
Human Lung Mast Cells: Therapeutic Implications in Asthma
by
 , ,
, ,
Remo Poto
1,2 ,
,
Gjada Criscuolo
1,2,
Gianni Marone
1,2,3,4,
Chris E. Brightling
5 and
Gilda Varricchi
1,2,3,4,* 1
Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
2
Center for Basic and Clinical Immunology Research (CISI), University of Naples Federico II, 80131 Naples, Italy
3
World Allergy Organization (WAO), Center of Excellence (CoE), 80131 Naples, Italy
4
Institute of Experimental Endocrinology and Oncology “G. Salvatore”, National Research Council (CNR), 80131 Naples, Italy
5
Department of Respiratory Sciences, Leicester NIHR BRC, Institute for Lung Health, University of Leicester, Leicester LE1 7RH, UK
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2022, 23(22), 14466; https://doi.org/10.3390/ijms232214466
Submission received: 27 October 2022
/
Revised: 15 November 2022
/
Accepted: 18 November 2022
/
Published: 21 November 2022
(This article belongs to the Special Issue Molecular Research and Therapy of Asthma)
Abstract
:Mast cells are strategically located in different compartments of the lung in asthmatic patients. These cells are widely recognized as central effectors and immunomodulators in different asthma phenotypes. Mast cell mediators activate a wide spectrum of cells of the innate and adaptive immune system during airway inflammation. Moreover, these cells modulate the activities of several structural cells (i.e., fibroblasts, airway smooth muscle cells, bronchial epithelial and goblet cells, and endothelial cells) in the human lung. These findings indicate that lung mast cells and their mediators significantly contribute to the immune induction of airway remodeling in severe asthma. Therapies targeting mast cell mediators and/or their receptors, including monoclonal antibodies targeting IgE, IL-4/IL-13, IL-5/IL-5Rα, IL-4Rα, TSLP, and IL-33, have been found safe and effective in the treatment of different phenotypes of asthma. Moreover, agonists of inhibitory receptors expressed by human mast cells (Siglec-8, Siglec-6) are under investigation for asthma treatment. Increasing evidence suggests that different approaches to depleting mast cells show promising results in severe asthma treatment. Novel treatments targeting mast cells can presumably change the course of the disease and induce drug-free remission in bronchial asthma. Here, we provide an overview of current and promising treatments for asthma that directly or indirectly target lung mast cells.
Keywords:
airway remodeling; asthma; basophil; biological therapies; eosinophil; macrophage; mast cell1. Introduction
Mast cells, first identified in humans by Paul Ehrlich in 1878 [1], play a role in allergic [2,3] and autoimmune disorders [4], microbial infections [5], cardiovascular diseases [6,7], immunodeficiencies [8], and cancer [9,10,11]. Mast cells are derived from CD34+ haemopoietic progenitors that migrate from the bone marrow to the blood and mature in almost all tissues [12]. These cells release a plethora of mediators and display several surface receptors [13,14]. Mast cells uniquely express the cell surface receptor of stem cell factor (SCF) [15], also known as KIT or CD117. SCF plays a critical role in the differentiation, proliferation, and modulation of human and rodent mast cells [16].
In the 1990s, human mast cells that contain only tryptase were termed MCT, whereas those that express both tryptase and chymase were classified as MCTC [17,18]. There are also definitions of mast cells being inflammatory, pro-, or anti-tumorigenic [19,20,21]. The transcriptional profiles of mast cells clearly demonstrate the heterogeneity of mast cells and their different gene expression [14,22,23,24]. Moreover, human mast cells analyzed ex vivo or differentiated in vitro showed significant differences [24]. Human and mouse mast cells have distinct proteomes and unique gene expressions compared to other immune cells [22,25]. Single-cell transcriptomics of human lungs provide evidence of mast cells [26,27]. Different triggers (e.g., IgE-mediated or IL-33) can induce distinct genomic and transcriptional changes in human mast cells [28]. Individual mast cells are exposed to their local environment (e.g., cytokines, different pH, growth factors, etc.) and, over time, are tuned by many different activating and inhibitory signals. Mast cells in different organs differ in their receptor and mediator expression, but there is also considerable heterogeneity among human lung mast cells [29]. It is possible to speculate that individual mast cells could all be unique to some extent.
In this review, we provide an overview of current and promising treatments for asthma that directly or indirectly target lung mast cells.
