
Therapeutic Outcomes and Prognostic Factors of Unresectable Intrahepatic Cholangiocarcinoma: A Data Mining Analysis

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
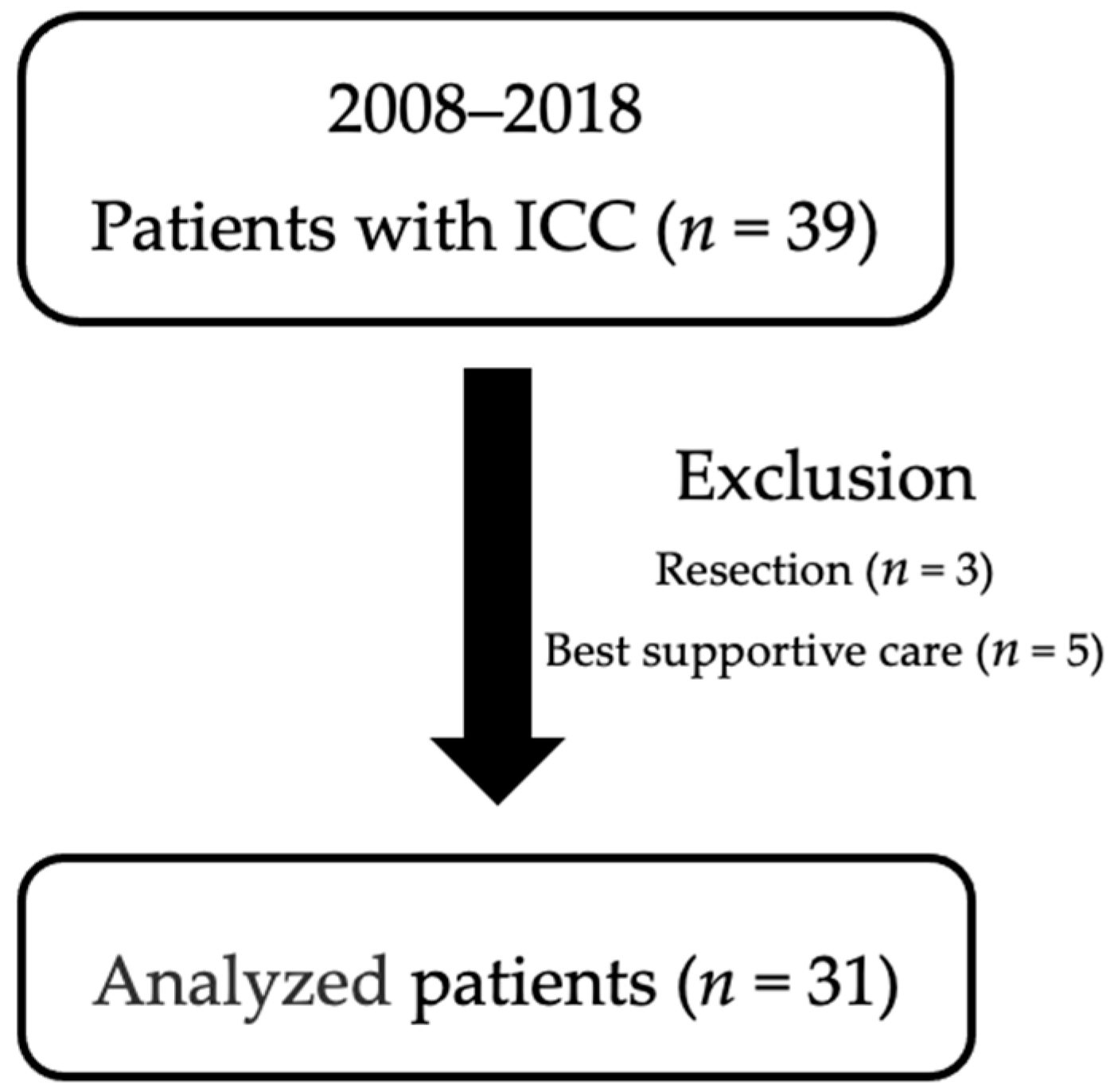
2.2. Subjects
2.3. Diagnosis of ICC
2.4. Inclusion and Exclusion Criteria
2.5. Data Collection
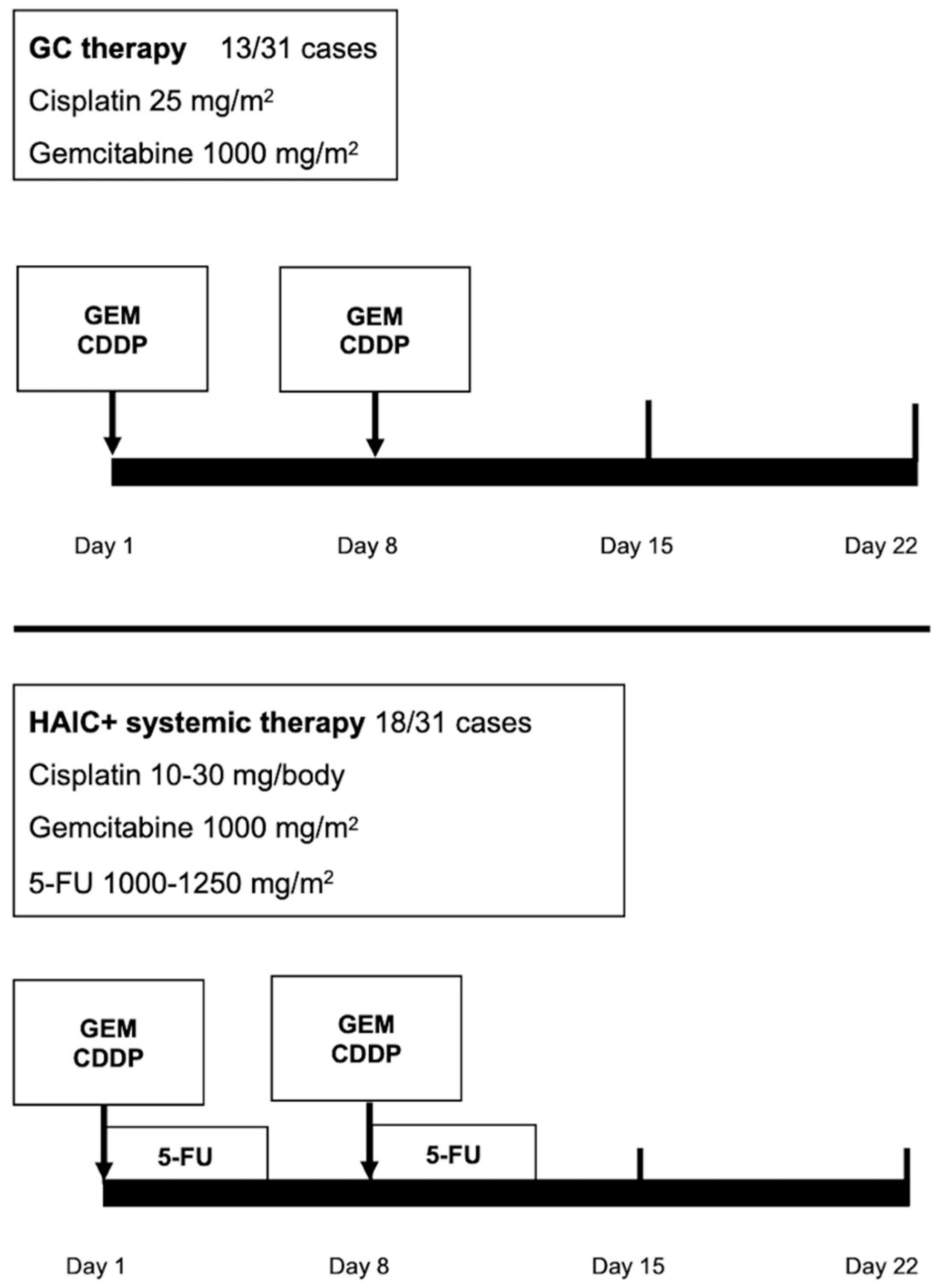
2.6. Treatment for ICC
2.7. Systemic Chemotherapy
2.8. HAIC Procedure
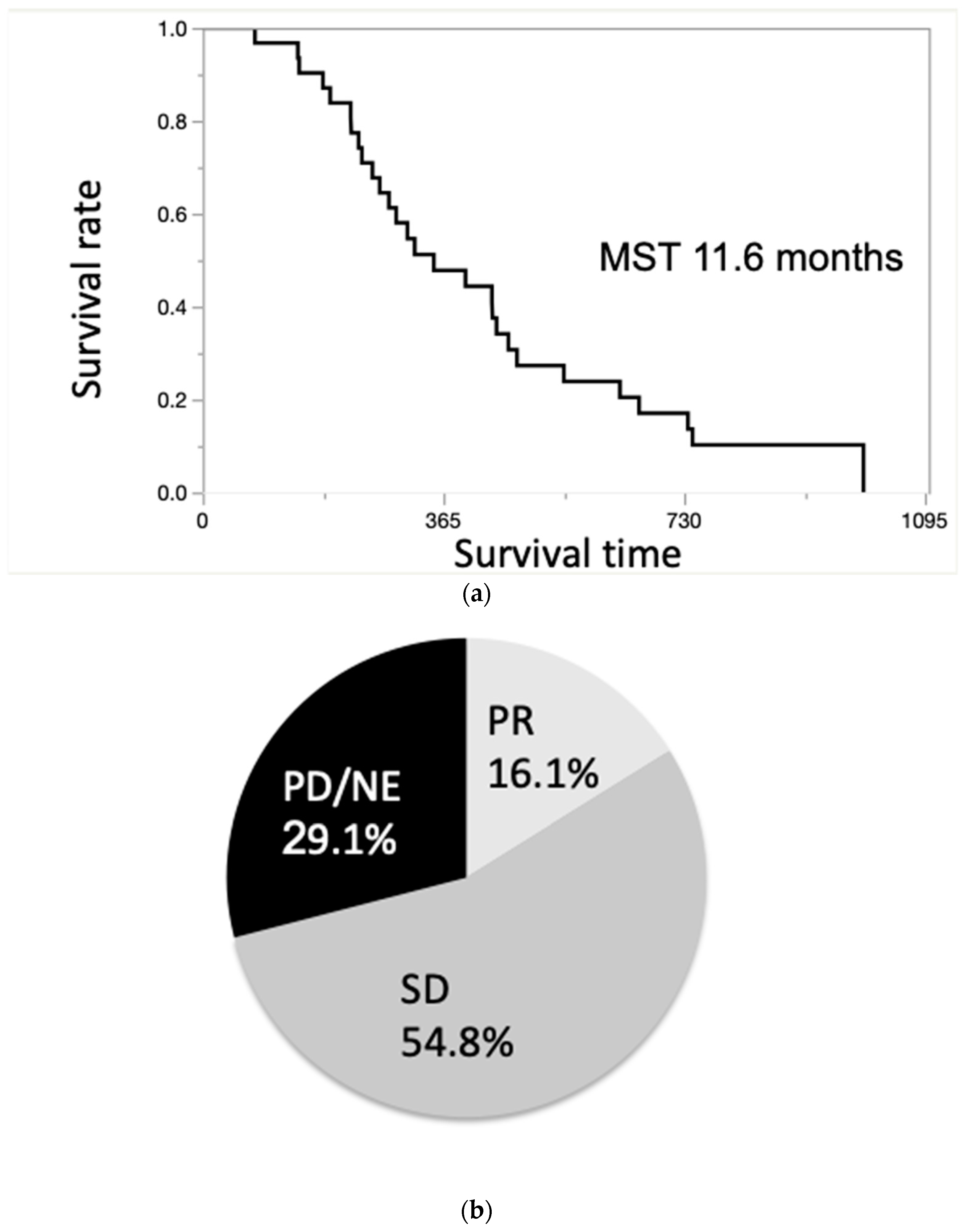
2.9. Main Outcomes
2.10. Survival Period
2.11. Follow-Up Process and Assessment of Response
2.12. Safety and Complications Evaluation
2.13. Statistics
3. Results
3.1. Characteristics of Patients with ICC
3.2. Therapeutic Effects
3.3. Multivariate Correlation Analysis for Survival Time
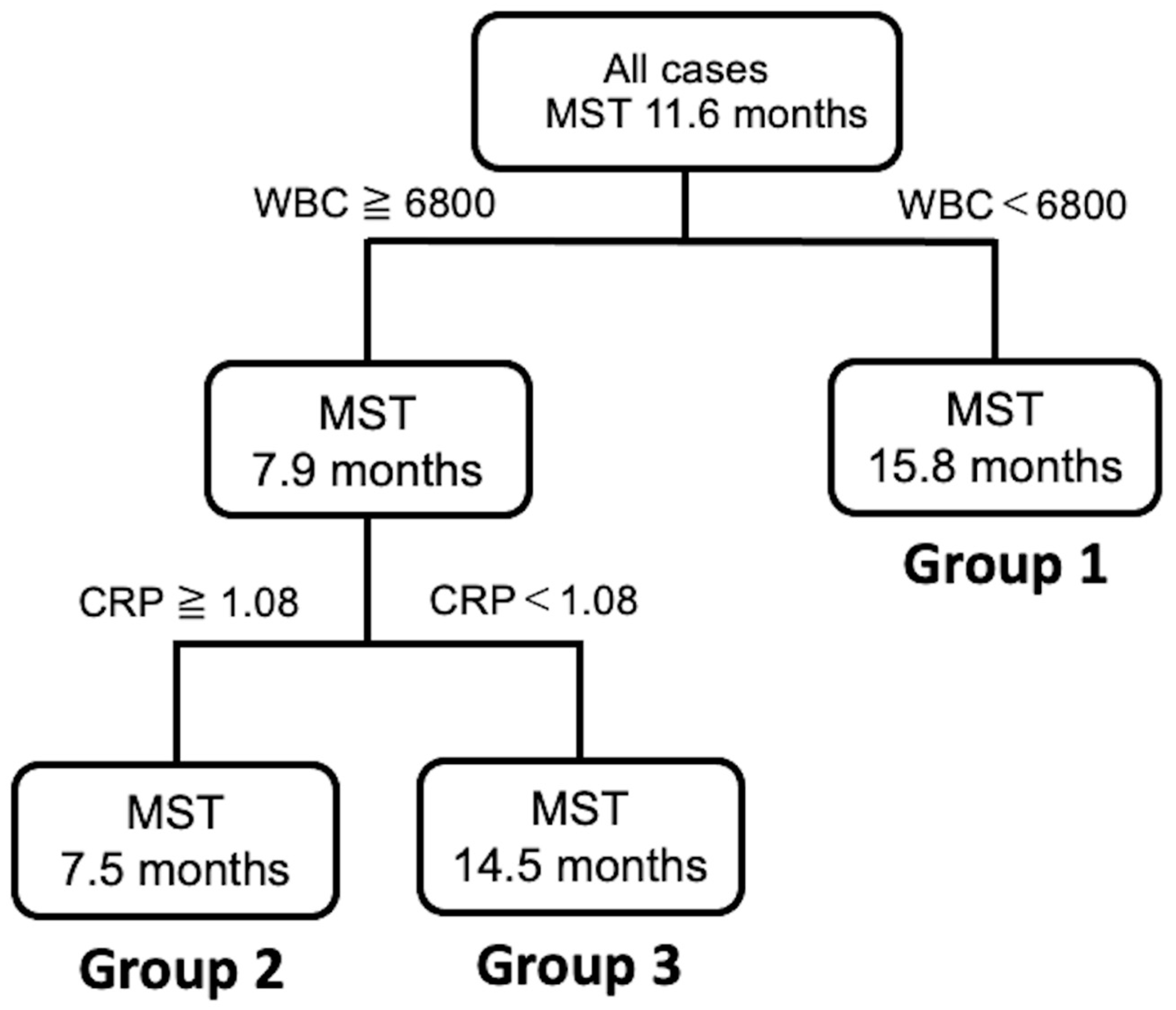
3.4. Decision Tree Analysis for Prognosis
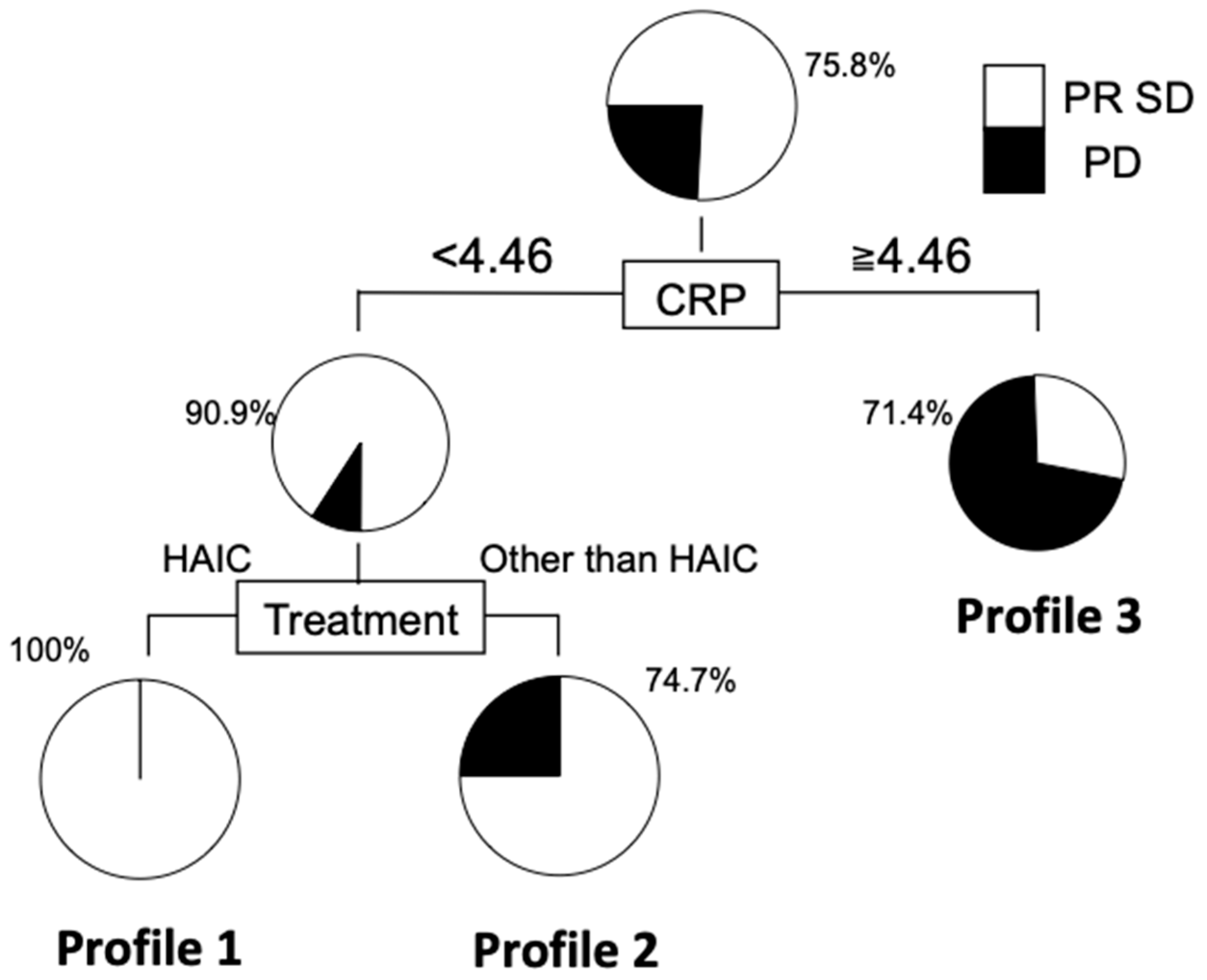
3.5. Decision Tree Analysis for Disease Control of ICC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laohaviroj, M.; Potriquet, J.; Jia, X.; Suttiprapa, S.; Chamgramol, Y.; Pairojkul, C.; Sithithaworn, P.; Mulvenna, J.; Sripa, B. A comparative proteomic analysis of bile for biomarkers of cholangiocarcinoma. Tumour. Biol. 2017, 39, 1010428317705764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudo, M.; Izumi, N.; Ichida, T.; Ku, Y.; Kokudo, N.; Sakamoto, M.; Takayama, T.; Nakashima, O.; Matsui, O.; Matsuyama, Y. Report of the 19th follow-up survey of primary liver cancer in Japan. Hepatol. Res. 2016, 46, 372–390. [Google Scholar] [CrossRef]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [Green Version]
- Yoh, T.; Hatano, E.; Yamanaka, K.; Nishio, T.; Seo, S.; Taura, K.; Yasuchika, K.; Okajima, H.; Kaido, T.; Uemoto, S. Is Surgical Resection Justified for Advanced Intrahepatic Cholangiocarcinoma? Liver Cancer 2016, 5, 280–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.B.; Kim, K.S.; Choi, J.Y.; Park, S.W.; Choi, J.S.; Lee, W.J.; Chung, J.B. The prognosis and survival outcome of intrahepatic cholangiocarcinoma following surgical resection: Association of lymph node metastasis and lymph node dissection with survival. Ann. Surg. Oncol. 2009, 16, 3048–3056. [Google Scholar] [CrossRef] [PubMed]
