
Metformin Treatment of Hidradenitis Suppurativa: Effect on Metabolic Parameters, Inflammation, Cardiovascular Risk Biomarkers, and Immune Mediators
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Demographics
2.2. Metformin Dosing, Duration, and Response (n = 20)
2.3. Other Medications for the Management of HS
2.4. Metabolic Parameters
2.4.1. BMI and Waist Circumference
2.4.2. Blood Pressure
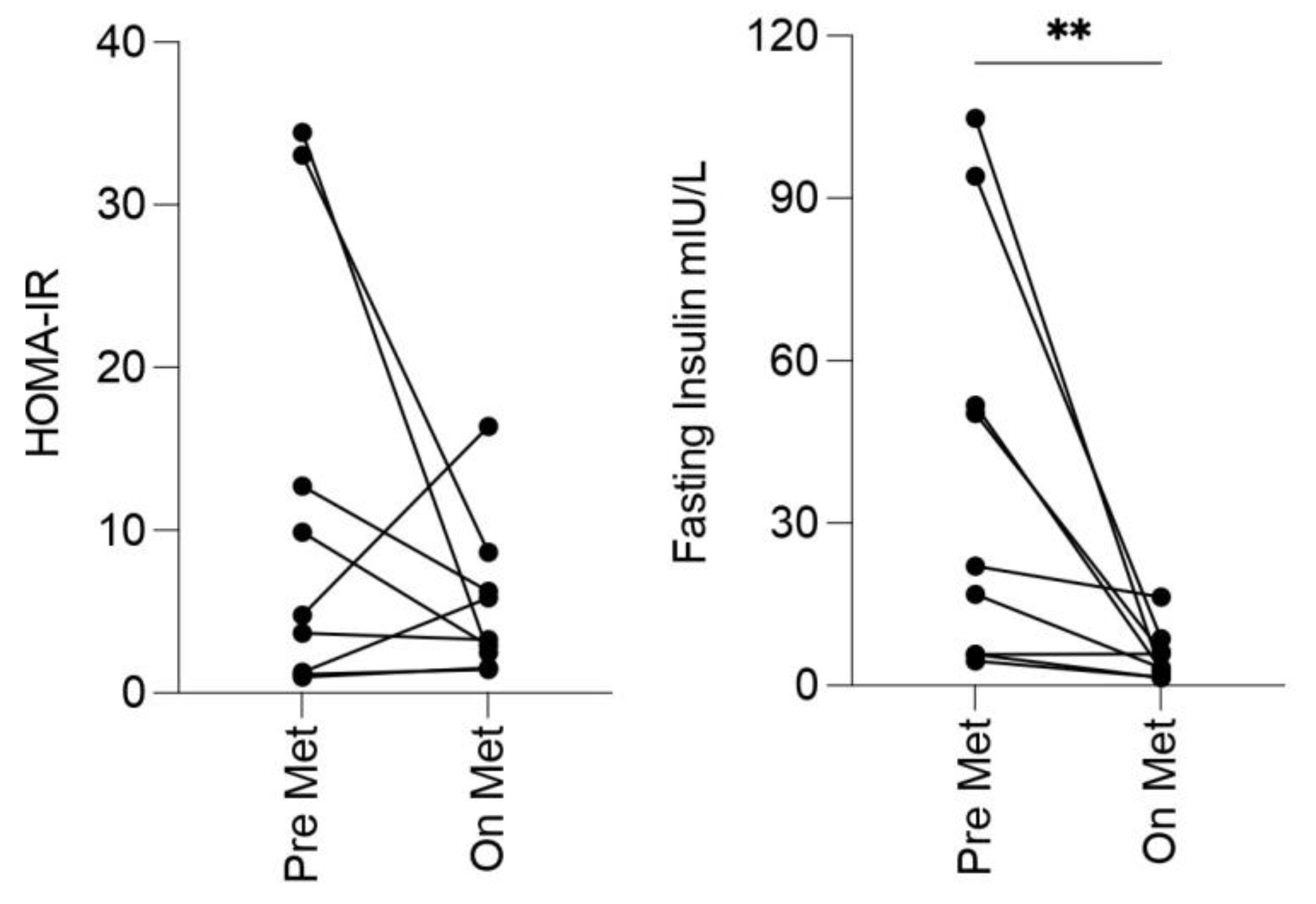
2.4.3. Insulin Resistance
2.4.4. Metabolic Syndrome
2.5. C-Reactive Protein (CRP)
2.6. Cardiovascular Disease Biomarkers
2.7. Serum Cytokines and Chemokines
2.8. Adipokines
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sabat, R.; Jemec, G.B.E.; Matusiak, L.; Kimball, A.B.; Prens, E.; Wolk, K. Hidradenitis suppurativa. Nat. Rev. Dis. Primers. 2020, 6, 18. [Google Scholar] [CrossRef]
- Vossen, A.R.; van der Zee, H.; Prens, E. Hidradenitis Suppurativa: A Systematic Review Integrating Inflammatory Pathways Into a Cohesive Pathogenic Model. Front. Immunol. 2019, 9, 2965. [Google Scholar] [CrossRef] [Green Version]
- Sartorius, K.; Emtestam, L.; Jemec, G.B.; Lapins, J. Objective scoring of hidradenitis suppurativa reflecting the role of tobacco smoking and obesity. Br. J. Dermatol. 2009, 161, 831–839. [Google Scholar] [CrossRef]
- Kromann, C.B.; Ibler, K.S.; Kristiansen, V.B.; Jemec, G.B. The influence of body weight on the prevalence and severity of hidradenitis suppurativa. Acta Derm. -Venereol. 2014, 94, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Boer, J. Resolution of hidradenitis suppurativa after weight loss by dietary measures, especially on frictional locations. J. Eur. Acad. Derm. Venereol. 2016, 30, 895–896. [Google Scholar] [CrossRef] [PubMed]
- Revuz, J.E.; Canoui-Poitrine, F.; Wolkenstein, P.; Viallette, C.; Gabison, G.; Pouget, F.; Poli, F.; Faye, O.; Roujeau, J.C.; Bonnelye, G.; et al. Prevalence and factors associated with hidradenitis suppurativa: Results from two case-control studies. J. Am. Acad. Dermatol. 2008, 59, 596–601. [Google Scholar] [CrossRef]
- Vazquez, B.G.; Alikhan, A.; Weaver, A.L.; Wetter, D.A.; Davis, M.D. Incidence of hidradenitis suppurativa and associated factors: A population-based study of Olmsted County, Minnesota. J. Investig. Dermatol. 2013, 133, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowley, J.J.; Mekkes, J.R.; Zouboulis, C.C.; Scheinfeld, N.; Kimball, A.; Sundaram, M.; Gu, Y.; Okun, M.M.; Kerdel, F. Association of hidradenitis suppurativa disease severity with increased risk for systemic comorbidities. Br. J. Dermatol. 2014, 171, 1561–1565. [Google Scholar] [CrossRef] [Green Version]
- Hughes, R. Immune Dysregulation and Metabolic Dysfunction in Hidradenitis Suppurativa. Master’s Thesis, Trinity College Dublin, Dublin, Ireland, 2015. [Google Scholar]
- Jennings, L.; Hambly, R.; Hughes, R.; Moriarty, B.; Kirby, B. Metformin use in hidradenitis suppurativa. J. Dermatolog. Treat. 2020, 31, 261–263. [Google Scholar] [CrossRef] [PubMed]
- Vilanova, I.; Hernandez, J.L.; Mata, C.; Duran, C.; Garcia-Unzueta, M.T.; Portilla, V.; Fuentevilla, P.; Corrales, A.; Gonzalez-Vela, M.C.; Gonzalez-Gay, M.A.; et al. Insulin resistance in hidradenitis suppurativa: A case-control study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 820–824. [Google Scholar] [CrossRef] [Green Version]
- Gold, D.A.; Reeder, V.J.; Mahan, M.G.; Hamzavi, I.H. The prevalence of metabolic syndrome in patients with hidradenitis suppurativa. J. Am. Acad. Dermatol. 2014, 70, 699–703. [Google Scholar] [CrossRef] [PubMed]
- Sabat, R.; Chanwangpong, A.; Schneider-Burrus, S.; Metternich, D.; Kokolakis, G.; Kurek, A.; Philipp, S.; Uribe, D.; Wolk, K.; Sterry, W. Increased prevalence of metabolic syndrome in patients with acne inversa. PLoS ONE 2012, 7, e31810. [Google Scholar] [CrossRef]
- Miller, I.M.; Ellervik, C.; Vinding, G.R.; Zarchi, K.; Ibler, K.S.; Knudsen, K.M.; Jemec, G.B. Association of metabolic syndrome and hidradenitis suppurativa. JAMA Dermatol. 2014, 150, 1273–1280. [Google Scholar] [CrossRef] [Green Version]
