
Interleukin-19 Levels Are Increased in Palmoplantar Pustulosis and Reduced following Apremilast Treatment
 , , , , ,
, , , , ,
Abstract
:1. Introduction
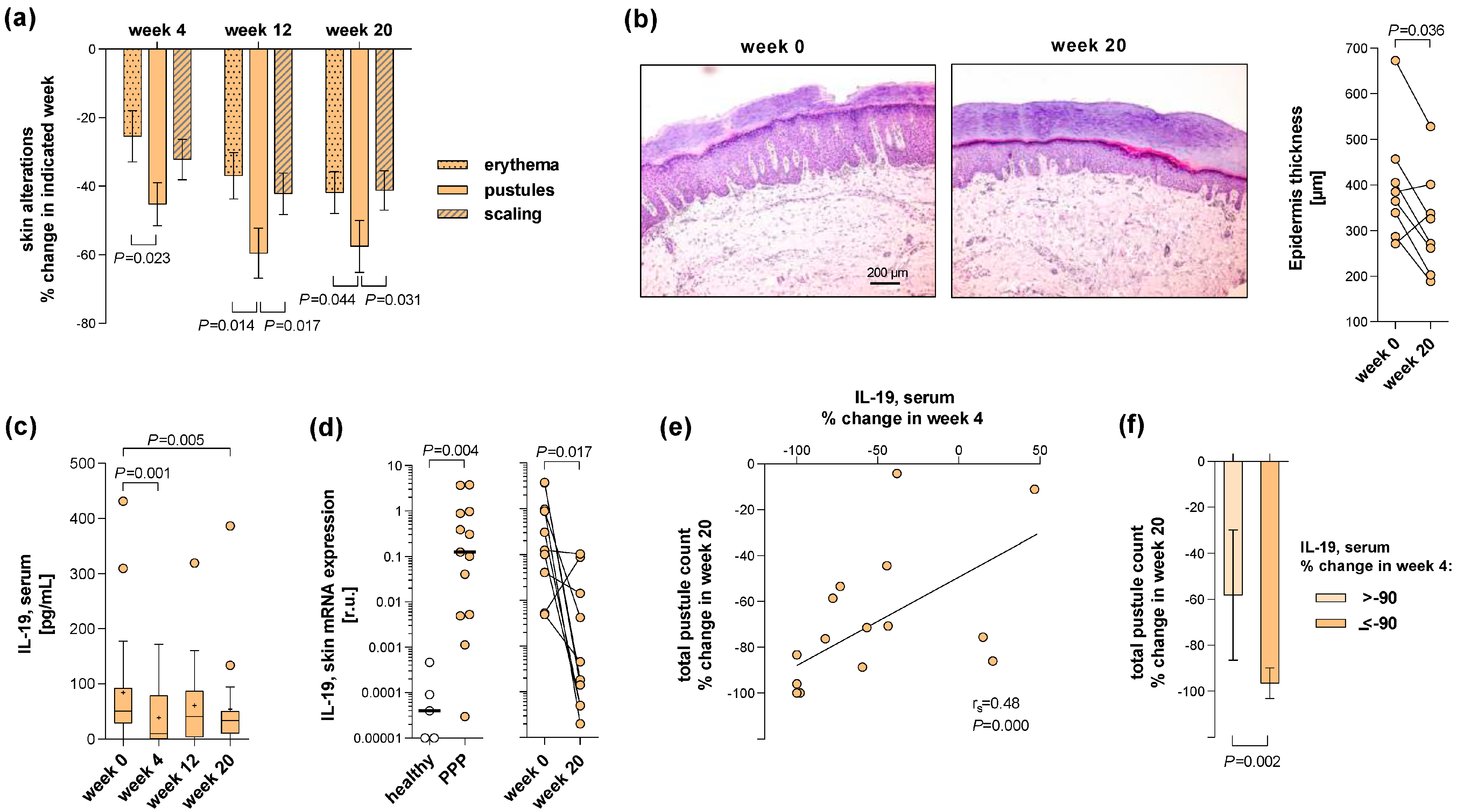
2. Results and Discussion
3. Materials and Methods
3.1. Samples from PPP Patients and Control Participants
3.2. Cell Cultures
3.3. Quantitative mRNA Expression Analysis
3.4. Histology and Immunohistochemistry
3.5. Enzyme-Linked Immunosorbent Assay
3.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Freitas, E.; Rodrigues, M.A.; Torres, T. Diagnosis, Screening and Treatment of Patients with Palmoplantar Pustulosis (PPP): A Review of Current Practices and Recommendations. Clin. Cosmet. Investig. Dermatol. 2020, 13, 561–578. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Kamijima, Y.; Sato, T.; Ooba, N.; Koide, D.; Iizuka, H.; Nakagawa, H. Epidemiology of psoriasis and palmoplantar pustulosis: A nationwide study using the Japanese national claims database. BMJ Open 2015, 5, e006450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lofvendahl, S.; Norlin, J.M.; Schmitt-Egenolf, M. Prevalence and incidence of palmoplantar pustulosis in Sweden: A population-based register study. Br. J. Dermatol. 2021, 185, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Wilsmann-Theis, D.; Jacobi, A.; Frambach, Y.; Philipp, S.; Weyergraf, A.; Schill, T.; Steinz, K.; Gerdes, S.; Mössner, R. Palmoplantar pustulosis—A cross-sectional analysis in Germany. Dermatol. Online J. 2017, 23, 1. [Google Scholar] [CrossRef]
- Misiak-Galazka, M.; Wolska, H.; Galazka, A.; Kwiek, B.; Rudnicka, L. General Characteristics and Comorbidities in Patients with Palmoplantar Pustulosis. Acta Dermatovenerol. Croat. 2018, 26, 109–118. [Google Scholar]
- Trattner, H.; Blüml, S.; Steiner, I.; Plut, U.; Radakovic, S.; Tanew, A. Quality of life and comorbidities in palmoplantar pustulosis—A cross-sectional study on 102 patients. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1681–1685. [Google Scholar] [CrossRef]
- Ghoreschi, K.; Balato, A.; Enerbäck, C.; Sabat, R. Therapeutics targeting the IL-23 and IL-17 pathway in psoriasis. Lancet 2021, 397, 754–766. [Google Scholar] [CrossRef]
- Bissonnette, R.; Suárez-Fariñas, M.; Li, X.; Bonifacio, K.M.; Brodmerkel, C.; Fuentes-Duculan, J.; Krueger, J.G. Based on Molecular Profiling of Gene Expression, Palmoplantar Pustulosis and Palmoplantar Pustular Psoriasis Are Highly Related Diseases that Appear to Be Distinct from Psoriasis Vulgaris. PLoS ONE 2016, 11, e0155215. [Google Scholar]
- Asumalahti, K.; Ameen, M.; Suomela, S.; Hagforsen, E.; Michaelsson, G.; Evans, J.; Munro, M.; Veal, C.; Allen, M.; Leman, J.; et al. Genetic analysis of PSORS1 distinguishes guttate psoriasis and palmoplantar pustulosis. J. Investig. Dermatol. 2003, 120, 627–632. [Google Scholar] [CrossRef]