- Lang, H.; Sotiropoulos, G.C.; Sgourakis, G.; Schmitz, K.J.; Paul, A.; Hilgard, P.; Zopf, T.; Trarbach, T.; Malago, M.; Baba, H.A.; et al. Operations for intrahepatic cholangiocarcinoma: Single-institution experience of 158 patients. J. Am. Coll. Surg. 2009, 208, 218–228. [Google Scholar] [CrossRef]
- Le Roy, B.; Gelli, M.; Pittau, G.; Allard, M.A.; Pereira, B.; Serji, B.; Vibert, E.; Castaing, D.; Adam, R.; Cherqui, D.; et al. Neoadjuvant chemotherapy for initially unresectable intrahepatic cholangiocarcinoma. Br. J. Surg. 2018, 105, 839–847. [Google Scholar] [CrossRef]
- Sumiyoshi, T.; Shima, Y.; Okabayashi, T.; Negoro, Y.; Shimada, Y.; Iwata, J.; Matsumoto, M.; Hata, Y.; Noda, Y.; Sui, K.; et al. Chemoradiotherapy for Initially Unresectable Locally Advanced Cholangiocarcinoma. World J. Surg. 2018, 42, 2910–2918. [Google Scholar] [CrossRef] [PubMed]
- Mavros, M.N.; Economopoulos, K.P.; Alexiou, V.G.; Pawlik, T.M. Treatment and Prognosis for Patients with Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-analysis. JAMA Surg. 2014, 149, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, B.W.; Wright, G.P. Regional therapies for the treatment of primary and metastatic hepatic tumors: A disease-based review of techniques and critical appraisal of current evidence. Am. J. Surg. 2019, 217, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M. Treatment of advanced hepatocellular carcinoma with emphasis on hepatic arterial infusion chemotherapy and molecular targeted therapy. Liver Cancer 2012, 1, 62–70. [Google Scholar] [CrossRef]
- Obi, S.; Sato, S.; Kawai, T. Current Status of Hepatic Arterial Infusion Chemotherapy. Liver Cancer 2015, 4, 188–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasai, K.; Kooka, Y.; Suzuki, Y.; Suzuki, A.; Oikawa, T.; Ushio, A.; Kasai, Y.; Sawara, K.; Miyamoto, Y.; Oikawa, K.; et al. Efficacy of hepatic arterial infusion chemotherapy using 5-fluorouracil and systemic pegylated interferon alpha-2b for advanced intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2014, 21, 3638–3645. [Google Scholar] [CrossRef]
