
C-Reactive Protein Levels Are Associated with Complement C4 Deposits and Interstitial Arteritis in ANCA-Associated Renal Vasculitis


Abstract
:1. Introduction
2. Results
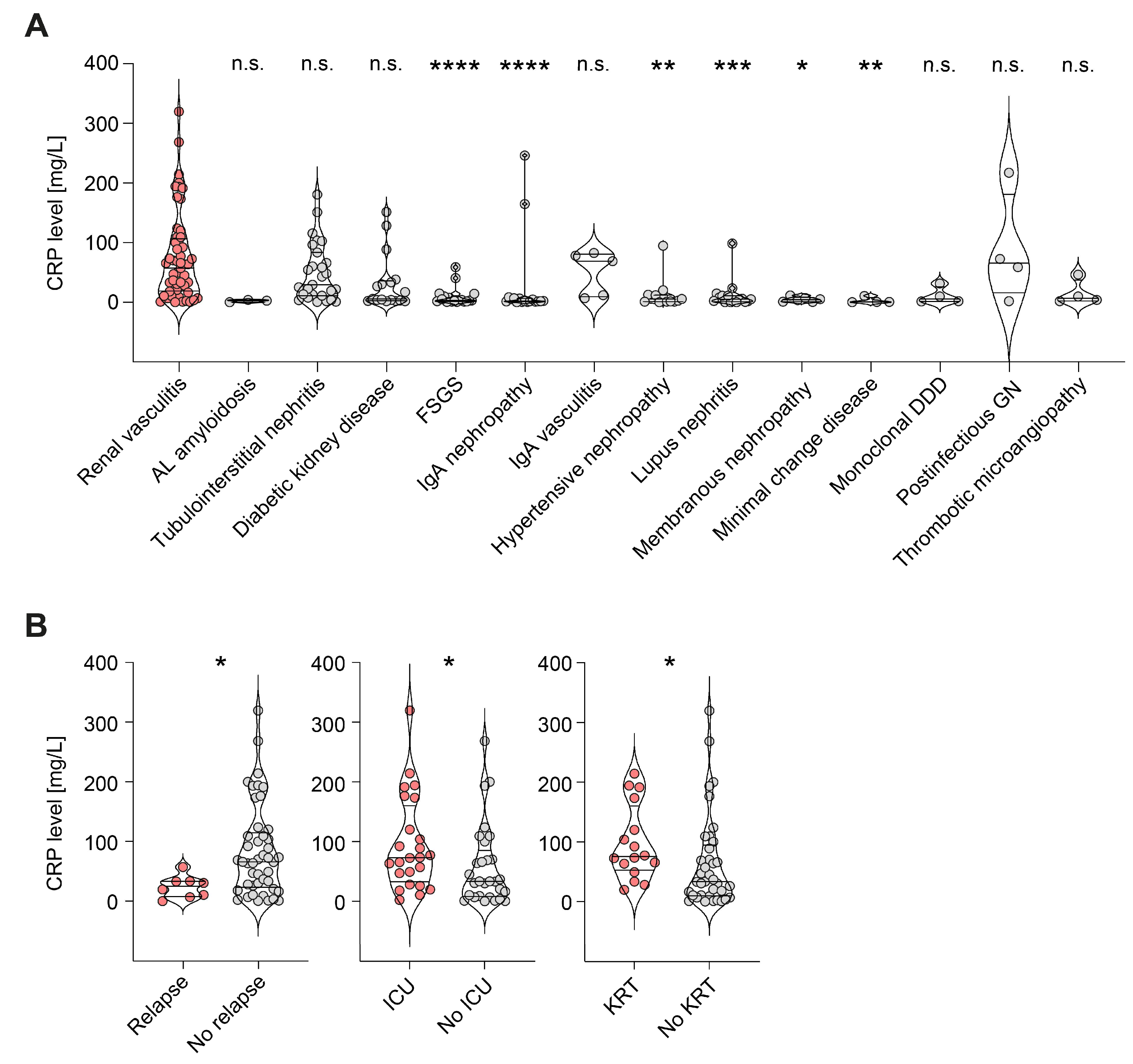
2.1. CRP Elevation Was Associated with Active ANCA-Associated Renal Vasculitis Independent of Extrarenal Disease Manifestations
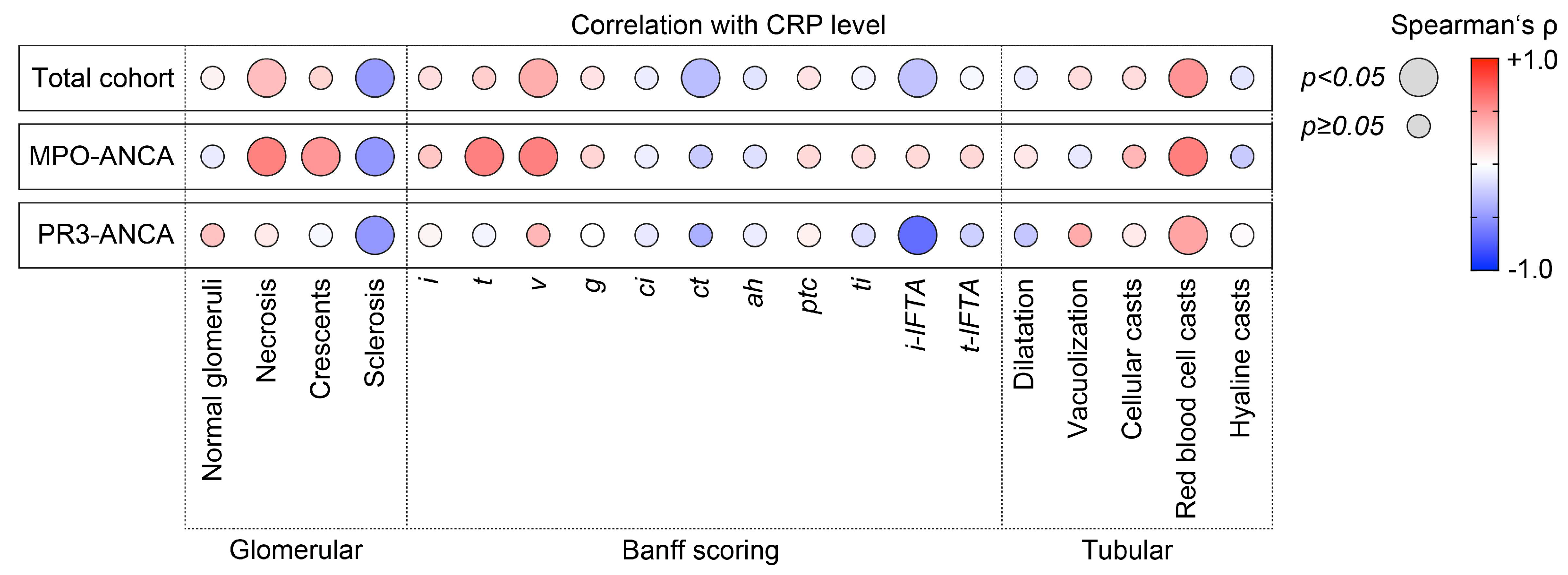
2.2. CRP Levels Were Correlated with Active Glomerular and Tubulointerstitial Renal Vasculitis with MPO-ANCA Seropositivity
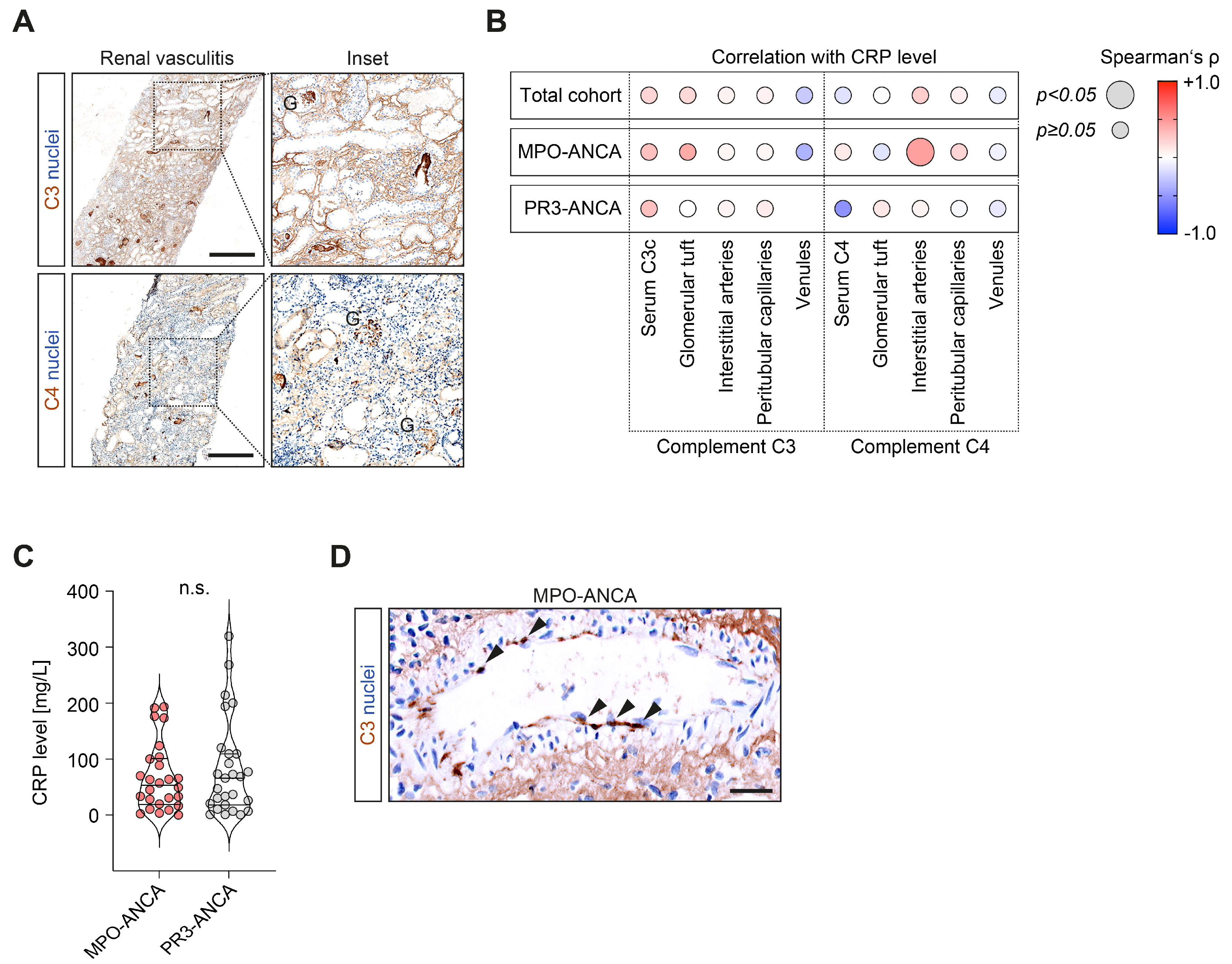
2.3. CRP Elevation Was Correlated with Complement C4 Deposits in Interstitial Arteries in MPO-ANCA-Associated Renal Vasculitis
3. Discussion
4. Materials and Methods
4.1. Study Population and Subgroup Formation
4.2. ANCA Autoantibody and Complement Measurements
4.3. Renal Histopathology
4.4. C3c and C4d Immunohistochemistry
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jennette, J.C.; Nachman, P.H. ANCA Glomerulonephritis and Vasculitis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1680–1691. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.; Gasim, A.; Derebail, V.K.; Chung, Y.; McGregor, J.G.; Lionaki, S.; Poulton, C.J.; Hogan, S.L.; Jennette, J.C.; Falk, R.J.; et al. Predictors of treatment outcomes in ANCA-associated vasculitis with severe kidney failure. Clin. J. Am. Soc. Nephrol. 2014, 9, 905–913. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C.; Wilkman, A.S.; Falk, R.J. Anti-neutrophil cytoplasmic autoantibody-associated glomerulonephritis and vasculitis. Am. J. Pathol. 1989, 135, 921–930. [Google Scholar] [PubMed]
- Flossmann, O.; Berden, A.; de Groot, K.; Hagen, C.; Harper, L.; Heijl, C.; Hoglund, P.; Jayne, D.; Luqmani, R.; Mahr, A.; et al. Long-term patient survival in ANCA-associated vasculitis. Ann. Rheum. Dis. 2011, 70, 488–494. [Google Scholar] [CrossRef]
- Lee, K.H.; Kronbichler, A.; Park, D.D.; Park, Y.; Moon, H.; Kim, H.; Choi, J.H.; Choi, Y.; Shim, S.; Lyu, I.S.; et al. Neutrophil extracellular traps (NETs) in autoimmune diseases: A comprehensive review. Autoimmun. Rev. 2017, 16, 1160–1173. [Google Scholar] [CrossRef]
- Berthelot, J.M.; Le Goff, B.; Neel, A.; Maugars, Y.; Hamidou, M. NETosis: At the crossroads of rheumatoid arthritis, lupus, and vasculitis. Joint Bone Spine 2017, 84, 255–262. [Google Scholar] [CrossRef]