- Mintoff, D.; Benhadou, F.; Pace, N.P.; Frew, J.W. Metabolic syndrome and hidradenitis suppurativa: Epidemiological, molecular, and therapeutic aspects. Int. J. Dermatol. 2021, 61, 1175–1186. [Google Scholar] [CrossRef]
- Jimenez-Gallo, D.; de la Varga-Martinez, R.; Ossorio-Garcia, L.; Albarran-Planelles, C.; Rodriguez, C.; Linares-Barrios, M. The Clinical Significance of Increased Serum Proinflammatory Cytokines, C-Reactive Protein, and Erythrocyte Sedimentation Rate in Patients with Hidradenitis Suppurativa. Mediat. Inflamm. 2017, 2017, 2450401. [Google Scholar] [CrossRef]
- Kanni, T.; Tzanetakou, V.; Savva, A.; Kersten, B.; Pistiki, A.; van de Veerdonk, F.L.; Netea, M.G.; van der Meer, J.W.; Giamarellos-Bourboulis, E.J. Compartmentalized Cytokine Responses in Hidradenitis Suppurativa. PLoS ONE 2015, 10, e0130522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zouboulis, C.C.; Nogueira da Costa, A. Drug repurposing through drug-gene interaction profiles for hidradenitis suppurativa/acne inversa treatment. J. Eur. Acad. Dermatol. Venereol. 2020, 35, e251–e254. [Google Scholar] [CrossRef]
- Garg, A.; Malviya, N.; Strunk, A.; Wright, S.; Alavi, A.; Alhusayen, R.; Alikhan, A.; Daveluy, S.D.; Delorme, I.; Goldfarb, N.; et al. Comorbidity screening in hidradenitis suppurativa: Evidence-based recommendations from the US and Canadian Hidradenitis Suppurativa Foundations. J. Am. Acad. Dermatol. 2021, 86, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Ingram, J.R.; Collier, F.; Brown, D.; Burton, T.; Burton, J.; Chin, M.F.; Desai, N.; Goodacre, T.E.E.; Piguet, V.; Pink, A.E.; et al. British Association of Dermatologists guidelines for the management of hidradenitis suppurativa (acne inversa) 2018. Br. J. Dermatol. 2019, 180, 1009–1017. [Google Scholar] [CrossRef] [Green Version]
- Scheinfeld, N. Hidradenitis suppurativa: A practical review of possible medical treatments based on over 350 hidradenitis patients. Dermatol. Online J. 2013, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Zouboulis, C.C.; Desai, N.; Emtestam, L.; Hunger, R.E.; Ioannides, D.; Juhasz, I.; Lapins, J.; Matusiak, L.; Prens, E.P.; Revuz, J.; et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 619–644. [Google Scholar] [CrossRef] [PubMed]
- Gulliver, W.; Zouboulis, C.C.; Prens, E.; Jemec, G.B.; Tzellos, T. Evidence-based approach to the treatment of hidradenitis suppurativa/acne inversa, based on the European guidelines for hidradenitis suppurativa. Rev. Endocr. Metab. Disord. 2016, 17, 343–351. [Google Scholar] [CrossRef] [Green Version]
- van der Zee, H.H.; Gulliver, W.P. Medical Treatments of Hidradenitis Suppurativa: More Options, Less Evidence. Dermatol. Clin. 2016, 34, 91–96. [Google Scholar] [CrossRef] [PubMed]
- van Rappard, D.C.; Mekkes, J.R.; Tzellos, T. Randomized Controlled Trials for the Treatment of Hidradenitis Suppurativa. Dermatol. Clin. 2016, 34, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Verdolini, R.; Clayton, N.; Smith, A.; Alwash, N.; Mannello, B. Metformin for the treatment of hidradenitis suppurativa: A little help along the way. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Blok, J.L. Interventions for hidradenitis suppurativa: An important step towards evidence-based medicine. Br. J. Dermatol. 2016, 174, 953–954. [Google Scholar] [CrossRef] [PubMed]
- Balik, E.; Eren, T.; Bulut, T.; Buyukuncu, Y.; Bugra, D.; Yamaner, S. Surgical approach to extensive hidradenitis suppurativa in the perineal/perianal and gluteal regions. World J. Surg. 2009, 33, 481–487. [Google Scholar] [CrossRef]
- Jennings, L.; Nestor, L.; Molloy, O.; Hughes, R.; Moriarty, B.; Kirby, B. The treatment of hidradenitis suppurativa with the glucagon-like peptide-1 agonist liraglutide. Br. J. Dermatol. 2017, 177, 858–859. [Google Scholar] [CrossRef]
- Medicines.ie. Humira 40mg Solution for Injection in Pre-Filled Pen-Summary of Product Characteristics (SPC) 2021. Available online: https://www.medicines.ie/medicines/humira-40mg-solution-for-injection-in-pre-filled-pen-32384/spc (accessed on 31 October 2021).