2. Activating and Inhibitory Receptors on Human Mast Cells
Human mast cells display a wide spectrum of cell surface receptors that can be activated by several immunologic and non-immunologic stimuli that modulate their development and effector functions [11,30]. Figure 1 schematically illustrates the main activating and inhibitory receptors on human lung mast cells relevant to bronchial asthma.
3. Role of Mast Cells in Asthma
FcεRI cross-linking by allergens, anti-IgE, or super allergens results in the release of histamine, cytokines/chemokines, enzymes such as tryptase and chymase, and the generation of eicosanoids (i.e., LTC4 and PGD2) from human mast cells [32,134]. Mast cell-derived mediators are responsible for bronchoconstriction, airway inflammation, and remodeling in different asthma endotypes [2]. The density of mast cells within airway smooth muscle (ASM) bundles is increased in asthmatic patients compared to controls [90]. There is an inverse correlation between the number of mast cells in the ASM and airway hyperresponsiveness (AHR) in asthmatics [90]. HLMCs adhere avidly to ASM cells [135], which favor mast cell survival and activation [136]. Elevated circulating mast cell progenitors are correlated with reduced lung function in allergic asthma [137]. The rapid IgE-dependent release of histamine and eicosanoids (e.g., LTC4 and PGD2) from isolated HLMCs [138] correlates with these mediators in bronchoalveolar lavage fluids following bronchial allergen challenge [139,140,141]. Histamine can promote mucus secretion and bronchoconstriction. Asthma is accompanied by airway remodeling [142] and angiogenesis [143,144], and lung mast cells may contribute to this by the release of several cytokines, chemokines [88], and VEGFs [58,126,145,146]. Submucosal mast cells, which are abundant in healthy controls, are shifted from the submucosal compartment to the epithelium in asthma [147]. IL-33-activated mast cells increase the expression of epithelial IL33, which in turn upregulates the production of type-2 cytokines (i.e., IL-5, IL-13, IL-4) in mast cells. These findings demonstrate a shift in the location of mast cells to the epithelium in asthma and identify intraepithelial mast cells as critical modulators of inflammation in asthma. Psychological stress is thought to induce mast cell activation via the stimulation of peripheral nerves and the release of substance P and corticotropin-release hormone (CRH) [148]. Human mast cells express CRH receptors and their activation induces the selective release of VEGF-A without degranulation [149]. These findings provide a hypothetical link between stress, mast cell activation, and asthma exacerbations [150]. The role of HLMCs in inducing the symptoms of human airway inflammation is also supported by the efficacy of drugs, which block either their function or target mediators primarily released by these cells.
4. Mast Cell-Targeted Treatments for Bronchial Asthma
4.1. Histamine Receptors
Although second-generation H1 antihistamines are widely used for the treatment of allergic rhinitis and urticaria [152,153], their therapeutic role in asthma is marginal. Histamine H4 receptor mediates chemotaxis of HLMCs [154]. In preclinical models, H4 receptor antagonists (e.g., JNJ39758979, ZPL-3893787, and toreforant) exhibited some anti-inflammatory effects. Some have been tested in randomized control trials (RCTs) for allergic diseases with mixed results [155,156,157].
4.2. Tryptase
Circulating β-tryptase levels were increased in asthmatics independently of type 2 inflammation and associated with lesser omalizumab response [92]. MTPS9579A, a mAb that inhibits the activity of tryptase, is in a phase II trial in patients with moderate-to-severe asthma (NCT04092582). E104 and 31A.v11 are anti-tryptase mAbs showing promising effects in preclinical models of allergic reactions [92,158].
4.3. Prostaglandin D2
PGD2, the major cyclooxygenase mediator synthesized by HLMCs, activates the CRTh2 on T helper 2 cells (Th2 cells) [159]. Several CRTh2 antagonists [i.e., fevipiprant, timapiprant (OC-459), AZD1981, BI671800, and setipiprant] failed to show efficacy in asthma and allergic rhinitis patients. In particular, fevipiprant was not effective in phase III trials in asthmatics [160]. GB001, a novel CRTh2 antagonist, was well tolerated and resulted in some benefits in reducing asthma exacerbations [161].
