1. Introduction
Successful procedural outcomes and long-term durability are the main goals in the interventional treatment of peripheral artery disease (PAD), especially in the femoropopliteal lesions. Endovascular treatment options have substantially improved over the last decades, but there is still room for enhancements, such as improvement in long-term patency and durability of stents in this highly mobile region [
1].
The BioMimics 3D vascular stent system (Veryan Medical Ltd., Horsham, UK) features a new-generation self-expanding nitinol stent, with a 3D helical centreline. It is designed to resist forces such as compression, bending and torsion of the artery, and aims to improve patency rates compared to other bare metal stents by mimicking natural structures [
2,
3]. In the MIMICS randomised controlled trial, the BioMimics 3D stent was superior to straight stents [
4]; the MIMICS 3D all-comers registry aims to assess the safety and performance of the BioMimics 3D stent in a real-world setting, leaving the additional use of drug-coated balloons (DCB) at the discretion of the operators. Data up to 2 years have been reported previously [
2]; we herein report final data out to 3 years.
To further elucidate the effect of DCB combined with stent treatment, a propensity-score-matched analysis was performed.
2. Materials and Methods
2.1. Study Design
The prospective, multi-centre, observational registry has been described in detail previously [
2]. In brief, the registry aimed to evaluate the safety, effectiveness and performance of the BioMimics 3D self-expanding stent system in a real-world population. Patients were enrolled in 23 centres in Europe between September 2016 and June 2018. Follow-up visits were planned at 30 days, and at 12, 24 and 36 months according to centres’ standard of care. This is the final report including 3-year data.
Inclusion criteria were adult patients ≤85 years of age, written informed consent, and symptomatic PAD of femoropopliteal lesions, scheduled for treatment with the BioMimics 3D stent according to the instructions for use. Exclusion criteria were inability to cross the lesion with a wire or balloon catheter, intolerance to antiplatelet and/or anticoagulation therapy, bleeding diathesis, severe hypertension, renal failure, known hypersensitivity to nickel–titanium, comorbidity that limits the life expectancy to less than 12 months, pregnant or breastfeeding patients, or patients that were unwilling to comply with the standard of care procedures and follow-up visit.
An independent clinical events committee was responsible for the systematic review and adjudication of all major adverse events, including death and all potentially device-related adverse events. The registry complies with the current version of the Declaration of Helsinki, relevant data protection regulations, international standards, and regulations applicable to medical device registries. It was approved by the respective ethics committees and each patient provided written informed consent. The registry is listed on
www.clinicaltrials.gov (NCT02900924).
2.2. Study Device and Procedure
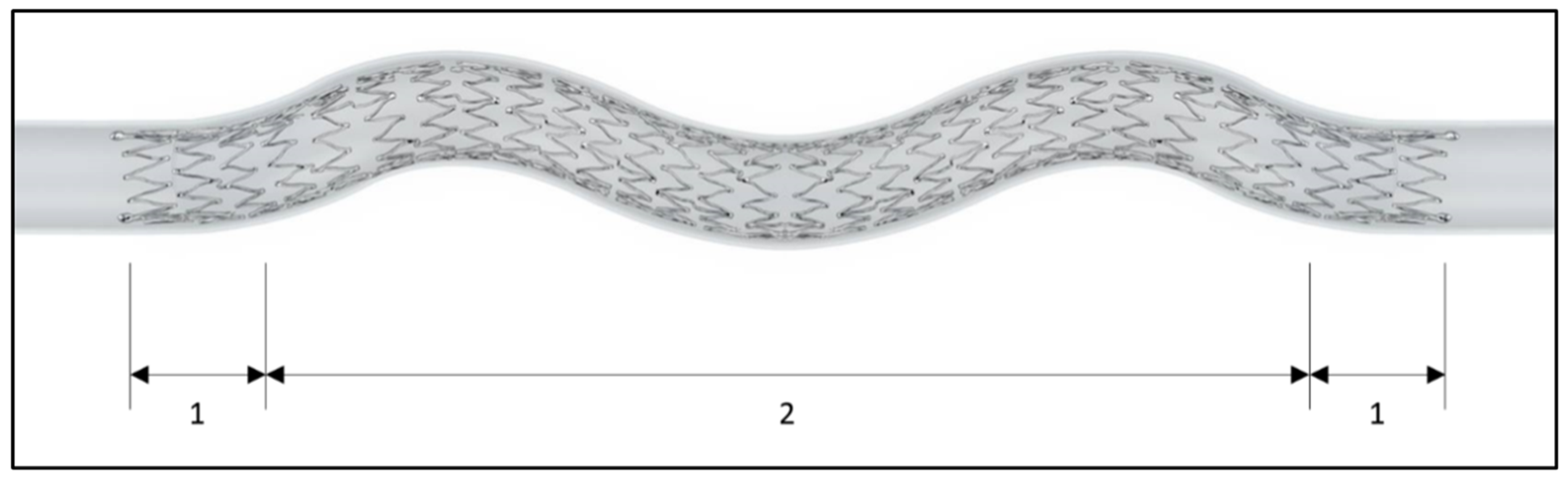
The BioMimics 3D stent system consists of a self-expanding nitinol stent, with three-dimensional helical centreline geometry stored in the nitinol-shape memory (
Figure 1), and a 6F over-the-wire delivery system. The stent is available in diameters of 5, 6, and 7 mm, and lengths of 60 to 150 mm. Additional DCB use was left at the investigators’ discretion. If the physician decided that no treatment with the BioMimics 3D stent was necessary during the procedure, the patient was not considered to be enrolled in the registry.
