
Renin-Angiotensin-Aldosterone System Inhibitors and Development of Gynecologic Cancers: A 23 Million Individual Population-Based Study
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Descriptive Analysis
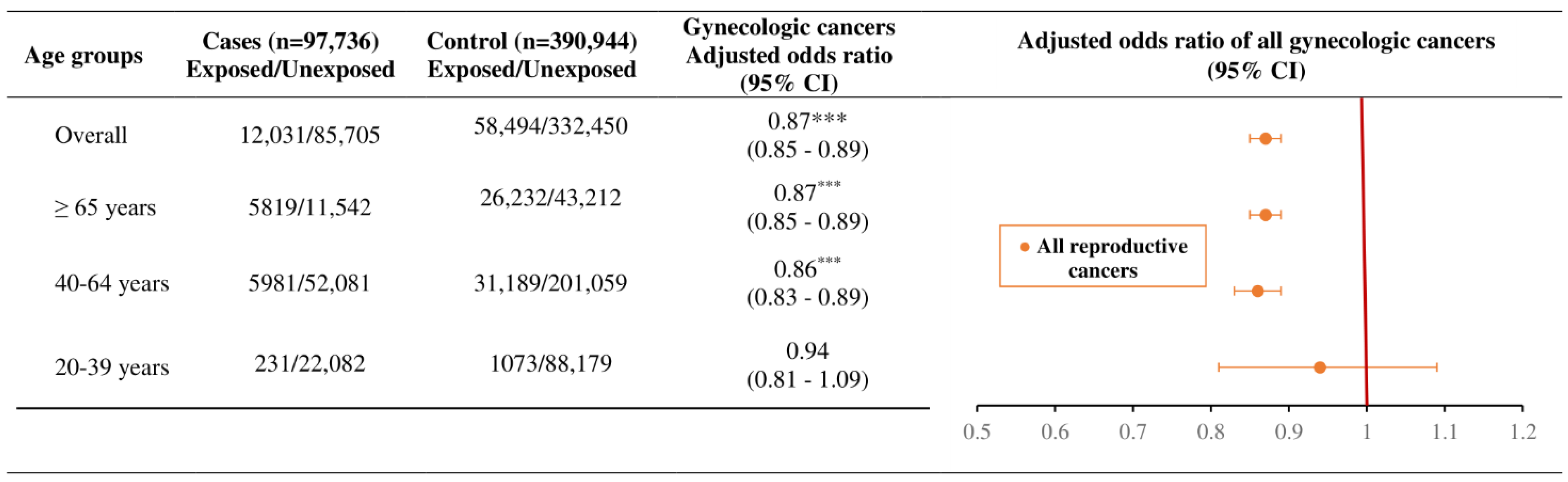
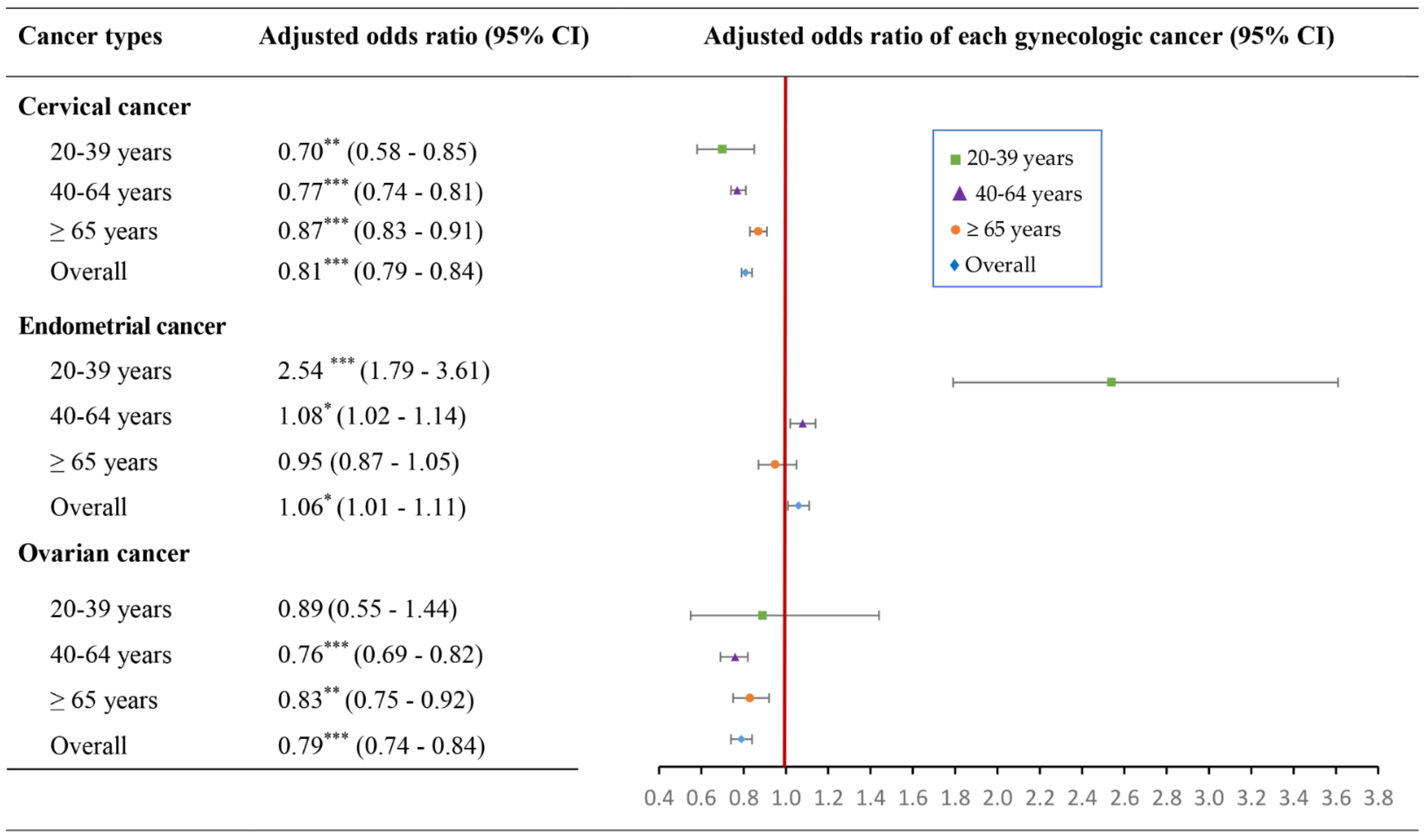
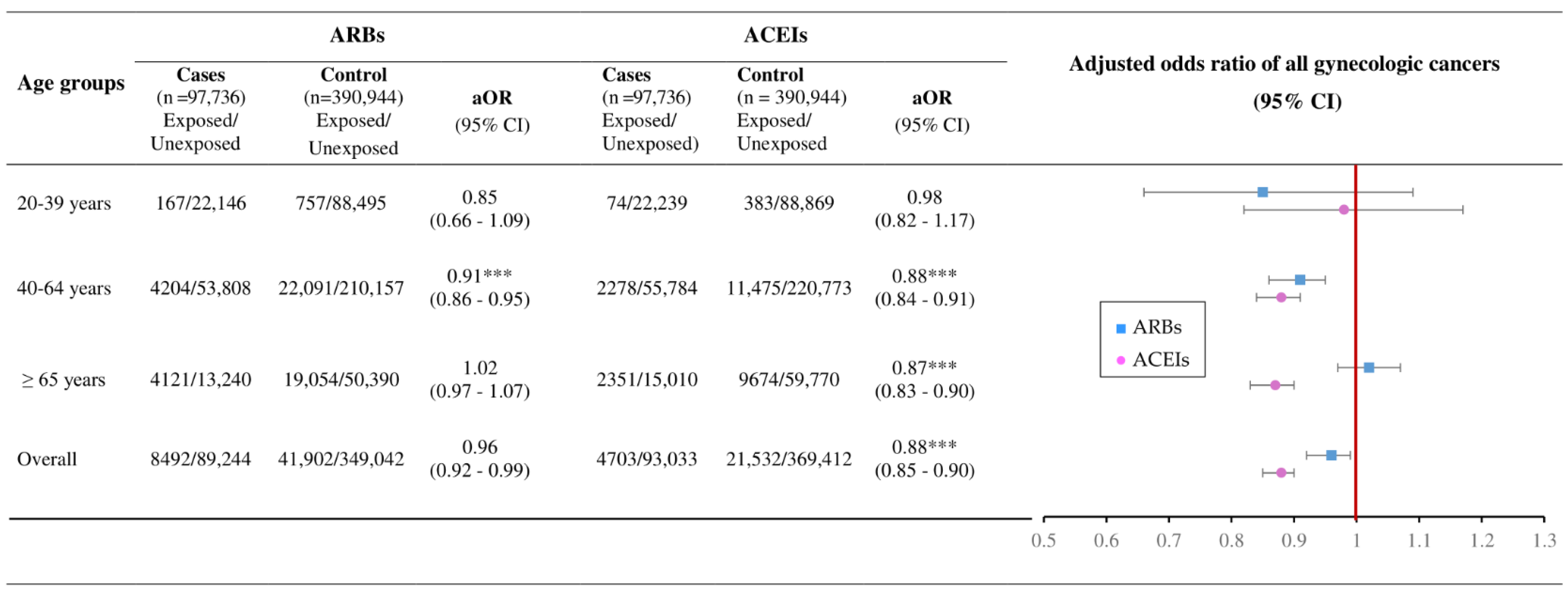
2.2. Association of RAAS Use with Overall Gynecologic Cancer
3. Discussion
3.1. Main Findings
3.2. Biological Plausibility
3.2.1. Postulated Mechanisms of RAAS Inhibitors against Gynecologic Cancers
3.2.2. Postulated Mechanisms of ARBs/ACEIs against Gynecologic Cancers
4. Materials and Methods
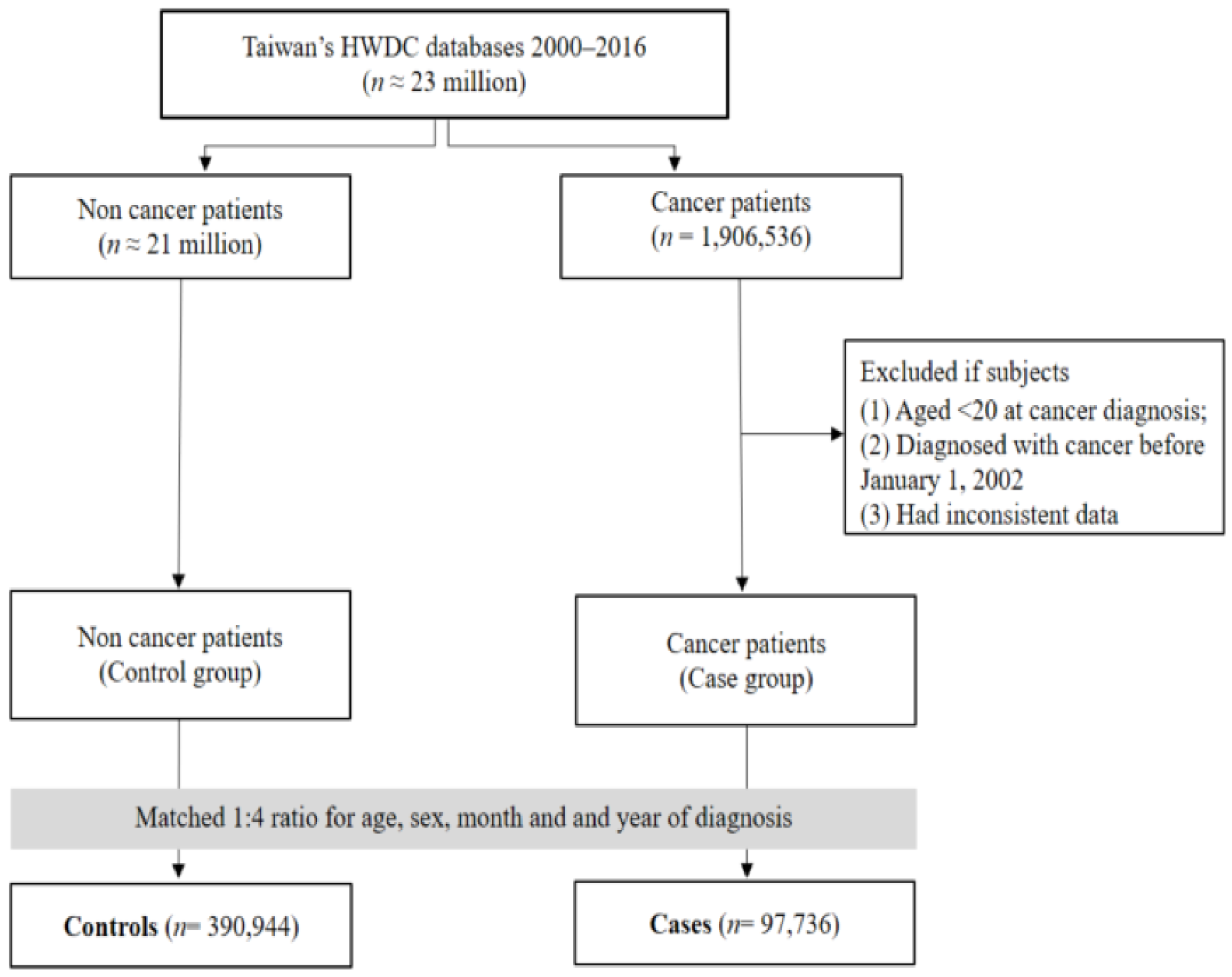
4.1. Data Sources
4.2. Definition of Case and Control
4.3. RAAS Users
4.4. Confounding Factors
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| aOR | Adjusted odds ratio |
| ACEIs | Angiotensin-converting enzyme inhibitors |
| ARBS | Angiotensin receptor blockers |