- Frangou, E.; Vassilopoulos, D.; Boletis, J.; Boumpas, D.T. An emerging role of neutrophils and NETosis in chronic inflammation and fibrosis in systemic lupus erythematosus (SLE) and ANCA-associated vasculitides (AAV): Implications for the pathogenesis and treatment. Autoimmun. Rev. 2019, 18, 751–760. [Google Scholar] [CrossRef]
- Kimoto, Y.; Horiuchi, T. The Complement System and ANCA Associated Vasculitis in the Era of Anti-Complement Drugs. Front. Immunol. 2022, 13, 926044. [Google Scholar] [CrossRef]
- Tesar, V.; Hruskova, Z. Complement Inhibition in ANCA-Associated Vasculitis. Front. Immunol. 2022, 13, 888816. [Google Scholar] [CrossRef]
- Peisajovich, A.; Marnell, L.; Mold, C.; Du Clos, T.W. C-reactive protein at the interface between innate immunity and inflammation. Expert Rev. Clin. Immunol. 2008, 4, 379–390. [Google Scholar] [CrossRef]
- Pathak, A.; Agrawal, A. Evolution of C-Reactive Protein. Front. Immunol. 2019, 10, 943. [Google Scholar] [CrossRef]
- Mold, C.; Gewurz, H.; Du Clos, T.W. Regulation of complement activation by C-reactive protein. Immunopharmacology 1999, 42, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; Ngwa, D.N.; Agrawal, A. Complement Activation by C-Reactive Protein Is Critical for Protection of Mice against Pneumococcal Infection. Front. Immunol. 2020, 11, 1812. [Google Scholar] [CrossRef] [PubMed]
- Suresh, M.V.; Singh, S.K.; Ferguson, D.A., Jr.; Agrawal, A. Role of the property of C-reactive protein to activate the classical pathway of complement in protecting mice from pneumococcal infection. J. Immunol. 2006, 176, 4369–4374. [Google Scholar] [CrossRef]
- Shrive, A.K.; Cheetham, G.M.; Holden, D.; Myles, D.A.; Turnell, W.G.; Volanakis, J.E.; Pepys, M.B.; Bloomer, A.C.; Greenhough, T.J. Three dimensional structure of human C-reactive protein. Nat. Struct. Biol. 1996, 3, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Pepys, M.B.; Wood, S.P. The physiological structure of human C-reactive protein and its complex with phosphocholine. Structure 1999, 7, 169–177. [Google Scholar] [CrossRef]
