Surgical Treatment of Diabetic Foot Ulcers Complicated by Osteomyelitis with Gentamicin-Loaded Calcium Sulphate-Hydroxyapatite Biocomposite

 , , ,
, , ,
Abstract
:1. Introduction
2. Experimental Section
3. Results
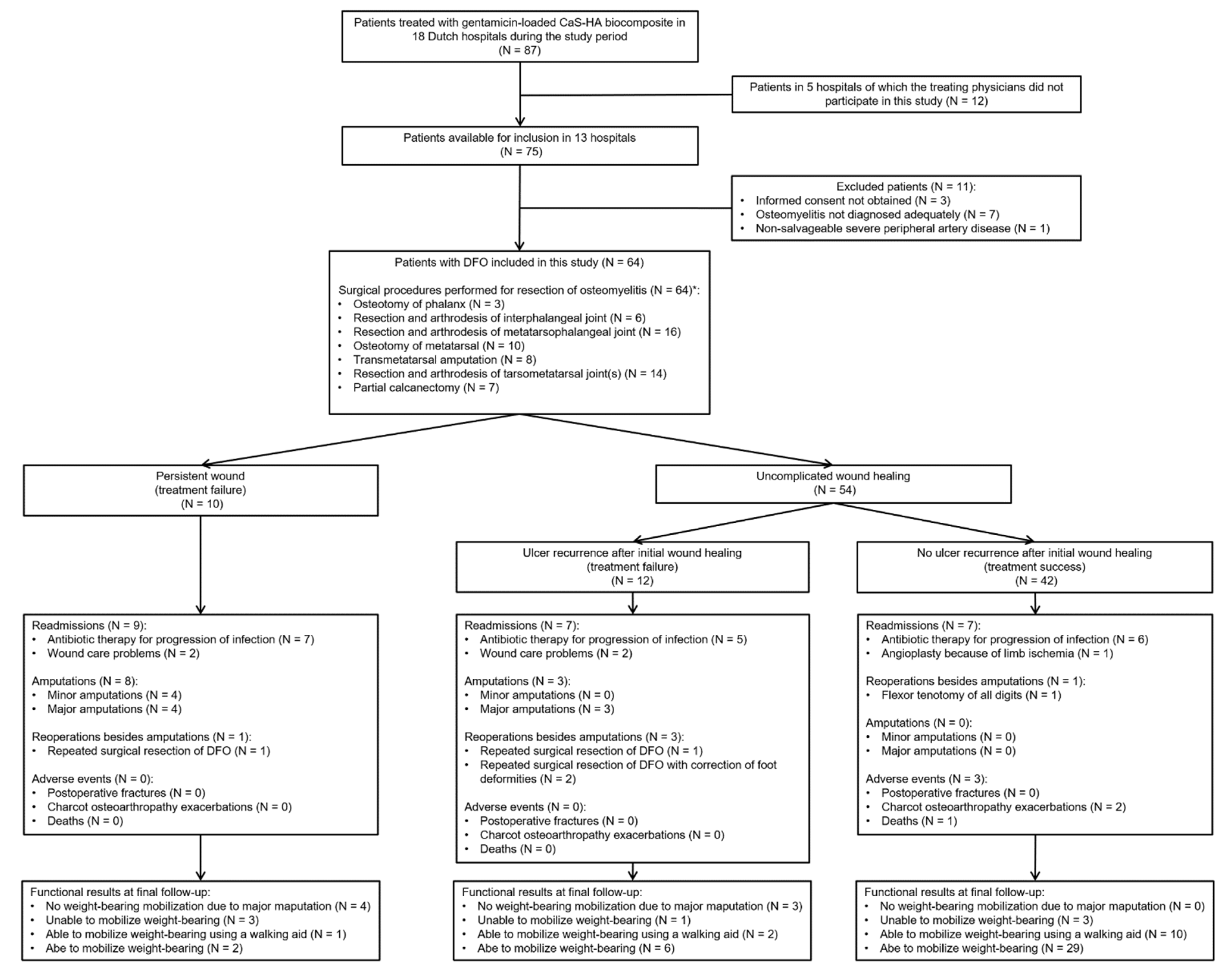
3.1. Patients and Procedures
3.2. Primary Outcomes
3.3. Secondary Outcomes
3.4. Treatment Failures
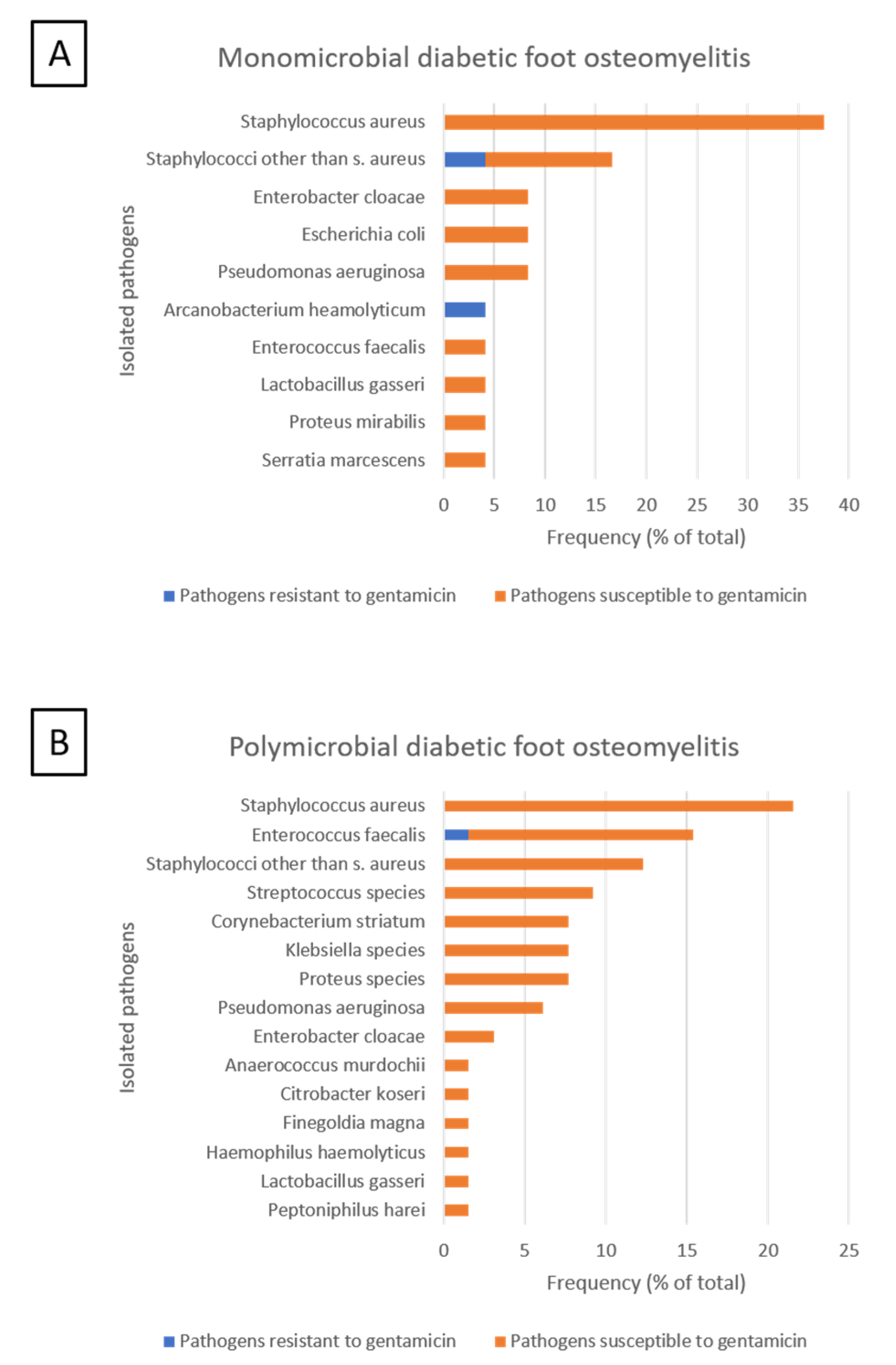
3.5. Microbiological Analysis
3.6. Postoperative Treatment
3.7. Adverse Events
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgical Procedures | No. (%) |
|---|---|
| Osteotomy of phalanx/phalanges, debridement and dead space filling with gentamicin-loaded CaS-HA biocomposite. | 3 (5) |
| Arthrotomy of interphalangeal joint(s), resection with base and head of adjacent phalanges, dead space filling with gentamicin-loaded CaS-HA biocomposite. | 3 (5) |
| Arthrotomy of interphalangeal joint(s), resection with base and head of adjacent phalanges, dead space filling with gentamicin-loaded CaS-HA biocomposite, arthrodesis with Kirschner wire. | 3 (5) |
| Arthrotomy of metatarsophalangeal joint(s), resection with metatarsal head(s) and base of proximal phalanx/phalanges, dead space filling with gentamicin-loaded CaS-HA biocomposite. | 14 (22) |
| Arthrotomy of metatarsophalangeal joint(s), resection with metatarsal head(s) and base of proximal phalanx/phalanges, dead space filling with gentamicin-loaded CaS-HA biocomposite, arthrodesis with Kirschner wire. | 2 (3) |
| Osteotomy of metatarsal(s), debridement of medullary canal(s), filling with gentamicin-loaded CaS-HA biocomposite. | 10 (16) |
| Amputation of metatarsal head(s), debridement of medullary canal(s) and filling with gentamicin-loaded CaS-HA biocomposite. | 8 (13) |
| Arthrotomy of tarsometatarsal joint(s), resection of joint with distal part of one or multiple tarsals and base of one or multiple metatarsals, dead space filling with gentamicin-loaded CaS-HA biocomposite. | 8 (13) |
| Arthrotomy of tarsometatarsal joint(s), resection with distal part of tarsal(s) and base of metatarsal(s), dead space filling with gentamicin-loaded CaS-HA biocomposite, temporary external fixation. | 1 (2) |
| Arthrotomy of tarsometatarsal joint(s), resection with distal part of tarsal(s) and base of metatarsal(s), dead space filling with gentamicin-loaded CaS-HA biocomposite, internal screw fixation. | 1 (2) |