| ATC Classification | Anatomical Therapeutic Chemical classification |
| CCI | Charlson comorbidity index |
| CI | Confidence interval |
| HWDC | Health and Welfare Data Science Center |
| ICD-9-CM | International Classification of Diseases, 9th revision, Clinical Modification |
| KDR | Kinase domain-containing receptor |
| MOHW | Ministry of Health and Welfare |
| NHI | National Health Insurance |
| TCR | Taiwan Cancer Registry |
| TMU-JIRB | Joint Institutional Review Board of Taipei Medical University |
| RAAS | Renin-angiotensin-aldosterone system |
| VEGF | Vascular endothelial growth factor |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ATC Code | Name | Covered by National Health Insurance in Taiwan |
|---|---|---|
| C09AA01 | captopril | 1995~ |
| C09AA02 | enalapril | 1995~ |
| C09AA03 | lisinopril | 1995~ |
| C09AA04 | perindopril | 1995~ |
| C09AA05 | ramipril | 1995~ |
| C09AA06 | quinapril | 1995~ |
| C09AA07 | benazepril | 1995~ |
| C09AA08 | cilazapril | 1995~ |
| C09AA09 | fosinopril | 1995~ |
| C09AA10 | trandolapril | Not Available |
| C09AA11 | spirapril | Not Available |
| C09AA12 | delapril | Not Available |
| C09AA13 | moexipril | Not Available |
| C09AA14 | temocapril | Not Available |
| C09AA15 | zofenopril | Not Available |
| C09AA16 | imidapril | 2001~ |
| C09CA01 | losartan | 1998~ |
| C09CA02 | eprosartan | 2007~ |
| C09CA03 | valsartan | 1998~ |
| C09CA04 | irbesartan | 2000~ |
| C09CA05 | tasosartan | Not Available |
| C09CA06 | candesartan | 2001~ |
| C09CA07 | telmisartan | 2001~ |
| C09CA08 | olmesartan | 2004~ |
| C09CA09 | azilsartan | 2014~ |
| C09CA10 | fimasartan | Not Available |
References
- Ino, K.; Shibata, K.; Yamamoto, E.; Hiroaki, K.; Nawa, A.; Mabuchi, Y. Role of the renin-angiotensin system in gynecologic cancers. Curr. Cancer Drug Targets 2011, 11, 405–411. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, H.; Siegel, R.; Laversanne, M.; Soerjomataram, I.; Jemal. A Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Cervical Cancer. World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 29 January 2023).
- Chandra, A.; Pius, C.; Nabeel, M.; Nair, M.; Vishwanatha, J.; Ahmad, S. Ovarian cancer: Current status and strategies for improving therapeutic outcomes. Cancer Med. 2019, 8, 7018–7031. [Google Scholar] [CrossRef]
- Lheureux, S.; Gourley, C.; Vergote, I.; Oza, A.M. Epithelial ovarian cancer. Lancet 2019, 393, 1240–1253. [Google Scholar] [CrossRef]
- Armstrong, D.K.; Alvarez, R.D.; Bakkum-Gamez, J.N.; Barroilhet, L.; Behbakht, K.; Berchuck, A. Ovarian Cancer, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 191–226. [Google Scholar] [CrossRef]
- Endometrial Cancer Statistics. Available online: https://www.wcrf.org/cancer-trends/endometrial-cancer-statistics/ (accessed on 10 December 2022).