2.3. Endpoints and Definitions
Endpoints at 36 months are death, target limb amputation, clinically driven target lesion revascularisation (CD-TLR), primary patency (site-assessed, defined as peak systolic velocity ratio <2.4 by duplex ultrasound), and functional and clinical outcomes, including ankle–brachial index (ABI) and Rutherford class.
2.4. Statistical Analysis
The analysis is based on the intention-to-treat population. Continuous variables are expressed as the mean ± standard deviations, categorical variables are expressed as frequencies. All calculations are based on the data available. The p-values were calculated using a Fisher’s exact test for categorical variables, Student’s t-test (means) for continuous variables and log-rank test for comparing Kaplan–Meier estimates. A p-value < 0.05 was considered significant.
A subgroup analysis of lesions treated with DCB was pre-specified in the clinical investigation plan. In addition, a propensity score model was used, that was built using a logistic regression to model the propensity to use a DCB as a function of the covariates, as detailed in
Supplemental Table S1 (
n = 15 variables). Missing data in the covariates were imputed using a single imputation via Monte Carlo Markov Chain methodology. The model fit was assessed via the c-statistic and the propensity scores before and after matching were plotted to examine the overlap between the groups. A 1:1 matched cohort was constructed using the GREEDY match algorithm. The analysis was performed using SAS version 9.4 (SAS institute, Cary, NC, USA).
3. Results
Baseline data have been described previously [
2]. In brief, patients were 70.1 ± 10.0 years old on average, 65.5% were male, 68.0% smokers, and 36.9% had diabetes (
Table 1). Lesions had a reference vessel diameter of 5.5 ± 0.7 mm and were 125.9 ± 91.0 mm long. The total stented length was 131.2 ± 80.1 mm (
Table 2 and
Table 3).
A DCB was used prior to BioMimics 3D stent placement in 23.7% (123/518), and after BioMimics 3D stent deployment, in 26.4% (137/518) of the lesions treated. The three most frequently used DCBs were the Lutonix DCB (34.0%), the In.Pact DCB (32.4%), and the Passeo-18 Lux DCB (14.0%).