- Mrowietz, U.; Bachelez, H.; Burden, A.D.; Rissler, M.; Sieder, C.; Orsenigo, R.; Chaouche-Teyara, K. Secukinumab for moderate-to-severe palmoplantar pustular psoriasis: Results of the 2PRECISE study. J. Am. Acad. Dermatol. 2019, 80, 1344–1352. [Google Scholar] [CrossRef] [Green Version]
- Terui, T.; Kobayashi, S.; Okubo, Y.; Murakami, M.; Zheng, R.; Morishima, H.; Goto, R.; Kimura, T. Efficacy and Safety of Guselkumab in Japanese Patients with Palmoplantar Pustulosis: A Phase 3 Randomized Clinical Trial. JAMA Dermatol. 2019, 155, 1153–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bissonnette, R.; Nigen, S.; Langley, R.; Lynde, C.; Tan, J.; Fuentes-Duculan, J.; Krueger, J. Increased expression of IL-17A and limited involvement of IL-23 in patients with palmo-plantar (PP) pustular psoriasis or PP pustulosis; results from a randomised controlled trial. J. Eur. Acad. Dermatol. Venereol. 2013, 28, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- McCluskey, D.; Benzian-Olsson, N.; Mahil, S.K.; Hassi, N.K.; Wohnhaas, C.T.; Burden, A.D.; Griffiths, C.E.; Ingram, J.R.; Levell, N.J.; Parslew, R.; et al. Single-cell analysis implicates TH17-to-TH2 cell plasticity in the pathogenesis of palmoplantar pustulosis. J. Allergy Clin. Immunol. 2022, 150, 882–893. [Google Scholar] [CrossRef]
- Mössner, R.; Frambach, Y.; Wilsmann-Theis, D.; Löhr, S.; Jacobi, A.; Weyergraf, A.; Müller, M.; Philipp, S.; Renner, R.; Traupe, H.; et al. Palmoplantar Pustular Psoriasis Is Associated with Missense Variants in CARD14, but Not with Loss-of-Function Mutations in IL36RN in European Patients. J. Investig. Dermatol. 2015, 135, 2538–2541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolk, K.; Frambach, Y.; Jacobi, A.; Wilsmann-Theis, D.; Phillipp, S.; Witte-Händel, E.; Wenzel, J.; Mössner, R.; Sabat, R. Increased levels of lipocalin 2 in palmoplantar pustular psoriasis. J. Dermatol. Sci. 2018, 90, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Masuda-Kuroki, K.; Murakami, M.; Tokunaga, N.; Kishibe, M.; Mori, H.; Utsunomiya, R.; Tsuda, T.; Shiraishi, K.; Tohyama, M.; Sayama, K. The microbiome of the “sterile” pustules in palmoplantar pustulosis. Exp. Dermatol. 2018, 27, 1372–1377. [Google Scholar] [CrossRef] [PubMed]
- Sabat, R. IL-10 family of cytokines. Cytokine Growth Factor Rev. 2010, 21, 315–324. [Google Scholar] [CrossRef]
- Wilsmann-Theis, D.; Kromer, C.; Gerdes, S.; Linker, C.; Magnolo, N.; Sabat, R.; Reich, K.; Mössner, R. A multicentre open-label study of apremilast in palmoplantar pustulosis (APLANTUS). J. Eur. Acad. Dermatol. Venereol. 2021, 35, 2045–2050. [Google Scholar] [CrossRef]
