
The Complex Interplay between the Gut Microbiome and Osteoarthritis: A Systematic Review on Potential Correlations and Therapeutic Approaches
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategies
2.3. Selection Process
2.4. Data Collection Process and Synthesis Methods
2.5. Risk of Bias Assessment
3. Results
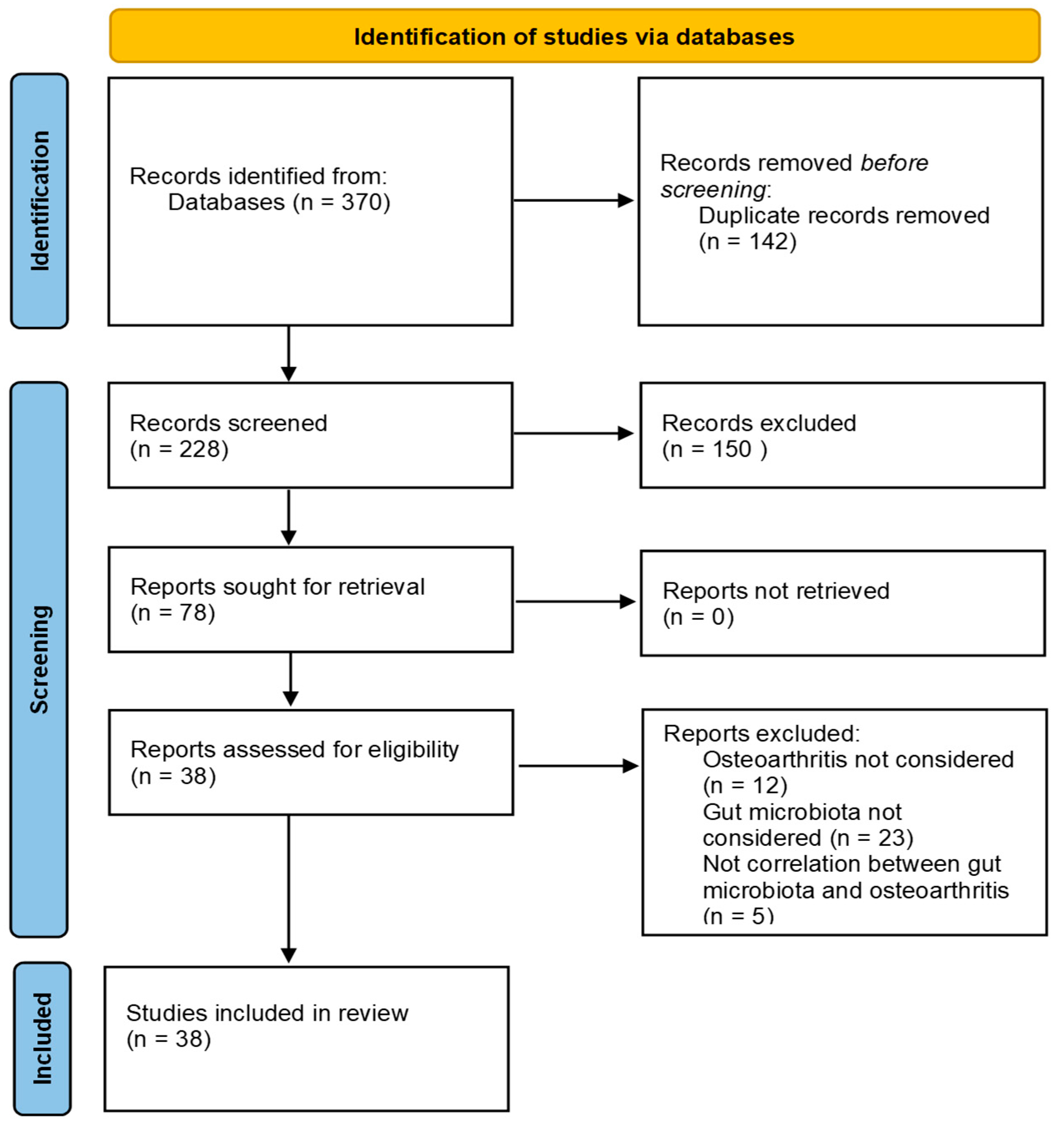
3.1. Study Selection
3.2. General Characteristics of In Vivo Studies
In Vivo Studies Results
3.3. General Characteristics of Clinical Studies
Clinical Studies Results
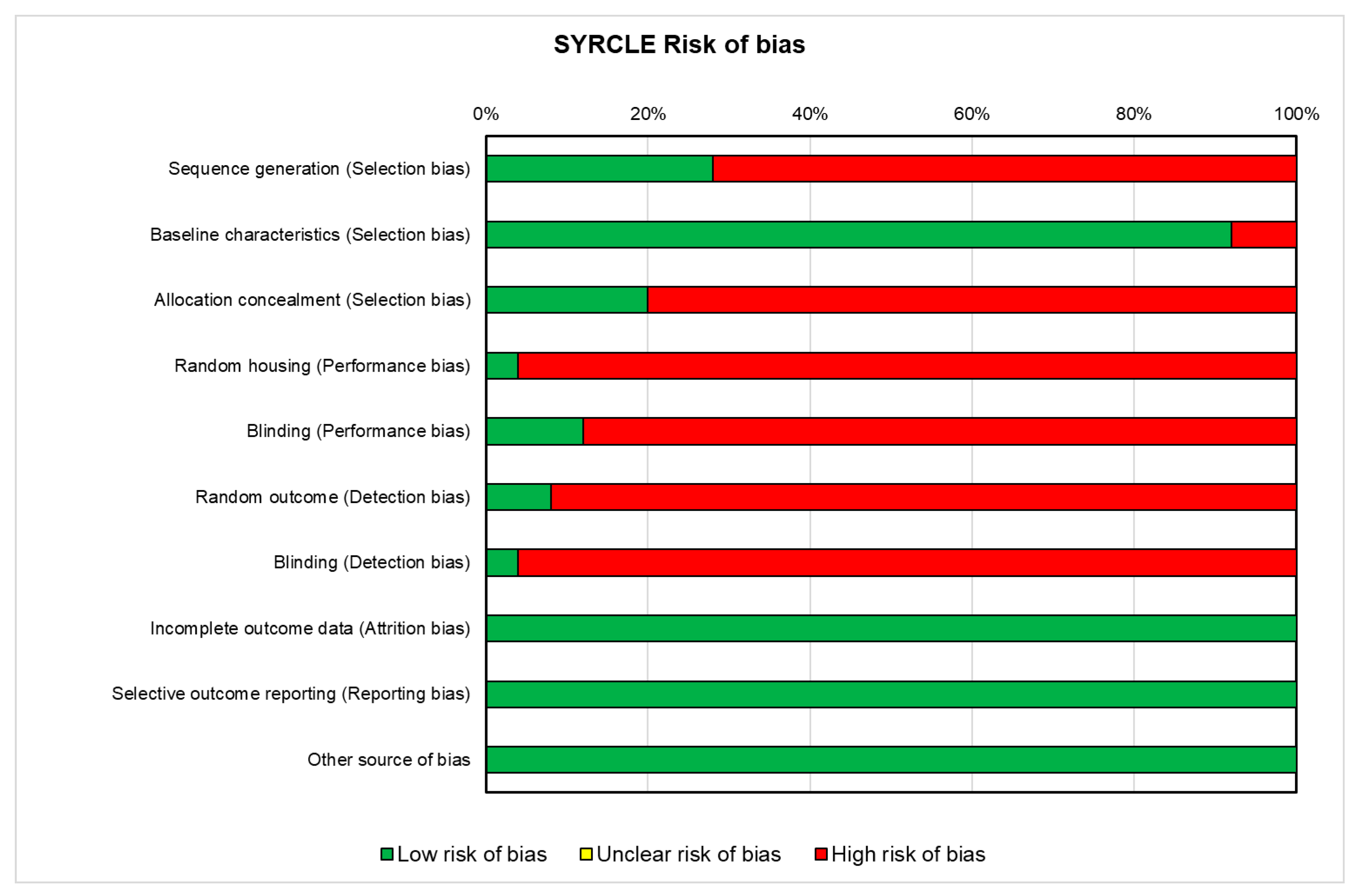
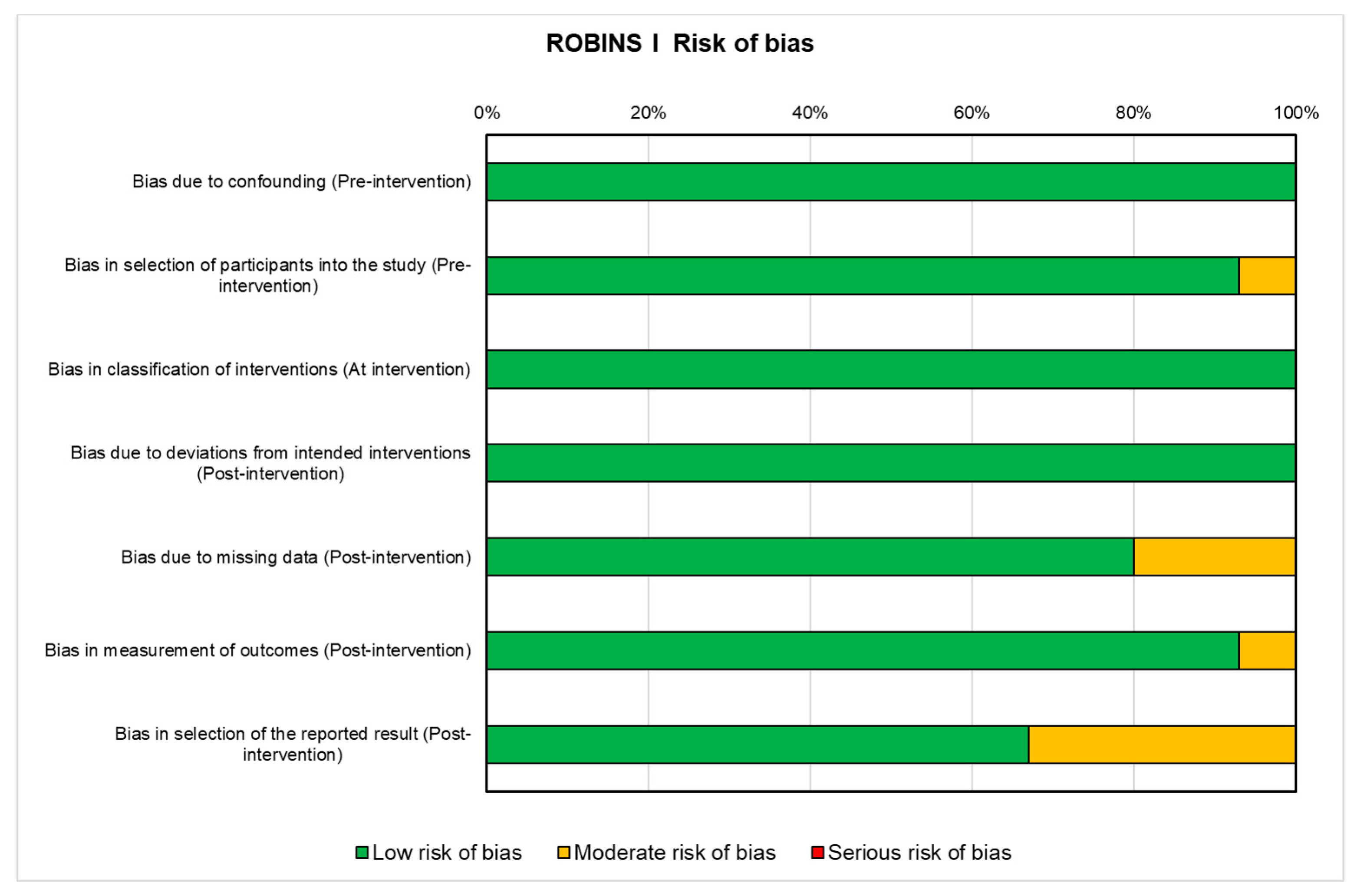
3.4. Risk of Bias Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef]
- Veronesi, F.; Berni, M.; Marchiori, G.; Cassiolas, G.; Muttini, A.; Barboni, B.; Martini, L.; Fini, M.; Lopomo, N.F.; Marcacci, M.; et al. Evaluation of cartilage biomechanics and knee joint microenvironment after different cell-based treatments in a sheep model of early osteoarthritis. Int. Orthop. 2021, 45, 427–435. [Google Scholar] [CrossRef]
- Kapoor, M.; Martel-Pelletier, J.; Lajeunesse, D.; Pelletier, J.P.; Fahmi, H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nat. Rev. Rheumatol. 2011, 7, 33–42. [Google Scholar] [CrossRef]
- Veronesi, F.; Della Bella, E.; Cepollaro, S.; Brogini, S.; Martini, L.; Fini, M. Novel therapeutic targets in osteoarthritis: Narrative review on knock-out genes involved in disease development in mouse animal models. Cytotherapy 2016, 18, 593–612. [Google Scholar] [CrossRef]
- Woodell-May, J.E.; Sommerfeld, S.D. Role of Inflammation and the Immune System in the Progression of Osteoarthritis. J. Orthop. Res. 2020, 38, 253–257. [Google Scholar] [CrossRef]
- Veronesi, F.; Salamanna, F.; Martini, L.; Fini, M. Naturally Occurring Osteoarthritis Features and Treatments: Systematic Review on the Aged Guinea Pig Model. Int. J. Mol. Sci. 2022, 23, 7309. [Google Scholar] [CrossRef]
- Allen, K.D.; Thoma, L.M.; Golightly, Y.M. Epidemiology of osteoarthritis. Osteoarthr. Cartil. 2022, 30, 184–195. [Google Scholar] [CrossRef]
- Glyn-Jones, S.; Palmer, A.J.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteoarthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef]
- Abramoff, B.; Caldera, F.E. Osteoarthritis: Pathology, Diagnosis, and Treatment Options. Med. Clin. N. Am. 2020, 104, 293–311. [Google Scholar] [CrossRef]
- Dieppe, P.A.; Lohmander, L.S. Pathogenesis and management of pain in osteoarthritis. Lancet 2005, 365, 965–973. [Google Scholar] [CrossRef]
- Liu, X.; Robbins, S.; Wang, X.; Virk, S.; Schuck, K.; Deveza, L.A.; Oo, W.M.; Carmichael, K.; Antony, B.; Eckstein, F.; et al. Efficacy and cost-effectiveness of Stem Cell injections for symptomatic relief and structural improvement in people with Tibio-femoral knee Osteoarthritis: Protocol for a randomised placebo-controlled trial. BMJ 2021, 11, e056382. [Google Scholar]
- Salamanna, F.; Veronesi, F.; Maglio, M.; Della Bella, E.; Sartori, M.; Fini, M. New and emerging strategies in platelet-rich plasma application in musculoskeletal regenerative procedures: General overview on still open questions and outlook. BioMed Res. Int. 2015, 2015, 846045. [Google Scholar] [CrossRef]
- Arora, V.; Singh, G.; O-Sullivan, I.; Ma, K.; Natarajan Anbazhagan, A.; Votta-Velis, E.G.; Bruce, B.; Richard, R.; van Wijnen, A.J.; Im, H.-J. Gut-microbiota modulation: The impact of the gut-microbiota on osteoarthritis. Gene 2021, 785, 145619. [Google Scholar] [CrossRef]
- Gerardi, V.; Del Zompo, F.; D’Aversa, F.; Gasbarrini, A. Il legame tra il microbiota intestinale e le patologie cardiovascolari [The relationship between gut microbiota and cardiovascular diseases]. G. Ital. Di Cardiol. 2016, 17, 11–14. [Google Scholar]
- Rutsch, A.; Kantsjö, J.B.; Ronchi, F. The Gut-Brain Axis: How Microbiota and Host Inflammasome Influence Brain Physiology and Pathology. Front. Immunol. 2020, 11, 604179. [Google Scholar] [CrossRef]
- Liu, L.; Tian, F.; Li, G.Y.; Xu, W.; Xia, R. The effects and significance of gut microbiota and its metabolites on the regulation of osteoarthritis: Close coordination of gut-bone axis. Front. Nutr. 2022, 9, 1012087. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, X.; Zhang, C.; Liu, Z.; Li, C.; Ren, Z. Gut Microbiota and Bone Diseases: A Growing Partnership. Front. Microbiol. 2022, 13, 877776. [Google Scholar] [CrossRef]
- Liu, B.N.; Liu, X.T.; Liang, Z.H.; Wang, J.H. Gut microbiota in obesity. World J. Gastroenterol. 2021, 27, 3837–3850. [Google Scholar] [CrossRef]
- Hall, A.B.; Tolonen, A.C.; Xavier, R.J. Human genetic variation and the gut microbiome in disease. Nat. Rev. Genet. 2017, 18, 690–699. [Google Scholar] [CrossRef]