At 3 years, 377 patients returned for their follow-up visit; 72 had died (88.6% follow-up compliance). Per Kaplan–Meier analysis, the overall survival was 85.4%, freedom from major amputation 98.5%, freedom from CD-TLR 78.0%, and site-assessed primary patency rate 70.2% (peak systolic velocity ratio was available for 333 patients at 30 days, and for 301, 237 and 222 patients at 12, 24 and 36 months, respectively) (
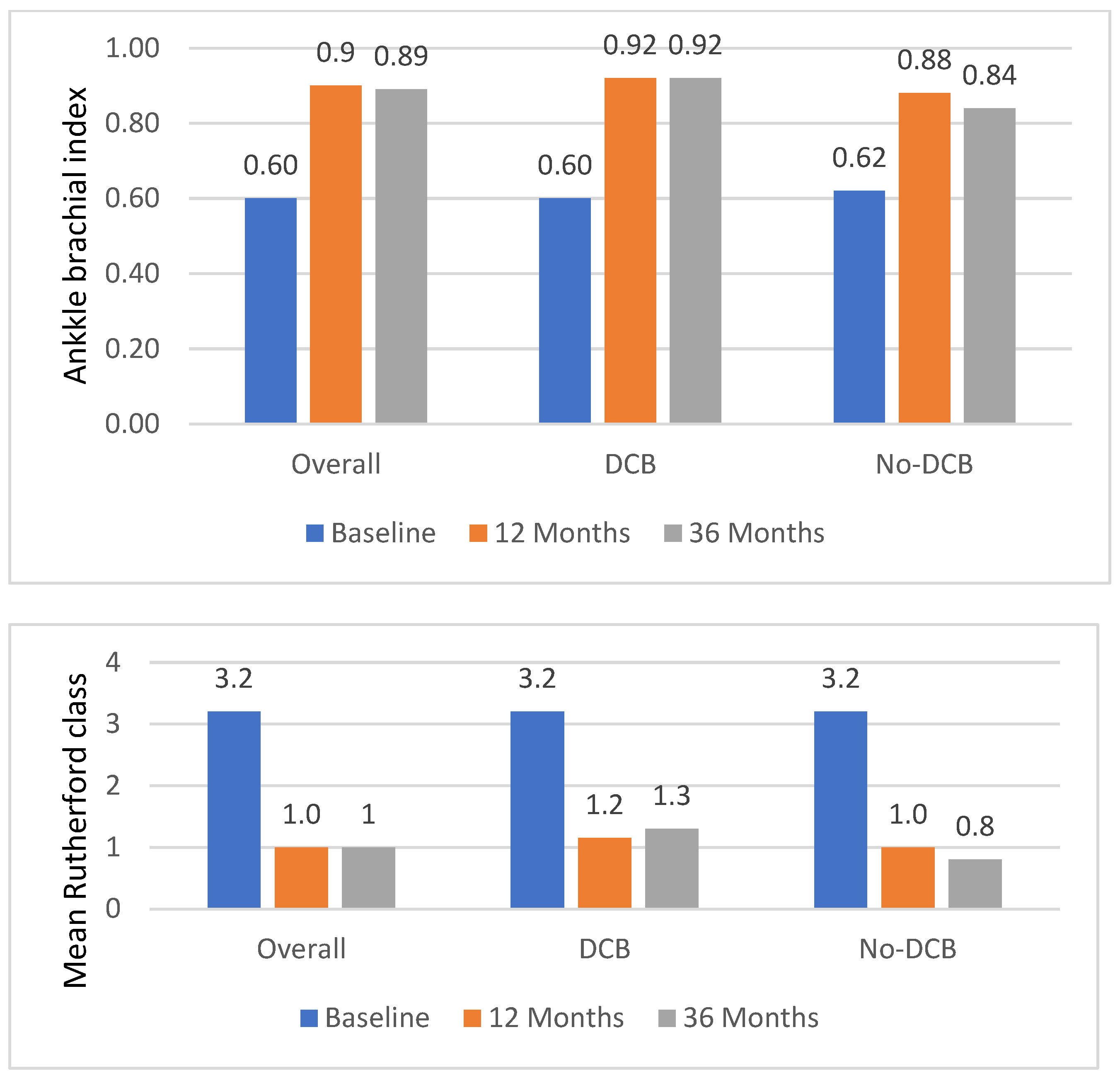
Table 4). Mean Rutherford class had decreased by 2.0 ± 1.3 classes to 1.00 ± 1.05 (
Figure 2).
There was no systematic X-ray assessment to assess stent fractures; nevertheless, four stent fractures were reported (one of which was not confirmed by the clinical events committee).
Propensity-Matched Cohorts
The propensity-matched cohorts consisted of 195 patients each. Both cohorts were well matched, as shown in
Supplemental Figure S1, and
Table 1 and
Table 2, except for a lower calcification grade rate (grade 4) in the DCB group (7.9% vs. 19.3%,
p = 0.001).
The total stent length was 128.3 ± 80.9 mm in the DCB group vs. 132.2 ± 79.2 mm in the no-DCB group,
p = 0.262 for lesions lengths of 123.6 ± 93.7 mm and 124.7 ± 86.6 mm,
p = 0.402, respectively (
Table 2 and
Table 3). In the unmatched cohort, the total stented length was 135.0 ± 85.5 mm vs. 127.7 ± 74.6 mm,
p = 0.872, and the lesion length was 137.6 ± 99.8 mm vs. 115.0 ± 80.7 mm,
p = 0.068, respectively. Spot-stenting, which we defined as stented length <80% of lesion length, was performed in 15.9% of lesions in the propensity-matched DCB cohort and 11.3% in the no-DCB cohort,
p = 0.237, and for 15.3% vs. 11.1%,
p = 0.239, in the unmatched cohort.
