The Neonatal Screening Program in Brazil, Focus on Sickle Cell Disease (SCD)

Abstract
:1. Background
2. The Neonatal Screening Program
3. Resolutions and Guidelines from the Brazilian Ministry of Health
4. The Sickle Cell Disease Network of Care Inside SUS: From Neonatal Screening to Follow-Up in Reference Centers
5. Challenges for the Full Implementation of the SCD Care Network
Author Contributions
Funding
Conflicts of Interest
References
- Brasil, IBGE. Demographic Census 2010. Available online: https://www.ibge.gov.br/ (accessed on 17 September 2018).
- Brasil, Ministério da Saúde. Portaria GM/MS nº22 de 15/01/1992—triagem para fenilcetonúria e hipotireoidismo Congênito. Diário Oficial da União, 15 January 1992. [Google Scholar]
- Paixão, M.C.; Cunha Ferraz, M.H.; Januário, J.N.; Viana, M.B.; Lima, J.M. Reliability of isoelectrofocusing for the detection of Hb S, Hb C, and HB D in a pioneering population-based program of newborn screening in Brazil. Hemoglobin 2001, 25, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Brasil, Ministério da saúde. Portaria GM/MS nº 822 de 06 de junho de 2001—Programa de triagem neonatal no Brasil. Diário Oficial da União, 6 June 2001. [Google Scholar]
- Carvalho, T.M.; Santos, H.P.; Santos, I.C.G.P.; Vargas, P.R.; Pedrosa, J. Newborn screening: A national public health programme in Brazil. J. Inherit. Metab. Dis. 2007, 30, 615. [Google Scholar] [CrossRef] [PubMed]
- Brasil, Ministério da saúde. Portaria SAS/MS Nº 55 de 29 de janeiro de 2010—Protocolo Clínico e Diretrizes Terapêuticas para Doença Falciforme”. Diário Oficial da União, 29 January 2010. [Google Scholar]
- Brasil, Ministério da saúde. Lei nº 8.080, de 19 de setembro de 1990, criação do SUS—Sistema Único de Saúde. Diário Oficial da União, 19 September 1990. [Google Scholar]
- Seta, M.H.; Oliveira, C.V.D.S.; Pepe, V.L.E. Health protection in Brazil: the National Sanitary Surveillance System. Cien Saude Colet 2017, 22, 3225–3234. [Google Scholar] [CrossRef] [PubMed]
- Ramalho, A.S.; Magna, L.A.; Paiva-Silva, R.B. A portaria nº 822/01 do Ministério da Saúde e as peculiaridades das hemoglobinopatias em saúde pública no Brasil. Cad. Saúde Pública 2003, 19, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Vichinsky, E. Sickle cell disease and thalassemia: disorders of globin production. (2008) pages 3-5, in Special anniversary brochure, American Society of Hematology: 50 Years in Hematology: Research That Revolutionized Patient Care. Available online: http://www.hematology.org/About/History/50-Years/1533.aspx (accessed on 13 January 2019).
- Bassett, M.T. Beyond Berets: The Black Panthers as Health Activists. Am. J. Public Health 2016, 106, 1741–1743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brasil, Ministério da saúde. Portaria de nº 1391 de 16 de agosto de 2005—Diretrizes para a Política Nacional de Atenção Integral às Pessoas com Doença Falciforme e outras Hemoglobinopatias. Diário Oficial da União, 16 August 2005. [Google Scholar]