- Konstantinidis, I.T.; Groot Koerkamp, B.; Do, R.K.; Gonen, M.; Fong, Y.; Allen, P.J.; D’Angelica, M.I.; Kingham, T.P.; DeMatteo, R.P.; Klimstra, D.S.; et al. Unresectable intrahepatic cholangiocarcinoma: Systemic plus hepatic arterial infusion chemotherapy is associated with longer survival in comparison with systemic chemotherapy alone. Cancer 2016, 122, 758–765. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Ricci, A.D.; Brandi, G. Futibatinib, an investigational agent for the treatment of intrahepatic cholangiocarcinoma: Evidence to date and future perspectives. Expert Opin. Investig. Drugs 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bellazzi, R.; Zupan, B. Predictive data mining in clinical medicine: Current issues and guidelines. Int. J. Med. Inform. 2008, 77, 81–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurosaki, M.; Matsunaga, K.; Hirayama, I.; Tanaka, T.; Sato, M.; Yasui, Y.; Tamaki, N.; Hosokawa, T.; Ueda, K.; Tsuchiya, K.; et al. A predictive model of response to peginterferon ribavirin in chronic hepatitis C using classification and regression tree analysis. Hepatol. Res. 2010, 40, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Pauker, S.G.; Kassirer, J.P. The threshold approach to clinical decision making. N. Engl. J. Med. 1980, 302, 1109–1117. [Google Scholar] [CrossRef]
- Yamada, S.; Kawaguchi, A.; Kawaguchi, T.; Fukushima, N.; Kuromatsu, R.; Sumie, S.; Takata, A.; Nakano, M.; Satani, M.; Tonan, T.; et al. Serum albumin level is a notable profiling factor for non-B, non-C hepatitis virus-related hepatocellular carcinoma: A data-mining analysis. Hepatol. Res. 2014, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Diouf, M.; Filleron, T.; Pointet, A.L.; Dupont-Gossard, A.C.; Malka, D.; Artru, P.; Gauthier, M.; Lecomte, T.; Aparicio, T.; Thirot-Bidault, A.; et al. Prognostic value of health-related quality of life in patients with metastatic pancreatic adenocarcinoma: A random forest methodology. Qual. Life Res. 2016, 25, 1713–1723. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.M.; Yu, Y.W.; Cheng, B.W.; Kuo, Y.L. Construction the model on the breast cancer survival analysis use support vector machine, logistic regression and decision tree. J. Med. Syst. 2014, 38, 106. [Google Scholar] [CrossRef] [PubMed]
