
The Use of Machine Learning Algorithms in the Evaluation of the Effectiveness of Resynchronization Therapy

 , , ,
, , ,
Abstract
:1. Introduction
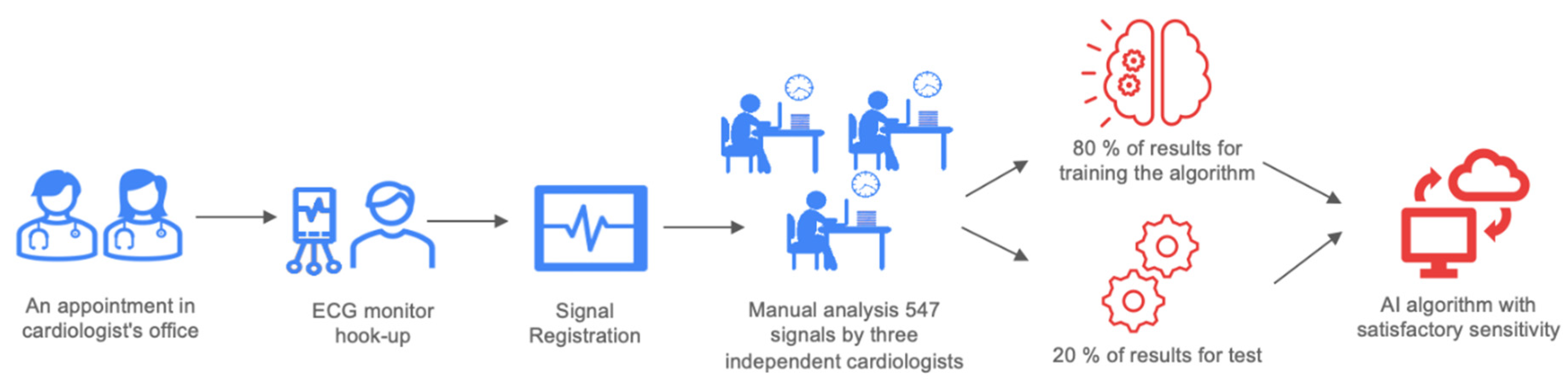
2. Material and Methods
- Class 1: effective CRT stimulation;
- Class 2: ineffective CRT stimulation;
- Class 3: CRT patient’s own rhythm/heartbeat morphology;
- Class 4: control group.
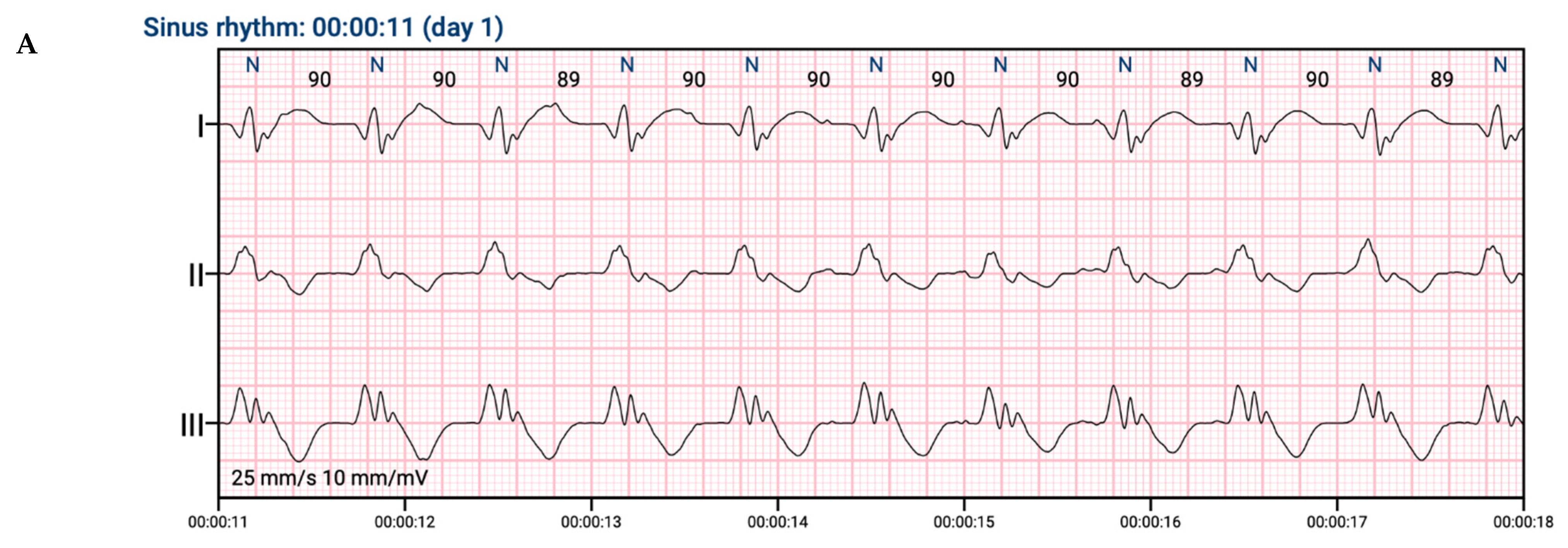
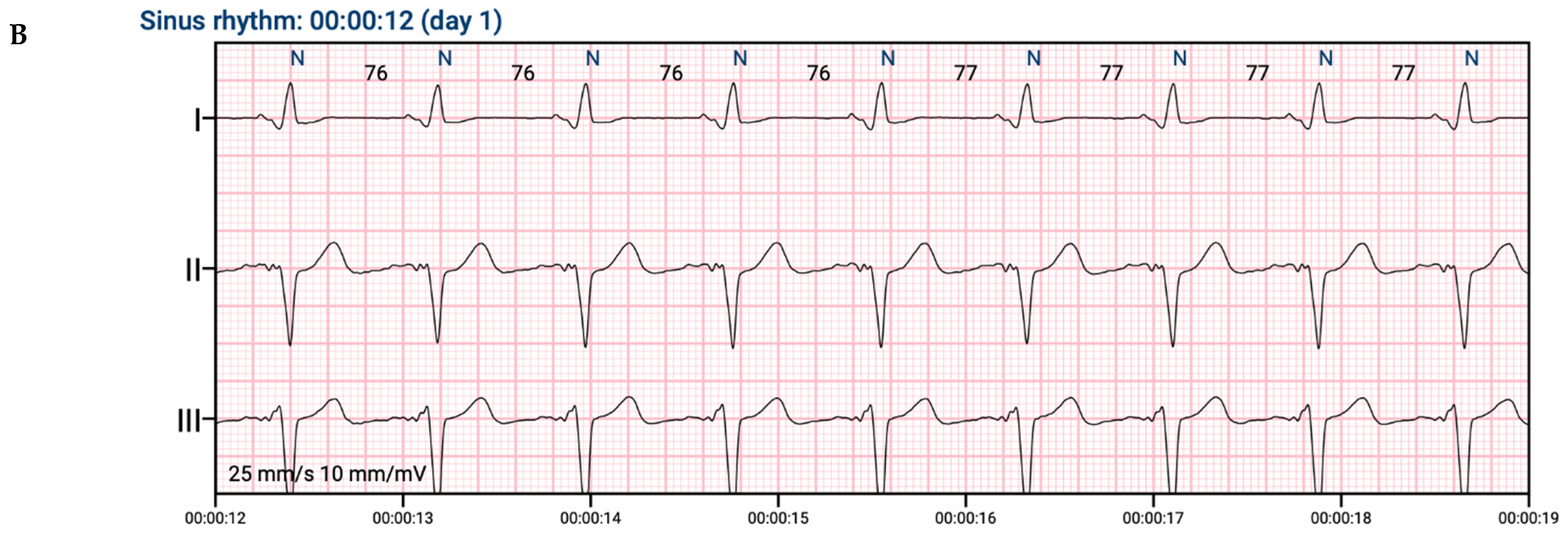
2.1. ECG Signal Processing
- R-detection: position of each heartbeat (understood as position of R-waves) in time was detected (by modified Pan–Tompkins algorithm) [10].
- Heartbeat segmentation: recording was segmented into 2-sec windows containing each detected heartbeat centered on the R-wave.
- Classification: a 2-sec window with labeled heartbeat was treated as an input to the classifier—deep convolutional neural network. Classifier was trained to distinguish 2 classes—effective and ineffective CRT pacing. As ineffective CRT pacing, all heartbeats from classes 2, 3, 4 were treated.