- Kimball, A.B.; Okun, M.M.; Williams, D.A.; Gottlieb, A.B.; Papp, K.A.; Zouboulis, C.C.; Armstrong, A.W.; Kerdel, F.; Gold, M.H.; Forman, S.B.; et al. Two Phase 3 Trials of Adalimumab for Hidradenitis Suppurativa. N. Engl. J. Med. 2016, 375, 422–434. [Google Scholar] [CrossRef]
- Kimball, A.; Jemec, G.; Armstrong, A.; Forman, S.; Shu, L.; Gu, Y.; Williams, D.; O’kun, M. Evaluating Optimal Medium-Term Dosing Strategy for Adalimumab in PAtients with Moderate-to-Severe- Hidradenitis Suppurativa Based on Analysis of Integrated Results from the PIONEER I and II Phase 3, Randomized, Placebo-Controlled Trials. In Proceedings of the 73rd American Academy of Dermatology Congress, San Francisco, CA, USA, 20–24 March 2015. [Google Scholar]
- Kimball, A.B.; Sobell, J.M.; Zouboulis, C.C.; Gu, Y.; Williams, D.A.; Sundaram, M.; Teixeira, H.D.; Jemec, G.B. HiSCR (Hidradenitis Suppurativa Clinical Response): A novel clinical endpoint to evaluate therapeutic outcomes in patients with hidradenitis suppurativa from the placebo-controlled portion of a phase 2 adalimumab study. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 989–994. [Google Scholar] [CrossRef] [Green Version]
- Zouboulis, C.C.; Tzellos, T.; Kyrgidis, A.; Jemec, G.B.E.; Bechara, F.G.; Giamarellos-Bourboulis, E.J.; Ingram, J.R.; Kanni, T.; Karagiannidis, I.; Martorell, A.; et al. Development and validation of the International Hidradenitis Suppurativa Severity Score System (IHS4), a novel dynamic scoring system to assess HS severity. Br. J. Dermatol. 2017, 177, 1401–1409. [Google Scholar] [CrossRef] [Green Version]
- Alikhan, A.; Sayed, C.; Alavi, A.; Alhusayen, R.; Brassard, A.; Burkhart, C.; Crowell, K.; Eisen, D.B.; Gottlieb, A.B.; Hamzavi, I.; et al. North American clinical management guidelines for hidradenitis suppurativa: A publication from the United States and Canadian Hidradenitis Suppurativa Foundations: Part II: Topical, intralesional, and systemic medical management. J. Am. Acad. Dermatol. 2019, 81, 91–101. [Google Scholar] [CrossRef] [Green Version]
- van der Zee, H.H.; van de Bunte, M.; van Straalen, K.R. Management of mild hidradenitis suppurativa: Our greatest challenge yet. Br. J. Dermatol. 2022, 186, 355–356. [Google Scholar] [CrossRef]
- Hambly, R.; Kirby, B. Prolonged clindamycin and rifampicin for hidradenitis suppurativa: Resist to prevent resistance. Br. J. Dermatol. 2019, 180, 702–703. [Google Scholar] [CrossRef]
- Gierek, M.; Ochala-Gierek, G.; Kitala, D.; Labus, W.; Bergler-Czop, B. Hidradenitis suppurativa: Bacteriological study in surgical treatment. Adv. Dermatol. Allergol. /Postępy Dermatol. Alergol. 2022, 39, 1101–1105. [Google Scholar] [CrossRef]
- Medicines.ie. Metformin (Glucophage) 500 mg Tablets-Summary of Product Characteristics (SPC) 2018. Available online: https://www.medicines.ie/medicines/glucophage-500mg-film-coated-tablets-32305/ (accessed on 8 April 2019).
- Rena, G.; Hardie, D.G.; Pearson, E.R. The mechanisms of action of metformin. Diabetologia 2017, 60, 1577–1585. [Google Scholar] [CrossRef] [Green Version]
- Johnson, N.P. Metformin use in women with polycystic ovary syndrome. Ann. Transl. Med. 2014, 2, 56. [Google Scholar]
- Pu, R.; Shi, D.; Gan, T.; Ren, X.; Ba, Y.; Huo, Y.; Bai, Y.; Zheng, T.; Cheng, N. Effects of metformin in obesity treatment in different populations: A meta-analysis. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820926000. [Google Scholar] [CrossRef]
- Rask Larsen, J.; Dima, L.; Correll, C.U.; Manu, P. The pharmacological management of metabolic syndrome. Expert. Rev. Clin. Pharmacol. 2018, 11, 397–410. [Google Scholar] [CrossRef]
- Gharib, M.; Elbaz, W.; Darweesh, E.; Sabri, N.A.; Shawki, M.A. Efficacy and Safety of Metformin Use in Rheumatoid Arthritis: A Randomized Controlled Study. Front. Pharmacol. 2021, 12, 726490. [Google Scholar] [CrossRef]
- Chang, J.E.; Choi, M.S. A Molecular Perspective on the Potential Benefits of Metformin for the Treatment of Inflammatory Skin Disorders. Int. J. Mol. Sci. 2020, 21, 8960. [Google Scholar] [CrossRef] [PubMed]
- Melnik, B.C.; Schmitz, G. Metformin: An Inhibitor of mTORC1 Signaling. J. Endocrinol. Diabetes Obes. 2014, 2, 1029. [Google Scholar]
