
Plasma Lysophosphatidic Acid Concentrations in Sex Differences and Psychiatric Comorbidity in Patients with Cocaine Use Disorder
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Sociodemographic Characteristics
2.2. Prevalence and Sex Differences in Cocaine-Related Variables, Psychiatric and Medical Comorbidity, and Use of Medication in Abstinent CUD Patients

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | CUD Group | |||||
|---|---|---|---|---|---|---|
| Total N = 88 | Men N = 74 | Women N = 14 | Statistic | p-Value | ||
| Age at first cocaine use 1 [Mean (SD)] | Years | 17.53 (7.93) | 19.13 (0.69) | 22 (1.51) | 210 | 0.027 |
| Age at onset of CUD 1 [Mean (SD)] | Years | 23.65 (10.60) | 26.98 (1.04) | 27.25 (1.55) | 333.500 | 0.293 |
| Length of CUD diagnosis 1 [Mean (SD)] | Years | 6.71 (6.74) | 7.65 (0.94) | 6.92 (1.86) | 413 | 0.708 |
| Severity criteria 1 [Mean (range)] | Criteria [1,2,3,4,5,6,7,8,9,10,11] | 7.28 (3.20) | 7.09 (0.39) | 8.29 (0.54) | 433 | 0.328 |
| Length of abstinence 1 [Mean (mode)] | Days | 42.90 (72.56) | 40.35 (8.86) | 52.83 (20.34) | 340.500 | 0.149 |
| Comorbid substance use disorders 2 [N (%)] | Alcohol | 46 (52.30) | 39 (52.70) | 7 (50) | 0.034 | 0.853 |
| Cannabis | 27 (30.70) | 27 (36.50) | - | 7.285 | 0.007 | |
| Sedatives | 7 (8) | 7 (9.50) | - | 1.422 | 0.233 | |
| Opiates | 5 (5.70) | 5 (6.80) | - | 0.992 | 0.319 | |
| Stimulants | 4 (4.50) | 3 (4.10) | 1 (7.10) | 0.259 | 0.613 | |
| Comorbid psychiatric disorders 2 N (%)] | Mood | 26 (29.50) | 23 (31.10) | 3 (21.40) | 0.521 | 0.470 |
| Anxiety | 23 (26.10) | 14 (18.90) | 9 (64.30) | 12.408 | <0.001 | |
| Personality | 20 (22.7) | 16 (21.60) | 4 (28.6) | 0.320 | 0.572 | |
| ADHD | 16 (18.20) | 15 (20.30) | 1 (7.10) | 1.348 | 0.243 | |
| Psychotic | 6 (6.80) | 6 (8.10) | - | 1.204 | 0.272 | |
| Eating | 5 (5.70) | 1 (1.40) | 4 (28.60) | 16.09 | <0.001 | |
| Psychiatric medication 2 [N (%)] | Anxiolytics | 37 (42) | 30 (40.50) | 7 (50) | 0.732 | 0.392 |
| Antidepressants | 31 (35.20) | 26 (35.10) | 5 (35.70) | 0.038 | 0.845 | |
| Disulfiram | 14 (15.90) | 13 (17.80) | 1 (7.70) | 0.819 | 0.365 | |
| Antipsychotics | 9 (10.20) | 7 (9.50) | 2 (14.30) | 0.391 | 0.532 | |
| Anticraving | 6 (6.80) | 3 (4.10) | 3 (21.40) | 6.046 | 0.014 | |
| Medical problem | No Yes | 82.07 17.30 | 10 (13.50) | 4 (28.60) | 2.507 | 0.113 |
2.3. Plasma Concentrations of LPA Species in Abstinent CUD Patients
2.4. Correlation Analysis between Plasma Concentrations of LPA and Cocaine-Related Variables
2.5. Plasma Concentrations of LPA Species in Comorbid Psychiatric Disorders in Abstinent CUD Patients
2.6. Plasma Concentrations of LPA Species in Comorbid Alcohol and Cannabis Use Disorders in Abstinent CUD Patients
2.7. Plasma Concentrations of LPA Species in Comorbid Medical Problems and Psychiatric Medication in Abstinent CUD Patients
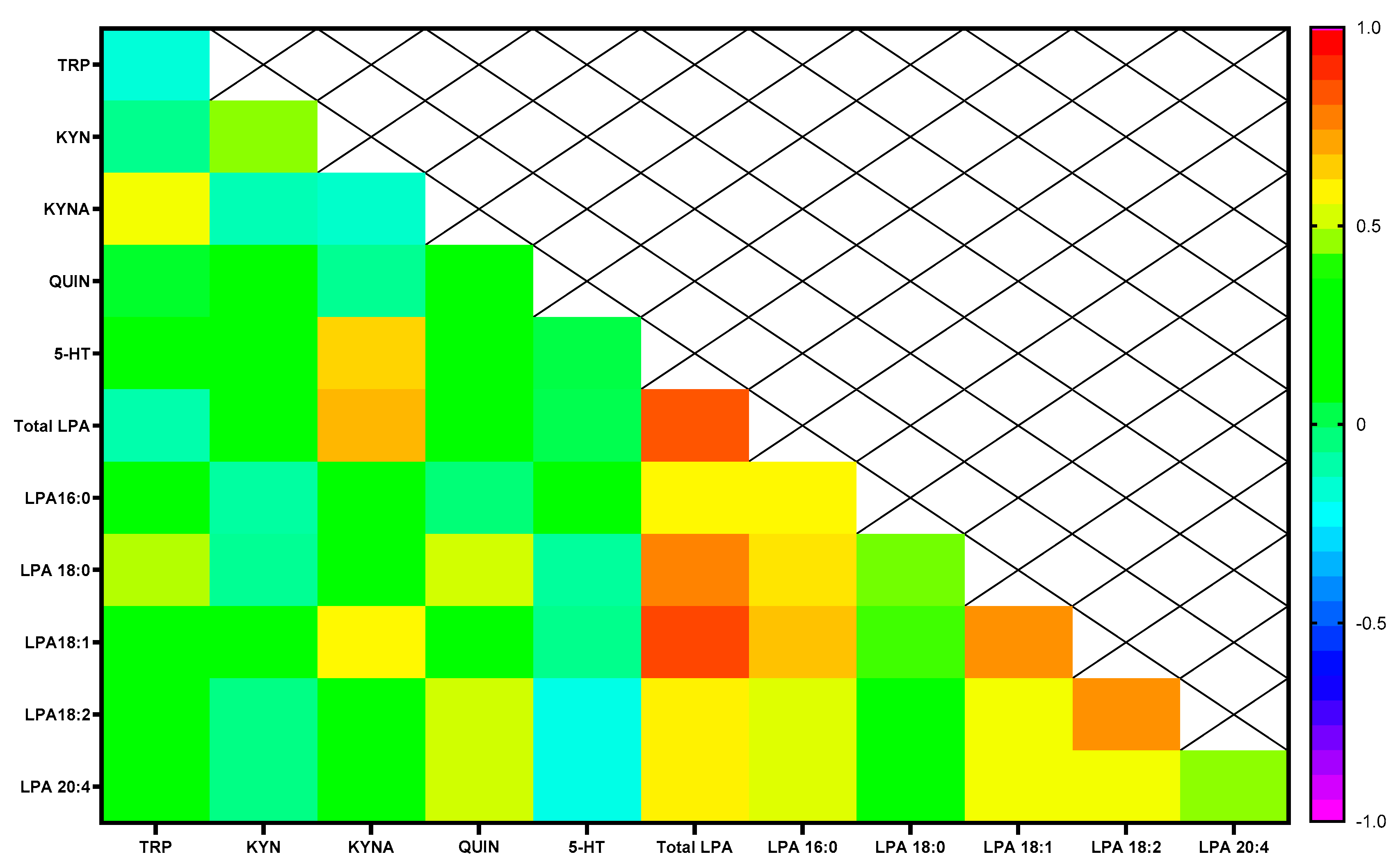
2.8. Correlations Analysis between Plasma Concentrations of LPA, Cortisol and Tryptophan Metabolites in Abstinent CUD Patients
3. Discussion
Limitations and Future Directions
4. Materials and Methods
4.1. Participants and Recruitment
4.2. Ethics Statements
4.3. Clinical Assessments
4.4. Collection of Plasma Samples
4.5. Determination of LPA Species
4.6. Determination of TRP, KYN, KYNA, QUIN and 5-HT
4.7. Determination of Cortisol
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- EMCDDA. European Drug Report 2022: Trends and Developments. In Managing Pharmaceuticals in International Health; EMCDDA: Lisbon, Portugal, 2022. [Google Scholar]
- UNODC. UNODC World Drug Report 2020: Global Drug Use Rising; While COVID-19 Has Far Reaching Impact on Global Drug Markets. 2020. Available online: https://www.unodc.org/unodc/press/releases/2020/June/media-advisory---global-launch-of-the-2020-world-drug-report.html (accessed on 24 September 2023).