- Tillett, W.S.; Francis, T. Serological Reactions in Pneumonia with a Non-Protein Somatic Fraction of Pneumococcus. J. Exp. Med. 1930, 52, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Volanakis, J.E.; Kaplan, M.H. Specificity of C-reactive protein for choline phosphate residues of pneumococcal C-polysaccharide. Proc. Soc. Exp. Biol. Med. 1971, 136, 612–614. [Google Scholar] [CrossRef]
- Kaplan, M.H.; Volanakis, J.E. Interaction of C-reactive protein complexes with the complement system. I. Consumption of human complement associated with the reaction of C-reactive protein with pneumococcal C-polysaccharide and with the choline phosphatides, lecithin and sphingomyelin. J. Immunol. 1974, 112, 2135–2147. [Google Scholar] [CrossRef]
- Haapasalo, K.; Meri, S. Regulation of the Complement System by Pentraxins. Front. Immunol. 2019, 10, 1750. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.S.; Ahn, S.S.; Park, Y.B.; Lee, S.K.; Lee, S.W. C-Reactive Protein to Serum Albumin Ratio Is an Independent Predictor of All-Cause Mortality in Patients with ANCA-Associated Vasculitis. Yonsei Med. J. 2018, 59, 865–871. [Google Scholar] [CrossRef]
- Tian, Y.; Liu, N.; Yin, H.; Duan, L. Relationship between C-Reactive Protein/Serum Albumin Ratio, Neutrophil/Lymphocyte Ratio, and ANCA-Associated Vasculitis Activity: A Retrospective Single Center Cohort Study. Front. Med. 2022, 9, 855869. [Google Scholar] [CrossRef]
- McGovern, D.; Williams, S.P.; Parsons, K.; Farrah, T.E.; Gallacher, P.J.; Miller-Hodges, E.; Kluth, D.C.; Hunter, R.W.; Dhaun, N. Long-term outcomes in elderly patients with ANCA-associated vasculitis. Rheumatology 2020, 59, 1076–1083. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.L.; Liang, Q.H.; Huang, B.T.; Ding, N.; Li, B.W.; Hao, J. The plasma level of mCRP is linked to cardiovascular disease in antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Res. Ther. 2020, 22, 228. [Google Scholar] [CrossRef] [PubMed]
- Lech, M.; Rommele, C.; Anders, H.J. Pentraxins in nephrology: C-reactive protein, serum amyloid P and pentraxin-3. Nephrol. Dial. Transplant. 2013, 28, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Demiselle, J.; Auchabie, J.; Beloncle, F.; Gatault, P.; Grange, S.; Du Cheyron, D.; Dellamonica, J.; Boyer, S.; Beauport, D.T.; Piquilloud, L.; et al. Patients with ANCA-associated vasculitis admitted to the intensive care unit with acute vasculitis manifestations: A retrospective and comparative multicentric study. Ann. Intensive Care 2017, 7, 39. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, B. Incidence of Arteritis and Peritubular Capillaritis in ANCA-associated Vasculitis. J. Am. Soc. Nephrol. 2021, 32, 2974–2975. [Google Scholar] [CrossRef] [PubMed]