4.4. Cysteinyl Leukotrienes
Leukotriene inhibitors (i.e., montelukast, zafirlukast, pranlukast, and zileuton) have been used with mixed results in allergic diseases. Montelukast, approved by the Food and Drug Administration (FDA) for the treatment of asthma and allergic rhinitis [162], is less effective compared to inhaled or intranasal glucocorticoids [163]. AZD5718, a reversible 5-lipoxygenase activating protein (FLAP) that suppresses leukotriene synthesis, is currently in Phase II trial for moderate-to-severe asthma treatment compared to montelukast (NCT05251259).
4.5. Mast Cell Cytokines and Their Receptors
IL-13 and IL-5 are produced by HLMCs [107]. Phase III studies demonstrated that two anti-IL-13 mAbs, lebrikizumab [164] and tralokinumab [165,166], did not reduce asthma exacerbation rates but did improve lung function in patients with severe asthma [166,167,168]. In contrast, dupilumab, a mAb which is a dual inhibitor of IL-4 and IL-13 through blockade of their shared IL-4Rα subunit, is approved for the treatment of severe uncontrolled asthma and chronic rhinosinusitis with nasal polyps [169,170,171]. The anti-IL-5 mAbs, mepolizumab [172,173] and reslizumab [174], and the anti-IL-5Rα mAb benralizumab [175] are approved as add-on therapy for the treatment of severe eosinophilic asthma [176]. These drugs markedly deplete blood eosinophils and decrease the frequency of asthma exacerbations and improve lung function in patients with severe uncontrolled asthma [174,177,178]. TNF-α is released by mouse mast cells [5], but its production by HLMCs is still controversial. Golimumab, a human mAb anti-TNF-α, showed an increase in adverse events and inconsistent efficacy in severe asthma patients [179].
A mAb anti-IL-17R, brodalumab, did not demonstrate efficacy in asthma [180]. Although mast cells are a major source of several cytokines, their production of other cytokines (i.e., IL-17A) may be selectively restricted to mast cell subtypes (e.g., synovial and skin mast cells [181]). Mast cells are also a source of IL-23 and express IL-23R [181]. Risankizumab, a mAb anti-IL-23, showed increased asthma worsening in a phase 2a trial [182].
4.6. Alarmins and Their Receptors
There is increasing evidence that bronchial epithelial cells represent not only a physical barrier but also an immune organ, which plays a central role in asthma pathobiology [183,184]. TSLP, IL-33, and IL-25 are upstream epithelial-derived cytokines, collectively known as alarmins [40,43,185]. These cytokines also activate downstream a broad range of cellular targets, including mast cells, to propagate the release of several cytokines involved in asthma [40].
4.7. Tezepelumab
Tezepelumab is a human IgG2λ mAb, which binds to TSLP, which is involved in different asthma phenotypes [40]. TSLP is overexpressed by the airway epithelium of asthmatics [115]. TSLP levels are increased in the BAL fluid of asthmatics [186] and serum during asthma exacerbations [187]. Tezepelumab was recently approved by the FDA and European Medicines Agency (EMA) for severe asthma treatment with no phenotype or biomarker limitations. In RCTs, tezepelumab reduced annual exacerbation rates regardless of blood eosinophil count, with an increase in prebronchodilator FEV1 compared to the placebo group [188,189]. In two different RCTs, tezepelumab reduced AHR, suggesting an effect on lung mast cell activation [190,191]. TSLP can promote airway remodeling in asthma through different mechanisms: it activates human lung fibroblasts [192] and causes angiogenic and lymphangiogenic factor release from HLMs [193]. In the phase II CASCADE study, the effects of tezepelumab on airway remodeling were examined in moderate-to-severe asthmatics [190]. Tezepelumab reduced airway submucosal eosinophils compared to placebo. A human mAb anti-TSLP (HBM9378) [194] and an inhaled antibody fragment against TSLP (CSJ117) [195] (NCT03138811; NCT04410523; NCT04946318) are under development for asthma treatment. Figure 4 schematically illustrates the inhibition of mast cell activation by different biologics and drugs.
4.8. Itepekimab
Itepekimab is a human IgG4 mAb that binds to IL-33. In a phase 2 trial, the safety and efficacy of itepekimab, dupilumab, itepekimab plus dupilumab, or placebo were compared in moderate-to-severe asthmatics [200]. Loss of asthma control was similar in the three groups but better than in the placebo. Itepekimab and dupilumab monotherapies increased pre-bronchodilator FEV1, reduced peripheral blood eosinophils, and improved asthma control and quality of life compared to placebo.