| Partial or complete extirpation of tarsal(s), dead space filling with gentamicin-loaded CaS-HA biocomposite. | 1 (2) |
| Partial or complete extirpation of tarsal(s), dead space filling with gentamicin-loaded CaS-HA biocomposite, temporary external fixation | 2 (3) |
| Partial or complete extirpation of tarsal(s), dead space filling with gentamicin-loaded CaS-HA biocomposite, internal screw fixation. | 1 (2) |
| Partial calcanectomy, surgical debridement and dead space filling with gentamicin-loaded CaS-HA biocomposite. | 4 (6) |
| Partial calcanectomy, drilling of multiple tunnels in the calcaneum, filling with gentamicin-loaded CaS-HA biocomposite (“silo technique”) [24]. | 3 (5) |
| Treatment Characteristics | No. (%) |
| Volume of gentamicin-loaded CaS-HA biocomposite used (mL). | 5 (4-5) |
| Form of gentamicin-loaded CaS-HA biocomposite used | |
| 59 (92) |
| 5 (8) |
| Use of pressure tourniquet during surgical procedure. | 21 (33) |
| Method of surgical wound closure | |
| 57 (89) |
| 6 (9) |
| 1 (2) |
| Perioperative antibiotic therapy | |
| 32 (50) |
| 1 (3) |
| 7 (23) |
| 1 (3) |
| 1 (3) |
| 2 (6) |
| 1 (3) |
| 5 (16) |
| 11 (34) |
| 1 (3) |
| 1 (3) |
| 1 (3) |
| Route of administration of perioperative antibiotic therapy | |
| 6 (9) |
| 26 (41) |
| Method of anaesthesia | |
| 18 (28) |
| 15 (24) |
| 29 (45) |
| 2 (3) |
| Duration of surgery (minutes) | 46 ± 21 |
References
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Zhang, Y.; Lazzarini, P.A.; McPhail, S.M.; van Netten, J.J.; Armstrong, D.G.; Pacella, R.E. Global Disability Burdens of Diabetes-Related Lower-Extremity Complications in 1990 and 2016. Diabetes Care 2020, 43, 964–974. [Google Scholar] [CrossRef]
- Prompers, L.; Huijberts, M.; Apelqvist, J.; Jude, E.; Piagessi, A.; Bakker, K.; Edmonds, M.; Holstein, P.; Jirkovska, A.; Mauricio, D.; et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia 2007, 50, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Jia, L.; Parker, C.N.; Parker, T.J.; Kinnear, E.M.; Derhy, P.H.; Alvarado, A.M.; Huygens, F.; Lazzarini, P.A. Incidence and risk factors for developing infection in patients presenting with uninfected diabetic foot ulcers. PLoS ONE 2017, 12, e0177916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raspovic, K.M.; Wukich, D.K. Self-reported quality of life and diabetic foot infections. J. Foot Ankle Surg. 2014, 53, 716–719. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.W.; Selvarajah, S.; Mathioudakis, N.; Sherman, R.E.; Hines, K.F.; Black, J.H., III; Abularrage, C.J. Burden of Infected Diabetic Foot Ulcers on Hospital Admissions and Costs. Ann. Vasc. Surg. 2016, 33, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Lavery, L.A.; Armstrong, D.G.; Peters, E.J.G.; Lipsky, B.A. Probe-to-bone test for diagnosing diabetic foot osteomyelitis: Reliable or relic? Diabetes Care 2007 30, 270–274. [CrossRef] [Green Version]
- Van Netten, J.J.; Bus, S.A.; Apelqvist, J.; Lipsky, B.A.; Hinchliffe, R.J.; Game, F.L.; Rayman, G.; Lazzarini, P.A.; Forsythe, R.O.; Peters, E.J.G.; et al. Definitions and criteria for diabetic foot disease. Diabetes Metab. Res. Rev. 2020, 36, e3268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsky, B.A.; Itani, K.; Norden, C. Treating foot infections in diabetic patients: A randomized, multicenter, open-label trial of linezolid versus ampicillin-sulbactam/amoxicillin-clavulanate. Clin. Infect. Dis. 2004, 38, 17–24. [Google Scholar] [CrossRef]
- Mutluoglu, M.; Sivrioglu, A.K.; Eroglu, M.; Uzun, G.; Turhan, V.; Ay, H.; Lipsky, B.A. The implications of the presence of osteomyelitis on outcomes of infected diabetic foot wounds. Scand. J. Infect. Dis. 2013, 45, 497–503. [Google Scholar] [CrossRef]
- Gurlek, A.; Bayraktar, M.; Savas, C.; Gedik, O. Amputation rate in 147 Turkish patients with diabetic foot: The Hacettepe University Hospital experience. Exp. Clin. Endocrinol. Diabetes 1998, 106, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Hartemann-Heurtier, A.; Senneville, E. Diabetic foot osteomyelitis. Diabetes Metab. 2008, 34, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Schaper, N.C.; van Netten, J.J.; Apelqvist, J.; Bus, S.A.; Hinchliffe, R.J.; Lipsky, B.A. Practical Guidelines on the prevention and management of diabetic foot disease (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsky, B.A.; Senneville, E.; Abbas, Z.G.; Aragón-Sánchez, F.J.; Diggle, M.; Embil, J.M.; Kono, S.; Lavery, L.A.; Malone, M.; van Asten, S.A.; et al. Guidelines on the diagnosis and treatment of foot infection in persons with diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3280. [Google Scholar] [CrossRef] [Green Version]