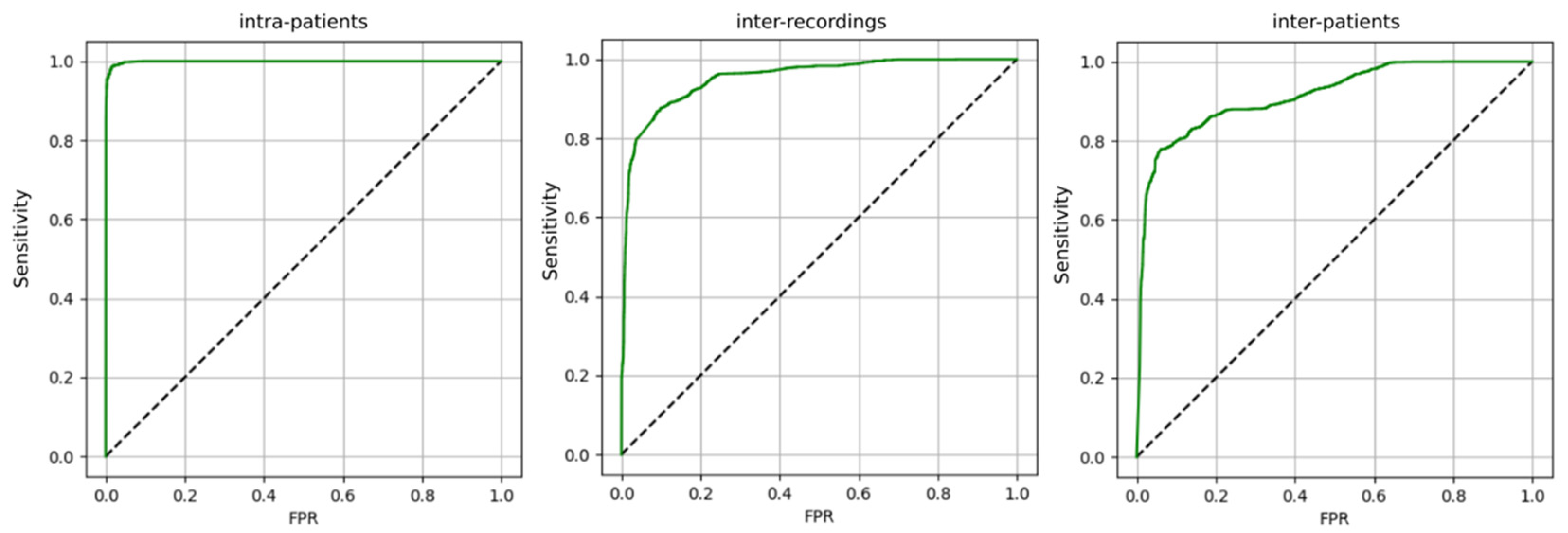
- Intra-patient—train and test sets can contain examples from all recordings;
- Inter-recording—train and test sets are separate in terms of recordings;
- Inter-patient—train and test sets are separate in terms of patients.
2.2. Theory/Calculation
- Sensitivity = TP/P;
- FPR = FP/N;
- Precision = TP/(TP + FP).
- Where:
- TP—number of heartbeats effectively stimulated in CRT therapy, correctly classified;
- FP—other heartbeats, falsely classified as effectively stimulated in CRT therapy;
- FPR—false positive rate;
- P—heartbeats effectively stimulated in CRT therapy;
- N—other heartbeats.