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Yang, Y.H.K. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef]
- Albayrak, M.; Celebi, H.; Albayrak, A.; Sayilir, A.; Yesil, Y.; Balcik, O.S. Elevated serum angiotensin converting enzyme levels as a reflection of bone marrow renin-angiotensin system activation in multiplloma. J. Renin-Angiotensin-Aldosterone Syst. 2012, 13, 259–264. [Google Scholar] [CrossRef]
- Haznedaroglu, I.C.; Beyazit, Y. Pathobiological aspects of the local bone marrow renin-angiotensin system: A review. J. Renin-Angiotensin-Aldosterone Syst. 2010, 11, 205–213. [Google Scholar] [CrossRef]
- Sama, I.E.; Ravera, A.; Santema, B.T.; Goor, H.V.; Maaten, J.M.T.; Cleland, J.G.F. Circulating plasma concentrations of angiotensin-converting enzyme 2 in men and women with heart failure and effects of renin-angiotensin-aldosterone inhibitors. Eur. Heart J. 2020, 41, 1810–1817. [Google Scholar] [CrossRef]
- Hallas, J.; Christensen, R.; Andersen, M.; Friis, M.; Bjerrum, L. Long term use of drugs affecting the renin-angiotensin system and the risk of cancer: A population-based case-control study. Br. J. Clin. Pharmacol. 2012, 74, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Cho, M.A.; Christensen, R.; Andersen, M.; Friis, S.; Bjerrum, L. Impact of Angiotensin Receptor Blockers, Beta Blockers, Calcium Channel Blockers and Thiazide Diuretics on Survival of Ovarian Cancer Patients. Cancer Res. Treat. 2020, 52, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Raba, G.; Zawlik, I.; Braun, M.; Paszek, S.; Potocka, N.; Skrzypa, M. Evaluation of the association between angiotensin converting enzyme insertion/deletion polymorphism and the risk of endometrial cancer in and characteristics of Polish women. Adv. Clin. Exp. Med. 2020, 29, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Lever, A.F.; Hole, D.J.; Gillis, C.R.; McCallum, I.R.; McInnes, G.T.; MacKinnon, P.L. Do inhibitors of angiotensin-I-converting ezyme protect against risk of cancer? Lancet 1998, 352, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Sipahi, I.; Debanne, S.M.; Rowland, D.Y.; Simon, D.I.; Fang, J.C. Angiotensin-receptor blockade and risk of cancer: Meta-analysis of randomised controlled trials. Lancet Oncol. 2010, 11, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Beyazit, F.; Ayhan, S.; Celik, H.T.; Gungor, T. Assessment of serum angiotensin-converting enzyme in patients with epithelial ovarian cancer. Arch. Gynecol. Obstet. 2015, 292, 415–420. [Google Scholar] [CrossRef]
- Brunswig-Spickenheier, B.; Mukhopadhyay, A.K. Local regulatory factors in regulation of ovarian function: Role of prorenin-renin-angiotensin-system. Indian J. Exp. Biol. 2003, 41, 669–681. [Google Scholar]
- Delforce, S.; Lumbers, E.R.; De Meaultsart, C.C.; Wang, Y.; Proietto, A.; Otton, G.; Scurry, J.; Verrills, N.; Scott, R.J.; Pringle, K.G. Expression of renin-angiotensin system (RAS) components in endometrial cancer. Endocr. Connect. 2017, 6, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Schwentner, L.; Lumbers, E.R.; Meaultsart, C.C.; Wang, Y.; Proietto, A.; Otton, G. Is there a role of the local tissue RAS in the regulation of physiologic and pathophysiologic conditions in the reproductive tract? J. Renin-Angiotensin-Aldosterone Syst. 2011, 12, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Vinson, G.P.; Saridogan, E.; Puddefoot, J.R.; Djahanbakhch, O. Tissue renin-angiotensin systems and reproduction. Hum. Reprod. 1997, 12, 651–662. [Google Scholar] [CrossRef]
- Kikkawa, F.; Mizuno, M.; Shibata, K.; Kajiyama, H.; Morita, T.; Ino, K. Activation of invasiveness of cervical carcinoma cells by angiotensin II. Am. J. Obstet. Gynecol. 2004, 190, 1258–1263. [Google Scholar] [CrossRef]