- Jeffcoate, W.J.; Bus, S.A.; Game, F.L.; Hinchliffe, R.J.; Price, P.E.; Schaper, N.C. Reporting standards of studies and papers on the prevention and management of foot ulcers in diabetes: Required details and markers of good quality. Lancet Diabetes Endocrinol. 2016, 4, 781–788. [Google Scholar] [CrossRef] [Green Version]
- Ha Van, G.; Siney, H.; Danan, J.P.; Sachon, C.; Grimaldi, A. Treatment of osteomyelitis in the diabetic foot. Contribution of conservative surgery. Diabetes Care 1996, 19, 1257–1260. [Google Scholar] [CrossRef]
- Aragón-Sánchez, F.J.; Cabrera-Galván, J.J.; Quintana-Marrero, Y.; Hernández-Herrero, M.J.; Lázaro-Martínez, J.L.; García-Morales, E.; Beneit-Montesinos, J.V.; Armstrong, D.G. Outcomes of surgical treatment of diabetic foot osteomyelitis: A series of 185 patients with histopathological confirmation of bone involvement. Diabetologia 2008, 51, 1962–1970. [Google Scholar] [CrossRef] [Green Version]
- Aragón-Sánchez, F.J.; Lázaro-Martínez, J.L.; Hernández-Herrero, C.; Campillo-Villorio, N.; Quintana-Marrero, Y.; García-Morales, E.; Hernández-Herrero, M.J. Does osteomyelitis in the feet of patients with diabetes really recur after surgical treatment? Natural history of a surgical series. Diabet. Med. 2012, 29, 813–818. [Google Scholar] [CrossRef]
- Henke, P.K.; Blackburn, S.A.; Wainess, R.W.; Cowan, J.; Terando, A.; Proctor, M.; Wakefield, T.W.; Upchurch, G.R., Jr.; Stanley, J.C.; Greenfield, L.J. Osteomyelitis of the foot and toe in adults is a surgical disease: Conservative management worsens lower extremity salvage. Ann. Surg. 2005, 241, 884–885. [Google Scholar] [CrossRef]
- Nilsson, M.; Zheng, M.H.; Tägil, M. The composite of hydroxyapatite and calcium sulphate: A review of preclinical evaluation and clinical applications. Expert Rev. Med. Devices 2013, 10, 675–684. [Google Scholar] [CrossRef]
- Markakis, K.; Faris, A.R.; Sharaf, H.; Faris, B.; Rees, S.; Bowling, F.L. Local Antibiotic Delivery Systems: Current and Future Applications for Diabetic Foot Infections. Int. J. Low Extrem. Wounds 2018, 17, 14–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNally, M.A.; Ferguson, J.Y.; Lau, A.C.K.; Diefenbeck, M.; Scarborough, M.; Ramsden, A.J.; Atkins, B.L. Single-stage treatment of chronic osteomyelitis with