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Khan, M.A.; Hashim, M.J.; Mustafa, H.; Baniyas, M.Y.; Al Suwaidi, S.K.B.M.; Alkatheeri, R.; Alblooshi, F.M.K.; Almatrooshi, M.E.A.H.; Alzaabi, M.E.H.; Al Darmaki, R.S.; et al. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus 2020, 12, e9349. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. Corrigendum to: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Lindenfeld, J.; Feldman, A.M.; Saxon, L.; Boehmer, J.; Carson, P.; Ghali, J.K.; Anand, I.; Singh, S.; Steinberg, J.S.; Jaski, B.; et al. Effects of Cardiac Resynchronization Therapy With or Without a Defibrillator on Survival and Hospitalizations in Patients With New York Heart Association Class IV Heart Failure. Circulation 2007, 115, 204–212. [Google Scholar] [CrossRef] [Green Version]
- Cleland, J.G.; Freemantle, N.; Erdmann, E.; Gras, D.; Kappenberger, L.; Tavazzi, L.; Daubert, J.-C. Long-term mortality with cardiac resynchronization therapy in the Cardiac Resynchronization-Heart Failure (CARE-HF) trial. Eur. J. Heart Fail. 2012, 14, 628–634. [Google Scholar] [CrossRef]
- Liang, Y.; Ding, R.; Wang, J.; Gong, X.; Yu, Z.; Pan, L.; Huang, J.; Li, R.; Su, Y.; Zhu, S.; et al. Prediction of response after cardiac resynchronization therapy with machine learning. Int. J. Cardiol. 2021, 344, 120–126. [Google Scholar] [CrossRef]
- Howell, S.J.; Stivland, T.; Stein, K.; Ellenbogen, K.A.; Tereshchenko, L.G. Using Machine-Learning for Prediction of the Response to Cardiac Resynchronization Therapy: The SMART-AV Study. JACC Clin. Electrophysiol. 2021, 7, 1505–1515. [Google Scholar] [CrossRef] [PubMed]
- Mullens, W.; Auricchio, A.; Martens, P.; Witte, K.; Cowie, M.R.; Delgado, V.; Dickstein, K.; Linde, C.; Vernooy, K.; Leyvaet, F.; et al. Optimized implementation of cardiac resynchronization therapy: A call for action for referral and optimization of care: A joint position statement from the Heart Failure Association (HFA), European Heart Rhythm Association (EHRA), and European Association of Cardiovascular Imaging (EACVI) of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 2349–2369. [Google Scholar]
- Van Stipdonk, A.; Wijers, S.; Meine, M.; Vernooy, K. ECG Patterns in Cardiac Resynchronization Therapy. J. Atr. Fibrillation 2015, 7, 33–38. [Google Scholar] [CrossRef]
- Korantzopoulos, P.; Zhang, Z.; Li, G.; Fragakis, N.; Liu, T. Meta-Analysis of the Usefulness of Change in QRS Width to Predict Response to Cardiac Resynchronization Therapy. Am. J. Cardiol. 2016, 118, 1368–1373. [Google Scholar] [CrossRef]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Cosín, J.; Díez, J.; on behalf of the TORIC Investigators. Torasemide in chronic heart failure: Results of the TORIC study. Eur. J. Heart Fail. 2002, 4, 507–513. [Google Scholar] [CrossRef]
- Bilchick, K.C.; Kamath, S.; DiMarco, J.P.; Stukenborg, G.J. Bundle-Branch Block Morphology and Other Predictors of Outcome After Cardiac Resynchronization Therapy in Medicare Patients. Circulation 2010, 122, 2022–2030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gold, M.R.; Thebault, C.; Linde, C.; Abraham, W.T.; Gerritse, B.; Ghio, S.; Sutton, M.S.J.; Daubert, J.-C. Effect of QRS duration and morphology on cardiac resynchronization therapy outcomes in mild heart failure: Results from the Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction (REVERSE) study. Circulation 2012, 126, 822–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versteeg, H.; Schiffer, A.A.; Widdershoven, J.W.; Meine, M.M.; Doevendans, P.A.; Pedersen, S.S. Response to Cardiac Resynchronization Therapy: Is It Time to Expand the Criteria? Pacing Clin. Electrophysiol. 2009, 32, 1247–1256. [Google Scholar] [CrossRef] [PubMed]
- Sieniewicz, B.J.; Gould, J.; Porter, B.; Sidhu, B.S.; Teall, T.; Webb, J.; Carr-White, G.; Rinaldi, C. Understanding non-response to cardiac resynchronisation therapy: Common problems and potential solutions. Heart Fail. Rev. 2018, 24, 41–54. [Google Scholar] [CrossRef] [Green Version]
