
Calprotectin, an Emerging Biomarker of Interest in COVID-19: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Search Strategy
2.2. Eligibility Criteria and Data Extraction
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
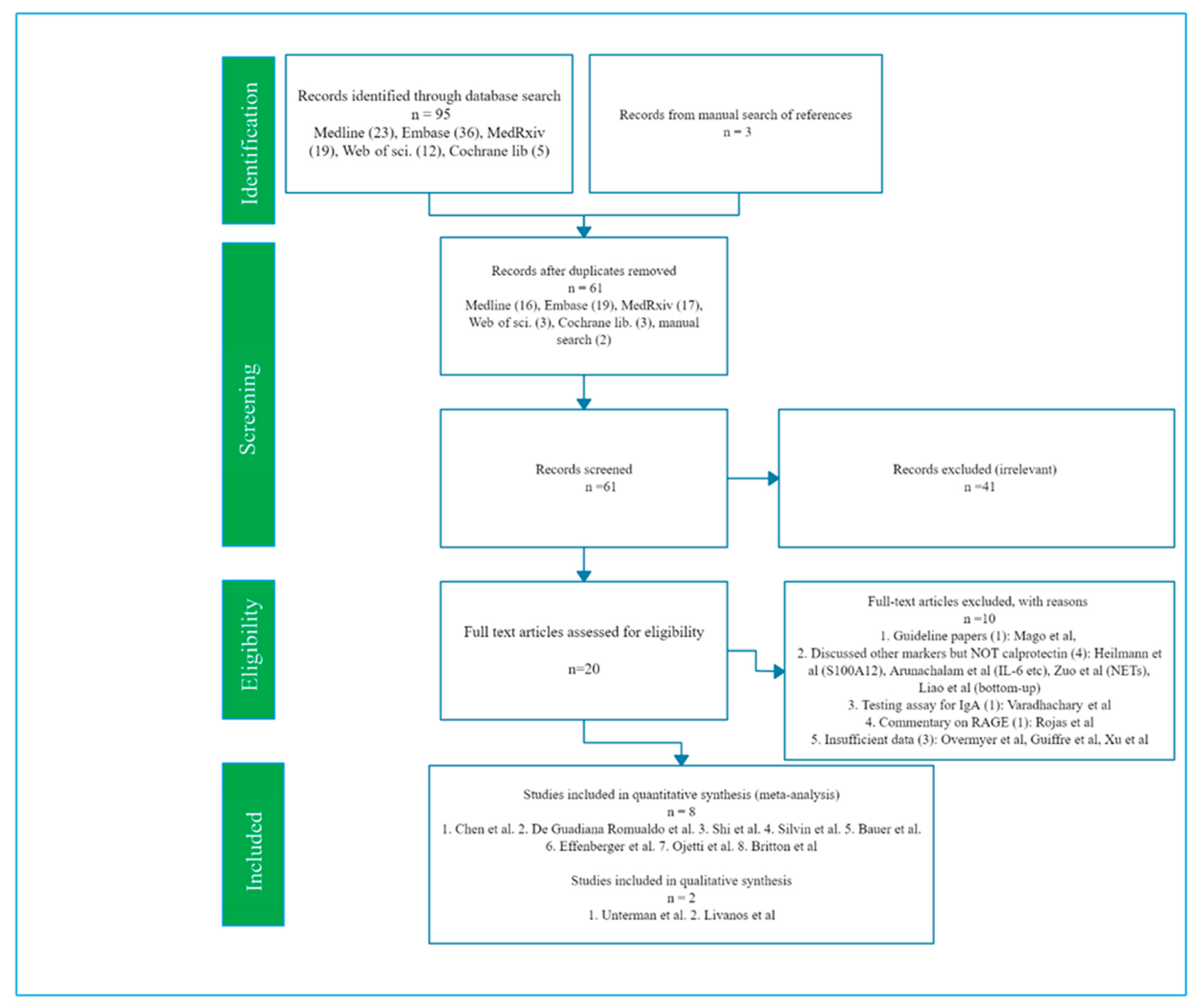
3.1. Literature Search
3.2. Study Characteristics
3.3. Meta-Analysis, Forest Plot and Sensitivity Analysis
3.4. Subgroup Analysis and Meta-Regression