a new absorbable, gentamicin-loaded, calcium sulphate/ hydroxyapatite biocomposite. Bone Jt. J. 2016, 98B, 1289–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niazi, N.S.; Drampalos, E.; Morrissey, N.; Jahangir, N.; Wee, A.; Pillai, A. Adjuvant antibiotic loaded bio composite in the management of diabetic foot osteomyelitis—A multicentre study. Foot 2019, 39, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Drampalos, E.; Mohammad, H.R.; Kosmidis, C.; Balal, M.; Wong, J.; Pillai, A. Single stage treatment of diabetic calcaneal osteomyelitis with an absorbable gentamicin-loaded calcium sulphate/hydroxyapatite biocomposite: The Silo technique. Foot 2018, 34, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Stravinskas, M.; Horstmann, P.; Ferguson, J.; Hettwer, W.; Nilsson, M.; Tarasevicius, S.; Petersen, M.M.; McNally, M.A.; Lidgren, L. Pharmacokinetics of gentamicin eluted from a regenerating bone graft substitute: In vitro and clinical release studies. Bone Jt. Res. 2016, 5, 427–435. [Google Scholar] [CrossRef]
- Colding-Rasmussen, T.; Horstmann, P.; Petersen, M.M.; Hettwer, W. Antibiotic Elution Characteristics and Pharmacokinetics of Gentamicin and Vancomycin from a Mineral Antibiotic Carrier: An in vivo Evaluation of 32 Clinical Cases. J. Bone Jt. Infect. 2018, 3, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, M.; Wang, J.S.; Wielanek, L.; Tanner, K.E.; Lidgren, L. Biodegradation and biocompatability of a calcium sulphate-hydroxyapatite bone substitute. J. Bone Jt. Surg. Br. 2004, 86, 120–125. [Google Scholar] [CrossRef]
- Hutting, K.H.; van Netten, J.J.; Dening, J.; ten Cate, W.A.; van Baal, J.G. Surgical debridement and gentamicin-loaded calcium sulphate/hydroxyapatite bone void filling to treat diabetic foot osteomyelitis. Diabet. Foot J. 2019, 22, 22–27. [Google Scholar]
- Whisstock, C.; Volpe, A.; Ninkovic, S.; Marin, M.; Meloni, M.; Bruseghin, M.; Boschetti, G.; Brocco, E. Multidisciplinary Approach for the Management and Treatment of Diabetic Foot Infections with a Resorbable, Gentamicin-Loaded Bone Graft Substitute. J. Clin. Med. 2020, 9, 3586. [Google Scholar] [CrossRef]
- Richtlijnen Database. Richtlijn Diabetische Voet. Available online: https://richtlijnendatabase.nl/richtlijn/diabetische_voet/startpagina_diabetische_voet.html (accessed on 1 April 2020).