- Boudhabhay, I.; Delestre, F.; Coutance, G.; Gnemmi, V.; Quemeneur, T.; Vandenbussche, C.; Lazareth, H.; Canaud, G.; Tricot, L.; Gosset, C.; et al. Reappraisal of Renal Arteritis in ANCA-Associated Vasculitis: Clinical Characteristics, Pathology, and Outcome. J. Am. Soc. Nephrol. 2021, 32, 2362–2374. [Google Scholar] [CrossRef]
- Brix, S.R.; Noriega, M.; Tennstedt, P.; Vettorazzi, E.; Busch, M.; Nitschke, M.; Jabs, W.J.; Ozcan, F.; Wendt, R.; Hausberg, M.; et al. Development and validation of a renal risk score in ANCA-associated glomerulonephritis. Kidney Int. 2018, 94, 1177–1188. [Google Scholar] [CrossRef]
- Wolbink, G.J.; Brouwer, M.C.; Buysmann, S.; ten Berge, I.J.; Hack, C.E. CRP-mediated activation of complement in vivo: Assessment by measuring circulating complement-C-reactive protein complexes. J. Immunol. 1996, 157, 473–479. [Google Scholar] [CrossRef]
- Kasperska-Zajac, A.; Grzanka, A.; Machura, E.; Misiolek, M.; Mazur, B.; Jochem, J. Increased serum complement C3 and C4 concentrations and their relation to severity of chronic spontaneous urticaria and CRP concentration. J. Inflamm. 2013, 10, 22. [Google Scholar] [CrossRef]
- Murakami, Y.; Imamichi, T.; Nagasawa, S. Characterization of C3a anaphylatoxin receptor on guinea-pig macrophages. Immunology 1993, 79, 633–638. [Google Scholar] [PubMed]
- Elsner, J.; Oppermann, M.; Czech, W.; Kapp, A. C3a activates the respiratory burst in human polymorphonuclear neutrophilic leukocytes via pertussis toxin-sensitive G-proteins. Blood 1994, 83, 3324–3331. [Google Scholar] [CrossRef] [PubMed]
- Elsner, J.; Oppermann, M.; Czech, W.; Dobos, G.; Schopf, E.; Norgauer, J.; Kapp, A. C3a activates reactive oxygen radical species production and intracellular calcium transients in human eosinophils. Eur. J. Immunol. 1994, 24, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Kretzschmar, T.; Jeromin, A.; Gietz, C.; Bautsch, W.; Klos, A.; Kohl, J.; Rechkemmer, G.; Bitter-Suermann, D. Chronic myelogenous leukemia-derived basophilic granulocytes express a functional active receptor for the anaphylatoxin C3a. Eur. J. Immunol. 1993, 23, 558–561. [Google Scholar] [CrossRef]