- Petersen, C.; Round, J.L. Defining dysbiosis and its influence on host immunity and disease. Cell. Microbiol. 2014, 16, 1024–1033. [Google Scholar] [CrossRef]
- Chen, Y.; Zhou, J.; Wang, L. Role and Mechanism of Gut Microbiota in Human Disease. Front. Cell. Infect. Microbiol. 2021, 11, 625913. [Google Scholar] [CrossRef]
- Schirmer, M.; Smeekens, S.P.; Vlamakis, H.; Jaeger, M.; Oosting, M.; Franzosa, E.A.; Ter Horst, R.; Jansen, T.; Jacobs, L.; Bonder, M.J.; et al. Linking the Human Gut Microbiome to Inflammatory Cytokine Production Capacity. Cell 2016, 167, 1125–1136.e8. [Google Scholar] [CrossRef]
- Mousa, W.K.; Chehadeh, F.; Husband, S. Microbial dysbiosis in the gut drives systemic autoimmune diseases. Front. Immunol. 2022, 13, 906258. [Google Scholar] [CrossRef]
- Favazzo, L.J.; Hendesi, H.; Villani, D.A.; Soniwala, S.; Dar, Q.A.; Schott, E.M.; Gill, S.R.; Zuscik, M.J. The gut microbiome-joint connection: Implications in osteoarthritis. Curr. Opin. Rheumatol. 2020, 32, 92–101. [Google Scholar] [CrossRef]
- Schott, E.M.; Farnsworth, C.W.; Grier, A.; Lillis, J.A.; Soniwala, S.; Dadourian, G.H.; Bell, R.D.; Doolittle, M.L.; Villani, D.A.; Awad, H.; et al. Targeting the gut microbiome to treat the osteoarthritis of obesity. JCI 2018, 3, e95997. [Google Scholar] [CrossRef]
- Guan, Z.; Jia, J.; Zhang, C.; Sun, T.; Zhang, W.; Yuan, W.; Leng, H.; Song, C. Gut microbiome dysbiosis alleviates the progression of osteoarthritis in mice. Clin. Sci. 2020, 134, 3159–3174. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Lan, H.; Hong, W.; Qian, D.; Peng, F.; Li, H.; Liang, C.; Du, M.; Gu, J.; Mai, J.; Bai, B.; et al. Quercetin modulates the gut microbiota as well as the metabolome in a rat model of osteoarthritis. Bioengineered 2021, 12, 6240–6250. [Google Scholar] [CrossRef]
- Zhang, H.; Qi, L.; Shen, Q.; Wang, R.; Guo, Y.; Zhang, C.; Richel, A. Comparative Analysis of the Bioactive Compounds in Chicken Cartilage: Protective Effects of Chondroitin Sulfate and Type II Collagen Peptides Against Osteoarthritis Involve Gut Microbiota. Front. Nutr. 2022, 9, 843360. [Google Scholar] [CrossRef]
- Liu, Q.; Hao, H.; Li, J.; Zheng, T.; Yao, Y.; Tian, X.; Zhang, Z.; Yi, H. Oral Administration of Bovine Milk-Derived Extracellular Vesicles Attenuates Cartilage Degeneration via Modulating Gut Microbiota in DMM-Induced Mice. Nutrients 2023, 15, 747. [Google Scholar] [CrossRef]
- Rios, J.L.; Bomhof, M.R.; Reimer, R.A.; Hart, D.A.; Collins, K.H.; Herzog, W. Protective effect of prebiotic and exercise intervention on knee health in a rat model of diet-induced obesity. Sci. Rep. 2019, 9, 3893. [Google Scholar] [CrossRef]
- O-Sullivan, I.; Natarajan Anbazhagan, A.; Singh, G.; Ma, K.; Green, S.J.; Singhal, M.; Wang, J.; Kumar, A.; Dudeja, P.K.; Unterman, T.G.; et al. Lactobacillus acidophilus Mitigates Osteoarthritis-Associated Pain, Cartilage Disintegration and Gut Microbiota Dysbiosis in an Experimental Murine OA Model. Biomedicines 2022, 10, 1298. [Google Scholar] [CrossRef]
- Xu, T.; Yang, D.; Liu, K.; Gao, Q.; Liu, Z.; Li, G. Miya Improves Osteoarthritis Characteristics via the Gut-Muscle-Joint Axis According to Multi-Omics Analyses. Front. Pharmacol. 2022, 13, 816891. [Google Scholar] [CrossRef]
- Cho, K.H.; Na, H.S.; Jhun, J.; Woo, J.S.; Lee, A.R.; Lee, S.Y.; Lee, J.S.; Um, I.G.; Kim, S.J.; Park, S.-H.; et al. Lactobacillus (LA-1) and butyrate inhibit osteoarthritis by controlling autophagy and inflammatory cell death of chondrocytes. Front. Immunol. 2022, 13, 930511. [Google Scholar] [CrossRef]
- Song, W.; Liu, Y.; Dong, X.; Song, C.; Bai, Y.; Hu, P.; Li, L.; Wang, T. Lactobacillus M5 prevents osteoarthritis induced by a high-fat diet in mice. J. Funct. Foods 2020, 72, 104039. [Google Scholar] [CrossRef]
- Guss, J.D.; Ziemian, S.N.; Luna, M.; Sandoval, T.N.; Holyoak, D.T.; Guisado, G.G.; Roubert, S.; Callahan, R.L.; Brito, I.L.; van der Meulen, M.C.; et al. The effects of metabolic syndrome, obesity, and the gut microbiome on load-induced osteoarthritis. Osteoarthr. Cartil. 2019, 27, 129–139. [Google Scholar] [CrossRef]
- Chen, L.; Huang, Z.; Li, Q.; Chen, C.; Luo, Y.; Kang, P. Activated intestinal microbiome-associated tryptophan metabolism upregulates aryl hydrocarbon receptor to promote osteoarthritis in a rat model. Int. Immunopharmacol. 2023, 118, 110020. [Google Scholar] [CrossRef]
- Jia, Y.J.; Li, T.Y.; Han, P.; Chen, Y.; Pan, L.J.; Jia, C.S. Effects of different courses of moxibustion treatment on intestinal flora and inflammation of a rat model of knee osteoarthritis. J. Integr. Med. 2022, 20, 173–181. [Google Scholar] [CrossRef]
- Xie, L.L.; Zhao, Y.L.; Yang, J.; Cheng, H.; Zhong, Z.D.; Liu, Y.R.; Pang, X.-L. Electroacupuncture Prevents Osteoarthritis of High-Fat Diet-Induced Obese Rats. BioMed Res. Int. 2020, 2020, 9380965. [Google Scholar] [CrossRef]