3.5. Publication Bias
4. Discussion
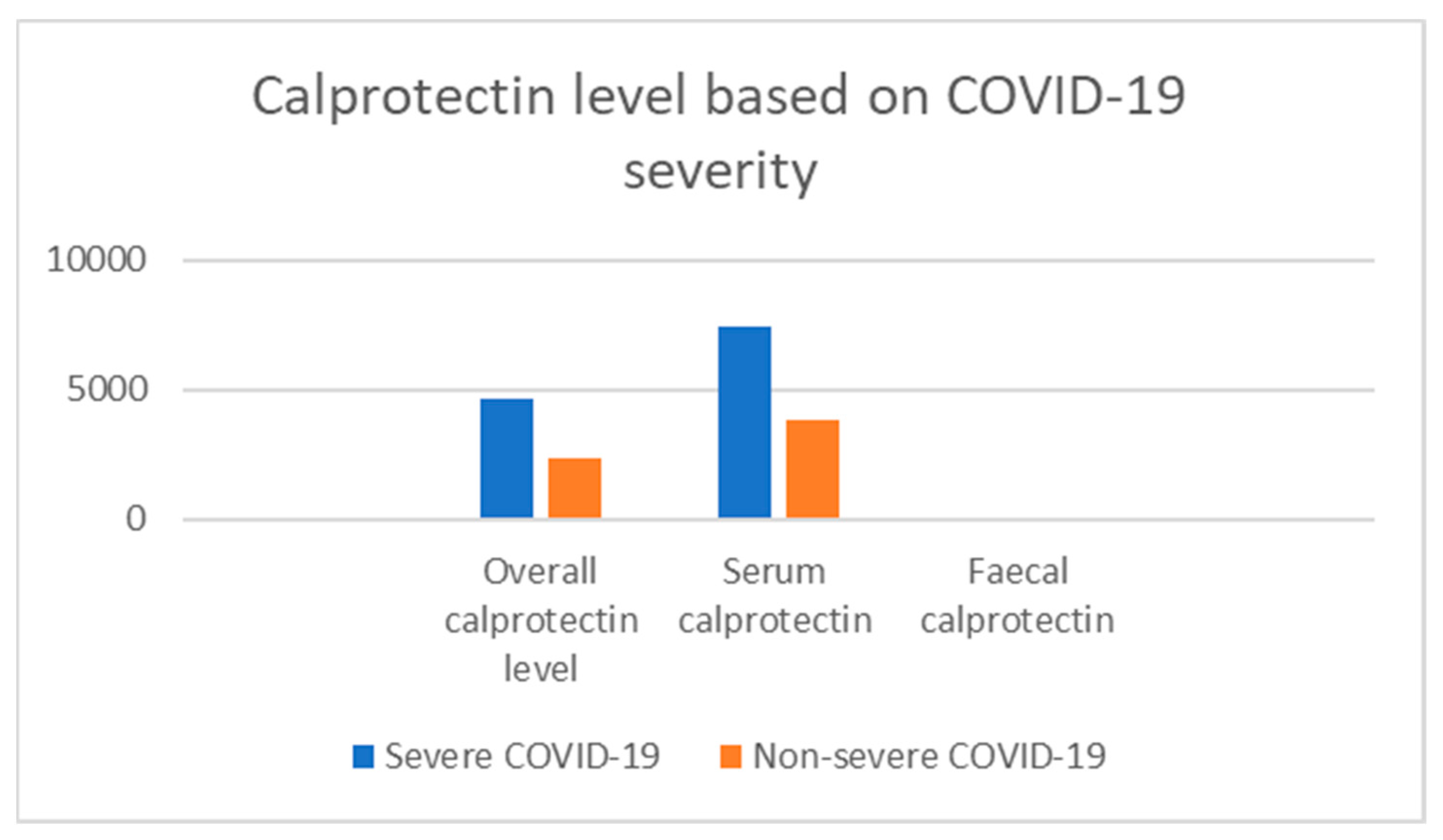
4.1. Diagnostic Performance of Serum Calprotectin in Selecting Severe COVID-19
4.2. Prognostic Value of Serum/Fecal Calprotectin
4.3. Diagnostic Superiority of Calprotectin over Other Acute Phase Reactants
4.4. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/?gclid=EAIaIQobChMItaXYjqSv6wIVA7eWCh0UEQlaEAMYASAAEgIOiPD_BwE/ (accessed on 6 February 2020).