- Tamarat, R.; Silvestre, J.S.; Durie, M.; Levy, B.I. Angiotensin II angiogenic effect in vivo involves vascular endothelial growth factor- and inflammation-related pathways. Lab. Investig. 2002, 82, 747–756. [Google Scholar] [CrossRef] [Green Version]
- Suganuma, T.; Ino, K.; Shibata, K.; Kajiyama, H.; Nagasaka, T.; Mizutani, S.; Kikkawa, F. Functional expression of the angiotensin II type 1 receptor in human ovarian carcinoma cells and its blockade therapy resulting in suppression of tumor invasion, angiogenesis, and peritoneal dissemination. Clin. Cancer Res. 2005, 11, 2686–2694. [Google Scholar] [CrossRef]
- Domińska, K.; Lachowicz-Ochedalska, A. The involvement of the renin-angiotensin system (RAS) in cancerogenesis. Postep. Biochem. 2008, 54, 294–300. [Google Scholar]
- Deshayes, F.; Nahmias, C. Angiotensin receptors: A new role in cancer? Trends Endocrinol. Metab. 2005, 16, 293–299. [Google Scholar] [CrossRef]
- Pawlikowski, M.; Meleń-Mucha, G.; Mucha, S. The involvement of the renin-angiotensin system in the regulation of cell proliferation in the rat endometrium. Cell. Mol. Life Sci. 1999, 55, 506–510. [Google Scholar] [CrossRef]
- Nowakowska, M.; Matysiak-Burzyńska, Z.; Kowalska, K.; Płuciennik, E.; Domińska, K.; Piastowska-Ciesielska, A.W. Angiotensin II promotes endometrial cancer cell survival. Oncol. Rep. 2016, 36, 1101–1110. [Google Scholar] [CrossRef]
- Ino, K.; Shibata, K.; Kajiyama, H.; Yamamoto, E.; Nagasaka, T.; Nawa, A. Angiotensin II type 1 receptor expression in ovarian cancer and its correlation with tumour angiogenesis and patient survival. Br. J. Cancer 2006, 94, 552–560. [Google Scholar] [CrossRef]
- Ishimatsu, S.; Itakura, A.; Okada, M.; Kotani, T.; Iwase, A.; Kajiyama, H. Angiotensin II augmented migration and invasion of coriocarcinoma cells involves PI3K activation through the AT1 receptor. Placenta 2006, 27, 587–591. [Google Scholar] [CrossRef]
- Ziaja, M.; Urbanek, K.A.; Kowalska, K.; Piastowska-Ciesielska, A.W. Angiotensin II and Angiotensin Receptors 1 and 2-Multifunctional System in Cells Biology, What Do We Know? Cells 2021, 10, 381. [Google Scholar] [CrossRef]
- Schmandt, R.E.; Iglesias, D.A.; Co, N.N.; Luet, K.K. Understanding obesity and endometrial cancer risk: Opportunities for prevention. Am. J. Obstet. Gynecol. 2011, 205, 518–525. [Google Scholar] [CrossRef]
- Secord, A.A.; Hasselblad, V.; Von Gruenigen, V.E.; Gehrig, P.A.; Modesitt, S.C.; Bae-Jump, V.; Havrilesky, L.J. Body mass index and mortality in endometrial cancer: A systematic review and meta-analysis. Gynecol. Oncol. 2016, 140, 184–190. [Google Scholar] [CrossRef]
- Onstad, M.A.; Schmandt, R.E.; Lu, K.H. Addressing the Role of Obesity in Endometrial Cancer Risk, Prevention, and Treatment. J. Clin. Oncol. 2016, 34, 4225–4230. [Google Scholar] [CrossRef]
- Renehan, A.G.; Zwahlen, M.; Egger, M. Adiposity and cancer risk: New mechanistic insights from epidemiology. Nat. Rev. Cancer 2015, 15, 484–498. [Google Scholar] [CrossRef]
- Allott, E.H.; Hursting, S.D. Obesity and cancer: Mechanistic insights from transdisciplinary studies. Endocr. Relat. Cancer 2015, 22, 365–386. [Google Scholar] [CrossRef]
- Park, J.; Morley, T.S.; Kim, M.; Clegg, D.J.; Scherer, P.E. Obesity and cancer—mechanisms underlying tumour progression and recurrence. Nat. Rev. Endocrinol. 2014, 10, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Klopp, A.H.; Zhang, Y.; Solley, T.; Amaya-Manzanares, F.; Marini, F.; Andreeff, M.; Debeb, B.; Woodward, W.; Schmandt, R.; Broaddus, R.; et al. Omental adipose tissue-derived stromal cells promote vascularization and growth of endometrial tumors. Clin. Cancer Res. 2012, 18, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Pope, B.D.; Warren, C.R.; Parker, K.K.; Cowan, C.A. Microenvironmental Control of Adipocyte Fate and Function. Trends Cell Biol. 2016, 26, 745–755. [Google Scholar] [CrossRef]