- Chen, Y.; Lv, J.; Jia, Y.; Wang, R.; Zhang, Z.; Liu, J.; Jia, C. Effect of Moxibustion on the Intestinal Flora of Rats with Knee Osteoarthritis Induced by Monosodium Iodoacetate. Evidence-based complementary and alternative medicine. eCAM 2020, 2020, 3196427. [Google Scholar]
- Collins, K.H.; Paul, H.A.; Reimer, R.A.; Seerattan, R.A.; Hart, D.A.; Herzog, W. Relationship between inflammation, the gut microbiota, and metabolic osteoarthritis development: Studies in a rat model. Osteoarthr. Cartil. 2015, 23, 1989–1998. [Google Scholar] [CrossRef]
- Li, K.; Liu, A.; Zong, W.; Dai, L.; Liu, Y.; Luo, R.; Ge, S.; Dong, G. Moderate exercise ameliorates osteoarthritis by reducing lipopolysaccharides from gut microbiota in mice. Saudi J. Biol. Sci. 2021, 28, 40–49. [Google Scholar] [CrossRef]
- Chan, L.C.; Zhang, Y.; Kuang, X.; Koohi-Moghadam, M.; Wu, H.; Lam, T.Y.C.; Chiou, J.; Wen, C. Captopril Alleviates Chondrocyte Senescence in DOCA-Salt Hypertensive Rats Associated with Gut Microbiome Alteration. Cells 2022, 11, 3173. [Google Scholar] [CrossRef]
- Yan, Y.; Yi, X.; Duan, Y.; Jiang, B.; Huang, T.; Inglis, B.M.; Zheng, B.; Si, W. Alteration of the gut microbiota in rhesus monkey with spontaneous osteoarthritis. BMC Microbiol. 2021, 21, 328. [Google Scholar] [CrossRef]
- Collins, K.H.; Schwartz, D.J.; Lenz, K.L.; Harris, C.A.; Guilak, F. Taxonomic changes in the gut microbiota are associated with cartilage damage independent of adiposity, high fat diet, and joint injury. Sci. Rep. 2021, 11, 14560. [Google Scholar] [CrossRef]
- Luna, M.; Guss, J.D.; Vasquez-Bolanos, L.S.; Alepuz, A.J.; Dornevil, S.; Strong, J.; Alabi, D.; Shi, Q.; Pannellini, T.; Otero, M. Obesity and load-induced post-traumatic osteoarthritis in the absence of fracture or surgical trauma. J. Orthop. Res. 2021, 39, 1007–1016. [Google Scholar] [CrossRef]
- Ulici, V.; Kelley, K.L.; Azcarate-Peril, M.A.; Cleveland, R.J.; Sartor, R.B.; Schwartz, T.A.; Loeser, R.F. Osteoarthritis induced by destabilization of the medial meniscus is reduced in germ-free mice. Osteoarthr. Cartil. 2018, 26, 1098–1109. [Google Scholar] [CrossRef]
- Hahn, A.K.; Wallace, C.W.; Welhaven, H.D.; Brooks, E.; McAlpine, M.; Christiansen, B.A.; Walk, S.T.; June, R.K. The microbiome mediates epiphyseal bone loss and metabolomic changes after acute joint trauma in mice. Osteoarthr. Cartil. 2021, 29, 882–893. [Google Scholar] [CrossRef]
- Wallace, I.J.; Bendele, A.M.; Riew, G.; Frank, E.H.; Hung, H.H.; Holowka, N.B.; Bolze, A.; Venable, E.; Yegian, A.; Dingwall, H.; et al. Physical inactivity and knee osteoarthritis in guinea pigs. Osteoarthr. Cartil. 2019, 27, 1721–1728. [Google Scholar] [CrossRef]
- Pedersini, P.; Savoldi, M.; Berjano, P.; Villafañe, J.H. A probiotic intervention on pain hypersensitivity and microbiota composition in patients with osteoarthritis pain: Study protocol for a randomized controlled trial. Arch. Rheumatol. 2021, 36, 296–301. [Google Scholar] [CrossRef]
- Taye, I.; Bradbury, J.; Grace, S.; Avila, C. Probiotics for pain of osteoarthritis; An N-of-1 trial of individual effects. Complement. Ther. Med. 2020, 54, 102548. [Google Scholar] [CrossRef]
- Wang, Z.; Zhu, H.; Jiang, Q.; Zhu, Y.Z. The gut microbiome as non-invasive biomarkers for identifying overweight people at risk for osteoarthritis. Microb. Pathog. 2021, 157, 104976. [Google Scholar] [CrossRef]
- Yu, X.H.; Yang, Y.Q.; Cao, R.R.; Bo, L.; Lei, S.F. The causal role of gut microbiota in development of osteoarthritis. Osteoarthr. Cartil. 2021, 29, 1741–1750. [Google Scholar] [CrossRef]
- Boer, C.G.; Radjabzadeh, D.; Medina-Gomez, C.; Garmaeva, S.; Schiphof, D.; Arp, P.; Koet, T.; Kurilshikov, A.; Fu, J.; Ikram, M.A.; et al. Intestinal microbiome composition and its relation to joint pain and inflammation. Nat. Commun. 2019, 10, 4881. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, Y.; Yao, X.; Li, S.; Wang, G.; Huang, Y.; Yang, Y.; Zhang, A.; Liu, C.; Zhu, D.; et al. Characterizations of the Gut Bacteriome, Mycobiome, and Virome in Patients with Osteoarthritis. Microbiol Spectr. 2023, 11, e0171122. [Google Scholar] [CrossRef]
- Ramasamy, B.; Magne, F.; Tripathy, S.K.; Venugopal, G.; Mukherjee, D.; Balamurugan, R. Association of Gut Microbiome and Vitamin D Deficiency in Knee Osteoarthritis Patients: A Pilot Study. Nutrients 2021, 13, 1272. [Google Scholar] [CrossRef]
- Guan, Z.; Jin, X.; Guan, Z.; Liu, S.; Tao, K.; Luo, L. The gut microbiota metabolite capsiate regulate SLC2A1 expression by targeting HIF-1α to inhibit knee osteoarthritis-induced ferroptosis. Aging Cell. 2023, 22, e13807. [Google Scholar] [CrossRef]