- Bharath, L.P.; Nikolajczyk, B.S. The intersection of metformin and inflammation. Am. J. Physiol. Cell Physiol. 2021, 320, C873–C879. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Myers, R.; Li, Y.; Chen, Y.; Shen, X.; Fenyk-Melody, J.; Wu, M.; Ventre, J.; Doebber, T.; Fujii, N.; et al. Role of AMP-activated protein kinase in mechanism of metformin action. J. Clin. Investig. 2001, 108, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Howell, J.J.; Hellberg, K.; Turner, M.; Talbott, G.; Kolar, M.J.; Ross, D.S.; Hoxhaj, G.; Saghatelian, A.; Shaw, R.J.; Manning, B.D. Metformin Inhibits Hepatic mTORC1 Signaling via Dose-Dependent Mechanisms Involving AMPK and the TSC Complex. Cell Metab. 2017, 25, 463–471. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Yang, F.; Ma, W.; Sun, Q. Metformin inhibits proliferation and proinflammatory cytokines of human keratinocytes in vitro via mTOR-signaling pathway. Pharm. Biol. 2016, 54, 1173–1178. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, L.; Cregan, S.; Biniecka, M.; Cunningham, C.; Veale, D.J.; Kane, D.J.; Fearon, U.; Mullan, R.H. Insulin-Resistant Pathways Are Associated With Disease Activity in Rheumatoid Arthritis and Are Subject to Disease Modification Through Metabolic Reprogramming: A Potential Novel Therapeutic Approach. Arthritis Rheumatol. 2020, 72, 896–902. [Google Scholar] [CrossRef]
- Kang, K.Y.; Kim, Y.K.; Yi, H.; Kim, J.; Jung, H.R.; Kim, I.J.; Cho, J.H.; Park, S.H.; Kim, H.Y.; Ju, J.H. Metformin downregulates Th17 cells differentiation and attenuates murine autoimmune arthritis. Int. Immunopharmacol. 2013, 16, 85–92. [Google Scholar] [CrossRef]
- Park, M.J.; Lee, S.Y.; Moon, S.J.; Son, H.J.; Lee, S.H.; Kim, E.K.; Byun, J.K.; Shin, D.Y.; Park, S.H.; Yang, C.W.; et al. Metformin attenuates graft-versus-host disease via restricting mammalian target of rapamycin/signal transducer and activator of transcription 3 and promoting adenosine monophosphate-activated protein kinase-autophagy for the balance between T helper 17 and Tregs. Transl. Res. 2016, 173, 115–130. [Google Scholar]
- Lee, S.Y.; Lee, S.H.; Yang, E.J.; Kim, E.K.; Kim, J.K.; Shin, D.Y.; Cho, M.L. Metformin Ameliorates Inflammatory Bowel Disease by Suppression of the STAT3 Signaling Pathway and Regulation of the between Th17/Treg Balance. PLoS ONE 2015, 10, e0135858. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Tian, T.; Gao, J.; Liu, X.; Hou, H.; Cao, R.; Li, B.; Quan, M.; Guo, L. Metformin ameliorates the development of experimental autoimmune encephalomyelitis by regulating T helper 17 and regulatory T cells in mice. J. Neuroimmunol. 2016, 292, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Kurzthaler, D.; Hadziomerovic-Pekic, D.; Wildt, L.; Seeber, B.E. Metformin induces a prompt decrease in LH-stimulated testosterone response in women with PCOS independent of its insulin-sensitizing effects. Reprod. Biol. Endocrinol. 2014, 12, 98. [Google Scholar] [CrossRef] [Green Version]
- Tzellos, T.; Zouboulis, C.C.; Gulliver, W.; Cohen, A.D.; Wolkenstein, P.; Jemec, G.B. Cardiovascular disease risk factors in patients with hidradenitis suppurativa: A systematic review and meta-analysis of observational studies. Br. J. Dermatol. 2015, 173, 1142–1155. [Google Scholar] [CrossRef]
- Lean, M.E.; Han, T.S.; Morrison, C.E. Waist circumference as a measure for indicating need for weight management. BMJ 1995, 311, 158–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Heart Foundation. Why Your Waist Size Matters. Available online: https://www.bhf.org.uk/informationsupport/heart-matters-magazine/medical/measuring-your-waist (accessed on 13 October 2021).
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [PubMed]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhu, L.; Hu, K.; Tang, Y.; Zeng, X.; Liu, J.; Xu, J. Effects of metformin treatment on serum levels of C-reactive protein and interleukin-6 in women with polycystic ovary syndrome: A meta-analysis: A PRISMA-compliant article. Medicine 2017, 96, e8183. [Google Scholar] [CrossRef]
- Jorgensen, A.R.; Yao, Y.; Ghazanfar, M.N.; Ring, H.C.; Thomsen, S.F. Burden, predictors and temporal relationships of comorbidities in patients with hidradenitis suppurativa: A hospital-based cohort study. J. Eur. Acad. Dermatol. Venereol. 2019, 34, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Gislason, G.H.; Hansen, P.R. Risk of Major Adverse Cardiovascular Events and All-Cause Mortality in Patients With Hidradenitis Suppurativa. JAMA Dermatol. 2016, 152, 429–434. [Google Scholar] [CrossRef] [Green Version]
- Silvestre-Roig, C.; Braster, Q.; Ortega-Gomez, A.; Soehnlein, O. Neutrophils as regulators of cardiovascular inflammation. Nat. Rev. Cardiol. 2020, 17, 327–340. [Google Scholar] [CrossRef]