- Masic, N.; Gagro, A.; Rabatic, S.; Sabioncello, A.; Dasic, G.; Jaksic, B.; Vitale, B. Decision-tree approach to the immunophenotype-based prognosis of the B-cell chronic lymphocytic leukemia. Am. J. Hematol. 1998, 59, 143–148. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Mehta, R.; Moris, D.; Sahara, K.; Bagante, F.; Paredes, A.Z.; Moro, A.; Guglielmi, A.; Aldrighetti, L.; Weiss, M.; et al. A Machine-Based Approach to Preoperatively Identify Patients with the Most and Least Benefit Associated with Resection for Intrahepatic Cholangiocarcinoma: An International Multi-Institutional Analysis of 1146 Patients. Ann. Surg. Oncol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Cantore, M.; Mambrini, A.; Fiorentini, G.; Rabbi, C.; Zamagni, D.; Caudana, R.; Pennucci, C.; Sanguinetti, F.; Lombardi, M.; Nicoli, N. Phase II study of hepatic intraarterial epirubicin and cisplatin, with systemic 5-fluorouracil in patients with unresectable biliary tract tumors. Cancer 2005, 103, 1402–1407. [Google Scholar] [CrossRef]
- Shitara, K.; Ikami, I.; Munakata, M.; Muto, O.; Sakata, Y. Hepatic arterial infusion of mitomycin C with degradable starch microspheres for unresectable intrahepatic cholangiocarcinoma. Clin. Oncol. (R Coll Radiol) 2008, 20, 241–246. [Google Scholar] [CrossRef]
- Morizane, C.; Okusaka, T.; Mizusawa, J.; Takashima, A.; Ueno, M.; Ikeda, M.; Hamamoto, Y.; Ishii, H.; Boku, N.; Furuse, J. Randomized phase II study of gemcitabine plus S-1 versus S-1 in advanced biliary tract cancer: A Japan Clinical Oncology Group trial (JCOG 0805). Cancer Sci. 2013, 104, 1211–1216. [Google Scholar] [CrossRef]