- NICE. NICE Guideline [NG19]: Diabetic Foot Problems: Prevention and Management. Available online: https://www.nice.org.uk/guidance/ng19/chapter/Recommendations#diabetic-foot-infection (accessed on 1 April 2020).
- Senneville, E.M.; Lipsky, B.A.; van Asten, S.A.V.; Peters, E.J. Diagnosing diabetic foot osteomyelitis. Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3250. [Google Scholar] [CrossRef] [Green Version]
- Mills, J.L.S.; Conte, M.S.; Armstrong, D.G.; Pomposelli, F.B.; Schanzer, A.; Sidawy, A.N.; Andros, G. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk stratification based on wound, ischemia, and foot infection (WIfI). J. Vasc. Surg. 2014, 59, 220–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ince, P.; Abbas, Z.G.; Lutale, J.K.; Basit, A.; Chohan, F.; Morbach, S.; Möllenberg, J.; Game, F.L.; Jeffcote, W.J. Use of the SINBAD Classification System and Score in Comparing Outcome of Foot Ulcer Management on Three Continents. Diabetes Care 2008, 31, 964–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bus, S.A.; Waaijman, R.; Arts, M.; de Haart, M.; Busch-Westbroek, T.; van Baal, J.G.; Nollet, F. Effect of custom-made footwear on foot ulcer recurrence in diabetes: A multicenter randomized controlled trial. Diabetes Care 2013, 36, 4109–4116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 9.0. 2019. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_9.0_Breakpoint_Tables.pdf (accessed on 1 December 2019).
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Faglia, E.; Clerici, G.; Caminiti, M.; Curci, V.; Somalvico, F. Influence of osteomyelitis location in the foot of diabetic patients with transtibial amputation. Foot Ankle Int. 2013, 34, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.A.; Valk, G.D.; van Deursen, R.W.; Armstrong, D.G.; Caravaggi, C.; Hlaváček, P.; Bakker, K.; Cavanagh, P.R. The effectiveness of footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in diabetes: A systematic review. Diabetes Metab. Res. Rev. 2008, 24 (Suppl. 1), S162–S180. [Google Scholar] [CrossRef] [PubMed]
- Ince, P.; Kendrick, D.; Game, F.; Jeffcoate, W. The association between baseline characteristics and the outcome of foot lesions in a UK population with diabetes. Diabet. Med. 2007, 24, 977–981. [Google Scholar] [CrossRef]
- Bus, S.A.; Armstrong, D.G.; Gooday, C.; Jarl, G.; Caravaggi, C.; Viswanathan, V.; Lazzarini, P.A. Guidelines on offloading foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3274. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Characteristics | All Patients | Patients with Persistent Wounds | Patients with Ulcer Recurrence | Patients with Treatment Success | p Value |
|---|---|---|---|---|---|
| (N = 64) | (n = 10) | (n = 12) | (n = 42) | ||
| Follow-up in weeks | 43 (20–61) | 14 (12–27) | 61 (23–91) | 44 (28–61) | 0.001 * |
| Male sex | 50 (78) | 8 (80) | 9 (75) | 33 (79) | >0.99 |
| Age, years | 63 ± 11 | 66 ± 9 | 56 ± 14 | 64 ± 11 | 0.089 |
| Type of diabetes mellitus | |||||
| Type 1 diabetes | 5 (8) | 0 | 2 (17) | 3 (7) | 0.385 |
| Type 2 diabetes | 59 (92) | 10 (100) | 10 (83) | 39 (93) | |
| Diabetes duration in years | 17 (13–21) | 17 (12–22) | 16 (10–20) | 17 (14–22) | 0.359 |