- Hu, D.; Wang, Z.; Wang, Y.; Liang, C. Targeting Macrophages in Atherosclerosis. Curr. Pharm. Biotechnol. 2021, 22, 2008–2018. [Google Scholar] [CrossRef]
- Nording, H.M.; Seizer, P.; Langer, H.F. Platelets in inflammation and atherogenesis. Front. Immunol. 2015, 6, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunez, J.; Sastre, C.; D’Ascoli, G.; Ruiz, V.; Bonanad, C.; Minana, G.; Valero, E.; Garcia-Blas, S.; Mollar, A.; Villaescusa, A.; et al. Relation of Low Lymphocyte Count to Frailty and its Usefulness as a Prognostic Biomarker in Patients >65 Years of Age With Acute Coronary Syndrome. Am. J. Cardiol. 2020, 125, 1033–1038. [Google Scholar] [CrossRef]
- Delgado, G.E.; Kramer, B.K.; Marz, W.; Hellstern, P.; Kleber, M.E.; Leipe, J. Immune Status and Mortality in Smokers, Ex-smokers, and Never-Smokers: The Ludwigshafen Risk and Cardiovascular Health Study. Nicotine Tob. Res. 2021, 23, 1191–1198. [Google Scholar] [CrossRef]
- Sager, H.B.; Koenig, W. Immune cell-based cardiovascular risk assessment: Spotlight on the neutrophil-lymphocyte ratio. Eur. Heart J. 2021, 42, 904–906. [Google Scholar] [CrossRef]
- Pujani, M.; Chauhan, V.; Singh, K.; Rastogi, S.; Agarwal, C.; Gera, K. The effect and correlation of smoking with platelet indices, neutrophil lymphocyte ratio and platelet lymphocyte ratio. Hematol. Transfus. Cell Ther. 2021, 43, 424–429. [Google Scholar] [CrossRef]
- Ji, H.; Li, Y.; Fan, Z.; Zuo, B.; Jian, X.; Li, L.; Liu, T. Monocyte/lymphocyte ratio predicts the severity of coronary artery disease: A syntax score assessment. BMC Cardiovasc. Disord. 2017, 17, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.Y.; Zhao, Q.; Liu, Z.S.; Zhang, C.Y.; Yang, J.; Meng, K. Relationship between monocyte/lymphocyte ratio and non-culprit plaque vulnerability in patients with acute coronary syndrome: An optical coherence tomography study. Medicine 2020, 99, e21562. [Google Scholar] [CrossRef]
- Forget, P.; Khalifa, C.; Defour, J.P.; Latinne, D.; Van Pel, M.C.; De Kock, M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res. Notes 2017, 10, 12. [Google Scholar] [CrossRef] [Green Version]
- Cetinarslan, T.; Turel Ermertcan, A.; Ozyurt, B.; Gunduz, K. Evaluation of the laboratory parameters in hidradenitis suppurativa: Can we use new inflammatory biomarkers? Dermatol. Ther. 2021, 34, e14835. [Google Scholar] [CrossRef]
- Chen, H.; Li, M.; Liu, L.; Dang, X.; Zhu, D.; Tian, G. Monocyte/lymphocyte ratio is related to the severity of coronary artery disease and clinical outcome in patients with non-ST-elevation myocardial infarction. Medicine 2019, 98, e16267. [Google Scholar] [CrossRef] [PubMed]
- Amoani, B.; Sakyi, S.A.; Mantey, R.; Laing, E.F.; Ephraim, R.D.; Sarfo-Katanka, O.; Koffie, S.; Obese, E.; Afranie, B.O. Increased metformin dosage suppresses pro-inflammatory cytokine levels in systemic circulation and might contribute to its beneficial effects. J. Immunoass. Immunochem. 2021, 42, 252–264. [Google Scholar] [CrossRef]
- Malara, A.; Hughes, R.; Jennings, L.; Sweeney, C.M.; Lynch, M.; Awdeh, F.; Timoney, I.; Tobin, A.M.; Lynam-Loane, K.; Tobin, L.; et al. Adipokines are dysregulated in patients with hidradenitis suppurativa. Br. J. Dermatol. 2018, 178, 792–793. [Google Scholar] [CrossRef]
- Gonzalez-Lopez, M.A.; Vilanova, I.; Ocejo-Vinals, G.; Arlegui, R.; Navarro, I.; Guiral, S.; Mata, C.; Perez-Paredes, M.G.; Portilla, V.; Corrales, A.; et al. Circulating levels of adiponectin, leptin, resistin and visfatin in non-diabetics patients with hidradenitis suppurativa. Arch. Dermatol. Res. 2020, 312, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Zhou, M.; Zhou, G.; Zhu, Q.; Li, W. Effect of metformin on adiponectin in PCOS: A meta-analysis and a systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 267, 61–67. [Google Scholar] [CrossRef]
- Dludla, P.V.; Nkambule, B.B.; Mazibuko-Mbeje, S.E.; Nyambuya, T.M.; Mxinwa, V.; Mokgalaboni, K.; Ziqubu, K.; Cirilli, I.; Marcheggiani, F.; Louw, J.; et al. Adipokines as a therapeutic target by metformin to improve metabolic function: A systematic review of randomized controlled trials. Pharmacol. Res. 2021, 163, 105219. [Google Scholar] [CrossRef]
- Canoui-Poitrine, F.; Le Thuaut, A.; Revuz, J.E.; Viallette, C.; Gabison, G.; Poli, F.; Pouget, F.; Wolkenstein, P.; Bastuji-Garin, S. Identification of three hidradenitis suppurativa phenotypes: Latent class analysis of a cross-sectional study. J. Investig. Dermatol. 2013, 133, 1506–1511. [Google Scholar] [CrossRef] [Green Version]