- Rushing, B.R.; McRitchie, S.; Arbeeva, L.; Nelson, A.E.; Azcarate-Peril, M.A.; Li, Y.Y.; Qian, Y.; Pathmasiri, W.; Sumner, S.; Loeser, R. Fecal metabolomics reveals products of dysregulated proteolysis and altered microbial metabolism in obesity-related osteoarthritis. Osteoarthr. Cartil. 2022, 30, 81–91. [Google Scholar] [CrossRef]
- Chen, J.; Wang, A.; Wang, Q. Dysbiosis of the gut microbiome is a risk factor for osteoarthritis in older female adults: A case control study. BMC Bioinform. 2021, 22, 299. [Google Scholar] [CrossRef]
- Wang, T.Q.; Li, L.R.; Tan, C.X.; Yang, J.W.; Shi, G.X.; Wang, L.Q.; Hu, H.; Liu, Z.S.; Wang, J.; Wang, T.; et al. Effect of Electroacupuncture on Gut Microbiota in Participants With Knee Osteoarthritis. Front. Cell. Infect. Microbiol. 2021, 11, 597431. [Google Scholar] [CrossRef]
- Arbeeva, L.; Azcarate-Peril, M.A.; Cui, Y.; Nelson, A.E.; Loeser, R.F. Association of plasma microbial composition with a leaky gut in obesity-related osteoarthritis: An exploratory study. Osteoarthr. Cartil. 2022, 4, 100317. [Google Scholar] [CrossRef]
- Loeser, R.F.; Arbeeva, L.; Kelley, K.; Fodor, A.A.; Sun, S.; Ulici, V.; Longobardi, L.; Cui, Y.; Stewart, D.A.; Sumner, S.J.; et al. Association of Increased Serum Lipopolysaccharide, But Not Microbial Dysbiosis, With Obesity-Related Osteoarthritis. Arthritis Rheumatol. 2022, 74, 227–236. [Google Scholar] [CrossRef]
- Lee, Y.H.; Song, G.G. The Gut Microbiome and Osteoarthritis: A Two-Sample Mendelian Randomization Study. J. Rheum. Dis. 2021, 28, 94–100. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | MeSH Terms |
|---|---|
| PubMed | ((“osteoarthritis”[MeSH Terms] OR “osteoarthritis”[All Fields] OR “osteoarthritides”[All Fields]) AND (“gastrointestinal microbiome”[MeSH Terms] OR (“gastrointestinal”[All Fields] AND “microbiome”[All Fields]) OR “gastrointestinal microbiome”[All Fields] OR (“gut”[All Fields] AND “microbiota”[All Fields]) OR “gut microbiota”[All Fields])) AND (y_10[Filter]) |
| Scopus | TITLE-ABS-KEY TITLE-ABS-KEY (osteoarthritis)) AND ((TITLE-ABS-KEY (gut AND microbiota)) OR (TITLE-ABS-KEY (gastrointestinal AND microbiome))) AND PUBYEAR > 2012 AND (LIMIT-TO (LANGUAGE, “English”)) AND (LIM-IT-TO (DOCTYPE, “ar”)) |
| Web of Science | (TS = osteoarthritis OR TS = osteoarthritides) AND (TS = gut microbiota OR TS = gastrointestinal microbiome)—with Publication Year from 2013 to 2023, English |
| Treatment Classification | Species/Age/Sex/ Animals Number | OA Model | Aim | Treatment | Experimental Groups and Time | OA Assessment | Microbiome Assessment | Main Results | Relation between OA and Gut Dysbiosis | Ref. Year, Country | SYRCLE Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Supplements | Rats, NR, NR, NR | MIA | To evaluate changes in gut microbiota and metabolism during quercetin therapy for OA | Quercetin | (1) OA; (2) Quercetin; (3) Control 29 days | NR | DNA sequencing (targeting 16s rRNA gene) | ↓SCFAs (acetic and propionic acid) in OA group vs. control; ↑SCFAs (acetic and propionic acid) in quercetin group vs. OA group; ↑LA and ↓Ruminococcacea in quercetin group vs. all groups | Quercetin treatment influences the features and composition of gut microbiota as well as metabolism in OA | Lan et al. 2021 [31], USA | High |
| Supplements | SD rats, 8–9 weeks old, male, 30 | MIA | To evaluate the effects of bioactive compounds of chicken cartilage for OA treatment | Chicken cartilage food supplements | (1) Sham (oral gavage of saline); (2) OA + oral gavage of saline; (3) OA + oral gavage of CS; (4) OA + oral gavage of collagen peptides; (5) OA + oral gavage of diacerein 4 weeks | Rotating rod test, ramp test, histopathology, Mankin score | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | ↑Athletic ability and ↓IL1β, IL6, PGE2, TNFα with CS treatment | CS reduces OA development by modulating gut microbiota | Zhang et al. 2022 [32], China | Moderate |
| Supplements | C57BL/6J mice, male, 6 weeks old, 57 | DMM | The therapeutic potential of mEVs for OA treatment | EV isolated from raw milk | (1) Healthy control; (2) DMM + PBS; (3) DMM + mEVs 10 weeks | Serum ELISA, histology, OARSI score, IHC | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | ↓MMP-1, diversity of gut microbiota and ↑COL2A1 in DMM + mEVs group vs. DMM + PBS group | mEV reduces cartilage degradation by decreasing catabolic protein expression and restoring the gut microbiota | Liu et al. 2023 [33], China | Moderate |