- Guan, W.J.; Zhong, N.S. Clinical Characteristics of Covid-19 in China. Reply. N. Engl. J. Med. 2020, 27, 382. [Google Scholar]
- Wang, T.; Du, Z.; Zhu, F.; Cao, Z.; An, Y.; Gao, Y.; Jiang, B. Comorbidities and multi-organ injuries in the treatment of COVID-19. Lancet 2020, 395, e52. [Google Scholar] [CrossRef]
- Zheng, M.; Gao, Y.; Wang, G.; Song, G.; Liu, S.; Sun, D.; Xu, Y.; Tian, Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 533–535. [Google Scholar] [CrossRef] [Green Version]
- Sreejit, G.; Flynn, M.C.; Patil, M.; Krishnamurthy, P.; Murphy, A.J.; Nagareddy, P.R. S100 family proteins in inflammation and beyond. Adv. Clin. Chem. 2020, 98, 173–231. [Google Scholar] [PubMed]
- Overmyer, K.A.; Shishkova, E.; Miller, I.J.; Balnis, J.; Bernstein, M.N.; Peters-Clarke, T.M.; Meyer, J.G.; Quan, Q.; Muehlbauer, L.K.; Trujillo, E.A.; et al. Large-scale Multi-omic Analysis of COVID-19 Severity. medRxiv 2020. [Google Scholar] [CrossRef]
- Wang, S.; Song, R.; Wang, Z.; Jing, Z.; Wang, S.; Ma, J. S100A8/A9 in Inflammation. Front. Immunol. 2018, 9, 1298. [Google Scholar] [CrossRef]
- Bresnick, A.R. S100 proteins as therapeutic targets. Biophys. Rev. 2018, 10, 1617–1629. [Google Scholar] [CrossRef]
- Ometto, F.; Friso, L.; Astorri, D.; Botsios, C.; Raffeiner, B.; Punzi, L.; Doria, A. Calprotectin in rheumatic diseases. Exp. Biol. Med. 2017, 242, 859–873. [Google Scholar] [CrossRef]
- Vogl, T.; Tenbrock, K.; Ludwig, S.; Leukert, N.; Ehrhardt, C.; Van Zoelen, M.A.; Nacken, W.; Foell, D.; Van der Poll, T.; Sorg, C.; et al. Mrp8 and Mrp14 are endogenous activators of Toll-like receptor 4, promoting lethal, endotoxin-induced shock. Nat. Med. 2007, 13, 1042–1049. [Google Scholar] [CrossRef]
- Silvin, A.; Chapuis, N.; Dunsmore, G.; Goubet, A.G.; Dubuisson, A.; Derosa, L.; Almire, C.; Hénon, C.; Kosmider, O.; Droin, N.; et al. Elevated calprotectin and abnormal myeloid cell subsets discriminate severe from mild COVID-19. Cell 2020, 182, 1401–1418.e18. [Google Scholar] [CrossRef] [PubMed]
- Haga, H.J.; Brun, J.G.; Berner Berntzen, H.; Cervera, R.; Khamashta, M.; Hughes, G.R. Calprotectin in patients with systemic lupus erythematosus: Relation to clinical and laboratory parameters of disease activity. Lupus 1993, 2, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Long, X.; Xu, Q.; Tan, J.; Wang, G.; Cao, Y.; Wei, J.; Luo, H.; Zhu, H.; Huang, L.; et al. Elevated serum levels of S100A8/A9 and HMGB1 at hospital admission are correlated with inferior clinical outcomes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 992–994. [Google Scholar] [CrossRef]
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and outcomes of COVID-19 hospitalisations: Systematic review and meta-analysis. BMJ Evid. Based Med. 2020. [Google Scholar] [CrossRef]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef]
- Henry, B.M.; De Oliveira, M.H.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Effenberger, M.; Grabherr, F.; Mayr, L.; Schwaerzler, J.; Nairz, M.; Seifert, M.; Hilbe, R.; Seiwald, S.; Scholl-Buergi, S.; Fritsche, G.; et al. Faecal calprotectin indicates intestinal inflammation in COVID-19. Gut 2020, 69, 1543–1544. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf/ (accessed on 10 September 2020).