- Observatorio Español de Las Drogas y Las Adicciones; Ministerio de Sanidad SS e Igualdad. INFORME 2022: Alcohol, Tabaco y Drogas Ilegales en España; Delegación del Gobierno para el Plan Nacional sobre Drogas: Madrid, Spain, 2022; 293p. [Google Scholar]
- Barroso-Moguel, R.; Villeda-Hernández, J.; Méndez-Armenta, M. Medical causes and effects of cocaine abuse. Arch. De Investig. Médica 1991, 22, 3–8. [Google Scholar]
- González-Saiz, F.; Vergara-Moragues, E.; Verdejo-García, A.; Fernández-Calderón, F.; Lozano, O.M. Impact of psychiatric comorbidity on the In-treatment outcomes of cocaine-dependent patients in therapeutic communities. Subst. Abuse 2014, 35, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Vergara-Moragues, E.; González-Saiz, F.; Lozano, O.M.; Espinosa, P.B.; Calderón, F.F.; Bilbao-Acebos, I.; Pérez García, M.; Verdejo García, A. Psychiatric comorbidity in cocaine users treated in therapeutic community: Substance-induced versus independent disorders. Psychiatry Res. 2012, 200, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Araos, P.; Vergara-Moragues, E.; Pedraz, M.; Pavón, F.J.; Campos Cloute, R.; Calado, M.; Ruiz, J.J.; García-Marchena, N.; Gornemann, I.; Torrens, M.; et al. Comorbilidad psicopatológica en consumidores de cocaína en tratamiento ambulatorio. Adicciones 2014, 26, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Back, S.E.; Dansky, B.S.; Carroll, K.M.; Foa, E.B.; Brady, K.T. Exposure therapy in the treatment of PTSD among cocaine-dependent individuals: Description of procedures. J. Subst. Abuse Treat. 2001, 21, 35–45. [Google Scholar] [CrossRef]
- Chen, K.W.; Banducci, A.N.; Guller, L.; Macatee, R.J.; Lavelle, A.; Daughters, S.B.; Lejuez, C.W. An examination of psychiatric comorbidities as a function of gender and substance type within an inpatient substance use treatment program. Drug Alcohol Depend. 2011, 118, 92–99. [Google Scholar] [CrossRef]
- Schwartz, E.K.C.; Wolkowicz, N.R.; De Aquino, J.P.; MacLean, R.R.; Sofuoglu, M. Cocaine Use Disorder (CUD): Current Clinical Perspectives. Subst. Abuse Rehabil. 2022, 13, 25–46. [Google Scholar] [CrossRef]
- Vergara-Moragues, E.; González-Saiz, F.; Lozano-Rojas, O.; Fernández Calderón, F.; Verdejo García, A.; Betanzos Espinosa, P.; Bilbao Acedos, I.; Pérez García, M. Relación entre la comorbilidad psicopatológica y las variables de resultados en dependientes de cocaína tratados en comunidad terapéutica. Adicciones 2013, 25, 128–136. [Google Scholar] [CrossRef]
- McHugh, R.K.; Votaw, V.R.; Sugarman, D.E.; Greenfield, S.F. Sex and gender differences in substance use disorders. Clin. Psychol. Rev. 2018, 66, 12–23. [Google Scholar] [CrossRef]
- Herrero, M.J.; Domingo-Salvany, A.; Torrens, M.; Brugal, M.T.; Itinere Investigators. Psychiatric comorbidity in young cocaine users: Induced versus independent disorders. Addiction 2008, 103, 284–293. [Google Scholar] [CrossRef]
- Quinones-Jenab, V.; Jenab, S. Influence of sex differences and gonadal hormones on cocaine addiction. ILAR J. 2012, 53, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Polcin, D.L.; Nayak, M.B.; Blacksher, S. Addressing trauma among women with serious addictive disorders: Treatment models, program factors and potential mediators. J. Drug Addict. Educ. Erad. 2008, 4, 221–237. [Google Scholar] [PubMed]
- Lopez-Quintero, C.; Cobos JP de los Hasin, D.S.; Okuda, M.; Wang, S.; Grant, B.F.; Blanco, C. Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: Results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug Alcohol Depend. 2011, 115, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Najavits, L.M.; Lester, K.M. Gender differences in cocaine dependence. Drug Alcohol Depend. 2008, 97, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Sanvicente-Vieira, B.; Rovaris, D.L.; Ornell, F.; Sordi, A.; Rothmann, L.M.; Niederauer, J.P.O.; Schuch, J.B.; von Diemen, L.; Kessler, F.H.P.; Grassi-Oliveira, R. Sex-based differences in multidimensional clinical assessments of early-abstinence crack cocaine users. PLoS ONE 2019, 14, e0218334. [Google Scholar] [CrossRef]