| Supplements | SD rats, 12 weeks old, NR, 49 | HFS diet | To determine the effects of prebiotic fiber supplementation, aerobic exercise, and the combination of the two, on OA development | Prebiotic fiber | (1) Sedentary + standard chow diet; (2) Sedentary + HFS diet; (3) Non-exercise + HFS diet + prebiotic fiber; (4) Exercise + HFS diet; (5) Exercise + HFS diet + prebiotic fiber 12 weeks | Histology | DNA sequencing (targeting 16s rRNA gene) | ↓Joint damage, leptin level, lipid profile, endotoxin in non-exercise + HFS diet + prebiotic fiber, exercise + HFS diet and exercise + HFS diet + prebiotic fiber groups; ↓dysbiosis in non-exercise + HFS diet + prebiotic fiber group | Prebiotic fiber supplementation, aerobic exercise, and the combination of both treatments prevent OA also by influencing inflammation and dysbiosis | Rios et al. 2019 [34], Canada | Moderate |
| Supplements | C57BL/6J mice, 5 weeks old, NR, NR | DMM | To evaluate the impact of obesity and oligofructose on gut microbiome and OA | Oligofructose supplementation | Low or HFD + diet supplemented with control fiber or prebiotic + DMM or sham surgery 2 weeks after DMM | Histology, OARSI score | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | Oligofructose treatment ↑colon transcriptome, ↓colonic macrophage cell signature and joint inflammation, preserving articular cartilage and protecting against OA | Oligofructose supplementation impacts on the gut microbiome and plays a protective role against trauma-induced OA | Schott et al. 2018 [26], USA | High |
| Probiotics | C57BL/6 mice, 11 weeks old, female, 40 | PMM | To evaluate the LA1 effect OA | LA1, Bifidobacterium breve, LA reuteri, Bacillus subtilis | (1) OA + PBS; (2) OA + LA1; (3) OA + Bifidobacterium breve (4) OA + LA reuteri; (5) OA + Bacillus subtilis 9 and 12 weeks after surgery | Histology | DNA sequencing (targeting 16s rRNA gene) | ↓IL1β, TNFα, NFKB, NLRP3, VEGF, NGF, artemin, GFRα3, RUNX2, MMP13, pain, heat tolerance and cartilage damage and ↑genus Akkermanis munniphila and Lachnospiraceae with LA1 treatment | LA1 protect joint tissue integrity during OA progression, as shown by significant alterations in the OA gut microbiome | O-Sullivan et al. 2022 [35], USA | High |
| Probiotics | Wistar rats, NR, female, 30 | ACL dissection | To investigate the effects of MY, a product made from Clostridium butyricum, on OA | MY | (1) Control; (2) OA; (3) OA + MY 4 weeks | Histology | DNA sequencing (targeting 16s rRNA gene) | MY ↑Chao1, Shannon and Pielou vs. untreated group; ↑Prevotella, Ruminococcus, Desulfovibrio, Shigella, Helicobacter and Streptococcus in OA group; ↑LA, Oscillospira, Clostridium and Coprococcus with MY treatment | MY protect against OA via the gut–muscle–joint axis by increasing the beneficial bacteria | Xu et al. 2022 [36], China | High |
| Probiotics | Wistar rats, 7 weeks old, male, 6 | MIA | Investigate the effect of live LA1 on OA progression | LA1 | (1) OA; (2) OA + LA1 24 days | Histology, Mankin and OARSI scores | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | LA1 and butyrate administration ↓pain, cartilage damage, intestinal damage, IL1β, MCP1, TNFα and ↑OCLN, ZO1, Bifidobacterium, Faecalibacterium prausnizii | LA1 or butyrate ameliorates OA progression by modulating the gut environment | Cho et al. 2022 [37], USA | High |
| Probiotics | Balb/c mice, 8 weeks old, NR, NR | HFD | To analyze the correlation between OA and gut microbiota and to evaluate the treatment with L. paracasei subsp. paracasei M5 (M5) and CS for OA prevention | M5, CS and CS-M5 | (1) Control diet + oral gavage saline; (2) HFD + oral gavage saline; (3) HFD + CS; (4) HFD + M5; (5) HFD + CS-M5 12 weeks | Histology, Mankin score | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | ↑COLII, adiponectin and ↓leptin in HFD + M5 and HFD + CS-M5 groups vs. all the other groups | M5 regulates adipokines levels and gut microbiota composition and inhibits OA development | Song et al. 2020 [38], China | High |
| ABT | C57BL/6N mice, 8 weeks, male and female, 54 | DMM | To evaluate the relationship between gut dysbiosis induced by ABT administration and structural changes in early-stage OA | Ampicillin, neomycin | (1) Control-female; (2) OA-female; (3) ABT-OA-female; (4) Control-male; (5) OA-male; (6) ABT-OA-male 8 weeks | DXA, Micro-CT, histology, IHC | Universal primers and specific bacterial primers, including those for α-proteobacteria, γ-proteobacteria, Bacteroidetes, Firmicutes and Actinobacteria | ABT-induced intestinal microbiota dysbiosis ↓LPS serum level, TNFα and IL6, which lead to ↓MMP13 | Gut microbiome dysbiosis alleviates OA progression | Guan et al. 2020 [27], China | High |
| ABT | C57BL/6J and TLR5KO mice, NR, male, 10–11 for group | Load-induced OA (cyclic compressive loading) | To evaluate the impact of obesity, metabolic syndrome and gut microbiome on load-induced OA | Ampicillin, neomycin | (1) Control C57BL/6J; (2) TLR5KO + metabolic syndrome; (3) TLR5KO + ABT; (4) C57BL/6J + HFD 4 weeks | Histology, OARSI score | DNA sequencing (targeting 16s rRNA gene) | ↓Thickness of subchondral bone plate in TLR5KO + ABT group; ↑LPS, KC, IL10, TNFα and ↓IL6 in C57BL/6J + HFD group vs. TLR5KO + ABT group | Changes in gut microbiota influence the severity of OA | Guss et al. 2019 [39], USA | High |