- Daubert, C.; Behar, N.; Martins, R.P.; Mabo, P.; Leclercq, C. Avoiding non-responders to cardiac resynchronization therapy: A practical guide. Eur. Heart J. 2016, 38, 1463–1472. [Google Scholar] [CrossRef]
- Piotrowicz, R.; Krzesiński, P.; Balsam, P.; Piotrowicz, E.; Kempa, M.; Lewicka, E.; Główczyńska, R.; Grabowski, M.; Kołtowski, Ł.; Peller, M.; et al. Telemedicine solutions in cardiology: A joint expert opinion by the Information Technology and Telemedicine Committee of the Polish Cardiac Society, the Section of Noninvasive Electrocardiology and Telemedicine of the Polish Cardiac Society, and the Clinical Research Committee of the Polish Academy of Sciences (short version, 2021). Kardiol. Pol. 2021, 79, 227–241. [Google Scholar] [CrossRef]
- Steinberg, J.S.; Varma, N.; Cygankiewicz, I.; Aziz, P.; Balsam, P.; Baranchuk, A.; Cantillon, D.J.; Dilaveris, P.; Dubner, S.J.; El-Sherif, N.; et al. 2017 ISHNE-HRS expert consensus statement on ambulatory ECG and external cardiac monitoring/telemetry. Heart Rhythm 2017, 14, e55–e96. [Google Scholar] [CrossRef] [Green Version]
- Steinhubl, S.R.; Topol, E.J. Moving from Digitalization to Digitization in Cardiovascular Care: Why Is it Important, and What Could it Mean for Patients and Providers? J. Am. Coll. Cardiol. 2015, 66, 1489–1496. [Google Scholar] [CrossRef] [Green Version]
- Maille, B.; Wilkin, M.; Million, M.; Rességuier, N.; Franceschi, F.; Koutbi-Franceschi, L.; Hourdain, J.; Martinez, E.; Zabern, M.; Gardella, C.; et al. Smartwatch Electrocardiogram and Artificial Intelligence for Assessing Cardiac-Rhythm Safety of Drug Therapy in the COVID-19 Pandemic. The QT-logs study. Int. J. Cardiol. 2021, 331, 333–339. [Google Scholar] [CrossRef]
- Smith, S.W.; Walsh, B.; Grauer, K.; Wang, K.; Rapin, J.; Li, J.; Fennell, W.; Taboulet, P. A deep neural network learning algorithm outperforms a conventional algorithm for emergency department electrocardiogram interpretation. J. Electrocardiol. 2019, 52, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, V.D.; Lee, S.-L.; Robertus, J.-L.; Nienaber, C.A.; Trayanova, N.A.; Ernst, S. Artificial intelligence in the diagnosis and management of arrhythmias. Eur. Heart J. 2021, 42, 3904–3916. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall Population | |
|---|---|---|
| Male | 417 (76.37) | |
| Mean Age | 68.58 ± 14.48 | |
| Heart failure symptoms [11] | 0 | 148 (27.11) |
| I | 15 (2.75) | |
| II | 193 (35.35) | |
| III | 142 (26.01) | |
| IV | 48 (8.79) | |
| Myocardial Infarction History | 200 (36.63) | |
| Atrial fibrillation | Paroxysmal | 98 (17.95) |
| Persistent | 24 (4.4) | |
| Permanent | 116 (21.25) | |
| Treatment | ||
| Oral anticoagulation | 301 (55.13) | |
| Beta-blocker | 483 (88.46) | |
| ACE-inhibitor | 302 (55.31) | |
| Angiotensin receptor blocker | 115 (21.06) | |
| Antiarrhythmic drugs | 149 (27.29) | |
| MRA | 256 (46.89) | |
| Diuretic-loop | 316 (57.88) | |
| Diuretic-thiazide | 57 (10.44) | |
| Statins | 361 (66.12) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krzowski, B.; Rokicki, J.; Główczyńska, R.; Fajkis-Zajączkowska, N.; Barczewska, K.; Mąsior, M.; Grabowski, M.; Balsam, P. The Use of Machine Learning Algorithms in the Evaluation of the Effectiveness of Resynchronization Therapy. J. Cardiovasc. Dev. Dis. 2022, 9, 17. https://doi.org/10.3390/jcdd9010017
Krzowski B, Rokicki J, Główczyńska R, Fajkis-Zajączkowska N, Barczewska K, Mąsior M, Grabowski M, Balsam P. The Use of Machine Learning Algorithms in the Evaluation of the Effectiveness of Resynchronization Therapy. Journal of Cardiovascular Development and Disease. 2022; 9(1):17. https://doi.org/10.3390/jcdd9010017
Chicago/Turabian StyleKrzowski, Bartosz, Jakub Rokicki, Renata Główczyńska, Nikola Fajkis-Zajączkowska, Katarzyna Barczewska, Mariusz Mąsior, Marcin Grabowski, and Paweł Balsam. 2022. "The Use of Machine Learning Algorithms in the Evaluation of the Effectiveness of Resynchronization Therapy" Journal of Cardiovascular Development and Disease 9, no. 1: 17. https://doi.org/10.3390/jcdd9010017