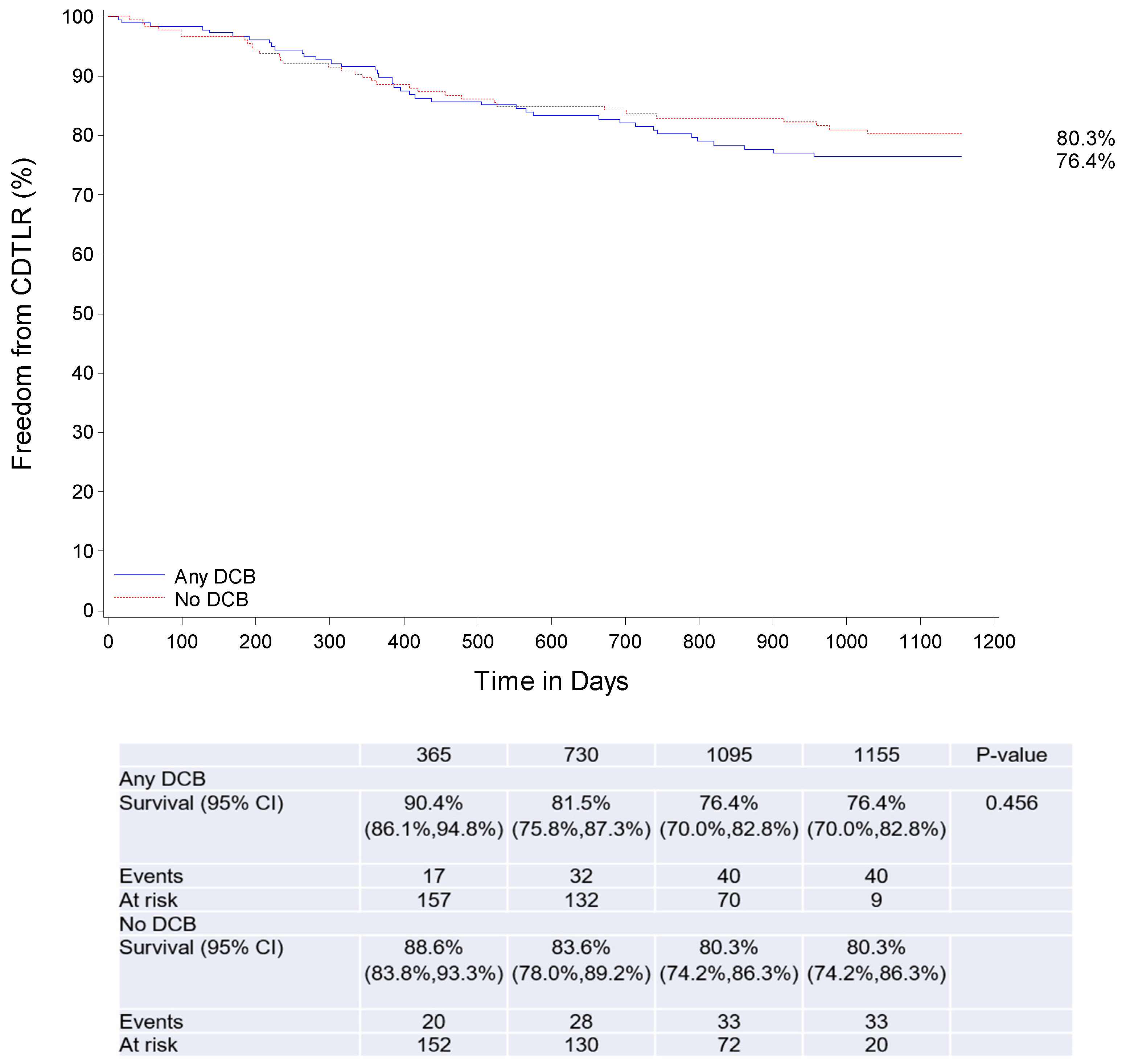
At 3 years, 153 patients in the DCB and 145 patients in the no-DCB group completed their follow-up visit, and 22 and 26 patients had died, respectively. There was no statistically significant difference in clinical outcomes. Three-year survival (day 1095) was 87.9% and 85.1% in the DCB and no-DCB propensity-matched cohorts, freedom from major amputation was 99.4% and 97.2%, CD-TLR was 76.4%, and 80.3% and primary patency 68.5% and 74.4%, respectively (
Table 4,
Figure 3).