- Velasco Arias, S.; López Doriga, B.; Tourné García, M.; Calderó Bea, M.D.; Barceló Barceló, I.; Luna Rodríguez, C. Evaluación de una intervención biopsicosocial para el malestar de las mujeres en atención primaria. Feminismo/s 2007, 10, 111–131. [Google Scholar] [CrossRef]
- Aoki, J.; Inoue, A.; Okudaira, S. Two pathways for lysophosphatidic acid production. Biochim. Biophys. Acta-Mol. Cell Biol. Lipids 2008, 1781, 513–518. [Google Scholar] [CrossRef]
- Riaz, A.; Huang, Y.; Johansson, S. G-protein-coupled lysophosphatidic acid receptors and their regulation of AKT signaling. Int. J. Mol. Sci. 2016, 17, 215. [Google Scholar] [CrossRef]
- Choi, J.W.; Herr, D.R.; Noguchi, K.; Yung, Y.C.; Lee, C.W.; Mutoh, T.; Lin, M.E.; Teo, S.T.; Park, K.E.; Mosley, A.N.; et al. LPA receptors: Subtypes and biological actions. Annu. Rev. Pharmacol. Toxicol. 2010, 50, 157–186. [Google Scholar] [CrossRef]
- Baker, D.L.; Desiderio, D.M.; Miller, D.D.; Tolley, B.; Tigyi, G.J. Direct quantitative analysis of lysophosphatidic acid molecular species by stable isotope dilution electrospray lonization liquid chromatography-mass spectrometry. Anal. Biochem. 2001, 292, 287–295. [Google Scholar] [CrossRef]
- Sano, T.; Baker, D.; Virag, T.; Wada, A.; Yatomi, Y.; Kobayashi, T.; Igarashi, Y.; Tigyi, G. Multiple mechanisms linked to platelet activation result in lysophosphatidic acid and sphingosine 1-phosphate generation in blood. J. Biol. Chem. 2002, 277, 21197–21206. [Google Scholar] [CrossRef] [PubMed]
- Bandoh, K.; Aoki, J.; Taira, A.; Tsujimoto, M.; Arai, H.; Inoue, K. Lysophosphatidic acid (LPA) receptors of the EDG family are differentially activated by LPA species. Structure-activity relationship of cloned LPA receptors. FEBS Lett. 2000, 478, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Anliker, B.; Choi, J.W.; Lin, M.E.; Gardell, S.E.; Rivera, R.R.; Kennedy, G.; Chun, J. Lysophosphatidic acid (LPA) and its receptor, LPA1, influence embryonic schwann cell migration, myelination, and cell-to-axon segregation. Glia 2013, 61, 2009–2022. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Chun, J. Lysophospholipids and their receptors in the central nervous system. Biochim. Et Biophys. Acta -Mol. Cell Biol. Lipids 2013, 1831, 20–32. [Google Scholar] [CrossRef]
- García-Marchena, N.; Pizarro, N.; Pavón, F.J.; Martínez-Huélamo, M.; Flores-López, M.; Requena-Ocaña, N.; Araos, P.; Silva-Peña, D.; Suárez, J.; Santín, L.J.; et al. Potential association of plasma lysophosphatidic acid (LPA) species with cognitive impairment in abstinent alcohol use disorders outpatients. Sci. Rep. 2020, 10, 17163. [Google Scholar] [CrossRef]
- Flores-López, M.; García-Marchena, N.; Pavón-Morón, F.J.; Requena-Ocaña, N.; Sánchez-Marín, L.; Martín-Chaves, L.; García-Medina, M.; Pedraza, C.; Castilla-Ortega, E.; Ruiz, J.J.; et al. Plasma concentrations of lysophosphatidic acid and the expression of its receptors in peripheral blood mononuclear cells are altered in patients with cocaine use disorders. Transl. Psychiatry 2023, 13, 215. [Google Scholar] [CrossRef]
- Choi, J.H.; Jang, M.; Oh, S.; Nah, S.Y.; Cho, I.H. Multi-target protective effects of gintonin in 1-Methyl-4-phenyl-1,2,3,6-tetrahydropyridine-mediated model of parkinson’s disease via lysophosphatidic acid receptors. Front. Pharmacol. 2018, 9, 515. [Google Scholar] [CrossRef]