- Sasaki, T.; Isayama, H.; Nakai, Y.; Ito, Y.; Yasuda, I.; Toda, N.; Kogure, H.; Hanada, K.; Maguchi, H.; Sasahira, N.; et al. A randomized phase II study of gemcitabine and S-1 combination therapy versus gemcitabine monotherapy for advanced biliary tract cancer. Cancer Chemother. Pharmacol. 2013, 71, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ando, E.; Tanaka, M.; Yamashita, F.; Kuromatsu, R.; Yutani, S.; Fukumori, K.; Sumie, S.; Yano, Y.; Okuda, K.; Sata, M. Hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis: Analysis of 48 cases. Cancer 2002, 95, 588–595. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Chen, A.P.; Setser, A.; Anadkat, M.J.; Cotliar, J.; Olsen, E.A.; Garden, B.C.; Lacouture, M.E. Grading dermatologic adverse events of cancer treatments: The Common Terminology Criteria for Adverse Events Version 4.0. J. Am. Acad. Dermatol. 2012, 67, 1025–1039. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Enviroment For Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2012. [Google Scholar]
- Allin, K.H.; Nordestgaard, B.G. Elevated C-reactive protein in the diagnosis, prognosis, and cause of cancer. Crit. Rev. Clin. Lab Sci. 2011, 48, 155–170. [Google Scholar] [CrossRef]
- Lin, Z.Y.; Liang, Z.X.; Zhuang, P.L.; Chen, J.W.; Cao, Y.; Yan, L.X.; Yun, J.P.; Xie, D.; Cai, M.Y. Intrahepatic cholangiocarcinoma prognostic determination using pre-operative serum C-reactive protein levels. BMC Cancer 2016, 16, 792. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.S.; Kim, S.Y.; Koh, M.; Lee, H.M.; Kim, K.; Jung, J.; Kim, H.S.; Moon, W.K.; Hwang, S.; Moon, A. C-reactive protein binds to integrin alpha2 and Fcgamma receptor I, leading to breast cell adhesion and breast cancer progression. Oncogene 2018, 37, 28–38. [Google Scholar] [CrossRef]
- Schimmack, S.; Yang, Y.; Felix, K.; Herbst, M.; Li, Y.; Schenk, M.; Bergmann, F.; Hackert, T.; Strobel, O. C-reactive protein (CRP) promotes malignant properties in pancreatic neuroendocrine neoplasms. Endocr Connect. 2019, 8, 1007–1019. [Google Scholar] [CrossRef] [Green Version]
