1. Introduction
Key factors for long-term clinical success in fixed prosthodontics are respect of function, biocompatibility, marginal and internal fit, fracture resistance, and appealing esthetics. In particular, a marginal gap, at the level of the restorative finish line, has a highly detrimental effect on the quality of the restoration, inducing micro-leakage, cement dissolution by oral fluids, and biofilm accumulation, with consequences such as caries or endodontic and periodontal problems [
1,
2,
3,
4]. Up to now, the precision of marginal fit has been reported up to 200 microns and beyond [
5,
6,
7,
8], although a precise, scientifically validated evaluation of the maximum acceptable marginal gap has never been provided; the threshold of 120 microns, defined by McLean, has been considered as a reference in dental literature since 1971 [
9]. It is generally accepted that all subsequent clinical and laboratory work steps influence the overall success of a fixed restoration, from tooth preparation to cementation [
10]. Here, the final impression is one of the most important steps to achieving the final marginal adaptation of the restoration, independent on the material and technique selected. In conventional impression procedures, the final result is strongly affected by dimensional distortions of impression materials and gypsum [
11,
12], to the extent that half of misfits have been considered to be ascribed to the impression procedure and to the production of the gypsum cast, the other half being mainly related to the production techniques of the prosthesis [
13,
14]. The introduction of the digital impression by using intraoral scanning (IOS) has changed the restorative scenario in prosthodontics by the acquisition of anatomic information without the use of physical impression materials, transforming shapes into digital files [
15,
16,
17,
18].
One of the most critical steps during impression taking, both conventional and digital, is detecting the finish line, in particular for subgingival tooth preparation. In this context, adequate soft tissue management without inflammation is mandatory for a successful impression, supported by gingival displacement to expose the finish. In the conventional impression procedure, this is usually obtained using gingival retraction cords or materials which temporarily modify the marginal soft tissue, with the purpose of detecting the necessary sub-gingival anatomic information and of widening the gingival sulcus without tearing the subtle light material margin, due to its low consistency [
19]. Following the digital impression technique, it is not different to the conventional approach. In both cases, the detection of the finish line relies on a clean, healthy gingival sulcus, proper soft tissue displacement, and clear visibility of the prepared tooth anatomy.
The aim of this randomized controlled clinical trial was to test the capability of an IOS device (Aadva IOS 100, GC, Japan) used in standardized conditions, to detect margins of abutments prepared with knife-edge finishing line located at three different levels in relation to the gingival sulcus.
The null hypothesis was that there was no difference in the capability of the IOS based on the vertical position of the prepared finish line.
2. Experimental Section
In this study, 60 patients (28 female and 32 male) with a mean age of 45 (±20.5) years (range 18–69) in need of a tooth-borne single crown in posterior sites were recruited. The present prospective clinical trial was approved by the Ethical Committee of the University of Siena (n.18895). For each included individual, a signed written consent was obtained after clear information about the study. Guidelines of the CONSORT statement were followed.
Inclusion Criteria: age ≥ 18 years; single full crown in posterior sites (maxilla or mandible); periodontally healthy or successfully treated; general good health.
Exclusion criteria: presence of any active infection; severe periodontal inflammation; presence of chronic systemic disease; smoking more than 15 cigarettes per day; bruxism habits.
2.1. Randomization/Allocation Concealment/Masking of Examiners
Included patients were recruited between May and November of 2018 in the Department of Fixed Prosthodontics at the University of Siena and randomly divided into three groups of twenty each (3 × n = 20) according to the location depth of the finishing line made on the prepared abutments in relation to the sulcus:
Group A: supragingival margin.
Group B: margin 0.5–1.0 mm into the sulcus.
Group C: margin 1.5–2.00 mm into the sulcus.
Treatment assignment was noted in a detailed registration and treatment assignment form. Allocation concealment was performed by opaque, sealed, and sequentially numbered envelopes. The statistician generated the allocation sequence by means of a computer-generated random list and instructed a different subject to assign a sealed envelope containing the type of IOS. The opaque envelope was opened before IOS selection and communicated to the operator (EFC—Edoardo Ferrari Cagidiaco). Blinding of the examiner was maintained throughout all experimental procedures (
Figure 1).