- van der Zee, H.H.; Jemec, G.B. New insights into the diagnosis of hidradenitis suppurativa: Clinical presentations and phenotypes. J. Am. Acad. Dermatol. 2015, 73, S23–S26. [Google Scholar] [CrossRef]
- Klein, S.; Allison, D.B.; Heymsfield, S.B.; Kelley, D.E.; Leibel, R.L.; Nonas, C.; Kahn, R.; Association for Weight Management and Obesity Prevention; NAASO, The Obesity Society; American Society for Nutrition; et al. Waist circumference and cardiometabolic risk: A consensus statement from shaping America’s health: Association for Weight Management and Obesity Prevention; NAASO, the Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Diabetes Care 2007, 30, 1647–1652. [Google Scholar] [PubMed] [Green Version]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model. Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Garg, A.; Neuren, E.; Strunk, A. Hidradenitis Suppurativa Is Associated with Polycystic Ovary Syndrome: A Population-Based Analysis in the United States. J. Investig. Dermatol. 2018, 138, 1288–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legro, R.S.; Kunselman, A.R.; Dodson, W.C.; Dunaif, A. Prevalence and predictors of risk for type 2 diabetes mellitus and impaired glucose tolerance in polycystic ovary syndrome: A prospective, controlled study in 254 affected women. J. Clin. Endocrinol. Metab. 1999, 84, 165–169. [Google Scholar] [CrossRef] [PubMed]
- DeUgarte, C.M.; Bartolucci, A.A.; Azziz, R. Prevalence of insulin resistance in the polycystic ovary syndrome using the homeostasis model assessment. Fertil. Steril. 2005, 83, 1454–1460. [Google Scholar] [CrossRef]
- Ingram, J.R. The epidemiology of hidradenitis suppurativa. Br. J. Dermatol. 2020, 183, 990–998. [Google Scholar] [CrossRef] [PubMed]
- Azziz, R.; Woods, K.S.; Reyna, R.; Key, T.J.; Knochenhauer, E.S.; Yildiz, B.O. The prevalence and features of the polycystic ovary syndrome in an unselected population. J. Clin. Endocrinol. Metab. 2004, 89, 2745–2749. [Google Scholar] [CrossRef] [Green Version]
- Gast, K.B.; Tjeerdema, N.; Stijnen, T.; Smit, J.W.; Dekkers, O.M. Insulin resistance and risk of incident cardiovascular events in adults without diabetes: Meta-analysis. PLoS ONE 2012, 7, e52036. [Google Scholar] [CrossRef] [Green Version]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuniga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef] [Green Version]
- Taylor, R. Insulin resistance and type 2 diabetes. Diabetes 2012, 61, 778–779. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.A.; Lee, J.H.; Lim, S.Y.; Ha, H.S.; Kwon, H.S.; Park, Y.M.; Lee, W.C.; Kang, M.I.; Yim, H.W.; Yoon, K.H.; et al. Metabolic syndrome as a predictor of type 2 diabetes, and its clinical interpretations and usefulness. J. Diabetes Investig. 2013, 4, 334–343. [Google Scholar] [CrossRef]
- Sivanand, A.; Gulliver, W.P.; Josan, C.K.; Alhusayen, R.; Fleming, P.J. Weight Loss and Dietary Interventions for Hidradenitis Suppurativa: A Systematic Review. J. Cutan. Med. Surg. 2020, 24, 64–72. [Google Scholar] [CrossRef]
- Clamp, L.D.; Hume, D.J.; Lambert, E.V.; Kroff, J. Enhanced insulin sensitivity in successful, long-term weight loss maintainers compared with matched controls with no weight loss history. Nutr. Diabetes 2017, 7, e282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelan, S.; Wadden, T.A.; Berkowitz, R.I.; Sarwer, D.B.; Womble, L.G.; Cato, R.K.; Rothman, R. Impact of weight loss on the metabolic syndrome. Int. J. Obes. 2007, 31, 1442–1448. [Google Scholar] [CrossRef] [Green Version]
- Giannarelli, R.; Aragona, M.; Coppelli, A.; Del Prato, S. Reducing insulin resistance with metformin: The evidence today. Diabetes Metab. 2003, 29, S28–S35. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, S.M.D.; Norman, R.J.P. Metabolic syndrome, diet and exercise. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 37, 140–151. [Google Scholar] [CrossRef]
- Al Wattar, B.H.; Fisher, M.; Bevington, L.; Talaulikar, V.; Davies, M.; Conway, G.; Yasmin, E. Clinical Practice Guidelines on the Diagnosis and Management of Polycystic Ovary Syndrome: A Systematic Review and Quality Assessment Study. J. Clin. Endocrinol. Metab. 2021, 106, 2436–2446. [Google Scholar] [CrossRef]