- Hwang, S.H.; Lee, B.H.; Choi, S.H.; Kim, H.J.; Jung, S.W.; Kim, H.S.; Jung, S.W.; Kim, H.S.; Shin, H.C.; Park, H.J.; et al. Gintonin, a novel ginseng-derived lysophosphatidic acid receptor ligand, stimulates neurotransmitter release. Neurosci Lett. 2015, 584, 356–361. [Google Scholar] [CrossRef]
- Kreek, M.J.; Levran, O.; Reed, B.; Schlussman, S.D.; Zhou, Y.; Butelman, E.R. Opiate addiction and cocaine addiction: Underlying molecular neurobiology and genetics. J. Clin. Investig. 2012, 122, 3387–3393. [Google Scholar] [CrossRef]
- Orio, L.; Pavón, F.; Blanco, E.; Serrano, A.; Araos, P.; Pedraz, M.; Rivera, P.; Calado, M.; Suárez, J.; de Fonseca, F.R.; et al. Lipid Transmitter Signaling as a New Target for Treatment of Cocaine Addiction: New Roles for Acylethanolamides and Lysophosphatidic Acid. Curr. Pharm. Des. 2013, 19, 7036–7049. [Google Scholar] [CrossRef]
- Flores-López, M.; García-Marchena, N.; Araos, P.; Requena-Ocaña, N.; Porras-Perales, O.; Torres-Galván, S.; Suarez, J.; Pizarro, N.; de la Torre, R.; Rubio, G.; et al. Sex Differences in Plasma Lysophosphatidic Acid Species in Patients with Alcohol and Cocaine Use Disorders. Brain Sci. 2022, 12, 588. [Google Scholar] [CrossRef] [PubMed]
- Bangasser, D.A.; Valentino, R.J. Sex differences in stress-related psychiatric disorders: Neurobiological perspectives. Front. Neuroendocrinol. 2014, 35, 303–319. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Kim, Y.K. Early Life Stress, Neuroinflammation, and Psychiatric Illness of Adulthood. Adv. Exp. Med. Biol. 2023, 105–134. [Google Scholar]
- Juruena, M.; Werne Baes, C.; Menezes, I.; Graeff, F. Early Life Stress in Depressive Patients: Role of Glucocorticoid and Mineralocorticoid Receptors and of Hypothalamic-Pituitary-Adrenal Axis Activity. Curr. Pharm. Des. 2015, 21, 1369–1378. [Google Scholar] [CrossRef]
- Yehuda, R.; Seckl, J. Minireview: Stress-related psychiatric disorders with low cortisol levels: A metabolic hypothesis. Endocrinology 2011, 152, 4496–4503. [Google Scholar] [CrossRef] [PubMed]
- Zorn, J.V.; Schür, R.R.; Boks, M.P.; Kahn, R.S.; Joëls, M.; Vinkers, C.H. Cortisol stress reactivity across psychiatric disorders: A systematic review and meta-analysis. Psychoneuroendocrinology 2017, 77, 25–36. [Google Scholar] [CrossRef]
- Messaoud, A.; Rym, M.; Wahiba, D.; Neffati, F.; Najjar, M.F.; Gobbi, G.; Manchia, M.; Valtorta, F.; Lotfi, G.; Comai, S. Investigation of the Relationship among Cortisol, Pro-inflammatory Cytokines, and the Degradation of Tryptophan into Kynurenine in Patients with Major Depression and Suicidal Behavior. Curr. Top. Med. Chem. 2021, 22, 2119–2125. [Google Scholar] [CrossRef]
- Sorgdrager, F.J.H.; Buning, J.W.; Bos, E.H.; Van Beek, A.P.; Kema, I.P. Hydrocortisone Affects Fatigue and Physical Functioning Through Metabolism of Tryptophan: A Randomized Controlled Trial. J. Clin. Endocrinol. Metab. 2018, 103, 3411–3419. [Google Scholar] [CrossRef]
- Messaoud, A.; Mensi, R.; Douki, W.; Neffati, F.; Najjar, M.F.; Gobbi, G.; Valtorta, F.; Gaha, L.; Comai, S. Reduced peripheral availability of tryptophan and increased activation of the kynurenine pathway and cortisol correlate with major depression and suicide. World J. Biol. Psychiatry 2019, 20, 703–711. [Google Scholar] [CrossRef]
- Songtachalert, T.; Roomruangwong, C.; Carvalho, A.F.; Bourin, M.; Maes, M. Anxiety Disorders: Sex Differences in Serotonin and Tryptophan Metabolism. Curr. Top. Med. Chem. 2018, 18, 1704–1715. [Google Scholar] [CrossRef]
- Lapin, I.P. Neurokynurenines (NEKY) as common neurochemical links of stress and anxiety. Adv. Exp. Med. Biol. 2003, 527, 121–125. [Google Scholar] [PubMed]
- Araos, P.; Vidal, R.; O’Shea, E.; Pedraz, M.; García-Marchena, N.; Serrano, A.; Suárez, J.; Castilla-Ortega, E.; Ruiz, J.J.; Campos-Cloute, R.; et al. Serotonin is the main tryptophan metabolite associated with psychiatric comorbidity in abstinent cocaine-addicted patients. Sci. Rep. 2019, 9, 16842. [Google Scholar] [CrossRef] [PubMed]