As detailed in
Figure 2, the mean baseline Rutherford class was identical amongst the groups (3.2 ± 0.8 in the DCB group and 3.2 ± 1.2 in the no-DCB group), whereas at follow-up, the mean Rutherford class was significantly higher in the DCB group (1.3 ± 1.1 vs. 0.8 ± 1.0,
p = 0.0001, at 3 years).
A summary of the unmatched DCB and no-DCB cohort data is provided in
Supplemental Tables S2–S5, and a comparison of outcomes in patients that received a DCB before vs. after stent implantation is provided in
Supplemental Table S6.
4. Discussion
The real-world MIMICS 3D registry showed that treating femoropopliteal lesions using the BioMimics 3D stent results in good 3-year outcomes, whether the stent is used in combination with a DCB or not.
4.1. 3-Year Outcomes in the Overall Cohort
BioMimics 3D is a next-generation stent with a 3D helical centreline that imparts a gentle helical shape to the artery, which allows the stent to shorten, elongate and twist with the artery. Furthermore, the helical geometry induces swirling flow that increases wall shear stress, which has been shown to reduce intimal hyperplasia [
5,
6]. Moreover, the 3D helical geometry improves the stent’s biomechanical compatibility which reduces vascular injury and the risk of stent fracture, both of which can be the consequence of using traditional straight stents in the mobile femoropopliteal arteries [
7]. The stent demonstrated statistically significant better primary patency at 2 years compared to straight stents, and numerically higher freedom from TLR in a randomised controlled trial, where the curves diverged beyond 12 months in favour of the BioMimics 3D stent [
4].
Likewise, the MIMICS 3D registry showed good outcomes in terms of TLR. Putting the data into perspective, whilst acknowledging that at this stage there are no direct RCTs comparing BioMimics 3D to drug-based devices, the MIMICS 3D TLR rate is similar to that seen in DES and DCB trials, whether in the overall, DCB or no-DCB cohort. In the overall cohort, with a mean lesion length of 125.9 ± 91.0 mm, freedom from CD-TLR at 3 years was slightly lower (78.0%) compared to 87.2% for the Zilver PTX DES (Cook Medical, Bloomington, Indiana) in the Zilver PTX randomized controlled trial, and 85.3% in the MAJESTIC trial using the Eluvia DES (Boston Scientific, Marlborough, MA), but in those trials, lesions were only approximately half as long as those in MIMICS 3D (lesion lengths of 66.4 mm and 70.8 mm, respectively) [
8,
9]. The Real-PTX randomised controlled trial had slightly longer lesions with 155.5 mm, and a lower freedom from TLR (68.9% for the Zilver PTX stent and 71.3% for DCBs) [
10]. The In.Pact Global DCB registry had a similar lesion length (120.9 mm, provisional stenting in 21.2%), and reported 76.9% freedom from TLR at 3 years [
11].
4.2. BioMimics 3D in Combination with DCB
Nearly half of the lesions in MIMICS 3D were additionally treated with a DCB. This, along with the very good outcomes, warrants further investigations of the effect of additional DCB therapy.
There are several reasons to consider the combination of bare metal stents and DCB therapy. First, stenting is used as bailout therapy after DCB therapy. This is required in around one quarter of procedures increasing with increased lesion length or when occlusions are treated [
10,
11,
12,
13,
14,
15]. In the IN.PACT Global study, provisional stenting was performed in 36.4% of cases in lesions ≥ 150 mm [
13].
Second, the combination of stent plus DCB may be used in the context of spot-stenting. Spot-stenting has the advantage of limiting axial stiffness of the artery, possibly preventing kinking and occlusion, as the vessel (in contrast to DES treatment) is only stented where needed, avoiding “full-metal jackets” [
16,
17]. With the limitation that we arbitrarily determined spot-stenting as the total stented length ≤ 80% of lesion length, 15% of DCB lesions were categorised as having been treated with spot-stenting.
Third, the combination of a stent with a DCB is attractive as it can address recoil post-DCB and reduce restenosis through the addition of a drug, without the irritation of the drug-releasing excipients. In our series, more than half of the lesions were treated with primary stent placement followed by DCB treatment, predominantly to treat complex lesions, combining the advantages of a stent and DCB. This may be particularly useful in long lesions [
18].