- Gisondi, P.; Girolomoni, G. Apremilast in the therapy of moderate-to-severe chronic plaque psoriasis. Drug Des. Dev. Ther. 2016, 10, 1763–1770. [Google Scholar] [CrossRef] [Green Version]
- Wolk, K.; Kunz, S.; Asadullah, K.; Sabat, R. Cutting edge: Immune cells as sources and targets of the IL-10 family members? J. Immunol. 2002, 168, 5397–5402. [Google Scholar] [CrossRef] [Green Version]
- Wolk, K.; Witte, K.; Witte, E.; Proesch, S.; Schulze-Tanzil, G.; Nasilowska, K.; Thilo, J.; Asadullah, K.; Sterry, W.; Volk, H.-D.; et al. Maturing dendritic cells are an important source of IL-29 and IL-20 that may cooperatively increase the innate immunity of keratinocytes. J. Leukoc. Biol. 2008, 83, 1181–1193. [Google Scholar] [CrossRef] [PubMed]
- Kunz, S.; Wolk, K.; Witte, E.; Witte, K.; Doecke, W.-D.; Volk, H.-D.; Sterry, W.; Asadullah, K.; Sabat, R. Interleukin (IL)-19, IL-20 and IL-24 are produced by and act on keratinocytes and are distinct from classical ILs. Exp. Dermatol. 2006, 15, 991–1004. [Google Scholar] [CrossRef] [PubMed]
- Witte, E.; Kokolakis, G.; Witte, K.; Philipp, S.; Doecke, W.D.; Babel, N.; Wittig, B.M.; Warszawska, K.; Kurek, A.; Erdmann-Keding, M.; et al. IL-19 is a component of the pathogenetic IL-23/IL-17 cascade in psoriasis. J. Investig. Dermatol. 2014, 134, 2757–2767. [Google Scholar] [CrossRef] [Green Version]
- Wolk, K.; Kunz, S.; Witte, E.; Friedrich, M.; Asadullah, K.; Sabat, R. IL-22 Increases the Innate Immunity of Tissues. Immunity 2004, 21, 241–254. [Google Scholar] [CrossRef] [Green Version]
- Christophers, E.; Schroder, J.M. Evolution of innate defense in human skin. Exp. Dermatol. 2022, 31, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Kingo, K.; Mossner, R.; Koks, S.; Rätsep, R.; Kruger, U.; Vasar, E.; Reich, K.; Silm, H. Association analysis of IL19, IL20 and IL24 genes in palmoplantar pustulosis. Br. J. Dermatol. 2007, 156, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Wolk, K.; Mitsui, H.; Witte, K.; Gellrich, S.; Gulati, N.; Humme, D.; Witte, E.; Gonsior, M.; Beyer, M.; Kadin, M.E.; et al. Deficient Cutaneous Antibacterial Competence in Cutaneous T-Cell Lymphomas: Role of Th2-Mediated Biased Th17 Function. Clin. Cancer Res. 2014, 20, 5507–5516. [Google Scholar] [CrossRef] [Green Version]
- Nauseef, W.M. Isolation of human neutrophils from venous blood. Methods Mol. Biol. 2007, 412, 15–20. [Google Scholar]
- Wolk, K.; Brembach, T.; Šimaitė, D.; Bartnik, E.; Cucinotta, S.; Pokrywka, A.; Irmer, M.; Triebus, J.; Witte-Händel, E.; Salinas, G.; et al. Activity and components of the granulocyte colony-stimulating factor pathway in hidradenitis suppurativa. Br. J. Dermatol. 2021, 185, 164–176. [Google Scholar] [CrossRef]