- Buettner, S.; Spolverato, G.; Kimbrough, C.W.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Gamblin, T.C.; Maithel, S.K.; Pulitano, C.; et al. The impact of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio among patients with intrahepatic cholangiocarcinoma. Surgery 2018, 164, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.; Harimoto, N.; Araki, K.; Kubo, N.; Igarashi, T.; Tsukagoshi, M.; Ishii, N.; Yamanaka, T.; Yoshizumi, T.; Shirabe, K. Absolute Neutrophil Count Predicts Postoperative Prognosis in Mass-forming Intrahepatic Cholangiocarcinoma. Anticancer. Res. 2019, 39, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Kawai, M.; Hirono, S.; Okada, K.I.; Miyazawa, M.; Shimizu, A.; Kitahata, Y.; Kobayashi, R.; Ueno, M.; Hayami, S.; Tanioka, K.; et al. Low lymphocyte monocyte ratio after neoadjuvant therapy predicts poor survival after pancreatectomy in patients with borderline resectable pancreatic cancer. Surgery 2019, 165, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Xu, Z.; Huang, Y.; Zhao, R.; Cui, Y.; Zhou, Y.; Wu, X. The predictive value and the correlation of peripheral absolute monocyte count, tumor-associated macrophage and microvessel density in patients with colon cancer. Medicine (Baltimore) 2018, 97, e10759. [Google Scholar] [CrossRef]
- Urakawa, S.; Yamasaki, M.; Goto, K.; Haruna, M.; Hirata, M.; Morimoto-Okazawa, A.; Kawashima, A.; Iwahori, K.; Makino, T.; Kurokawa, Y.; et al. Peri-operative monocyte count is a marker of poor prognosis in gastric cancer: Increased monocytes are a characteristic of myeloid-derived suppressor cells. Cancer Immunol. Immunother. 2019, 68, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Peng, D.; Lu, J.; Hu, H.; Li, B.; Ye, X.; Cheng, N. Lymphocyte to Monocyte Ratio Predicts Resectability and Early Recurrence of Bismuth-Corlette Type IV Hilar Cholangiocarcinoma. J. Gastrointest. Surg. 2020, 24, 330–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subimerb, C.; Pinlaor, S.; Lulitanond, V.; Khuntikeo, N.; Okada, S.; McGrath, M.S.; Wongkham, S. Circulating CD14(+) CD16(+) monocyte levels predict tissue invasive character of cholangiocarcinoma. Clin. Exp. Immunol. 