If DCB therapy is combined with a stent, it makes sense to use a stent with good long-term outcomes that could extend the period of high patency beyond the initial 12 months when drug-eluting devices might lose their effectiveness [
13]. BioMimics 3D might be particularly useful in this scenario as it has prolonged clinical benefits due to its helical centreline, mimicking natural arterial geometry and inducing swirling flow as discussed above. This theoretical advantage has been tested in preclinical bench tests, but also in vivo, when BioMimics 3D demonstrated superior patency rates compared to straight nitinol stents [
4]. Moreover, the transition zones which have reduced radial force at the stent edges might reduce edge reactions in the highly mobile and dynamic femoropopliteal region [
19]. The purpose of the reduction in radial force is to mitigate a step change in profile at the stent ends, which could otherwise lead to a flow disturbance.
Notably, in our series, CD-TLR and patency rates were good in all subgroups, without a significant difference between DCB and non-DCB-treated lesions, whether in the unmatched or propensity-matched analysis. As for the overall cohort, outcomes were comparable to contemporary DES and DCB therapies. A randomised controlled trial would be desired to allow a direct comparison between the different treatment modalities.
4.3. Limitations
Potential limitations include those inherent to observational real-world studies. MIMICS 3D is not randomised, hampering the comparison to other devices and leaving room for bias. Inherent to a registry, patients were treated according to the standard of care. This means that the use of a DCB was left to the discretion of the operator. Furthermore, no routine imaging follow-up was performed, which might have resulted in an underreporting of stent fractures or restenosis. No imaging core laboratory was used, therefore the description of lesion length and patency was left to the study centre. Furthermore, the cut-off value for spot-stenting was arbitrarily selected. Lastly, while the propensity matching aimed to reduce the impact of baseline characteristics, results might still be biased because propensity matching is not as effective as randomisation.
5. Conclusions
The MIMICS 3D registry showed satisfying outcomes in patients treated with the helical centreline BioMimics 3D nitinol stent, which are comparable to those of drug-eluting stents. There was no difference in terms of CD-TLR, whether the stent was used alone or in combination with a DCB. This means that suboptimal results after DCB treatment should not be accepted as the combination of DCB plus BioMimics 3D results in good outcomes, and that DCB, in addition to BioMimics 3D stent treatment, may be an alternative to DES therapy when drug treatment is deemed necessary. Ultimately, a randomised controlled trial is needed to allow for a comparison between the different treatment modalities.
Supplementary Materials
The following supporting information can be downloaded at:
https://www.mdpi.com/article/10.3390/jcdd10030126/s1, Table S1: Logistic regression results for a drug-coated balloon vs. no drug-coated balloon (c-statistic = 0.68); Figure S1: Propensity score distribution in the full dataset prior to matching (left panel) and in the matched cohort (right panel); Table S2: Baseline characteristics (unmatched cohorts); Table S3: Lesion characteristics (unmatched cohort); Table S4: Procedural characteristics (unmatched cohorts); Table S5: Three-year clinical outcomes per Kaplan–Meier estimate (unmatched cohorts); Table S6: Three-year clinical outcomes per Kaplan-Meier estimates in patients that received DCB therapy before and after stent placement.
Author Contributions
Conceptualization, M.L., M.P. and P.G.; methodology, M.L. and M.P.; validation, M.P. and P.G.; investigation, M.P., T.Z., C.R., K.D., K.H., V.S., G.T. and M.L.; resources, M.P., T.Z., C.R., K.D., K.H., V.S., G.T. and M.L.; writing—original draft preparation, M.P.; writing—review and editing, T.Z., C.R., K.D., K.H., V.S., G.T., P.G. and M.L.; visualization, M.P.; supervision, M.L. and M.P.; project administration, M.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Veryan Medical Ltd.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Ethics Committee of the Westphalia-Lippe Medical Council and the Westphalian Wilhelms-University (2016-275-f-S, 09 September 2016), LÄK Thuringia Ethics Committee (56508/2016/126, 28 September 2016); Albert-Ludwig University Freiburg Ethics Committee (479/2016, 29 September 2016); Ethics Committee of the Faculty of Medicine of the University of Leipzig; Ethics Committee of the Saxony State Medical Council (158-17-lk, 27 April 2017); Ethics Committee at the Hessen State Medical Council (MC-201/2016, 29 September 2016); Ethics Committee of the Medical Association of Hamburg (MC-365/16, 24 January 2017); Medical Association of Lower Saxony (Grae/2019/2016, 15 November 2016), Ethics Committee of the Faculty of Medicine of the University of Duisburg-Essen (17-7466-BO, 30 March 2017); ZNA Medical Ethics Committee; Ethics Committee at the OLV (Onze Lieve Vrouwe) (4840, 02 December 2016); Local Ethics Committee AZ Sint Blasius (2016/079, 21 November 2016); Local Feasibility Committee Rijnstate; Central Ethics Review Board Lund (2017-0969, 12 October 2017); Ethics Committee at the Eberhard-Karls-University and the University of Tübingen (730/2017/BO2, 26 January 2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data associated with the paper are not publicly available, but are available from the corresponding author on reasonable request.