- Wolk, K.; Haugen, H.S.; Xu, W.; Witte, E.; Waggie, K.; Anderson, M.; Vom Baur, E.; Witte, K.; Warszawska, K.; Philipp, S.; et al. IL-22 and IL-20 are key mediators of the epidermal alterations in psoriasis while IL-17 and IFN-gamma are not. J. Mol. Med. 2009, 87, 523–536. [Google Scholar] [CrossRef]
- Wolk, K.; Wenzel, J.; Tsaousi, A.; Witte-Händel, E.; Babel, N.; Zelenak, C.; Volk, H.; Sterry, W.; Schneider-Burrus, S.; Sabat, R. Lipocalin-2 is expressed by activated granulocytes and keratinocytes in affected skin and reflects disease activity in acne inversa/hidradenitis suppurativa. Br. J. Dermatol. 2017, 177, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- Wolk, K.; Warszawska, K.; Hoeflich, C.; Witte, E.; Schneider-Burrus, S.; Witte, K.; Kunz, S.; Buss, A.; Roewert, H.J.; Krause, M.; et al. Deficiency of IL-22 Contributes to a Chronic Inflammatory Disease: Pathogenetic Mechanisms in Acne Inversa. J. Immunol. 2010, 186, 1228–1239. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PPP Patients (n = 68) | Healthy Donors (n = 19) | PsV Patients (n = 44) | |
|---|---|---|---|
| Age (years), mean ± SD; range | 49.5 ± 13.7; 18–78 | 43.8 ± 8.1; 33–58 | 39.0 ± 12.1; 19–64 |
| Sex distribution (% female) | 78 | 79 | 52 |
| PPP pustule score *, mean ± SD; range | 3.00 ± 1.23; 1–5 | - | - |
| PASI | - | - | 11.9 ± 5.7; 3.0–31.7 |
| Disease duration (years), mean ± SD; range | 7.6 ± 10.6; 0–43 | - | 15.9 ± 11.6; 1–42 |
| Healthy Donors (n = 5) | PsV Patients (n = 13) | |
|---|---|---|
| Age (years), mean ± SD; range | 54.6 ± 8.8; 43–63 | 45.8 ± 12.4; 25–63 |
| Sex distribution (% female) | 80 | 15 |
| PASI | - | 15.7 ± 10.9; 6.1–36.5 |
| Disease duration (years), mean ± SD; range | - | 20.0 ± 11.6; 6–42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolk, K.; Wilsmann-Theis, D.; Witte, K.; Brembach, T.-C.; Kromer, C.; Gerdes, S.; Ghoreschi, K.; Reich, K.; Mössner, R.; Sabat, R. Interleukin-19 Levels Are Increased in Palmoplantar Pustulosis and Reduced following Apremilast Treatment. Int. J. Mol. Sci. 2023, 24, 1276. https://doi.org/10.3390/ijms24021276
Wolk K, Wilsmann-Theis D, Witte K, Brembach T-C, Kromer C, Gerdes S, Ghoreschi K, Reich K, Mössner R, Sabat R. Interleukin-19 Levels Are Increased in Palmoplantar Pustulosis and Reduced following Apremilast Treatment. International Journal of Molecular Sciences. 2023; 24(2):1276. https://doi.org/10.3390/ijms24021276
Chicago/Turabian StyleWolk, Kerstin, Dagmar Wilsmann-Theis, Katrin Witte, Theresa-Charlotte Brembach, Christian Kromer, Sascha Gerdes, Kamran Ghoreschi, Kristian Reich, Rotraut Mössner, and Robert Sabat. 2023. "Interleukin-19 Levels Are Increased in Palmoplantar Pustulosis and Reduced following Apremilast Treatment" International Journal of Molecular Sciences 24, no. 2: 1276. https://doi.org/10.3390/ijms24021276