- Pati, S.; Angel, P.; Drake, R.R.; Wagner, J.J.; Cummings, B.S. Lipidomic changes in the rat hippocampus following cocaine conditioning, extinction, and reinstatement of drug-seeking. Brain Behav. 2019, 9, e01451. [Google Scholar] [CrossRef]
- Cummings, B.S.; Pati, S.; Sahin, S.; Scholpa, N.E.; Monian, P.; Trinquero, P.M.; Clark, J.K.; Wagner, J.J. Differential effects of cocaine exposure on the abundance of phospholipid species in rat brain and blood. Drug Alcohol Depend. 2015, 152, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Ladrón de Guevara-Miranda, D.; Moreno-Fernández, R.D.; Gil-Rodríguez, S.; Rosell-Valle, C.; Estivill-Torrús, G.; Serrano, A.; Pavón, F.J.; Rodríguez de Fonseca, F.; Santín, L.J.; Castilla-Ortega, E. Lysophosphatidic acid-induced increase in adult hippocampal neurogenesis facilitates the forgetting of cocaine-contextual memory. Addict. Biol. 2019, 24, 458–470. [Google Scholar] [CrossRef]
- Flores-López, M.; García-Marchena, N.; Pavon, F.J.; Lara, E.; Porras-Perales, O.; Araos, P.; Requena-Ocaña, N.; Torres-Galván, S.; Mañas-Padilla, M.C.; Rubio, G.; et al. Plasma concentrations of lysophosphatidic acid and autotaxin in abstinent patients with alcohol use disorder and comorbid liver disease. Biomedicines 2021, 9, 1207. [Google Scholar] [CrossRef]
- Michalczyk, A.; Budkowska, M.; Dołȩgowska, B.; Chlubek, D.; Safranow, K. Lysophosphatidic acid plasma concentrations in healthy subjects: Circadian rhythm and associations with demographic, anthropometric and biochemical parameters. Lipids Health Dis. 2017, 16, 140. [Google Scholar] [CrossRef]
- Hosogaya, S.; Yatomi, Y.; Nakamura, K.; Ohkawa, R.; Okubo, S.; Yokota, H.; Ohta, M.; Yamazaki, H.; Koike, T.; Ozaki, Y. Measurement of plasma lysophosphatidic acid concentration in healthy subjects: Strong correlation with lysophospholipase D activity. Ann. Clin. Biochem. 2008, 45, 364–368. [Google Scholar] [CrossRef]
- Rachakonda, V.P.; Reeves, V.L.; Aljammal, J.; Wills, R.C.; Trybula, J.S.; Delany, J.P.; Kienesberger, P.C.; Kershaw, E.E. Serum autotaxin is independently associated with hepatic steatosis in women with severe obesity. Obesity 2015, 23, 965–972. [Google Scholar] [CrossRef]
- Li, M.; Xiao, D.; Zhang, J.; Qu, H.; Yang, Y.; Yan, Y.; Liu, X.; Wang, J.; Liu, L.; Wang, J.; et al. Expression of LPA2 is associated with poor prognosis in human breast cancer and regulates HIF-1 expression and breast cancer cell growth. Oncol. Rep. 2016, 36, 3479–3487. [Google Scholar] [CrossRef]
- Mazzocca, A.; Schönauer, L.M.; De Nola, R.; Lippolis, A.; Marrano, T.; Loverro, M.; Sabbà, C.; Di Naro, E. Autotaxin is a novel molecular identifier of type I endometrial cancer. Med. Oncol. 2018, 35, 157. [Google Scholar] [CrossRef]
- de la Franier, B.; Thompson, M. Detection of the ovarian cancer biomarker lysophosphatidic acid in serum. Biosensors 2020, 10, 13. [Google Scholar] [CrossRef]
- Samet, S.; Fenton, M.C.; Nunes, E.; Greenstein, E.; Aharonovich, E.; Hasin, D. Effects of independent and substance-induced major depressive disorder on remission and relapse of alcohol, cocaine and heroin dependence. Addiction 2013, 108, 115–123. [Google Scholar] [CrossRef]
- Herrero, M.J.; Domingo-Salvany, A.; Torrens, M.; Brugal, M.T.; Gutierrez, F. Profile in young current regular users of cocaine. Subst. Use Misuse 2008, 43, 1378–1394. [Google Scholar] [CrossRef] [PubMed]