2.2. Clinical Setting
Abutment tooth preparations of Group A were performed following the generally accepted recommendations for CAD/CAM (Computer-Aided Design/Computer-Aided Manufacturing)-restorations with supragingivally located margins in order to remain visible [
20]. In Group B, the margins were placed 0.5–1.0 mm into the sulcus and in Group C, the margins were placed around 1.5–2.0 mm in depth. Clinical pictures were taken of each quadrant and the corresponding preparations (
Figure 2).
All abutments received a temporary crown for 2 weeks [
21,
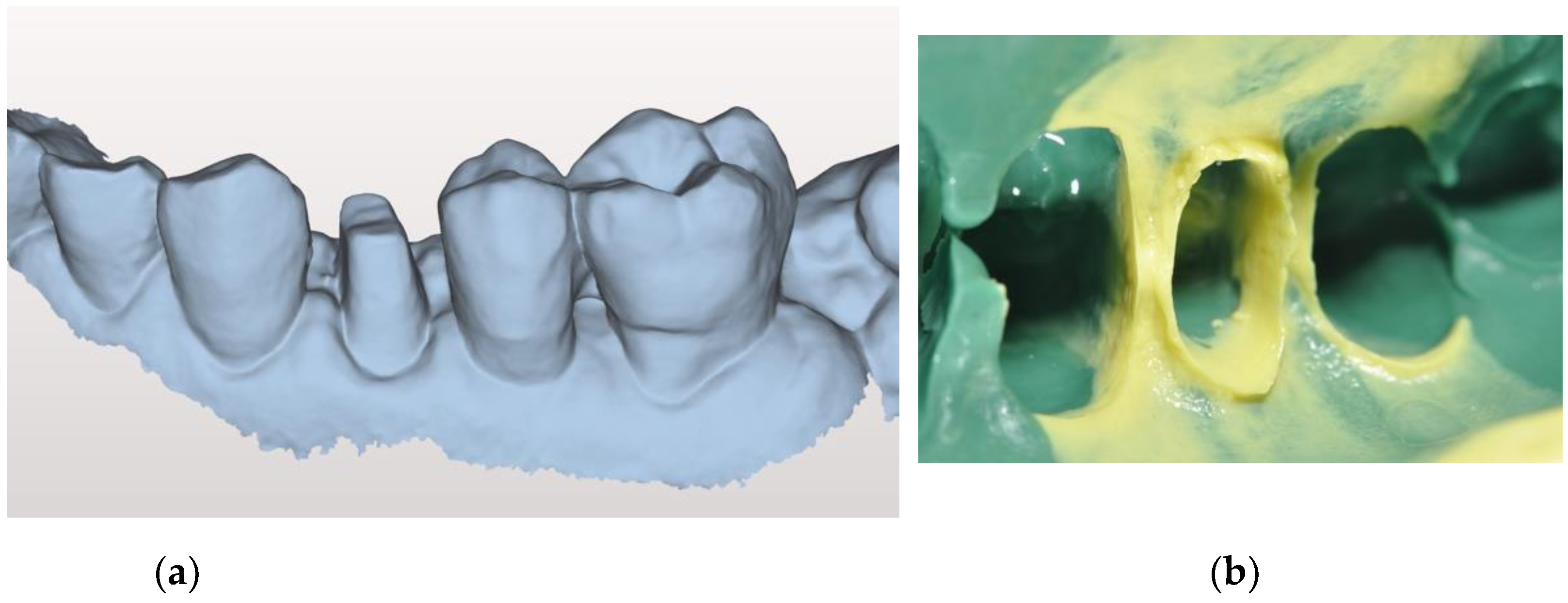
22] and then the final IOS impressions were made. The impression site was prepared according to the double retraction cord technique: the first, thinner cord (Ultrapack #00; Ultradent, South Jordan, UT, USA) was gently placed into the gingival sulcus, followed by the insertion of a second, wider-diameter cord (Ultrapack #1; Ultradent, South Jordan, UT, USA) at a more coronal level, visible around the preparation margins. IOS was initially performed according to the manufacturer’s guidelines (Aadva IOS 100, GC Co., Tokyo, Japan): firstly, the upper arch was scanned, followed by the lower arch, and then the bite registration was performed. A total of twenty scans of each group (A, B, and C) were collected and saved in the standard tessellation language (STL) format (
Figure 3a).
