patients Allow Detection and Prognostic Stratification. Journal of Clinical Medicine. 2021; 10(6):1325. https://doi.org/10.3390/jcm10061325
Chicago/Turabian StyleJabandziev, Petr, Tatsuhiko Kakisaka, Julia Bohosova, Tereza Pinkasova, Lumir Kunovsky, Ondrej Slaby, and Ajay Goel. 2021. "MicroRNAs in Colon Tissue of Pediatric Ulcerative Pancolitis Patients Allow Detection and Prognostic Stratification" Journal of Clinical Medicine 10, no. 6: 1325. https://doi.org/10.3390/jcm10061325