- Zubaran, C.; Foresti, K.; Thorell, M.R.; Franceschini, P.R. Anxiety symptoms in crack cocaine and inhalant users admitted to a psychiatric hospital in southern Brazil. Rev. Assoc. Med. Bras. 2013, 59, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Hess, A.R.B.; de Almeida, R.M.M. Female crack cocaine users under treatment at therapeutic communities in southern brazil: Characteristics, pattern of consumption, and psychiatric comorbidities. Trends Psychiatry Psychother. 2019, 41, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Griffin, E.A.; Melas, P.A.; Zhou, R.; Li, Y.; Mercado, P.; Kempadoo, K.A.; Stephenson, S.; Colnaghi, L.; Taylor, K.; Hu, M.C.; et al. Prior alcohol use enhances vulnerability to compulsive cocaine self-administration by promoting degradation of HDAC4 and HDAC5. Sci Adv. 2017, 3, e1701682. [Google Scholar] [CrossRef] [PubMed]
- Thalman, C.; Horta, G.; Qiao, L.; Endle, H.; Tegeder, I.; Cheng, H.; Laube, G.; Sigurdsson, T.; Hauser, M.J.; Tenzer, S.; et al. Synaptic phospholipids as a new target for cortical hyperexcitability and E/I balance in psychiatric disorders. Mol. Psychiatry 2018, 23, 1699–1710. [Google Scholar] [CrossRef]
- Krishnan, V.; Nestler, E.J. The molecular neurobiology of depression. Nature 2008, 455, 894–902. [Google Scholar] [CrossRef]
- Pedraza, C.; Sánchez-López, J.; Castilla-Ortega, E.; Rosell-Valle, C.; Zambrana-Infantes, E.; García-Fernández, M.; Rodriguez de Fonseca, F.; Chun, J.; Santín, L.J.; Estivill-Torrús, G. Fear extinction and acute stress reactivity reveal a role of LPA(1) receptor in regulating emotional-like behaviors. Brain Struct. Funct. 2014, 219, 1659–1672. [Google Scholar] [CrossRef]
- Moreno-Fernandez, R.D.; Tabbai, S.; Castilla-Ortega, E.; Perez-Martin, M.; Estivill-Torrus, G.; Rodriguez de Fonseca, F.; Santin, L.J.; Pedraza, C. Stress, Depression, Resilience and Ageing: A Role for the LPA-LPA1 Pathway. Curr. Neuropharmacol. 2017, 16, 271–283. [Google Scholar]
- Tabbai, S.; Moreno-Fernández, R.D.; Zambrana-Infantes, E.; Nieto-Quero, A.; Chun, J.; García-Fernández, M.; Estivill-Torrús, G.; Rodríguez de Fonseca, F.; Santín, L.J.; Oliveira, T.G.; et al. Effects of the LPA1 receptor deficiency and stress on the hippocampal LPA species in mice. Front. Mol. Neurosci. 2019, 12, 146. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Fernández, R.D.; Pérez-Martín, M.; Castilla-Ortega, E.; Rosell Del Valle, C.; García-Fernández, M.I.; Chun, J.; Estivill-Torrús, G.; Rodríguez de Fonseca, F.; Santín, L.J.; Pedraza, C. MaLPA1-null mice as an endophenotype of anxious depression. Transl. Psychiatry 2017, 7, e1077. [Google Scholar] [CrossRef] [PubMed]
- Reimherr, F.W.; Marchant, B.K.; Gift, T.E.; Steans, T.A. ADHD and Anxiety: Clinical Significance and Treatment Implications. Curr. Psychiatry Rep. 2017, 19, 109. [Google Scholar] [CrossRef]
- Sciberras, E.; Efron, D.; Patel, P.; Mulraney, M.; Lee, K.J.; Mihalopoulos, C.; Engel, L.; Rapee, R.M.; Anderson, V.; Nicholson, J.M.; et al. Does the treatment of anxiety in children with Attention-Deficit/Hyperactivity Disorder (ADHD) using cognitive behavioral therapy improve child and family outcomes? Protocol for a randomized controlled trial. BMC Psychiatry 2019, 19, 359. [Google Scholar] [CrossRef]
- Kordahji, H.; Ben-David, S.; Elkana, O. Attachment Anxiety Moderates the Association Between ADHD and Psychological Distress. Psychiatr. Q. 2021, 92, 1711–1724. [Google Scholar] [CrossRef]
- León-Barriera, R.; Ortegon, R.S.; Chaplin, M.M.; Modesto-Lowe, V. Treating ADHD and Comorbid Anxiety in Children: A Guide for Clinical Practice. Clin. Pediatr. 2023, 62, 39–46. [Google Scholar] [CrossRef]
- Castilla-Ortega, E.; Pavón, F.J.; Sánchez-Marín, L.; Estivill-Torrús, G.; Pedraza, C.; Blanco, E.; Suárez, J.; Santín, L.; Rodríguez de Fonseca, F.; Serrano, A. Both genetic deletion and pharmacological blockade of lysophosphatidic acid LPA1 receptor results in increased alcohol consumption. Neuropharmacology 2016, 103, 92–103. [Google Scholar] [CrossRef]
- Virkkunen, M.; Narvanen, S. Plasma insulin, tryptophan and serotonin levels during the glucose tolerance test among habitually violent and impulsive offenders. Neuropsychobiology 1987, 17, 19–23. [Google Scholar] [CrossRef]