2010, 161, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Miyata, T.; Yamashita, Y.I.; Yoshizumi, T.; Shiraishi, M.; Ohta, M.; Eguchi, S.; Aishima, S.; Fujioka, H.; Baba, H. CXCL12 expression in intrahepatic cholangiocarcinoma is associated with metastasis and poor prognosis. Cancer Sci. 2019, 110, 3197–3203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayers, P.M.; Machin, D. Sample size: How many patients are necessary? Br. J. Cancer. 1995, 72, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Number or Median (Range) |
|---|---|
| Age (years) | 71 (50–90) |
| ECOG PS 0/1/2 | 26/4/1 |
| Sex Male/Female | 18/13 |
| Etiology HBV/HCV/non-B, non-C | 3/1/27 |
| Stage II/III/IVA/IVB | 6/4/5/16 |
| Tumor size (mm) | 74 (20–197) |
| Total bilirubin (mg/dL) | 0.92 (0.39–33.88) |
| AST (U/L) | 48 (19–347) |
| ALT (U/L) | 26 (11–443) |
| LDH (U/L) | 291 (142–2511) |
| γ-GTP (U/L) | 181 (14–3025) |
| ALP (U/L) | 455 (240–3256) |
| Albumin (g/dL) | 3.55 (2.49–4.36) |
| BUN (mg/dL) | 14.4 (7.3–24.5) |
| Creatinine (mg/dL) | 0.68 (0.41–1.12) |
| CRP (mg/dL) | 0.95 (0.06–22) |
| Sodium (mEq/L) | 139 (135–143) |
| Potassium (mEq/L) | 4.1 (3.6–5.4) |
| Chloride (mEq/L) | 104 (98–107) |
| Hb (g/dL) | 12.9 (8.9–16.5) |
| White blood cells (/μL) | 6300 (2600–14,600) |
| Neutrophils (/μL) | 4718.7 (1562.6–13,484.9) |
| NLR | 3.19 (1.82–28.58) |
| CEA (ng/mL) | 3.4 (1.2–104.9) |
| CA 19-9 (U/mL) | 106.2 (1–6293.6) |
| Survival Time | WBC | NLR | CRP | CEA | CA 19-9 | Tumor Size | T-Bili | ALB | γ-GTP | Sodium | BUN | Creatinine | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Survival time | 1.0000 | −0.4008 | −0.2068 | −0.3535 | −0.1906 | −0.2955 | −0.0900 | −0.0445 | 0.3572 | −0.0872 | 0.2733 | 0.1841 | −0.1699 |
| WBC | −0.4008 | 1.0000 | 0.4877 | 0.1128 | −0.0399 | 0.1296 | 0.1533 | 0.0332 | −0.4599 | 0.1729 | −0.3679 | 0.0802 | −0.0499 |
| NLR | −0.2068 | 0.4877 | 1.0000 | 0.2253 | −0.1303 | −0.1574 | 0.0110 | −0.0817 | −0.3592 | −0.1277 | −0.2184 | 0.2264 | −0.0644 |
| CRP | −0.3535 | 0.1128 | 0.2253 | 1.0000 | 0.1262 | 0.0921 | −0.0990 | 0.1523 | −0.1782 | −0.0594 | −0.1096 | −0.1443 | −0.0026 |
| CEA | −0.1906 | −0.0399 | −0.1303 | 0.1262 | 1.0000 | 0.4246 | −0.0804 | 0.0123 | −0.3247 | −0.0249 | −0.1701 | −0.0431 | 0.1217 |