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Song, F.; Gilbody, S. Bias in meta-analysis detected by a simple, graphical test. Increase in studies of publication bias coincided with increasing use of meta-analysis. BMJ 1998, 316, 471. [Google Scholar] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guadiana Romualdo, L.G.; Mulero, M.D.; Olivo, M.H.; Rojas, C.R.; Arenas, V.R.; Morales, M.G.; Abellán, A.B.; Conesa-Zamora, P.; García-García, J.; Hernández, A.C.; et al. Circulating levels of GDF-15 and calprotectin for prediction of in-hospital mortality in COVID-19 patients: A case series. J. Infect. 2020. [Google Scholar] [CrossRef]
- Shi, H.; Zuo, Y.; Yalavarthi, S.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.N.; Woods, R.J.; Lood, C.; Knight, J.S.; et al. Neutrophil calprotectin identifies severe pulmonary disease in COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Bauer, W.; Diehl-Wiesenecker, E.; Ulke, J.; Galtung, N.; Havelka, A.; Hegel, J.K.; Tauber, R.; Somasundaram, R.; Kappert, K. Outcome prediction by serum calprotectin in patients with COVID-19 in the emergency department. J. Infect. 2020. [Google Scholar] [CrossRef]
- Ojetti, V.; Saviano, A.; Covino, M.; Acampora, N.; Troiani, E.; Franceschi, F.; Abbate, V.; Addolorato, G.; Agostini, F.; Ainora, M.E.; et al. COVID-19 and intestinal inflammation: Role of fecal calprotectin. Dig. Liver Dis. 2020, 52, 1231–1233. [Google Scholar] [CrossRef]
- Britton, G.J.; Chen-Liaw, A.; Cossarini, F.; Livanos, A.E.; Spindler, M.P.; Plitt, T.; Eggers, J.; Mogno, I.; Gonzalez-Reiche, A.S.; Siu, S.; et al. SARS-CoV-2-specific IgA and limited inflammatory cytokines are present in the stool of select patients with acute COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- National Institute of Health. Quality Assessment Tool for Case Series Studies for Meta-Analysis. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools/ (accessed on 12 September 2020).
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford (accessed on 15 September 2020).
- Unterman, A.; Sumida, T.S.; Nouri, N.; Yan, X.; Zhao, A.Y.; Gasque, V.; Schupp, J.C.; Asashima, H.; Liu, Y.; Cosme, C.; et al. Single-Cell Omics Reveals Dyssynchrony of the Innate and Adaptive Immune System in Progressive COVID-19. medRxiv. 2020. [Google Scholar] [CrossRef]
- Livanos, A.E.; Jha, D.; Cossarini, F.; Gonzalez-Reiche, A.S.; Tokuyama, M.; Aydillo, T.; Parigi, T.L.; Ramos, I.; Dunleavy, K.; Lee, B.; et al. Gastrointestinal involvement attenuates COVID-19 severity and mortality. medRxiv. 2020. [Google Scholar] [CrossRef]
- Wan, Y.; Li, J.; Shen, L.; Zou, Y.; Hou, L.; Zhu, L.; Faden, H.S.; Tang, Z.; Shi, M.; Jiao, N.; et al. Enteric involvement in hospitalised patients with COVID-19 outside Wuhan. Lancet Gastroenterol. Hepatol. 2020, 5, 534–535. [Google Scholar] [CrossRef]
- D’Amico, F.; Baumgart, D.C.; Danese, S.; Peyrin-Biroulet, L. Diarrhea during COVID-19 infection: Pathogenesis, epidemiology, prevention and management. Clin. Gastroenterol. Hepatol. 2020, 18, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Yalavarthi, S.; Shi, H.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.; Weber, A.; Barnes, B.J.; Egeblad, M.; et al. Neutrophil extracellular traps (NETs) as markers of disease severity in COVID-19. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and validation of a clinical risk score to predict the occurrence of critical illness in hospitalized patients with COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Bohn, M.K.; Lippi, G.; Horvath, A.; Sethi, S.; Koch, D.; Ferrari, M.; Wang, C.B.; Mancini, N.; Steele, S.; Adeli, K. Molecular, serological, and biochemical diagnosis and monitoring of COVID-19: IFCC taskforce evaluation of the latest evidence. Clin. Chem. Lab. Med. 2020, 58, 1037–1052. [Google Scholar] [CrossRef] [PubMed]