- Virkkunen, M.; Ebeling, H.; Moilanen, I.; Tani, P.; Pennanen, S.; Liesivuori, J.; Tiihonen, J. Total plasma L-tryptophan, free L-tryptophan and competing amino acid levels in a homicidal male adolescent with conduct disorder. Acta Psychiatr. Scand. 2003, 108, 244–246. [Google Scholar] [CrossRef]
- Ma, L.; Nagai, J.; Chun, J.; Ueda, H. An LPA species (18:1 LPA) plays key roles in the self-amplification of spinal LPA production in the peripheral neuropathic pain model. Mol. Pain 2013, 9, 1744–8069. [Google Scholar] [CrossRef] [PubMed]
- Kuwajima, K.; Sumitani, M.; Kurano, M.; Kano, K.; Nishikawa, M.; Uranbileg, B.; Tsuchida, R.; Ogata, T.; Aoki, J.; Yatomi, Y.; et al. Lysophosphatidic acid is associated with neuropathic pain intensity in humans: An exploratory study. PLoS ONE. 2018, 13, e0207310. [Google Scholar] [CrossRef] [PubMed]
- Gustin, S.M.; Burke, L.A.; Peck, C.C.; Murray, G.M.; Henderson, L.A. Pain and Personality: Do Individuals with Different Forms of Chronic Pain Exhibit a Mutual Personality? Pain Pract. 2016, 16, 486–494. [Google Scholar] [CrossRef]
- Proctor, S.L.; Estroff, T.W.; Empting, L.D.; Shearer-Williams, S.; Hoffmann, N.G. Prevalence of substance use and psychiatric disorders in a highly select chronic pain population. J. Addict. Med. 2013, 7, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.Y.; Lee, J.W.; Lee, M.Y.; Kim, S.H.; Mok, H.J.; Ha, K.; Ahn, Y.M.; Kim, K.P. Serum lipidomic analysis for the discovery of biomarkers for major depressive disorder in drug-free patients. Psychiatry Res. 2018, 265, 174–182. [Google Scholar] [CrossRef]
- Gotoh, L.; Yamada, M.; Hattori, K.; Sasayama, D.; Noda, T.; Yoshida, S.; Kunugi, H.; Yamada, M. Lysophosphatidic acid levels in cerebrospinal fluid and plasma samples in patients with major depressive disorder. Heliyon 2019, 5, e01699. [Google Scholar] [CrossRef]
- Riya, S.; Sultana, S.; Daria, S.; Proma, M.A.; Bhuiyan, M.A.; Haque, M.A.; Islam, M.R. Evaluation of Serum Lysophosphatidic Acid and Lysophosphatidylcholine Levels in Major Depressive Disorder Patients. Cureus 2020, 12, e12388. [Google Scholar] [CrossRef]
- Tiihonen, J.; Virkkunen, M.; Räsänen, P.; Pennanen, S.; Sainio, E.L.; Callaway, J.; Halonen, P.; Liesivuori, J. Free L-tryptophan plasma levels in antisocial violent offenders. Psychopharmacology 2001, 157, 395–400. [Google Scholar] [CrossRef]
- Wilson, S.T.; Stanley, B.; Brent, D.A.; Oquendo, M.A.; Huang, Y.Y.; Haghighi, F.; Hodgkinson, C.A.; Mann, J.J. Interaction between tryptophan hydroxylase i polymorphisms and childhood abuse is associated with increased risk for borderline personality disorder in adulthood. Psychiatr. Genet. 2012, 22, 15. [Google Scholar] [CrossRef]
- Mercedes Perez-Rodriguez, M.M.; Weinstein, S.; New, A.S.; Bevilacqua, L.; Yuan, Q.; Zhou, Z.; Hodgkinson, C.; Goodman, M.; Koenigsberg, H.W.; Goldman, D. Tryptophan-hydroxylase 2 haplotype association with borderline personality disorder and aggression in a sample of patients with personality disorders and healthy controls. J. Psychiatr. Res. 2010, 44, 1075–1081. [Google Scholar] [CrossRef]
- Kanchanatawan, B.; Sirivichayakul, S.; Carvalho, A.F.; Anderson, G.; Galecki, P.; Maes, M. Depressive, anxiety and hypomanic symptoms in schizophrenia may be driven by tryptophan catabolite (TRYCAT) patterning of IgA and IgM responses directed to TRYCATs. Prog. Neuro-Psychopharmacol. Biol. Psychiatry. 2018, 80, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhang, M.; Luo, Y.; Ni, X.; Lu, H.; Wen, Y.; Fan, N. Preliminary comparative analysis of kynurenine pathway metabolites in chronic ketamine users, schizophrenic patients, and healthy controls. Hum. Psychopharmacol. 2020, 35, e2738. [Google Scholar] [CrossRef] [PubMed]