Acknowledgments
We thank Beatrix Doerr, consultant medical writer, and Helen Parise, consultant statistician, for their help in preparing this manuscript, reimbursed by Veryan Medical Ltd.
Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: all authors, except Peter Gaines, received study fees paid to their institution. Michael Piorkowski has received speaker honoraria from Veryan Medical Ltd.; Thomas Zeller reports consulting fees, honoraria and travel grants from Veryan Medial Ltd.; Christos Rammos has received research funding from Veryan Medical Ltd., Biotronik and Medalliance, consulting fees from Boston Scientific and BD Bard, honoraria from Shockwave, BD Bard and Biotronik, and is part of the Speaker Working Group Aorta of the DGK; Peter Gaines serves as a consultant for Veryan Medical Ltd.; Michael Lichtenberg has received speaker honoraria from Veryan Medical Ltd. and also serves as a consultant for Veryan Medical Ltd. The funder was involved in the design of the study, in the collection, analyses or interpretation of data, and reimbursed the costs of the medical writer and the publishing charges. The sponsor was not involved in the final decision to publish.
References
- Aboyans, V.; Ricco, J.B.; Bartelink, M.L.; Björck, M.; Brodmann, M.; Cohner, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [PubMed] [Green Version]
- Lichtenberg, M.; Zeller, T.; Gaines, P.; Piorkowski, M. BioMimics 3D vascular stent system for femoropopliteal interventions. Vasa 2022, 51, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, T.M.; Zeller, T.; Nakamura, M.; Gaines, P.A. Treatment of Femoropopliteal Lesions With the BioMimics 3D Vascular Stent System: Two-Year Results From the MIMICS-2 Trial. J. Endovasc. Ther. 2021, 28, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Zeller, T.; Gaines, P.A.; Ansel, G.M.; Caro, C.G. Helical Centerline Stent Improves Patency: Two-Year Results From the Randomized Mimics Trial. Circ. Cardiovasc. Interv. 2016, 9, e002930. [Google Scholar] [CrossRef] [PubMed]
- Caro, C.G.; Seneviratne, A.; Heraty, K.B.; Monaco, C.; Burke, M.G.; Krams, R.; Chang, C.C.; Coppola, G.; Gilson, P. Intimal hyperplasia following implantation of helical-centreline and straight-centreline stents in common carotid arteries in healthy pigs: Influence of intraluminal flow. J. R. Soc. Interface 2013, 10, 20130578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, T.M.; Zeller, T.; Nakamura, M.; Caro, C.G.; Lichtenberg, M. Swirling Flow and Wall Shear: Evaluating the BioMimics 3D Helical Centerline Stent for the Femoropopliteal Segment. Int. J. Vasc. Med. 2018, 2018, 9795174. [Google Scholar] [CrossRef] [PubMed]
- Rits, J.; van Herwaarden, J.A.; Jahrome, A.K.; Krievins, D.; Moll, F.L. The incidence of arterial stent fractures with exclusion of coronary, aortic, and non-arterial settings. Eur. J. Vasc. Endovasc. Surg. 2008, 36, 339–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dake, M.D.; Ansel, G.M.; Jaff, M.R.; Ohki, T.; Saxon, R.R.; Smouse, H.B.; Machan, L.S.; Snyder, S.A.; O’leary, E.E.; Ragheb, A.O.; et al. Durable Clinical Effectiveness With Paclitaxel-Eluting Stents in the Femoropopliteal Artery: 5-Year Results of the Zilver PTX Randomized Trial. Circulation 2016, 133, 1472–1483. [Google Scholar] [CrossRef] [PubMed]