- Song, F.; Chen, Q.; Rao, W.; Zhang, R.; Wang, Y.; Ge, H.; Wei, Q. OVA66 promotes tumour angiogenesis and progression through enhancing autocrine VEGF-VEGFR2 signalling. EBioMedicine 2019, 41, 156–166. [Google Scholar] [CrossRef]
- Nilsson, M.B.; Giri, U.; Gudikote, J.; Tang, X.; Lu, W.; Tran, H. KDR Amplification Is Associated with VEGF-Induced Activation of the mTOR and Invasion Pathways but does not Predict Clinical Benefit to the VEGFR TKI Vandetanib. Clin. Cancer Res. 2016, 22, 1940–1950. [Google Scholar] [CrossRef]
- Sher, I.; Adham, S.A.; Petrik, J.; Coomber, B.L. Autocrine VEGF-A/KDR loop protects epithelial ovarian carcinoma cells from anoikis. Int. J. Cancer 2009, 124, 553–561. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Lee, S.-H.; Park, J.; Park, R.W.; Shin, S.J.; Kim, J.; Sung, J.D.; Kim, D.J.; Yang, K. Renin-Angiotensin-Aldosterone System Inhibitors and Risk of Cancer: A Population-Based Cohort Study Using a Common Data Model. Diagnostics 2022, 12, 263. [Google Scholar] [CrossRef]
- Shin, K.; Yang, J.; Yu, Y.; Son, E.; Kim, K.; YH, K. Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers and cancer risk: An updated meta-analysis of observational studies. Ther. Adv. Drug Saf. 2022, 13, 20420986221129335. [Google Scholar] [CrossRef]
- Dolley-Hitze, T.; Jouan, F.; Martin, B.; Mottier, S.; Edeline, J.; Moranne, O. Angiotensin-2 receptors (AT1-R and AT2-R), new prognostic factors for renal clear-cell carcinoma? Br. J. Cancer 2010, 103, 1698–1705. [Google Scholar] [CrossRef] [PubMed]
- Chehl, N.; Gong, Q.; Chipitsyna, G.; Aziz, T.; Yeo, C.J.; Arafat, H.A. Angiotensin II regulates the expression of monocyte chemoattractant protein-1 in pancreatic cancer cells. J. Gastrointest. Surg. 2009, 13, 2189–2200. [Google Scholar] [CrossRef]
- Zhao, Y.; Cao, K.; Melamed, A.; Worley, M.; Gockley, A.; Jones, D. Losartan treatment enhances chemotherapy efficacy and reduces ascites in ovarian cancer models by normalizing the tumor stroma. Proc. Natl. Acad. Sci. USA 2019, 116, 2210–2219. [Google Scholar] [CrossRef]
- Erman, A.; Chen-Gal, B.; Dijk, D.J.V.; Sulkes, J.; Kaplan, B.; Boner, G.; Neri, A. Ovarian angiotensin-converting enzyme activity in humans: Relationship to estradiol, age, and uterine pathology. J. Clin. Endocrinol. Metab. 1996, 81, 1104–1107. [Google Scholar]
- Cotter, T.P.; Kealy, N.P.; Duggan, P.F.; Curtain, A.; Bredin, C.P. Elevated serum angiotensin converting enzyme levels in metastatic ovarian dysgerminoma. Respir. Med. 1997, 91, 237–239. [Google Scholar] [CrossRef]
- Bangalore, S.; Kumar, S.; E Kjeldsen, S.; Makani, H.; Grossman, E.; Wetterslev, J.; Gupta, A.K.; Sever, P.S.; Gluud, C.; Messerli, F.H. Antihypertensive drugs and risk of cancer: Network meta-analyses and trial sequential analyses of 324,168 participants from randomised trials. Lancet Oncol. 2011, 12, 65–82. [Google Scholar] [CrossRef]
- Friis, S.; Sørensen, H.T.; Mellemkjaer, L.; McLaughlin, J.K.; Nielsen, G.L.; Blot, W.J.; Olsen, J.H. Angiotensin-converting enzyme inhibitors and the risk of cancer: A population-based cohort study in Denmark. Cancer 2001, 92, 2462–2470. [Google Scholar] [CrossRef]
- Universal Health Coverage in Taiwan. National Health Insurance Administration, MOHAW, Taiwan. Available online: https://www.nhi.gov.tw/English/Content_List.aspx?n=4D7051840BF42F52&topn=ED4A30E51A609E49 (accessed on 10 December 2022).