Any scanning shot considered incorrect or showing evident defects was discarded.
As the control, a conventional impression was made using polyvinyl siloxane (Ex’lance, GC) (
Figure 3b).
The viscoelastic properties of the material facilitate the detection of the area below the gingival margins. Impressions were cleansed, disinfected, poured in Type IV Dental Die Stone (FujiRock, GC, Tokyo, Japan), and finally scanned by a laboratory scanner (Aadva lab scanner, GC, Tokyo, Japan), generating STL files of the control protocol.
2.3. Software Measurements
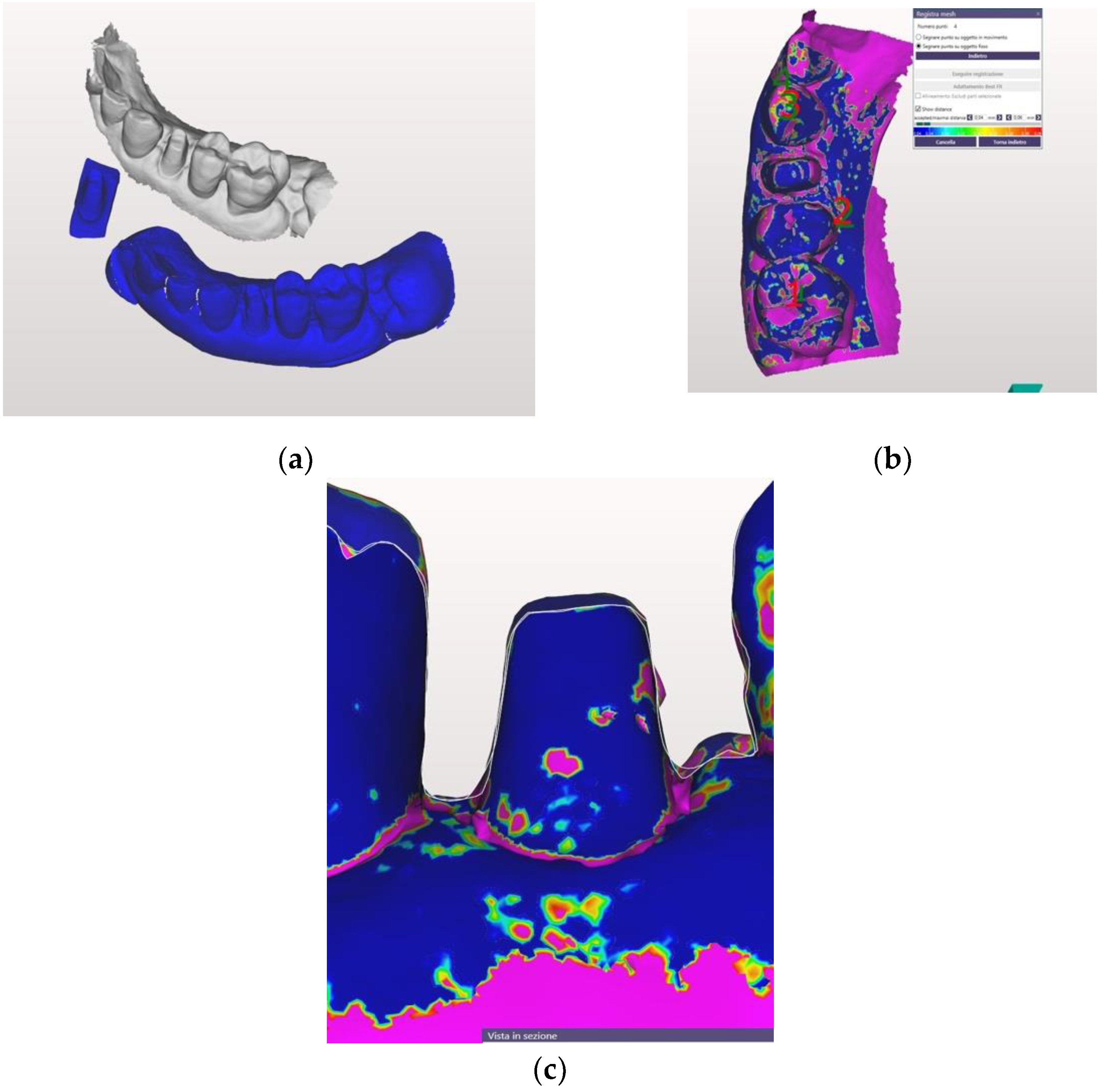
Each STL file generated by both the IOS and the lab scanner was processed by the same dental master technician, using the Exocad software (Exocad GmbH, Darmstadt, Germany), applying the “best-fit“ algorithm in order to align the scan of the conventional with the digital impression (
Figure 4a).