- el-Lati, S.G.; Dahinden, C.A.; Church, M.K. Complement peptides C3a- and C5a-induced mediator release from dissociated human skin mast cells. J. Invest. Dermatol. 1994, 102, 803–806. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, L.G.; Woodruff, T.M. Is the complement activation product C3a a proinflammatory molecule? Re-evaluating the evidence and the myth. J. Immunol. 2015, 194, 3542–3548. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.J.; Mirtsos, C.; Suh, D.; Lu, Y.C.; Lin, W.J.; McKerlie, C.; Lee, T.; Baribault, H.; Tian, H.; Yeh, W.C. C5L2 is critical for the biological activities of the anaphylatoxins C5a and C3a. Nature 2007, 446, 203–207. [Google Scholar] [CrossRef]
- Daffern, P.J.; Pfeifer, P.H.; Ember, J.A.; Hugli, T.E. C3a is a chemotaxin for human eosinophils but not for neutrophils. I. C3a stimulation of neutrophils is secondary to eosinophil activation. J. Exp. Med. 1995, 181, 2119–2127. [Google Scholar] [CrossRef]
- Tsuruta, T.; Yamamoto, T.; Matsubara, S.; Nagasawa, S.; Tanase, S.; Tanaka, J.; Takagi, K.; Kambara, T. Novel function of C4a anaphylatoxin. Release from monocytes of protein which inhibits monocyte chemotaxis. Am. J. Pathol. 1993, 142, 1848–1857. [Google Scholar]
- Zhao, Y.; Xu, H.; Yu, W.; Xie, B.D. Complement anaphylatoxin C4a inhibits C5a-induced neointima formation following arterial injury. Mol. Med. Rep. 2014, 10, 45–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnum, S.R. C4a: An Anaphylatoxin in Name Only. J. Innate Immun. 2015, 7, 333–339. [Google Scholar] [CrossRef]
- Xu, P.C.; Li, Z.Y.; Yang, X.W.; Zhao, M.H.; Chen, M. Myeloperoxidase influences the complement regulatory function of modified C-reactive protein. Innate Immun. 2014, 20, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Singh, U.; Devaraj, S.; Jialal, I. C-reactive protein stimulates myeloperoxidase release from polymorphonuclear cells and monocytes: Implications for acute coronary syndromes. Clin. Chem. 2009, 55, 361–364. [Google Scholar] [CrossRef]