| CA 19-9 | −0.2955 | 0.1296 | −0.1574 | 0.0921 | 0.4246 | 1.0000 | −0.0457 | −0.1256 | −0.0552 | −0.0850 | −0.0705 | 0.0032 | 0.0792 |
| Tumor size | −0.0900 | 0.1533 | 0.0110 | −0.0990 | −0.0804 | −0.0457 | 1.0000 | −0.0994 | −0.2606 | −0.0711 | −0.1549 | −0.1808 | −0.1740 |
| T-Bili | −0.0445 | 0.0332 | −0.0817 | 0.1523 | 0.0123 | −0.1256 | −0.0994 | 1.0000 | 0.2332 | 0.7911 | 0.3134 | −0.2855 | 0.0459 |
| ALB | 0.3572 | −0.4599 | −0.3592 | −0.1782 | −0.3247 | −0.0552 | −0.2606 | 0.2332 | 1.0000 | 0.1202 | 0.5898 | −0.0332 | −0.1107 |
| γ-GTP | −0.0872 | 0.1729 | −0.1277 | −0.0594 | −0.0249 | −0.0850 | −0.0711 | 0.7911 | 0.1202 | 1.0000 | 0.1842 | −0.0936 | 0.2061 |
| Sodium | 0.2733 | −0.3679 | −0.2184 | −0.1096 | −0.1701 | −0.0705 | −0.1549 | 0.3134 | 0.5898 | 0.1842 | 1.0000 | 0.1092 | 0.0401 |
| BUN | 0.1841 | 0.0802 | 0.2264 | −0.1443 | −0.0431 | 0.0032 | −0.1808 | −0.2855 | −0.0332 | −0.0936 | 0.1092 | 1.0000 | 0.0853 |
| Creatinine | −0.1699 | −0.0499 | −0.0644 | −0.0026 | 0.1217 | 0.0792 | −0.1740 | 0.0459 | −0.1107 | 0.2061 | 0.0401 | 0.0853 | 1.0000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shirono, T.; Niizeki, T.; Iwamoto, H.; Shimose, S.; Suzuki, H.; Kawaguchi, T.; Kamachi, N.; Noda, Y.; Okamura, S.; Nakano, M.; et al. Therapeutic Outcomes and Prognostic Factors of Unresectable Intrahepatic Cholangiocarcinoma: A Data Mining Analysis. J. Clin. Med. 2021, 10, 987. https://doi.org/10.3390/jcm10050987
Shirono T, Niizeki T, Iwamoto H, Shimose S, Suzuki H, Kawaguchi T, Kamachi N, Noda Y, Okamura S, Nakano M, et al. Therapeutic Outcomes and Prognostic Factors of Unresectable Intrahepatic Cholangiocarcinoma: A Data Mining Analysis. Journal of Clinical Medicine. 2021; 10(5):987. https://doi.org/10.3390/jcm10050987
Chicago/Turabian StyleShirono, Tomotake, Takashi Niizeki, Hideki Iwamoto, Shigeo Shimose, Hiroyuki Suzuki, Takumi Kawaguchi, Naoki Kamachi, Yu Noda, Shusuke Okamura, Masahito Nakano, and et al. 2021. "Therapeutic Outcomes and Prognostic Factors of Unresectable Intrahepatic Cholangiocarcinoma: A Data Mining Analysis" Journal of Clinical Medicine 10, no. 5: 987. https://doi.org/10.3390/jcm10050987