The superimposition of the STL files allowed measurement of the distance between each preparation margin and the adjacent gingival tissue, after making a section of each abutment in either the mesial-distal or buccal-lingual direction (
Figure 4b,c).
The straight distance between the most coronal part of the gingival margin and the apical finish line of the preparation were used as distances to be recorded, and both vertical distances (made by conventional and digital impressions) were measured and recorded. The most coronal part of the gingival tissue was always the same, and the most apical part into the sulcus varied accordingly for each impression. Four measures were taken, two interproximally (mesial and distal) and buccally (buccal), for a total of six measures of each abutment considering three modes of impressions.
2.4. Statistical Analysis
All the data were collected and processed statistically. Descriptive statistics (means, standard deviations, 95% confidence intervals) were performed on the studied parameters using Stata 15-IC (IBM, NY, USA). The Wilcoxon rank sum test was used to analyze the media each measure.
Two-way analysis of variance (ANOVA) for each site and the Bonferroni test were conducted to assess the overall statistical significance of the differences among the groups (p > 0.05).
3. Results
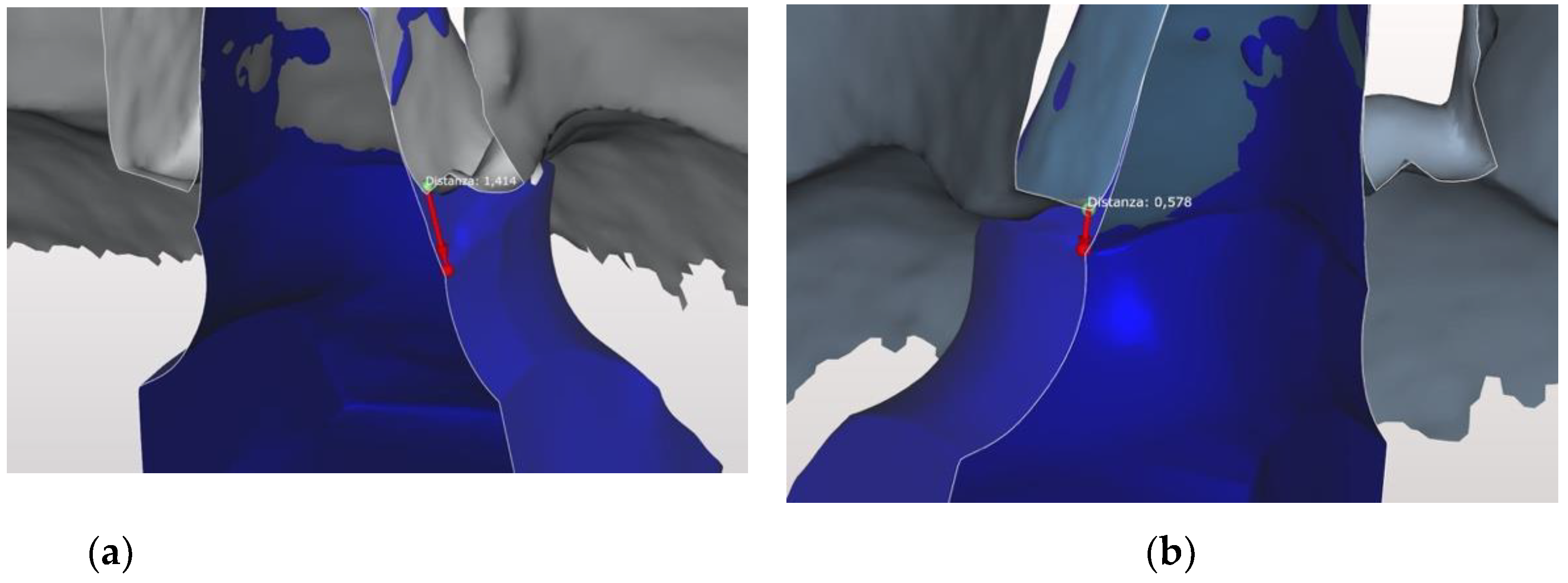
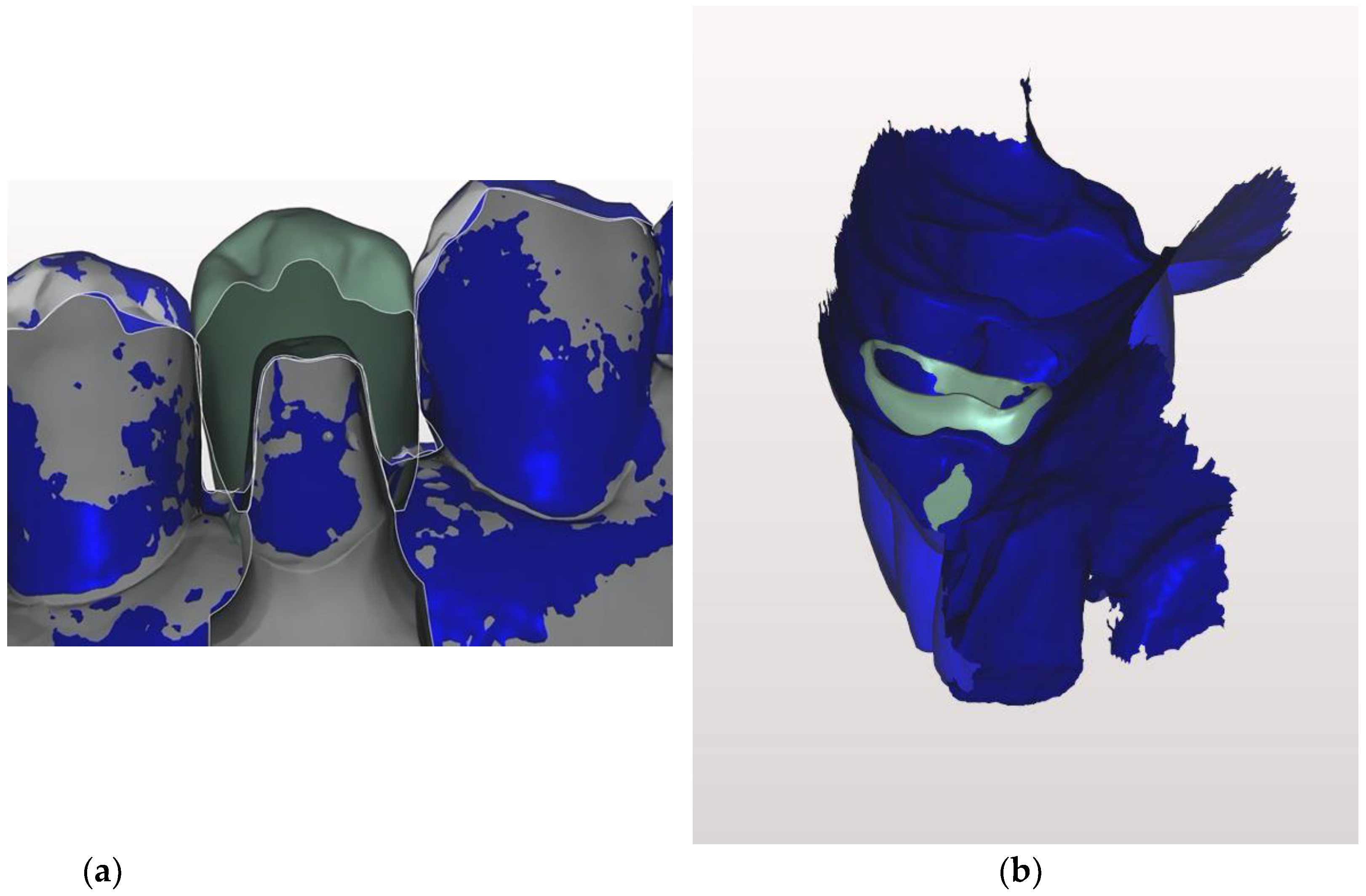
Table 1 shows the results for the mean distance of the prepared root that cannot be detected with the digital impression compared to the conventional one.