- Cançado, R.D.; Jesus, J.A. A doença falciforme no Brasil. Rev. Bras. Hematol. Hemoter. 2007, 29, 204–206. [Google Scholar] [CrossRef]
- Lobo, C.L.; Pinto, J.F.; Nascimento, E.M.; Moura, P.G.; Cardoso, G.P.; Hankins, J.S. The effect of hydroxcarbamide therapy on survival of children with sickle cell disease. Br. J. Haematol. 2013, 161, 852–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, A.P.; Januário, J.N.; Cangussu, C.B.; Macedo, D.L.; Viana, M.B. Mortality of children with sickle cell disease: A population study. J. Pediatr. (Rio J). 2010, 86, 279–284. [Google Scholar] [CrossRef]
- Lobo, C.L.C.; Nascimento, E.M.D.; Jesus, L.J.C.; Freitas, T.G.; Lugon, J.R.; Ballas, S.K. Mortality in children, adolescents and adults with sickle cell anemia in Rio de Janeiro, Brazil. Rev. Bras. Hematol. Hemoter. 2018, 40, 37–42. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
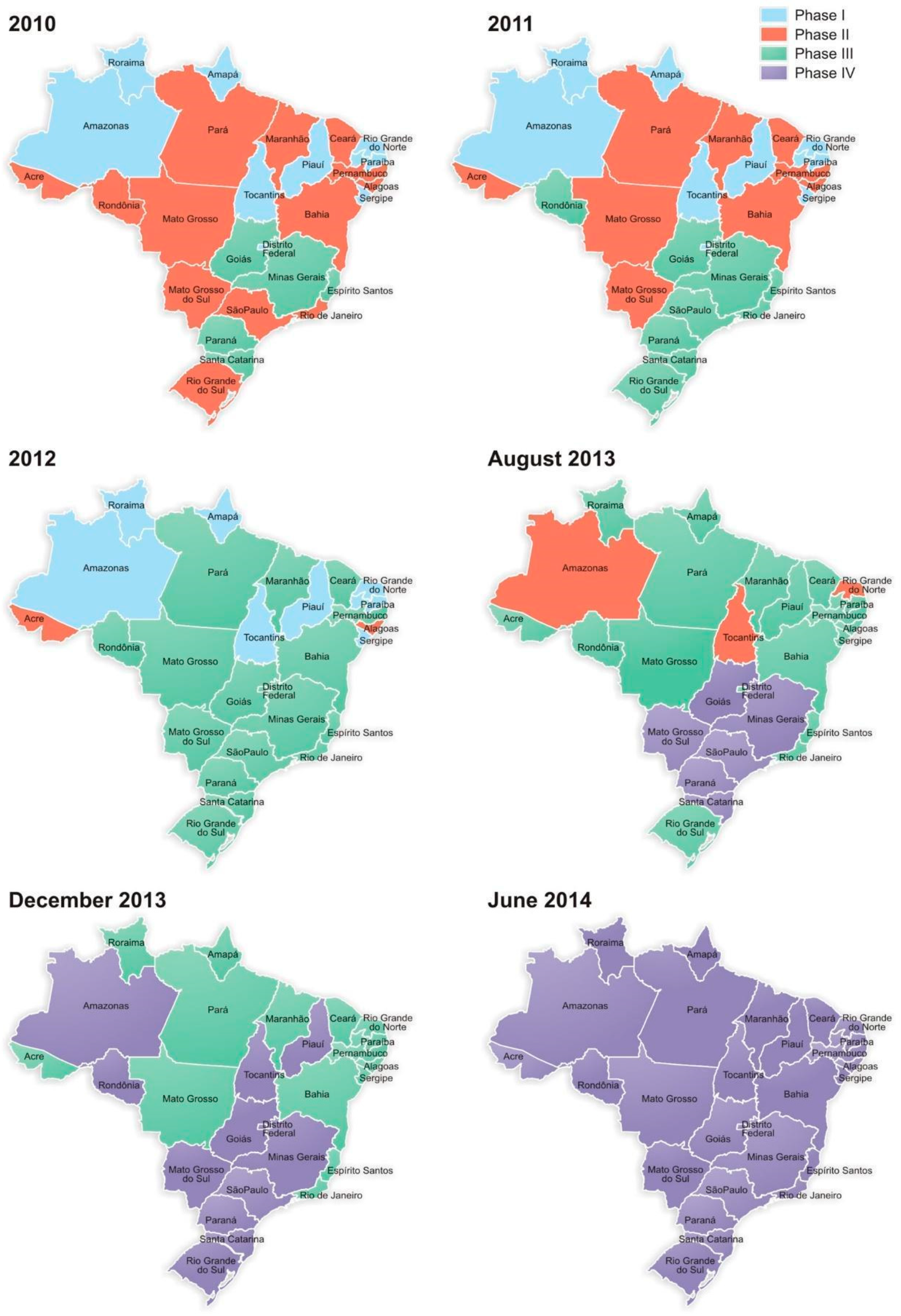
| Phases | Diseases | Year of National Implementation |
|---|---|---|
| Phase I | Phenylketonuria and congenital hypothyroidism | 2006 |
| Phase II | Sickle cell disease and other hemoglobinopathies | 2013 |
| Phase III | Cystic fibrosis | 2013 |
| Phase IV | Congenital adrenal hyperplasia and biotinidase deficiency | 2014 |
| Regions of Brazil | State | Incidence/Live Births | Incidence of the S Mutation |
|---|---|---|---|
| Northeast | Maranhão | 1:1400 | 1:23 |
| Pernambuco | 1:1400 | 1:23 | |
| Bahia | 1:650 | 1:17 | |
| Center-west | Goiás | 1:1400 | 1:28 |
| Mato Grosso do Sul | 1:8300 | 1:70 | |
| Southeast | Minas Gerais | 1:1400 | 1:30 |
| Espírito Santo | 1:1800 | 1:28 | |
| Rio de Janeiro | 1:1200 | 1:21 | |
| São Paulo | 1:4000 | 1:35 | |
| South | Paraná | 1:13,000 | 1:65 |
| Santa Catarina | 1:13,000 | 1:65 | |
| Rio Grande do Sul | 1:13,500 | 1:65 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Pinto, A.C.; Alencar de Queiroz, M.C.; Antoniazzo Zamaro, P.J.; Arruda, M.; Pimentel dos Santos, H. The Neonatal Screening Program in Brazil, Focus on Sickle Cell Disease (SCD). Int. J. Neonatal Screen. 2019, 5, 11. https://doi.org/10.3390/ijns5010011
Silva-Pinto AC, Alencar de Queiroz MC, Antoniazzo Zamaro PJ, Arruda M, Pimentel dos Santos H. The Neonatal Screening Program in Brazil, Focus on Sickle Cell Disease (SCD). International Journal of Neonatal Screening. 2019; 5(1):11. https://doi.org/10.3390/ijns5010011
Chicago/Turabian StyleSilva-Pinto, Ana C., Maria Cândida Alencar de Queiroz, Paula Juliana Antoniazzo Zamaro, Miranete Arruda, and Helena Pimentel dos Santos. 2019. "The Neonatal Screening Program in Brazil, Focus on Sickle Cell Disease (SCD)" International Journal of Neonatal Screening 5, no. 1: 11. https://doi.org/10.3390/ijns5010011