| Insulin treatment | 40 (63) | 5 (50) | 9 (75) | 26 (62) | 0.482 |
| Heart failure | 18 (28) | 3 (30) | 3 (25) | 12 (29) | >0.99 |
| Nephropathy | 21 (33) | 4 (40) | 6 (50) | 11 (26) | 0.262 |
| Haemodialysis | 5 (8) | 0 | 2 (17) | 3 (7) | 0.385 |
| BMI > 35 kg/m2 | 5 (8) | 0 | 1 (8) | 4 (10) | 0.819 |
| Retinopathy | 23 (36) | 4 (40) | 4 (33) | 15 (36) | >0.99 |
| Charcot osteoarthropathy | 18 (28) | 0 (0) | 7 (58) | 11 (26) | 0.010 ** |
| Loss of protective sensation | 59 (92) | 10 (100) | 12 (100) | 37 (88) | 0.496 |
| Limb ischemia [33] | |||||
| 33 (52) | 3 (30) | 10 (84) | 20 (48) | 0.035 *** |
| 24 (37) | 7 (70) | 1 (8) | 16 (38) | |
| 7 (11) | 0 | 1 (8) | 6 (14) | |
| Previous ipsilateral amputation | |||||
| 42 (66) | 9 (90) | 6 (50) | 27 (64) | 0.486 |
| 3 (5) | 0 | 0 | 3 (7) | |
| 9 (14) | 1 (10) | 4 (33) | 4 (10) | |
| 6 (9) | 0 | 1 (8) | 5 (12) | |
| 4 (6) | 0 | 1 (8) | 3 (7) | |
| Previous contralateral major amputation | 4 (6) | 0 | 1 (8) | 3 (7) | >0.99 |
| Foot deformity | |||||
| 32 (50) | 6 (60) | 3 (25) | 23 (55) | 0.071 |
| 9 (14) | 1 (10) | 2 (17) | 6 (14) | |
| 8 (13) | 3 (30) | 1 (8) | 4 (10) | |
| 15 (23) | 0 | 6 (50) | 9 (21) | |
| Previous ulcer on index ulcer location | 24 (38) | 5 (50) | 7 (58) | 12 (29) | 0.111 |
| Index ulcer duration in weeks | 20 (13–46) | 19 (10–42) | 37 (21–79) | 18 (10–43) | 0.039 † |
| Index ulcer location | |||||
| 41 (64) | 5 (50) | 5 (42) | 31 (74) | 0.101 |
| 14 (22) | 2 (20) | 5 (42) | 7 (17) | |
| 9 (14) | 3 (30) | 2 (17) | 4 (9) | |
| Index ulcer on plantar aspect of foot | 37 (58) | 8 (80) | 7 (58) | 22 (52) | 0.276 |
| Index ulcer size in cm2 | 3 (2–5) | 4 (3–4) | 5 (2–7) | 3 (2–4) | 0.367 |
| SINBAD classification score [34] | 5 (4–5) | 5 (4–5) | 5 (4–5) | 5 (5–5) | 0.153 |
| Previous treatment of DFO | |||||
| 16 (25) | 2 (20) | 3 (25) | 11 (26) | 0.571 |
| 9 (14) | 3 (30) | 2 (17) | 4 (10) | |
| 39 (61) | 5 (50) | 7 (58) | 27 (64) | |
| Duration of antibiotic therapy in weeks | 8 (6–10) | 7 (6–10) | 9 (6–19) | 8 (6–10) | 0.477 |
| Preoperative revascularization procedure | |||||
| 48 (75) | 7 (70) | 10 (83) | 31 (74) | 0.840 |
| 15 (23) | 3 (30) | 2 (17) | 10 (24) | |
| 1 (2) | 0 | 0 | 1 (2) | |
| Surgical procedure with gentamicin-loaded CaS-HA biocomposite involved a minor amputation | 8 (13) | 4 (40) | 3 (25) | 1 (2) | 0.001 †† |
| Fixation methods used in the surgical procedure with gentamicin-loaded CaS-HA biocomposite | |||||
| 55 (86) | 10 (100) | 9 (75) | 36 (86) | 0.448 |
| 7 (11) | 0 | 2 (17) | 5 (12) | |
| 2 (3) | 0 | 1 (8) | 1 (2) | |
| Microbiological analysis of osteomyelitis | |||||
| 15 (23) | 3 (30) | 2 (17) | 10 (24) | 0.755 |
| 24 (38) | 2 (20) | 3 (25) | 19 (45) | 0.779 |
| 16 (25) | 2 (20) | 2 (17) | 12 (28) | |
| 8 (12) | 0 | 1 (8) | 7 (17) | |
| 25 (39) | 5 (50) | 7 (58) | 13 (31) | 0.179 |
| 11 (17) | 1 (10) | 2 (17) | 8 (19) | |
| 13 (20) | 3 (30) | 5 (42) | 5 (12) | |
| 1 (2) | 1 (10) | 0 | 0 | |
| 3 (5) | 2 (20) | 1 (8) | 0 | 0.020 ‡ |
| Characteristic | Univariable Analysis | |
|---|---|---|
| Hazard Ratio (95%-CI) | p Value | |
| Gentamicin-resistant osteomyelitis | 3.847 (1065–13.899) | 0.040 |
| Index ulcer location | 0.029 | |