There was no difference between the two kinds of impression in Group A in both sites, in Group B a difference of 0.483 mm and 0.682 mm at the interproximal and buccal site respectively, and in Group C 0.750 mm and 0.964 mm at the interproximal and buccal site respectively (
Figure 5a,b and
Figure 6a,b).
The difference between the depth of the sulci, analyzed according to the two vertical preparations (Group B /<1 mm vs. Group C /1.5–2.0 mm), was statistically significant, with a difference of 0.28 mm (SE—Standard Error: 0.5; IC—Interval of Confidence: 95% −0.4–0.2) (p < 0.00).
The analysis performed on a site level (mesial/distal/vestibular) on the depth of both vertical preparations revealed significant differences (F = 12.15;
p < 0.0001) (
Table 2 and
Table 3). After a post hoc analysis (Bonferroni) the vestibular site of the Group B vertical preparation was always statistically inferior to the other sites prepared deeply (Group C) (
Table 4 and
Table 5).
The number of intraoral scans rejected from the study due to evident errors was 2 for Group A, 3 for Group B and 4 for Group C, respectively; and, essentially, were the first scanning shots made by the operator. However, 20 scanning shots for each group were finally performed and evaluated.
4. Discussion
The restorative finishing line of full crowns can be designed according to various geometries, mainly horizontally or vertically oriented, and as shoulder, chamfer, and knife edge preparations, with mixed typologies based on the angulation of the marginal zone. When a partial crown is prepared for an esthetic restoration a horizontal margin is usually prepared, such as a shoulder design, with a sharp external angle. The presence of this sharp angle facilitates the check of the distance between the finish line and adjacent tooth, as well as the distance between the finish line and the soft tissues. However, the preparation of an abutment for a digital impression must consider limitations due to the digital impression device [
23].
Based on the results of this clinical trial, the null hypothesis, that there was no difference in the capability of the IOS independent of the vertical position of the prepared finish line, was rejected (p < 0.005). It was pointed out that the deeper into the sulcus the position of the margin is, more of the part of the prepared root will be lost during the digital impression.
Several clinical parameters were kept under control to ensure uniformity in order to reduce the risk of bias in this RCT. All the soft tissues around preparation margins were in similarly healthy condition; the operator was a long-time experienced user of IOS and each patient received detailed instructions before performing the digital impression.
The accuracy of digital impression systems has been extensively studied in recent years [
20,
23]. However, the wide majority of studies were performed in vitro and designed to detect differences among different scanners [
23].
The problem is that the in vitro laboratory conditions often differ from real, daily clinical situations [
24]. The clinical use of IOS can be heavily complicated by factors such as: humidity of the oral environment, saliva flow, soft tissue presence and health condition, possible movements of the patient, scanning procedure and technique, limited access of the scanning probe to posterior teeth (for instance, hampered by lips and cheeks), and the varying translucency of enamel and dentine [
25]. However, the results of this study showed that when all the aforementioned factors were controlled as fully as possible during impression taking, the depth of the finishing line inside the sulcus can negatively influence the final quality and accuracy of the digital impression.
A possible explanation for this finding is related to the discrete nature of intraoral scans. Unlike conventional impressions, which record a continuous surface, digital scans sample the surface at discrete intervals. A continuous surface is then generated in the software by ‘joining the dots’ according to the “stitching” algorithm. If the sample density of information is too low relative to the topology of the region (e.g., in a small patch of the impression near the gingival crevice and containing an angular crown margin too), the generated 3D surface will not replicate the true anatomy.
The results of this study clearly pointed out limitations in taking a predictable digital impression when a margin placed 1.5–2 mm into the sulcus was used and showed the need for a coronally positioned finishing line in order to catch the margins.
It was stated that low quality of impressions and insufficient preparations were the greatest obstacles for the production of high-end dental restorations [
26]. In this context, IOS seems to be a logical step to prevent many possible errors.
However, it must be considered that performing a preparation is a common procedure in general dental practice, as a necessary prerequisite for the fabrication of fixed prosthetic restoration, and influences overall success substantially. During preparation, biological and technical necessities often oppose each other and therefore sometimes make it a difficult procedure for the dentist. Additionally, in daily practice the cervical margin is often located equigingivally and/or subgingivally and the positioning of the margin can be a serious obstacle to taking a perfect digital impression [
27].