- Bassols, J.; Martinez-Calcerrada, J.M.; Osiniri, I.; Diaz-Roldan, F.; Xargay-Torrent, S.; Mas-Pares, B.; Dorado-Ceballos, E.; Prats-Puig, A.; Carreras-Badosa, G.; de Zegher, F.; et al. Effects of metformin administration on endocrine-metabolic parameters, visceral adiposity and cardiovascular risk factors in children with obesity and risk markers for metabolic syndrome: A pilot study. PLoS ONE 2019, 14, e0226303. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Tan, G.S.; Zhang, K. Relationship of the Serum CRP Level With the Efficacy of Metformin in the Treatment of Type 2 Diabetes Mellitus: A Meta-Analysis. J. Clin. Lab. Anal. 2016, 30, 13–22. [Google Scholar] [CrossRef]
- Cameron, A.R.; Morrison, V.L.; Levin, D.; Mohan, M.; Forteath, C.; Beall, C.; McNeilly, A.D.; Balfour, D.J.; Savinko, T.; Wong, A.K.; et al. Anti-Inflammatory Effects of Metformin Irrespective of Diabetes Status. Circ. Res. 2016, 119, 652–665. [Google Scholar] [CrossRef] [Green Version]
- Orio, F.; Manguso, F.; Di Biase, S.; Falbo, A.; Giallauria, F.; Labella, D.; Tolino, A.; Lombardi, G.; Colao, A.; Palomba, S. Metformin administration improves leukocyte count in women with polycystic ovary syndrome: A 6-month prospective study. Eur. J. Endocrinol. 2007, 157, 69–73. [Google Scholar] [CrossRef] [Green Version]
- Ibanez, L.; Jaramillo, A.M.; Ferrer, A.; de Zegher, F. High neutrophil count in girls and women with hyperinsulinaemic hyperandrogenism: Normalization with metformin and flutamide overcomes the aggravation by oral contraception. Hum. Reprod. 2005, 20, 2457–2462. [Google Scholar] [CrossRef]
- Kearney, N.; McCourt, C.; Hambly, R.; Hughes, R.; O’Kane, D.; Kirby, B. Association of Biologic Treatment in Hidradenitis Suppurativa With Reduced Neutrophil-Lymphocyte Ratio and Platelet-Lymphocyte Ratio. JAMA Dermatol. 2023, 159, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Wolk, K.; Join-Lambert, O.; Sabat, R. Aetiology and pathogenesis of hidradenitis suppurativa. Br. J. Dermatol. 2020, 183, 999–1010. [Google Scholar] [CrossRef]
- Navrazhina, K.; Garcet, S.; Frew, J.W.; Zheng, X.; Coats, I.; Guttman-Yassky, E.; Krueger, J.G. The inflammatory proteome of hidradenitis suppurativa skin is more expansive than that of psoriasis vulgaris. J. Am. Acad. Dermatol. 2022, 86, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Frew, J.W.; Hawkes, J.E.; Krueger, J.G. A systematic review and critical evaluation of inflammatory cytokine associations in hidradenitis suppurativa. F1000Research 2018, 7, 1930. [Google Scholar] [CrossRef] [PubMed]
- Bai, B.; Chen, H. Metformin: A Novel Weapon Against Inflammation. Front. Pharmacol. 2021, 12, 622262. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liu, X.; Ye, S. Effects of metformin on blood and urine pro-inflammatory mediators in patients with type 2 diabetes. J. Inflamm. 2016, 13, 34. [Google Scholar] [CrossRef]
- Xu, X.; Du, C.; Zheng, Q.; Peng, L.; Sun, Y. Effect of metformin on serum interleukin-6 levels in polycystic ovary syndrome: A systematic review. BMC Women’s Health 2014, 14, 93. [Google Scholar] [CrossRef] [Green Version]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef]
- Wolk, K.; Sabat, R. Adipokines in psoriasis: An important link between skin inflammation and metabolic alterations. Rev. Endocr. Metab. Disord. 2016, 17, 305–317. [Google Scholar] [CrossRef]
- Nakamura, K.; Fuster, J.J.; Walsh, K. Adipokines: A link between obesity and cardiovascular disease. J. Cardiol. 2014, 63, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ascaso, J.F.; Pardo, S.; Real, J.T.; Lorente, R.I.; Priego, A.; Carmena, R. Diagnosing insulin resistance by simple quantitative methods in subjects with normal glucose metabolism. Diabetes Care 2003, 26, 3320–3325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gayoso-Diz, P.; Otero-Gonzalez, A.; Rodriguez-Alvarez, M.X.; Gude, F.; Garcia, F.; De Francisco, A.; Quintela, A.G. Insulin resistance (HOMA-IR) cut-off values and the metabolic syndrome in a general adult population: Effect of gender and age: EPIRCE cross-sectional study. BMC Endocr. Disord. 2013, 13, 47. [Google Scholar] [CrossRef] [Green Version]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HS Metformin (n = 20) | HS Control (n = 20) | p-Value | |
|---|---|---|---|
| Female (n, %) | 19 (95%) | 15 (75%) | 0.077 |
| Age (mean ± SD) | 38.1 ± 11.2 | 37.95 ± 12.3 | 0.968 |
| Disease duration (mean ± SD) | 12.65 years ± 8.7 | 10.8 years ± 8.6 | 0.504 |
| Smoking (n, %) | 0.374 | ||
| Current | 7 (35%) | 11 (55%) | |
| Ex | 6 (30%) | 3 (15%) | |
| Non | 7 (35%) | 6 (30%) | |
| Hurley stage (n, %) | 0.347 | ||