| ABT | SD rats, 8 weeks old, male, 32 | ABT pretreatment combined with a Try-rich diet (or not) | To evaluate the role of aryl hydrocarbon R in OA and its association with intestinal microbiome | ABT and Try intervention | (1) Sham surgery; (2) OA control; (3) ABT; (4) ABT + Try 9 weeks | Histology, OARSI score | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | ↑Col2A1, SOX9 and ↓MMP13, LPS in ABT group vs. OA control group; ↑AhR, CyP1A1, Col2A1, MMP13 in ABT + Try group vs. OA control and ABT groups | Try supplementation activated intestinal microbiome-related Try metabolism, antagonizing the effects of ABT, exacerbating OA | Chen et al. 2023 [40], China | Low |
| Non-pharmacological treatments | Wistar rats, 8 weeks old, male, 37 | MIA | To evaluate the effect and dose-effect of MS on OA | MS | (1) Healthy control; (2) OA; (3) OA + MS for 2 weeks; (4) OA + MS for 4 weeks; (5) OA + MS for 6 weeks 2, 4, 6 weeks | Histology, Mankin score | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | ↑Chondrocytes, IL10 and ↓IL1β, TNFα in OA + MS for 4 and 6 weeks groups vs. OA and OA + MS for 2 weeks groups | MS treatment regulates intestinal microbiome composition and inflammation, influencing OA progression | Jia et al. 2022 [41], China | Moderate |
| Non-pharmacological treatments | SD rats, 8 weeks old, male, 30 | HFD | To evaluate the effect of acupunctures on gut microbiome and OA recovery | ST36, GB34, and ST36 + GB34 acupuncture treatments | (1) Control chow diet; (2) HFD; (3) HFD + ST36; (4) HFD + GB34; (5) HFD + ST36 + GB34 14 weeks | Histology, Mankin score | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | ↓Cartilage loss, MMP1, MMP13 in HFD + ST36, HFD + GB34 and HFD + ST36 + GB34 groups vs. HDF group; ↓inflammatory cytokines, VEGF, MIP1α, MIP2, MCP1, LPS level, 65 and P-p65 in HFD + ST36 + GB34 group vs. HFD, HFD + ST36 groups | ST36 and GB34 treatments inhibit OA degradation by regulating the lipid metabolism and gut microbiota | Xie et al. 2020 [42], China | High |
| Non-pharmacological treatments | Wistar rats, 12 weeks, male, 36 | MIA | To analyze the effect of MS on the intestinal flora during OA | MS or DS | (1) Healthy control; (2) OA; (3) OA + MS; (4) OA + DS 4 weeks | Histology | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | ↓IL1β, TNFα, LPS in MS and DS groups | MS reduces OA cartilage damage by regulating the composition of intestinal flora | Chen et al. 2020 [43], China | Low |
| HFD | Rats, 8–12 weeks old, NR, 32 | HFD | To evaluate the relationship between inflammation, gut microbiota, and metabolic OA | No treatment | (1) Diet-induced obesity; (2) Chow diet 28 weeks | Mankin score | DNA sequencing (targeting 16s rRNA gene) | ↑Mankin score, synovial fluid and serum analytes, LPS in diet-induced obesity group vs. chow diet group | The high presence of Lactobacillus species (spp.) and Methanobrevibacter spp. had a strong predictive relationship with OA Mankin score | Collins et al. 2015 [44], Canada | High |
| HFD | C57BL/6J mice, 12 weeks old, male, 54 | HFD | To evaluate if wheel-running exercise prevents OA induced by HFD by reducing LPS from intestinal microorganisms | No treatments | (1) Control; (2) HFD 8 weeks | Histology, Mankin score, histochemistry | DNA sequencing (targeting 16s rRNA gene) | HFD treatment ↓gut microbial diversity, gut barrier-protecting bacteria and ↑endotoxin-producing bacteria. The voluntary wheel running ↓TLR4, MMP13 and LPS levels in blood and synovial fluid | Exercising can remodel gut microbial ecosystems, reduce the circulating levels of LPS, contributing to the relief of chronic inflammation and OA | Li et al. 2021 [45], China | Low |
| Anti-hypertensive | SD rats, 6 weeks old, NR, 24 | DOCA, OA and hypertensive | Impact of hypertension on the articular cartilage and subchondral bone and the therapeutical effect of senescence removal by anti-hypertensive drug captopril | Captopril | (1) Healthy control; (2) DOCA; (3) DOCA + captopril 14 weeks | Micro-CT, histology, IHC | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | ↑p16 and proteoglycan loss in DOCA group vs. control; ↓senescence cells in DOCA + captopril group | Captopril has an anti-senolytic effect and decreases cartilage degeneration by restoring gut microbial structure | Chan et al. 2022 [46], China | High |