- National Health Insurance Administration. ICD-9-CM and ICD-10-CM/PCS Mapping Table; MOHAW: Taipei, Taiwan, 2020. [Google Scholar]
- Grimes, D.A.; Schulz, K.F. Compared to what? Finding controls for case-control studies. Lancet 2005, 365, 1429–1433. [Google Scholar] [CrossRef]
- Gadducci, A.; Biglia, N.; Tana, R.; Cosio, S.; Gallo, M. Metformin use and gynecological cancers: A novel treatment option emerging from drug repositioning. Crit. Rev. Oncol. Hematol. 2016, 105, 73–83. [Google Scholar] [CrossRef]
- Lee, D.Y.; Lee, T.S. Associations between metabolic syndrome and gynecologic cancer. Obstet. Gynecol. Sci. 2020, 63, 215–224. [Google Scholar] [CrossRef]
- Chen, Y.H.; Wang, P.H.; Chen, P.N.; Yang, S.F.; Hsiao, Y.H. Molecular and Cellular Mechanisms of Metformin in Cervical Cancer. Cancers 2021, 13, 2545. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, J.; Chen, X.; Zhang, F.; Li, X. Aspirin use and endometrial cancer risk: A meta-analysis and systematic review. Ann. Transl. Med. 2020, 8, 461. [Google Scholar] [CrossRef]
- Zhang, D.; Bai, B.; Xi, Y.; Wang, T.; Zhao, Y. Is aspirin use associated with a decreased risk of ovarian cancer? A systematic review and meta-analysis of observational studies with dose-response analysis. Gynecol. Oncol. 2016, 42, 368–377. [Google Scholar] [CrossRef]
- Markowska, A.; Antoszczak, M.; Markowska, J.; Huczyński, A. Statins: HMG-CoA Reductase Inhibitors as Potential Anticancer Agents against Malignant Neoplasms in Women. Pharmaceuticals 2020, 13, 422. [Google Scholar] [CrossRef]
- Rosner, B. Fundamentals of Biostatistics; Nelson Education: Toronto, ON, Canada, 2015. [Google Scholar]
- Zhang, C.; Man, Z.; Nguyen, T. Analysis of 1: M conditional logistic regression modelling method. In Proceedings of the International Congress on Modelling and Simulation, Hobart, Australia, 3–8 December 2017; pp. 942–947. [Google Scholar]




| Characteristics | Cases (With Cancer) (n = 97,736) | Controls (Without Cancer) (n = 390,944) |
|---|---|---|
| Age | ||
| Mean ± SD | 50.81 ± 13.86 | 50.81 ± 13.86 |
| 20–39 y, n (%) | 22,313 (22.83) | 89,252 (22.83) |
| 40–64 y, n (%) | 58,062 (59.41) | 232,248 (59.41) |
| >=65 y, n (%) | 17,361 (17.76) | 69,444 (17.76) |
| Comorbid conditions, n (%) | ||
| Myocardial infarction | 194 (0.20) | 774 (0.20) |
| Congestive heart failure | 1473 (1.51) | 6331 (1.62) |
| Peripheral vascular disease | 602 (0.62) | 2932 (0.75) |
| Cerebrovascular disease | 3723 (3.81) | 17,466 (4.47) |
| Dementia | 627 (0.64) | 3427 (0.88) |
| Chronic pulmonary disease | 2680 (2.74) | 12,665 (3.24) |
| Rheumatic disease | 1363 (1.39) | 6472 (1.66) |
| Peptic ulcer disease | 10,245 (10.48) | 49,475 (12.66) |
| Liver disease | 5058 (5.18) | 24,268 (6.20) |
| Diabetes | 11,622 (11.89) | 55,471 (14.19) |
| Hemiplegia or paraplegia | 157 (0.16) | 770 (0.20) |
| Renal disease | 2019 (2.07) | 8880 (2.27) |
| CCI score | ||
| Mean ± SD | 0.46 ± 0.82 | 0.52 ± 0.92 |
| Other drugs, n (%) | ||
| Metformin | 6817 (6.97) | 33,423 (8.55) |
| Aspirin | 6226 (6.37) | 29,946 (7.66) |
| Statin | 7613 (7.79) | 40,040 (10.24) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, N.T.H.; Nguyen, P.-A.; Huang, C.-W.; Wang, C.-H.; Lin, M.-C.; Hsu, M.-H.; Bao, H.B.; Chien, S.-C.; Yang, H.-C. Renin-Angiotensin-Aldosterone System Inhibitors and Development of Gynecologic Cancers: A 23 Million Individual Population-Based Study. Int. J. Mol. Sci. 2023, 24, 3814. https://doi.org/10.3390/ijms24043814
Nguyen NTH, Nguyen P-A, Huang C-W, Wang C-H, Lin M-C, Hsu M-H, Bao HB, Chien S-C, Yang H-C. Renin-Angiotensin-Aldosterone System Inhibitors and Development of Gynecologic Cancers: A 23 Million Individual Population-Based Study. International Journal of Molecular Sciences. 2023; 24(4):3814. https://doi.org/10.3390/ijms24043814
Chicago/Turabian StyleNguyen, Nhi Thi Hong, Phung-Anh Nguyen, Chih-Wei Huang, Ching-Huan Wang, Ming-Chin Lin, Min-Huei Hsu, Hoang Bui Bao, Shuo-Chen Chien, and Hsuan-Chia Yang. 2023. "Renin-Angiotensin-Aldosterone System Inhibitors and Development of Gynecologic Cancers: A 23 Million Individual Population-Based Study" International Journal of Molecular Sciences 24, no. 4: 3814. https://doi.org/10.3390/ijms24043814