| Reference | |
| 3.022 (1127–8104) | 0.028 |
| 3.624 (1187–11.060) | 0.024 |
| Surgical procedure with gentamicin-loaded CaS-HA biocomposite involved a minor amputation | 3.965 (1608–9777) | 0.003 |
| Author (Year) | Study Design | Patients | Intervention | Follow-Up | Results | QUADAS-2 Score [37] |
|---|---|---|---|---|---|---|
| This study | Multicenter RCS | Inclusion of 64 patients with DFO after unsuccessful conventional treatment (antibiotic therapy alone, or surgical debridement or minor amputation with adjunctive antibiotic therapy). |
| Median 43 (IQR, 20–61) weeks. |
| Risk of bias: |
|
|
| ||||
|
|
| ||||
|
| |||||
|
| |||||
| Applicability concerns: | ||||||
| ||||||
| ||||||
| ||||||
| Whisstock, et al. [29] (2020) | Single- center RCS | Inclusion of 35 patients (aged 18–80 years) with DFO, with or without Charcot neuroarthropathy and an otherwise normal function of the lower extremity. |
| 12 months. Three patients lost to follow-up. |
| Risk of bias: |
|
|
| ||||
|
|
| ||||
|
| |||||
| ||||||
| Applicability concerns: | ||||||
| ||||||
| ||||||
| ||||||
| Hutting, et al. [28] (2019) | Case report | Treatment of 1 patient with CN-related deformity and midfoot DFO after unsuccessful surgical treatment. |
| 12 months |
| Risk of bias: |
|
| |||||
|
|
| ||||
| ||||||
| ||||||
| Applicability concerns: | ||||||
| ||||||
| ||||||
| ||||||
| Niazi, et al. [23] (2019) | Multicenter RCS | Inclusion of 70 patients with DFO of the forefoot (62%), midfoot (33%), or hindfoot (5%). CN-related deformity in 9 patients (13%) |
| Mean 10 (range, 4–28) months |
| Risk of bias: |
|
|
| ||||
|
| |||||
|
| |||||
|
| |||||
| Applicability concerns: | ||||||
| ||||||
| ||||||
| ||||||
| Drampalos, et al. [24] (2018) | Single-center RCS | Inclusion of 12 patients with calcaneal DFO without involvement of the posterior subtalar joint. |
| Mean 16 (range, 12–18) weeks |
| Risk of bias: |
|
|
| ||||
| ||||||
| ||||||
| ||||||
| Applicability concerns: | ||||||
| ||||||
| ||||||
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hutting, K.H.; aan de Stegge, W.B.; van Netten, J.J.; ten Cate, W.A.; Smeets, L.; Welten, G.M.J.M.; Scharn, D.M.; de Vries, J.-P.P.M.; van Baal, J.G. Surgical Treatment of Diabetic Foot Ulcers Complicated by Osteomyelitis with Gentamicin-Loaded Calcium Sulphate-Hydroxyapatite Biocomposite. J. Clin. Med. 2021, 10, 371. https://doi.org/10.3390/jcm10020371
Hutting KH, aan de Stegge WB, van Netten JJ, ten Cate WA, Smeets L, Welten GMJM, Scharn DM, de Vries J-PPM, van Baal JG. Surgical Treatment of Diabetic Foot Ulcers Complicated by Osteomyelitis with Gentamicin-Loaded Calcium Sulphate-Hydroxyapatite Biocomposite. Journal of Clinical Medicine. 2021; 10(2):371. https://doi.org/10.3390/jcm10020371
Chicago/Turabian StyleHutting, Kor H., Wouter B. aan de Stegge, Jaap J. van Netten, Wouter A. ten Cate, Luuk Smeets, Gijs M. J. M. Welten, Dick M. Scharn, Jean-Paul P. M. de Vries, and Jeff G. van Baal. 2021. "Surgical Treatment of Diabetic Foot Ulcers Complicated by Osteomyelitis with Gentamicin-Loaded Calcium Sulphate-Hydroxyapatite Biocomposite" Journal of Clinical Medicine 10, no. 2: 371. https://doi.org/10.3390/jcm10020371