- Xing, G.Q.; Chen, M.; Liu, G.; Heeringa, P.; Zhang, J.J.; Zheng, X.; Jie, E.; Kallenberg, C.G.; Zhao, M.H. Complement activation is involved in renal damage in human antineutrophil cytoplasmic autoantibody associated pauci-immune vasculitis. J. Clin. Immunol. 2009, 29, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, M. Complement C4, Infections, and Autoimmune Diseases. Front. Immunol. 2021, 12, 694928. [Google Scholar] [CrossRef]
- Mershon-Shier, K.L.; Vasuthasawat, A.; Takahashi, K.; Morrison, S.L.; Beenhouwer, D.O. In vitro C3 deposition on Cryptococcus capsule occurs via multiple complement activation pathways. Mol. Immunol. 2011, 48, 2009–2018. [Google Scholar] [CrossRef]
- Takahashi, M.; Ishida, Y.; Iwaki, D.; Kanno, K.; Suzuki, T.; Endo, Y.; Homma, Y.; Fujita, T. Essential role of mannose-binding lectin-associated serine protease-1 in activation of the complement factor D. J. Exp. Med. 2010, 207, 29–37. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, D.; Baier, E.; Kluge, I.A.; Strobel, P.; Tampe, B. Intrarenal synthesis of complement C3 localized to distinct vascular compartments in ANCA-associated renal vasculitis. J. Autoimmun. 2022, 133, 102924. [Google Scholar] [CrossRef]
- Hakroush, S.; Kluge, I.A.; Baier, E.; Tampe, D.; Tampe, B. Relevance of Complement C4 Deposits Localized to Distinct Vascular Compartments in ANCA-Associated Renal Vasculitis. Int. J. Mol. Sci. 2022, 23, 14325. [Google Scholar] [CrossRef]
- Hakroush, S.; Kluge, I.A.; Strobel, P.; Korsten, P.; Tampe, D.; Tampe, B. Systematic Histological Scoring Reveals More Prominent Interstitial Inflammation in Myeloperoxidase-ANCA Compared to Proteinase 3-ANCA Glomerulonephritis. J. Clin. Med. 2021, 10, 1231. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, D.; Korsten, P.; Strobel, P.; Tampe, B. Complement Components C3 and C4 Indicate Vasculitis Manifestations to Distinct Renal Compartments in ANCA-Associated Glomerulonephritis. Int. J. Mol. Sci. 2021, 22, 6588. [Google Scholar] [CrossRef] [PubMed]
- Tampe, D.; Strobel, P.; Korsten, P.; Hakroush, S.; Tampe, B. Consideration of Therapeutic Plasma Exchange in Association with Inflammatory Lesions in ANCA-Associated Glomerulonephritis: A Real-World Retrospective Study from a Single Center. Front. Immunol. 2021, 12, 645483. [Google Scholar] [CrossRef]