- Kadriu, B.; Farmer, C.A.; Yuan, P.; Park, L.T.; Deng, Z.D.; Moaddel, R.; Henter, I.D.; Shovestul, B.; Ballard, E.D.; Kraus, C.; et al. The kynurenine pathway and bipolar disorder: Intersection of the monoaminergic and glutamatergic systems and immune response. Mol. Psychiatry 2021, 26, 4085–4095. [Google Scholar] [CrossRef] [PubMed]
- Milaneschi, Y.; Allers, K.A.; Beekman, A.T.F.; Giltay, E.J.; Keller, S.; Schoevers, R.A.; Süssmuth, S.D.; Niessen, H.G.; Penninx, B.W.J.H. The association between plasma tryptophan catabolites and depression: The role of symptom profiles and inflammation. Brain Behav. Immun. 2021, 97, 167–175. [Google Scholar] [CrossRef]
- Singh, R.; Savitz, J.; Teague, T.K.; Polanski, D.W.; Mayer, A.R.; Bellgowan, P.S.; Meier, T.B. Mood symptoms correlate with kynurenine pathway metabolites following sports-related concussion. J. Neurol. Neurosurg. Psychiatry 2016, 87, 670–675. [Google Scholar] [CrossRef]
- Aarsland, T.I.M.; Landaas, E.T.; Hegvik, T.A.; Ulvik, A.; Halmøy, A.; Ueland, P.M.; Haavik, J. Serum concentrations of kynurenines in adult patients with attention-deficit hyperactivity disorder (ADHD): A case-control study. Behav. Brain Funct. 2015, 11, 36. [Google Scholar] [CrossRef]
- Torrens, M.; Serrano, D.; Astals, M.; Pérez-Domínguez, G.; Martín-Santos, R. Diagnosing comorbid psychiatric disorders in substance abusers: Validity of the Spanish versions of the psychiatric research interview for substance and mental disorders and the structured clinical interview for DSM-IV. Am. J. Psychiatry 2004, 161, 1231–1237. [Google Scholar] [CrossRef]
- Hasin, D.; Hatzenbuehler, M.L.; Keyes, K.; Ogburn, E. Substance use disorders: Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) and International Classification of Diseases, tenth edition (ICD-10). Addiction 2006, 101 (Suppl. 1), 59–75. [Google Scholar] [CrossRef]





| Total Sample N = 148 | |||||
|---|---|---|---|---|---|
| Variables | Control Group N = 60 | CUD Group N = 88 | Statistic | p-Value | |
| Age 1 (Mean ± SD) | Years | 37.52 ± 1.20 | 37 ± 8.43 | 2267.500 | 0.143 |
| Body Mass Index 1 (Mean ± SD) | kg/m2 | 25.65 ± 3.51 | 25.98 ± 4.80 | 2582.500 | 0.991 |
| Sex 2 [N (%)] | Women Men | 10 (16.7) 50 (83.3) | 14 (15.9) 74 (84.1) | 0.015 | 0.902 |
| Education Degree 2 [N (%)] | Elementary Secondary University | 1 (1.70) 35 (58.30) 24 (40) | 17 (19.30) 58 (65.90) 13 (14.80) | 18.547 | <0.001 |
| Occupation 2 [N (%)] | Employed Unemployed Other | 59 (98.30) - 1 (1.7) | 35 (39.80) 7 (8) 46 (52.3) | 49.500 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Requena-Ocaña, N.; Flores-López, M.; García-Marchena, N.; Pavón-Morón, F.J.; Pedraza, C.; Wallace, A.; Castilla-Ortega, E.; Rodríguez de Fonseca, F.; Serrano, A.; Araos, P. Plasma Lysophosphatidic Acid Concentrations in Sex Differences and Psychiatric Comorbidity in Patients with Cocaine Use Disorder. Int. J. Mol. Sci. 2023, 24, 15586. https://doi.org/10.3390/ijms242115586
Requena-Ocaña N, Flores-López M, García-Marchena N, Pavón-Morón FJ, Pedraza C, Wallace A, Castilla-Ortega E, Rodríguez de Fonseca F, Serrano A, Araos P. Plasma Lysophosphatidic Acid Concentrations in Sex Differences and Psychiatric Comorbidity in Patients with Cocaine Use Disorder. International Journal of Molecular Sciences. 2023; 24(21):15586. https://doi.org/10.3390/ijms242115586
Chicago/Turabian StyleRequena-Ocaña, Nerea, María Flores-López, Nuria García-Marchena, Francisco J. Pavón-Morón, Carmen Pedraza, Agustín Wallace, Estela Castilla-Ortega, Fernando Rodríguez de Fonseca, Antonia Serrano, and Pedro Araos. 2023. "Plasma Lysophosphatidic Acid Concentrations in Sex Differences and Psychiatric Comorbidity in Patients with Cocaine Use Disorder" International Journal of Molecular Sciences 24, no. 21: 15586. https://doi.org/10.3390/ijms242115586