When the finishing line is located in the sulcus and the IOS is used, a certain amount of prepared root can’t be captured [
28]. The prepared root which is not captured in the digital impression and that remains uncovered by the margin of the crown will be covered by a long epithelium attachment the same type of periodontal attachment formed after scaling and root planning [
29].
The skill of the operator and the role of temporary crowns may help to address margins positioned more in depth into the sulcus.
However, few scientific data are available regarding the capability of IOS to catch margins located deeply into the sulcus. Consequently, the results of this randomized clinical trial strongly suggest the use of IOS in combination with supragingival preparations only.
It has to be emphasized that only one IOS device has been evaluated in this study; therefore, these results cannot be directly translated to other trials using different IOS devices. Similar clinical studies with a wider number of IOS are desirable.
5. Conclusions
Based on the results of this clinical study, the following conclusions can be drawn:
1. The deeper the position of the finishing line into the sulcus, it is more difficult to capture the margin using IOS.
2. Digital impression is not recommended when crowns’ margins are positioned deep (1.5–2 mm) into the sulcus.
Author Contributions
Conceptualization, E.F.C. and M.F.; methodology, E.F.C., M.F., and F.Z.; software, N.D.; validation, N.D. and T.J.; formal analysis, N.D.; investigation, E.F.C. and M.F.; resources, E.F.C.; writing—original draft preparation, E.F.C. and F.Z.; writing—review and editing, M.F. and T.J.; supervision, M.F.; funding acquisition, M.F. All authors have read and agreed to the published version of the manuscript. Authorship was limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol n.18895, code PSO001, Siena 16.01.2020).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy of patients.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gardner, F.M. Margins of complete crowns—Literature review. J. Prosthet. Dent. 1982, 48, 396–400. [Google Scholar] [CrossRef]
- Anusavice, K.J.; Carroll, J.E. Effect of incompatibility stress on the fit of metal-ceramic crowns. J. Dent. Res. 1987, 66, 1341–1345. [Google Scholar] [CrossRef] [PubMed]
- Yeo, I.S.; Yang, J.H.; Lee, J.B. In vitro marginal fit of three all-ceramic crown systems. J. Prosthet. Dent. 2003, 90, 459–464. [Google Scholar] [CrossRef]
- Larson, T.D. The clinical significance of marginal fit. Northwest Dent. 2012, 91, 22–29. [Google Scholar]
- Contrepois, M.; Soenen, A.; Bartala, M.; Laviole, O. Marginal adaptation of ceramic crowns: A systematic review. J. Prosthet. Dent. 2013, 110, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Boitelle, P.; Mawussi, B.; Tapie, L.; Fromentin, O. A systematic review of CAD/CAM fit restoration evaluations. J. Oral. Rehabil. 2014, 41, 853–874. [Google Scholar] [CrossRef]
- Yildirim, G.; Uzun, I.H.; Keles, A. Evaluation of marginal and internal adaptation of hybrid and nanoceramic systems with microcomputed tomography: An in vitro study. J. Prosthet. Dent. 2017, 118, 200–207. [Google Scholar] [CrossRef]
- Papadiochou, S.; Pissiotis, A.L. Marginal adaptation and CAD-CAM technology: A systematic review of restorative material and fabrication techniques. J. Prosthet. Dent. 2018, 119, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Mclean, J.W. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef]
- Martignoni, M.; Schonenberger, A. Precision Fixed Prosthodontics: Clinical and Laboratory Aspects; Quintessence Publishing: Berlin, Germany, 1990. [Google Scholar]
- Johnson, G.H.; Craig, R.G. Accuracy of four types of rubber impression materials compared with time of pour and a repeat pour of models. J. Prosthet. Dent. 1985, 53, 484–490. [Google Scholar] [CrossRef]
- Millstein, P.L. Determining the accuracy of gypsum casts made from type IV dental stone. J. Oral Rehab. 1992, 19, 239–243. [Google Scholar] [CrossRef]