- Tampe, D.; Korsten, P.; Strobel, P.; Hakroush, S.; Tampe, B. Comprehensive Analysis of Sex Differences at Disease Manifestation in ANCA-Associated Glomerulonephritis. Front. Immunol. 2021, 12, 736638. [Google Scholar] [CrossRef] [PubMed]
- Hakroush, S.; Tampe, D.; Strobel, P.; Korsten, P.; Tampe, B. Comparative Histological Subtyping of Immune Cell Infiltrates in MPO-ANCA and PR3-ANCA Glomerulonephritis. Front. Immunol. 2021, 12, 737708. [Google Scholar] [CrossRef]
- Roufosse, C.; Simmonds, N.; Clahsen-van Groningen, M.; Haas, M.; Henriksen, K.J.; Horsfield, C.; Loupy, A.; Mengel, M.; Perkowska-Ptasinska, A.; Rabant, M.; et al. A 2018 Reference Guide to the Banff Classification of Renal Allograft Pathology. Transplantation 2018, 102, 1795–1814. [Google Scholar] [CrossRef]
- Loupy, A.; Haas, M.; Roufosse, C.; Naesens, M.; Adam, B.; Afrouzian, M.; Akalin, E.; Alachkar, N.; Bagnasco, S.; Becker, J.U.; et al. The Banff 2019 Kidney Meeting Report (I): Updates on and clarification of criteria for T cell- and antibody-mediated rejection. Am. J. Transplant. 2020, 20, 2318–2331. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, D.; Korsten, P.; Strobel, P.; Tampe, B. Systematic Scoring of Tubular Injury Patterns Reveals Interplay between Distinct Tubular and Glomerular Lesions in ANCA-Associated Glomerulonephritis. J. Clin. Med. 2021, 10, 2682. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, D.; Korsten, P.; Strobel, P.; Tampe, B. Bowman’s capsule rupture links glomerular damage to tubulointerstitial inflammation in ANCA-associated glomerulonephritis. Clin. Exp. Rheumatol. 2021, 39 (Suppl. S129), 27–31. [Google Scholar] [CrossRef] [PubMed]
- Hakroush, S.; Tampe, B. Neutrophils associate with Bowman’s capsule rupture specifically in PR3-ANCA glomerulonephritis. J. Nephrol. 2022, 35, 1177–1183. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, B. Correspondence on ‘Bowman’s capsule rupture on renal biopsy improves the outcome prediction of ANCA-associated glomerulonephritis classifications’. Ann. Rheum. Dis. 2022, 81, e95. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinical Data | No. of Patients | Manifestation | No. of Manifestation | p-Value |
|---|---|---|---|---|
| Lung—CRP (mg/L) | 31 | 33.4 (18.3–109.5) | 63.7 (17.7–105.3) | 0.9608 |