| Hurley 1 | 2 (10%) | 2 (10%) | |
| Hurley 2 | 16 (80%) | 18 (90%) | |
| Hurley 3 | 2 (10%) | 0 | |
| BMI kg/m2 (mean ± SD) | 35 ± 9.8 | 33.6 ± 9 | 0.624 |
| WC cm (mean ± SD) | 103.7 ± 19 | 102.35 ± 19.8 | 0.823 |
| SBP (mean ± SD) | 131 ± 14.9 | 130.5 ± 18.8 | 0.528 |
| DBP (mean ± SD) | 81.3 ± 9 | 79.2 ±12.3 | 0.116 |
| HbA1c mmol/mol (mean ± SD) | 36.2 ± 2.7 | 35.8 ± 4.3 | 0.74 |
| HOMA-IR (mean ± SD) | 4.7 ± 4 (n = 14) | 4.2 ± 2.8 (n = 16) | 0.673 |
| Insulin resistance (HOMA-IR ≥ 2.6) (n, %) | 10 (71.4%) (n = 14) | 13 (81.3%) (n = 16) | 0.526 |
| Metabolic syndrome (n, %) | 9 (45%) (n = 20) | 8 (42%) (n = 19) | 0.855 |
| CRP (mg/L) (mean ± SD) | 5.17 ± 3.8 (n = 19) | 8.19 ± 11.9 (n = 20) | 0.3 |
| n = 19 | n = 17 | ||
| Neutrophils (×109/L) (mean ± SD) | 4.88 ± 1.5 | 5.15 ± 2 | 0.658 |
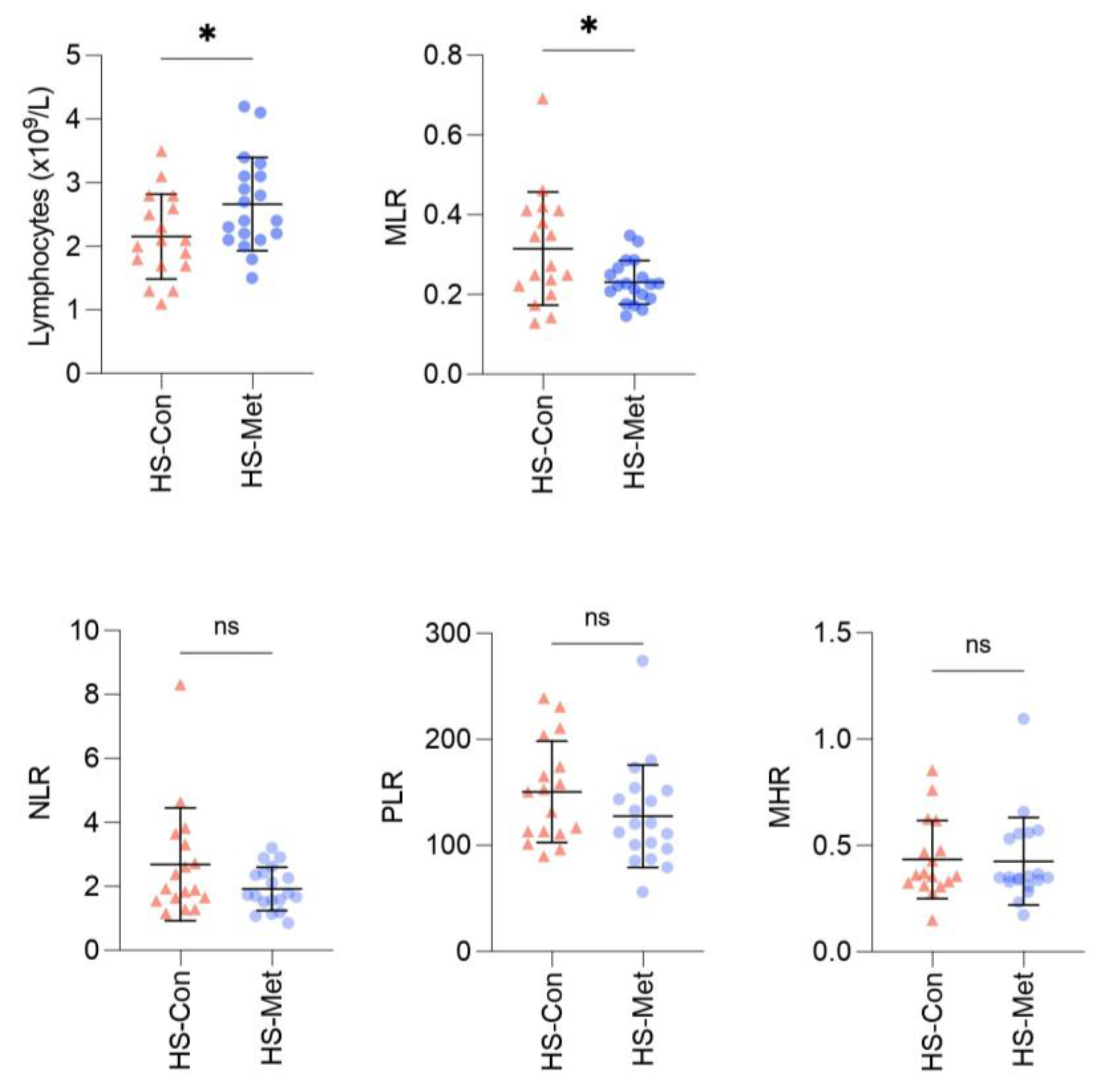
| Lymphocytes (×109/L) (mean ± SD) | 2.66 ± 0.73 | 2.15 ± 0.67 | 0.037 |
| Platelets (×109/L) (mean ± SD) | 314.16 ± 56 | 300.65 ± 57.4 | 0.48 |
| Monocytes (×109/L) (mean ± SD) | 0.59 ± 0.12 | 0.62 ± 0.18 | 0.596 |
| NLR (mean ± SD) | 1.92 ± 0.68 | 2.69 ± 1.76 | 0.108 |
| PLR (mean ± SD) | 127.65 ± 48.2 | 150.6 ± 47.74 | 0.161 |
| MLR (mean ± SD) | 0.23 ± 0.05 | 0.32 ± 0.14 | 0.032 |
| MHR (mean ± SD) | 0.43 ± 0.21 | 0.43 ± 0.18 | 0.898 |
| Pre-Metformin (n = 9) | On Metformin (n = 9) | p-Value | |
|---|---|---|---|
| Fasting glucose mmol/L (median, IQR) | 4.9 (4.6–5.3) | 4.9 (4.8–5.3) | 0.69 |
| Fasting insulin mIU/L (median, IQR) | 22.0 (5.7–72.9) | 3.3 (2.0–7.5) | 0.008 |
| HOMA-IR (median, IQR) | 4.8 (1.2–22.9) | 3.3 (2.0–7.5) | 0.43 |
| HbA1c mmol/mol (median, IQR) | 35.0 (32.5–37.8) | 36.0 (35.0–38.0) | 0.11 |
| CV Risk Biomarker | Group | Mean | p-Value |
|---|---|---|---|
| NLR | HS Control (n = 17) | 2.69 | 0.027 |
| General population mean a | 1.65 | ||
| HS Metformin (n = 19) | 1.92 | 0.094 | |
| General population mean | 1.65 | ||
| PLR | HS Control (n = 17) | 150.6 | 0.01 |
| General population mean a | 117.05 | ||
| HS Metformin (n = 19) | 127.65 | 0.35 | |
| General population mean a | 117.05 | ||
| MLR | HS Control (n = 17) | 0.32 | 0.325 |
| ACS mean a | 0.28 | ||
| HS Metformin (n = 19) | 0.23 | 0.001 | |
| ACS mean a | 0.28 |
| Correlation | r | p-Value |
|---|---|---|
| CRP and lymphocyte count | 0.106 | 0.546 |
| CRP and neutrophil count | 0.179 | 0.304 |
| CRP and NLR | 0.023 | 0.896 |
| CRP and PLR | 0.052 | 0.766 |
| CRP and MLR | −0.084 | 0.631 |
| CRP and MHR | 0.218 | 0.208 |
| HOMA-IR and lymphocyte count | −0.4 | 0.841 |
| HOMA-IR and neutrophil count | 0.209 | 0.296 |
| HOMA-IR and NLR | 0.091 | 0.653 |
| HOMA-IR and PLR | 0.068 | 0.763 |
| HOMA-IR and MLR | −0.035 | 0.861 |
| HOMA-IR and MHR | 0.157 | 0.435 |
| Analyte | HS Controls n = 18 Median (IQR) | HS Metformin n = 17 Median (IQR) | p-Value |
|---|---|---|---|
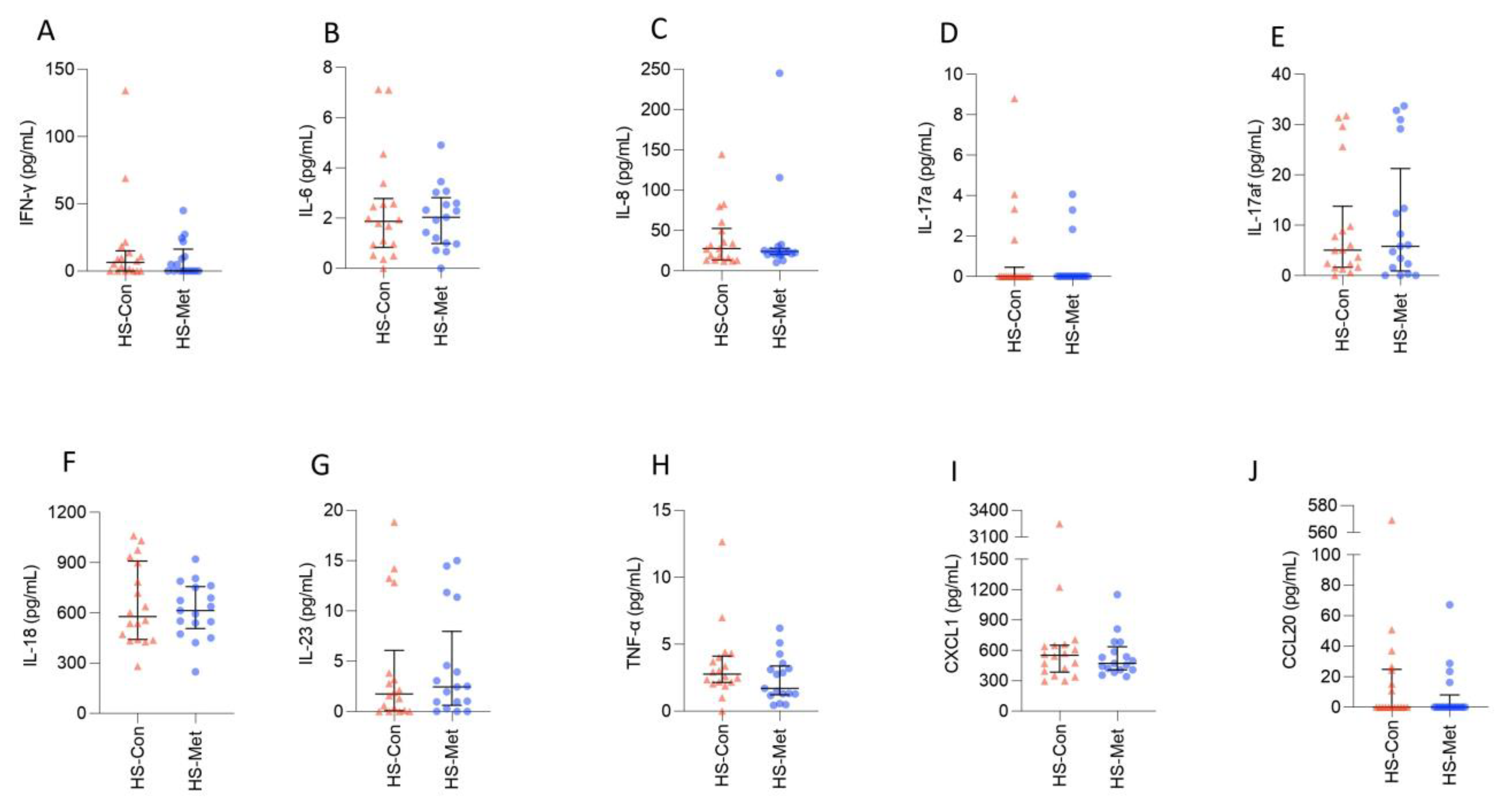
| IFN-γ (pg/mL) | 6.43 (0–15) | 0.19 (0–16.34) | 0.52 |
| IL-6 (ng/mL) | 1.9 (0.84–2.78) | 2 (0.99–2.81) | 0.8 |
| IL-8 (ng/mL) | 27.39 (13.34–52.44) | 24.03 (20.05–27.75) | 0.81 |
| IL-17a (pg/mL) | 0 (0–0.45) | 0 (0–0) | 0.74 |
| IL-17af (pg/mL) | 5.06 (1.65–13.77) | 5.83 (0.93–21.24) | 0.98 |
| IL-18 (pg/mL) | 578 (441–908) | 613 (506–757) | 0.96 |
| IL-23 (pg/mL) | 1.75 (0.09–6.08) | 2.46 (0.63–7.97) | 0.68 |
| TNF-α (pg/mL) | 2.78 (2.15–4.1) | 1.7 (1.22–3.38) | 0.19 |
| CXCL1 (ng/mL) | 553 (384–652) | 471 (408–635) | 0.73 |
| CCL20 (pg/mL) | 0 (0–24.89) | 0 (0–8.11) | 0.37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hambly, R.; Kearney, N.; Hughes, R.; Fletcher, J.M.; Kirby, B. Metformin Treatment of Hidradenitis Suppurativa: Effect on Metabolic Parameters, Inflammation, Cardiovascular Risk Biomarkers, and Immune Mediators. Int. J. Mol. Sci. 2023, 24, 6969. https://doi.org/10.3390/ijms24086969
Hambly R, Kearney N, Hughes R, Fletcher JM, Kirby B. Metformin Treatment of Hidradenitis Suppurativa: Effect on Metabolic Parameters, Inflammation, Cardiovascular Risk Biomarkers, and Immune Mediators. International Journal of Molecular Sciences. 2023; 24(8):6969. https://doi.org/10.3390/ijms24086969
Chicago/Turabian StyleHambly, Roisin, Niamh Kearney, Rosalind Hughes, Jean M. Fletcher, and Brian Kirby. 2023. "Metformin Treatment of Hidradenitis Suppurativa: Effect on Metabolic Parameters, Inflammation, Cardiovascular Risk Biomarkers, and Immune Mediators" International Journal of Molecular Sciences 24, no. 8: 6969. https://doi.org/10.3390/ijms24086969