- Müller-Hülsbeck, S.; Keirse, K.; Zeller, T.; Schroë, H.; Diaz-Cartelle, J. Long-Term Results from the MAJESTIC Trial of the Eluvia Paclitaxel-Eluting Stent for Femoropopliteal Treatment: 3-Year Follow-up. Cardiovasc. Interv. Radiol. 2017, 40, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Bausback, Y.; Wittig, T.; Schmidt, A.; Zeller, T.; Bosiers, M.; Peeters, P.; Brucks, S.; Lottes, A.E.; Scheinert, D.; Steiner, S. Drug-Eluting Stent Versus Drug-Coated Balloon Revascularization in Patients With Femoropopliteal Arterial Disease. J. Am. Coll. Cardiol. 2019, 73, 667–679. [Google Scholar] [CrossRef] [PubMed]
- Torsello, G.; Stavroulakis, K.; Brodmann, M.; Micari, A.; Tepe, G.; Veroux, P.; Benko, A.; Choi, D.; Vermassen, F.E.G.; Jaff, M.R.; et al. Three-Year Sustained Clinical Efficacy of Drug-Coated Balloon Angioplasty in a Real-World Femoropopliteal Cohort. J. Endovasc. Ther. 2020, 27, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Shishehbor, M.H.; Schneider, P.A.; Zeller, T.; Razavi, M.K.; Laird, J.R.; Wang, H.; Tieché, C.; Parikh, S.A.; Iida, O.; Jaff, M.R. Total IN.PACT drug-coated balloon initiative reporting pooled imaging and propensity-matched cohorts. J. Vasc. Surg. 2019, 70, 1177–1191.e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodmann, M.; Lansink, W.; Guetl, K.; Micari, A.; Menk, J.; Zeller, T. Long-Term Outcomes of the 150 mm Drug-Coated Balloon Cohort from the IN.PACT Global Study. Cardiovasc. Interv. Radiol. 2022, 45, 1276–1287. [Google Scholar] [CrossRef] [PubMed]
- Thieme, M.; Von Bilderling, P.; Paetzel, C.; Karnabatidis, D.; Perez Delgado, J.; Lichtenberg, M.; Lutonix Global SFA Registry Investigators. The 24-Month Results of the Lutonix Global SFA Registry: Worldwide Experience with Lutonix Drug-Coated Balloon. JACC Cardiovasc. Interv. 2017, 10, 1682–1690. [Google Scholar] [CrossRef] [PubMed]
- Widder, J.D.; Cortese, B.; Levesque, S.; Berliner, D.; Eccleshall, S.; Graf, K.; Doutrelant, L.; Ahmed, J.; Bressollette, E.; Zavalloni, D.; et al. Coronary artery treatment with a urea-based paclitaxel-coated balloon: The European-wide FALCON all-comers DCB Registry (FALCON Registry). EuroIntervention 2019, 15, e382–e388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deloose, K.; Bosiers, M.; Peeters, P.; Verbist, J.; Maene, L.; Beelen, R.; Keirse, K.; Hendriks, J.; Lauwers, P.; Wauters, J.; et al. Combining the Passeo-18 Lux Drug-Coated Balloon and the Pulsar-18 Bare Metal Stent: 12- and 24-Month Outcomes of the BIOLUX 4EVER Investigator-Initiated Trial. J. Endovasc. Ther. 2020, 27, 936–945. [Google Scholar] [CrossRef]
- Lichtenberg, M.; Breuckmann, F.; Kramer, V.; Betge, S.; Sixt, S.; Hailer, B.; Nikol, S.; Arjumand, J.; Wittenberg, G.; Teßarek, J.; et al. Effectiveness of the Pulsar-18 self-expanding stent with optional drug-coated balloon angioplasty in the treatment of femoropopliteal lesions—The BIOFLEX PEACE All-Comers Registry. Vasa 2019, 48, 425–432. [Google Scholar] [CrossRef]
- Schmidt, A.; Piorkowski, M.; Görner, H.; Steiner, S.; Bausback, Y.; Scheinert, S.; Banning-Eichenseer, U.; Staab, H.; Branzan, D.; Varcoe, R.L.; et al. Drug-Coated Balloons for Complex Femoropopliteal Lesions: 2-Year Results of a Real-World Registry. JACC Cardiovasc. Interv. 2016, 9, 715–724. [Google Scholar] [CrossRef]
- Ansari, F.; Pack, L.K.; Brooks, S.S.; Morrison, T.M. Design considerations for studies of the biomechanical environment of the femoropopliteal arteries. J. Vasc. Surg. 2013, 58, 804–813. [Google Scholar] [CrossRef] [Green Version]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 



{kind=link}
{kind=link}
{kind=link}