| No treatments | Rhesus macaque, 6–15 years old, female, 20 | Spontaneous OA | To explore the relationship between OA and intestinal microbiota | No treatment | (1) Healthy control; (2) OA NR | MRI | DNA extraction from fecal samples and metagenomics analysis | ↑LA in OA monkeys; ↑Prevotella and Ruminococcus in non-OA monkeys | The diversity and composition of intestinal microbiota in monkeys with OA are different compared to the normal monkeys | Yan et al. 2021 [47], China | High |
| No treatments | Mice LD and littermate control (WT), 16 weeks old, male and female, 5–10 for sex and group | DMM | To define a relationship between knee cartilage damage and gut microbiota | No treatment | LD and WT mice, fed HFD/chow or rescued with fat implantation 13 weeks | Histology, Mankin score | DNA sequencing (targeting 16s rRNA gene) | ↑Synovial fluid LPS levels in HFD WT mice vs. all groups; ↓Bacteroidetes:Firmicutes ratio of the gut microbiota in HFD and OA-rescued animals vs. chow | Causal relationships between gut microbiome and cartilage health, independent of diet or adiposity | Collins et al. 2021 [48], USA | High |
| No treatments | C57BL/6J and TLR5KO mice, 4 weeks old, male, 88 | Load-induced OA | To evaluate the influence of obesity on cartilage degeneration | No treatment | (1) Severe obesity (C57Bl6/J + HFD) (2) mild obesity (TLR5KO + standard chow) (3) normal adiposity (C57Bl6/J + standard chow) (4) TLR5KO + ABT + normal diet 6 weeks | Micro-CT, histology | DNA sequencing (targeting 16s rRNA gene) | No differences in the severity of cartilage degeneration among groups, constituents of the gut microbiota (Verrucomicrobia, Proteobacteria, Tenericutes and Actinobacteria) differed among groups | No association between components of the gut microbiota with OA | Luna et al. 2021 [49], USA | High |
| No treatments | C57BL/6J mice, NR, male, 43 | DMM | To evaluate the contribution of gut microbiota to develop OA after joint injury | No treatment | (1) C57BL/6J GF; (2) C57BL/6J SPF (two groups: 13.5 weeks age at DMM and 43 weeks age at DMM) 8 weeks | Histology, OARSI score | DNA sequencing (targeting V3–V4 region of 16s rRNA gene) | ↓Cartilage damage and proteoglycan loss in GF group vs. SPF groups | Gut microbiota promote OA progression | Ulici et al. 2018 [50], USA | High |
| No treatments | C57BL/6 mice GF and conventional, 20 weeks old, NR, 50 | ACL injury | To evaluate the gut microbiota effect on OA progression | No treatment | (1) GF OA; (2) GF contralateral; (3) GF naïve; (4) conventional OA; (5) conventional contralateral; (6) conventional naïve 1 week | Micro-CT | Global metabolomic profiling | ↑Trabecular bone volume and ↓trabecular bone loss, sensitive to injury in GF groups vs. conventional groups | Gut microbiota promotes OA development | Hahn et al. 2021 [51], USA | High |
| No treatments | Hartley guinea pigs, 7 weeks old, male, 36 | Spontaneous OA | To evaluate sedentary lifestyle contribution to OA incidence and severity | No treatment | (1) Sedentary; (2) physically active 22 weeks | Histology | DNA sequencing (targeting V4 region of 16s rRNA gene) | No taxa distinguished the microbial composition of samples collected from sedentary and physically active animals | Gut microbial communities of sedentary and physically active OA animals were indistinguishable | Wallace et al. 2019 [52], USA | Moderate |
| Treatment Classification | Study Design | Age/Gender/Number | OA Assessment Methods | Study Aim | Treatment | Groups | Follow-Up or Experimental Time | Microbiota Assessment | Main Results | Ref., Year, Country | ROBINS I Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Probiotics | RCT | Mean age: 50 ± 90 yrs, NR, 60 | KL | Effect of probiotics on OA pain | Probiotic formulation of LA casei | (1) Healthy control; (2) OA | 6 weeks | VAS, pressure pain threshold, IL6, TNFα, IL6 R, IL1 R, CRP, DNA sequencing (targeting 16s rRNA gene) | Probiotics and conservative treatment improve OA-related pain | Pedersini et al. 2021 [53], Italy | Low |
| Probiotics | Trial of individual effects | 67 yrs, female, 1 | NR | Effectiveness of probiotics on OA pain | LA rhamnosus, Saccharomyces cerevisiae (boulardii) and Bifidobacterium animalis ssp lactis vs. placebo treatment | (1) OA | 32 weeks | VAS, GHQ-12, PSFS, CDSA | Probiotic use reduces OA pain | Taye et al. 2020 [54], Australia | Low |
| Non-pharmacological treatments | Multicentric RCT | 45–75 yrs, NR, 90 | X-ray | Effect of EA on gut microbiota in OA pts | EA | (1) Healthy controls; (2) OA sham acupuncture; (3) OA EA | 8 weeks | DNA sequencing (targeting 16s rRNA gene) | ↑Streptococcus significant associated with OA severity | Wang et al. 2021 [55], China | Low |
| No treatments | Retrospective | NR, NR, 18345 | NR | Link between gut microbiota imbalance and OA progression | No treatments | (1) OA | NR | DNA sequencing (targeting 16s rRNA gene) | Methanobacteriaceae and desulfoovibrionales onegatively correlated with knee OA risk | Yu et al. 2021 [56], China | Low |