- Mago, S.; Vaziri, H.; Tadros, M. The utility of fecal calprotectin in the era of COVID-19 pandemic. Gastroenterology 2020. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.; Kumar, M.P.; Singh, A.K.; Sharma, V. Fecal calprotectin levels in COVID-19: Lessons from a systematic review on its use in inflammatory bowel disease during the pandemic. Dig. Liver Dis. 2020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PICOS | Inclusion | Exclusion |
|---|---|---|
| Participants | Adults ≥ 18 years with confirmed COVID-19 infection | Adolescents < 18 years |
| Intervention | Calprotectin level measured | Other diagnostic parameters used |
| Comparison | Severe and non-severe COVID-19 infections | - |
| Outcome | -Difference in calprotectin levels between the groups -Association between calprotectin level and clinical/laboratory assessment of disease activity -Association with risk of disease progress/therapeutic response | - |
| Study design | -Observational clinical studies -Randomized controlled trial (RCTs) -Case reports-Editorials | -Opinion papers, correspondents, review papers, healthcare guidelines, protocol -Non-human studies -Animal model and in-vitro studies |
| Author | Design (Follow-Up) | Sample Size (N) * | Country | Gender, % M ** | Age, Mean Years (±SD) *** | % Deaths ** | Study Quality b | Peer-Review |
|---|---|---|---|---|---|---|---|---|
| Serum | ||||||||
| Chen et al. (July, 2020) [14] | Retrospective | 121 (ICU = 40, non-ICU = 81) | Wuhan (China) | 64% (70 vs. 61) | 63(ICU = 67, non-ICU = 62) | 30% died (82.5% vs. 3.7%) | Good | Yes |
| De Guadiana R. et al. (August, 2020) [25] | Case series | 66 (Non-survivors = 58, survivors = 8) | Cartagena (Spain) | 65% (68 vs. 58) | Total = 61 ± 16: non-survivors = 74 ± 9, survivors = 60 ± 16 | 12% (i.e., 8) died | Good | Yes |
| Silvin et al. (August, 2020) [12] | Cohort | 158 (severe = 50, non-severe = 39, healthy controls = 86) | France | 44% (67 vs. 30) | 53 (severe = 62, non-severe = 53, control = 50) | 24% vs. 4% | Good | Yes |
| Shi et al. (July 2020) [26] | Cohort | 172 (Room air group = 41; non-invasive oxygen = 71; invasive ventilation= 60) | Michigan (USA) | 56%M | 61.48 ± 17,7 | NR | Good | Yes |
| Bauer et al. (November 2020) [27] | Cohort | 19 (ICU = 8, non-ICU = 11) | Berlin (Germany) | 42%M | 67.6 | 10.5% | Good | Yes |
| Fecal | ||||||||
| Effenberger et al., August 2020 [18] | Cohort | 40 (COVID-19 with diarrhea = 22, without diarrhea = 18) | Innstruk Austria | Severe = 68%M, non-severe = 50%M | Severe = 72.3, non-severe = 58.4 | NR | Moderate | Yes |
| Ojetti et al. (November 2020) [28] | Cohort | 65 (19 vs. 46) | Rome (Italy) | 77% (53 vs. 87) | 38 (56 vs. 36) | NR | Good | Yes |
| Britton et al. (September, 2020) [29] | Retrospective | 44 (31 vs. 13) | NY (USA) | 48% (55 vs. 31) | 56 (53 vs. 63) | 16% (16 vs. 15) | Good | No |
| Author | Severe Group (Mean ± SD) | Non-Severe Group (Mean ± SD) | Confidence Interval (p-Value) | Primary Results/Conclusion |
|---|---|---|---|---|
| Serum | ||||
| Chen et al. (June 2020) [14] | 9220 | 7800 | p-value = 0.0001 | Calprotectin circulating level strongly correlated with mean oxygen score and is significantly raised in COVID-19 patients who died. Hence, a potential role in the assessment of prognosis in these patients. AUC for calprotectin (ICU vs. non-ICU) = 0.860, 85% sensitivity, 82.7% specific, 6195.015 cut-off (COVID-GRAM score 0.810, HMGB1—0.781). Serum calprotectin was highly correlated with quick-Sequential Organ Failure score (qSOFA) score and oxygen demand. |
| De Guadiana Romualdo et al. (August 2020) [25] | 7900 (5060) | 3540 (2270) | p-value < 0.001 | Serum calprotectin correlated positively with ferritin, CRP, Calprotectin plasma level was significantly higher in non-survivors COVID-19 group, suggesting a possible prognostic value for serum calprotectin in COVID-19 infection. |