- Schneider, A.; Kurtzman, G.M.; Silverstein, L.H. Improving implant framework passive fit and accuracy through the use of verification stents and casts. J. Dent. Technol. 2001, 18, 23–25. [Google Scholar]
- Heckmann, S.M.; Karl, M.; Wichmann, M.G.; Winter, W.; Graef, F.; Taylor, T.D. Cement fixation and screw retention: Parameters of passive fit: An in vitro study of three-unit implant-supported fixed partial dentures. Clin. Oral Impl. Res. 2004, 15, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Kihara, H.; Hatakeyama, W.; Komine, F.; Takafuji, K.; Takahashi, T.; Yokota, J.; Oriso, K.; Kondo, H. Accuracy and practicality of intraoral scanner in dentistry: A literature review. J. Prosthodont. Res. 2020, 64, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Aswani, K.; Wankhade, S.; Khalikar, A.; Deogade, S. Accuracy of an intraoral digital impression: A review. J. Indian Prosthodont. Soc. 2020, 20, 27–37. [Google Scholar] [CrossRef]
- Zarone, F.; Ruggiero, G.; Ferrari, M.; Mangano, F.; Joda, T.; Sorrentino, R. Accuracy of a chairside intraoral scanner compared with a laboratory scanner for the completely edentulous maxilla: An in vitro 3-dimensional comparative analysis. J. Prosthet. Dent. 2020, 124, 767. [Google Scholar] [CrossRef]
- Mangano, F.; Lerner, H.; Margiani, B.; Solop, P.; Latuta, N.; Admakin, O. Congruence between Meshes and Library Files of Implant Scanbodies: An In Vitro Study Comparing Five Intraoral Scanners. J. Clin. Med. 2020, 9, 2174. [Google Scholar] [CrossRef] [PubMed]
- Safari, S.; Vossoghi Sheshkalani, M.; Hoseini Ghavam, F.; Hamedi, M. Gingival Retraction Methods for Fabrication of Fixed Partial Denture: Literature Review. J. Dent. Biomater. 2016, 3, 205–213. [Google Scholar]
- Goodacre, C.J.; Campagni, W.V.; Aquilino, S.A. Tooth preparations for complete crowns: An art form based on scientific principles. J. Prosthet. Dent. 2001, 85, 363–376. [Google Scholar] [CrossRef] [Green Version]
- Di Fiore, A.; Vigolo, P.; Monaco, C.; Graiff, L.; Ferrari, M.; Stellini, E. Digital impression of teeth prepared with a subgingival vertical finish line: A new clinical approach to manage the interim crown. J. Osseointegr. 2019, 11, 544–547. [Google Scholar]
- Schmitz, J.; Valenti, M. Interim restoration technique for gingival displacement with a feather edge preparation design and digital scan. J. Prosthet. Dent. 2019, 123. [Google Scholar] [CrossRef] [PubMed]
- Guth, J.F.; Keul, C.; Stimmelmayr, M.; Beuer, F.; Edelhoff, D. Accuracy of digital models obtained by direct and indirect data capturing. Clin. Oral Invest. 2013, 17, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Keeling, A.; Mandelli, F.; Lo Giudice, G.; Garcia-Godoy, F.; Joda, T. The ability of marginal detection using different intraoral scanning systems: A pilot randomized controlled trial. Am. J. Dent. 2018, 31, 272–276. [Google Scholar] [PubMed]
- Abduo, J. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur. J. Prosth. Rest. Dent. 2018, 26, 101–121. [Google Scholar]
- Cho, S.H.; Schaefer, O.; Thompson, G.A.; Guentsch, A. Comparison of accuracy and reproducibility of casts made by digital and conventional methods. J. Prosthet. Dent. 2015, 113, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Bader, J.D.; Rozier, R.G.; McFall, W.T., Jr.; Ramsey, D.L. Effect of crown margins on periodontal conditions in regularly attending patients. J. Prosthet. Dent. 1991, 65, 75–79. [Google Scholar] [CrossRef]
- Mandelli, F.; Ferrini, F.; Gastaldi, G.; Gherlone, E.; Ferrari, M. Improvement of a Digital Impression with Conventional Materials: Overcoming Intraoral Scanner Limitations. Int. J. Prosthodont. 2017, 30, 373–376. [Google Scholar] [CrossRef] [Green Version]
- Caton, J.G.; Zander, H.A. The attachment between tooth and gingival tissues after periodic root planning and soft tissue curettage. J. Periodontology 1979, 9, 462–466. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}