| Sinus—CRP (mg/L) | 9 | 68.9 (5.1–109.4) | 53.4 (20.1–103.1) | 0.9880 |
| Joint—CRP (mg/L) | 12 | 65 (34.3–104.2) | 49.3 (13.6–106.8) | 0.3847 |
| Ear—CRP (mg/L) | 4 | 55.3 (0.6–177.4) | 57.4 (20.2–102.1) | 0.7070 |
| Eye—CRP (mg/L) | 2 | 191.3 (20.5–268.5) | 53.4 (17.8–101.2) | 0.2222 |
| Nerve—CRP (mg/L) | 6 | 82.5 (26.7–132) | 49.3 (18.3–104) | 0.4189 |
| Skin—CRP (mg/L) | 9 | 63.8 (28.3–71.4) | 53.4 (16.9–109.5) | 0.9138 |
| Variable | β | p-Value |
|---|---|---|
| Glomerular necrosis—% of total | +0.36 | 0.0460 |
| Glomerular crescents—% of total | +0.39 | 0.0229 |
| Tubulitis t—score | +0.29 | 0.1828 |
| Interstitial arteritis v—score | +0.66 | 0.0017 |
| Red blood cell casts—score | +0.45 | 0.0091 |
| Complement C3 | MPO-ANCA | PR3-ANCA | p-Value |
| Glomerular tuft—% of total | 17/26 (65.4) | 20/27 (74.1) | 0.4909 |
| Interstitial arteries—% of total | 1/26 (3.8) | 2/27 (7.4) | 0.5749 |
| Peritubular capillaries—% of total | 17/26 (65.4) | 17/27 (63) | 0.8542 |
| Venules—% of total | 1/26 (3.8) | 0/27 (0) | 0.3036 |
| Complement C4 | MPO-ANCA | PR3-ANCA | p-Value |
| Glomerular tuft—% of total | 17/26 (65.4) | 16/27 (22.2) | 0.6456 |
| Interstitial arteries—% of total | 8/26 (30.8) | 12/27 (44.4) | 0.3045 |
| Peritubular capillaries—% of total | 14/26 (53.8) | 13/27 (48.1) | 0.6783 |
| Venules—% of total | 10/26 (38.5) | 6/27 (22.2) | 0.1980 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korsten, P.; Baier, E.; Hakroush, S.; Tampe, B. C-Reactive Protein Levels Are Associated with Complement C4 Deposits and Interstitial Arteritis in ANCA-Associated Renal Vasculitis. Int. J. Mol. Sci. 2023, 24, 3072. https://doi.org/10.3390/ijms24043072
Korsten P, Baier E, Hakroush S, Tampe B. C-Reactive Protein Levels Are Associated with Complement C4 Deposits and Interstitial Arteritis in ANCA-Associated Renal Vasculitis. International Journal of Molecular Sciences. 2023; 24(4):3072. https://doi.org/10.3390/ijms24043072
Chicago/Turabian StyleKorsten, Peter, Eva Baier, Samy Hakroush, and Björn Tampe. 2023. "C-Reactive Protein Levels Are Associated with Complement C4 Deposits and Interstitial Arteritis in ANCA-Associated Renal Vasculitis" International Journal of Molecular Sciences 24, no. 4: 3072. https://doi.org/10.3390/ijms24043072