| Silvin et al. (August 2020) [12] | 4983.4 (2815.1) | 985.0 (1161.9) | p-value < 0.0001 | Severe COVID-19 patients have a peripheral blood and lungs characterized by HLA-DRlow monocytes and immature neutrophils. They also possess higher calprotectin levels that correlates positively with neutrophil count and severity of COVID-19 infection. Absence of non-classical monocytes could select patients at high risk of ICU admission or death. Serum calprotectin correlated with the ROC AUC (discriminating capacity) of the plasma calprotectin level was 0.9590 (non-classical monocytes = 0.8705, CD16low = 0.7983, IFNα = 0.5613). |
| Shi et al. (July 2020) [26] | 11251.26 (7776.52) | 4709.79 (5214.13) | p-value < 0.0001 | Calprotectin level was significantly raised in ICU group compared to the non-ICU group, which suggests that higher calprotectin levels are associated with higher deaths. Serum calprotectin also correlated with D-Dimer, qSOFA score (it reflects the functional state of the organs), COVID-GRAM risk scores. AUC for calprotectin (need invasive ventilation vs. No need for invasive ventilation) = 0.794 (CRP = 0.614, ferritin = 0.562). |
| Bauer et al. (November 2020) [27] | 3770 (1765) | 2080 (988) | p-value = 0.15 | Calprotectin is a new and important discriminator in COVID-19 with regards to disease outcome especially multiple organ failure. Estimation of the serum levels of calprotectin can be easily adopted into routine laboratories and performs better than traditional biomarkers such as CRP, lactate and PCT (procalcitonin). |
| Fecal | ||||
| Effenberger et al. (August 2020) [18] | 80.2 (26.51) | 17.3 (3.83) | p-value = 0.001 | FC levels were significantly higher in COVID-19 patients with diarrhea and correlated positively with serum IL-6 but not with CRP and ferritin. Fecal SARS-CoV-2 was only detected in COVID-19 group with ongoing diarrhea but not in the other two groups. |
| Ojetti et al. (November 2020) [28] | 71.3 | 11.9 | p-value = 0.001 | A significant association exist between high fecal calprotectin level and COVID-19 pneumonia as well as disease severity. Systemic involvement often accompanies the pneumonia even in asymptomatic COVID-19 patients. Such systemic involvements may not present with gastrointestinal symptoms but can be demonstrated by high fecal calprotectin level. |
| Britton et al. (September 2020) [29] | 2.5 | 2.0 | p-value = 0.12 | SARS-CoV-2 RNA was seen in stools of 41% of patients, and is seen more in those that have diarrhea than in others who did not have diarrhea. Severe COVID-19 was associated with elevated IL-23 and intestinal virus-specific IgA level. Fecal calprotectin did not correlate with gastrointestinal symptoms or viral level detected. |
| Author | Methodology | Primary Results/Conclusion |
|---|---|---|
| Unterman et al. (2020) [30] | Single cell analysis | Calprotectin circulating level is significantly elevated in COVID-19 patients who died. Hence, a potential role in the evaluation of prognosis in these patients. |
| Livanos et al. (2020) [31] | Single cell analysis | Study negates the concept of gut tropism. It reports that there is a significant decrease in severity and deaths of COVID-19 when patients present with GI symptoms such as diarrhea, nausea and vomiting |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Udeh, R.; Advani, S.; de Guadiana Romualdo, L.G.; Dolja-Gore, X. Calprotectin, an Emerging Biomarker of Interest in COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 775. https://doi.org/10.3390/jcm10040775
Udeh R, Advani S, de Guadiana Romualdo LG, Dolja-Gore X. Calprotectin, an Emerging Biomarker of Interest in COVID-19: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(4):775. https://doi.org/10.3390/jcm10040775
Chicago/Turabian StyleUdeh, Raphael, Shailesh Advani, Luis García de Guadiana Romualdo, and Xenia Dolja-Gore. 2021. "Calprotectin, an Emerging Biomarker of Interest in COVID-19: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 4: 775. https://doi.org/10.3390/jcm10040775