| No treatments | Prospective | 56.9 yrs, male (606), female (821), 1427 | KL, X-ray, WOMAC | Relationship between joint pain and microbiome composition in OA | No treatments | (1) Healthy control; (2) OA | NR | Analysis of taxonomic profiling of gastrointestinal microbiota from stool samples | ↑Streptococcus spp. significantly associated with ↑WOMAC in OA pts | Boer et al. 2019 [57], Netherlands | Low |
| No treatments | Prospective | NR, female (34) and male (10) OA pts, female (28) and male (18) control pts | NR | Characterizations of the gut bacteriome, mycobiome, and virome in OA pts | No treatments | (1) Healthy control; (2) OA | NR | DNA extraction and whole-metagenome shotgun sequencing | Gut microbiome of OA pts completely altered compared to that of healthy individuals | Chen et al. 2021 [58], China | Low |
| No treatments | Observational | Mean age: 45.5 ± 10.2 yrs, NR, 24 | KL, WOMAC | Gut microbiome composition in OA pts and normal individuals with or without VDD | No treatments | (1) OA-VDD (n = 7); (2) OA (n = 4); (3) VDD (n = 7); (4) NVD (n = 6) | 6 months | DNA sequencing (targeting V3-V4 region of 16s rRNA gene) | Association between gut microbiome, vitamin D and knee OA | Ramasamy et al. 2021 [59], India | Low |
| No treatments | Cross-sectional | Mean age: 53.69 ± 4.58 yrs, NR, 78 | KL | Gut microbiota and metabolites effect in OA | No treatments | (1) Healthy control; (2) OA | NR | Albumin, hemoglobin, pro-albumin, superoxide dismutase, monoamine oxidase, glutathione reductase, total iron binding serum concentration analyses | Protective effect of gut microbiota and its metabolite capsiate on ferroptosis-relative OA | Guan et al. 2023 [60], China | Low |
| No treatments | Retrospective | >45 yrs, NR, 92 | KL | Perturbations in gut microbial composition and the gut metabolome linked to individuals with obesity and OA | No treatments | (1) Healthy control; (2) OA | NR | Untargeted fecal metabolomics analysis | Perturbations in leukotriene metabolism, and changes in microbial metabolites modify OA proteolysis | Rushing et al. 2022 [61], USA | Low |
| No treatments | Retrospective | Mean age: 65.0 ± 7.7 yrs, NR, 57 | NR | Relationship between gut microbiome and OA in the older female adults | No treatments | (1) Healthy control; (2) OA | NR | DNA sequencing (targeting 16s rRNA gene) | Alterations in the gut microbial composition and function in OA | Chen et al. 2021 [62], China | Low |
| No treatments | Prospective | <75 yrs, NR, 182 | NR | Gut microbiome and risk for OA | No treatments | (1) Healthy control; (2) OA | NR | DNA sequencing (targeting 16s rRNA gene) | Diversity and richness of the gut microbiome ↓in overweight OA pts | Wang et al. 2021 [63], China | Low |
| No treatments | Cross-sectional | >55 yrs, NR, 70 | KL | Correlation among plasma microbiota, LPS, and obesity-associated OA | NR | (1) OA | NR | LPS level and DNA sequencing (targeting 16s rRNA gene) | Correlation between serum LPS and plasma microbiome | Arbeeva et al. 2022 [64], USA | Low |
| No treatments | Prospective | >45 yrs, NR, 92 | KL | Role of dysbiosis in obesity-associated OA | No treatments | (1) Healthy control; (2) OA | NR | DNA sequencing (targeting 16s rRNA gene), cytokine and LPS measures | ↑Intestinal permeability contribute to OA development associated with obesity | Loeser et al. 2022 [65], USA | Low |
| No treatments | Two-sample Mendelian randomization | NR, NR, 11400 | KL | Correlation between intestinal microbiota and OA occurrence | No treatments | (1) Healthy control; (2) OA | NR | NR | No association between intestinal microbiome and OA | Lee et al. 2021 [66], Korea | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchese, L.; Contartese, D.; Giavaresi, G.; Di Sarno, L.; Salamanna, F. The Complex Interplay between the Gut Microbiome and Osteoarthritis: A Systematic Review on Potential Correlations and Therapeutic Approaches. Int. J. Mol. Sci. 2024, 25, 143. https://doi.org/10.3390/ijms25010143
Marchese L, Contartese D, Giavaresi G, Di Sarno L, Salamanna F. The Complex Interplay between the Gut Microbiome and Osteoarthritis: A Systematic Review on Potential Correlations and Therapeutic Approaches. International Journal of Molecular Sciences. 2024; 25(1):143. https://doi.org/10.3390/ijms25010143
Chicago/Turabian StyleMarchese, Laura, Deyanira Contartese, Gianluca Giavaresi, Laura Di Sarno, and Francesca Salamanna. 2024. "The Complex Interplay between the Gut Microbiome and Osteoarthritis: A Systematic Review on Potential Correlations and Therapeutic Approaches" International Journal of Molecular Sciences 25, no. 1: 143. https://doi.org/10.3390/ijms25010143