4.9. Astegolimab and Etokimab
Astegolimab is a human IgG2 mAb that targets ST2, the IL-33 receptor, and blocks IL-33 signaling [46,202]. In the phase 2b ZENYATTA study, astegolimab was well-tolerated and reduced the number of exacerbation rates in severe asthma patients [202]. Astegolimab did not significantly modify FEV1 compared to placebo in the entire population of asthmatics. FEV1 improvement appeared to be higher in patients with low blood eosinophils.
Etokimab (ANB020) is a humanized mAb that binds to IL-33. A preliminary study found that etokimab has the potential to desensitize subjects allergic to peanuts [201].
4.10. Tozorakimab
Tozorakimab (formerly MEDI3506) is a mAb that binds to IL-33 [216]. RCTs are evaluating the safety and efficacy of tozorakimab compared to placebo in adults with moderate-to-severe asthma (NCT04570657) and chronic obstructive pulmonary disease (COPD) with a history of exacerbations (NCT05166889).
mAbs blocking IL-25 have shown beneficial effects in a mouse model of allergic asthma [217].
4.11. FcεRI and IgE
Omalizumab, a humanized IgG1-k mAb that binds to Fcε, was the first mAb approved by the FDA for the treatment of patients with moderate and severe asthma [218]. It binds to free IgE and inhibits the IgE–FcεRI interaction by preventing the binding of IgE to FcεRI on human mast cells and basophils. Omalizumab also downregulates FcεRI expression [219]. Omalizumab did not improve FEV1 in RCTs [220,221,222], but there is some evidence that it can improve FEV1 in real-life settings [212,222]. It reduces asthma symptoms and exacerbations [223,224,225].
Ligelizumab is a second-generation humanized anti-IgE mAb, which has a higher affinity for the Cε3 domain of IgE compared to omalizumab and may affect IgE production by B cells [213]. Ligelizumab failed to meet the primary endpoints in phase II clinical trials of asthma, and it was discontinued (NCT02075008, NCT02336425). The safety and efficacy of ligelizumab are presently investigated in chronic urticaria (NCT05024058, NCT04513548, NCT03580356, NCT03580369, NCT02477332, NCT04903613). There are several promising compounds targeting FcεRI and/or IgE under investigation. GI-301, an IgE trap-Fc fusion protein, and the anti-IgE mAb UB-221 showed higher affinity to IgE compared to omalizumab (NCT05298215). Combined treatment with omalizumab and omalizumab-resistant IgE–Fc fragment (IgE-R419N-Fc3-4 mutant) caused more inhibition of basophil activation than either agent alone [226]. It has been proposed that exon skipping of the β-subunit of FcεRI in mast cells eliminated FcεRI expression and function in these cells [227].
4.12. Intracellular Signaling Pathways
Several promising small molecular weight compounds target intracellular signaling pathways, including spleen tyrosine kinase (SYK), Bruton’s tyrosine kinase (BTK), and Janus kinase (JAK), to block mast cell activation [214,228,229]. SYK inhibitors (i.e., fostamatinib, LAS189386, TAS05567, BAY61-3606) and aerosolized SYK antisense oligodeoxynucleotides block mast cell degranulation and inhibit models of allergic disorders [230,231,232,233]. SYK inhibitors also inhibit IgE-mediated contraction of human lung slices and histamine and leukotriene release [234]. The intranasal SYK inhibitor R112 improved symptoms in seasonal rhinitis patients [235,236].
Several BTK inhibitors are used for the management of hematological tumors [237] and are in development for the treatment of mast cell-driven diseases, including acalabrutinib for anaphylaxis [238] (NCT05038904), remibrutinib for CSU and food allergy (NCT05432388, NCT05032157, NCT05170724, NCT05513001), fenebrutinib for CSU (NCT036933625), and ibrutinib for food allergy [239] and anaphylaxis (NCT03149315). Concern has risen regarding the risk of cardiovascular adverse events associated with BTK inhibitors [237].
A phase I study assessed the safety and efficacy of GDC-0214, an inhaled JAK inhibitor, in adults with mild asthma [214]. This compound caused a dose-dependent reduction in fractional exhaled nitric oxide (FeNo) in patients with mild asthma. Additional studies on the effects of JAK inhibitors are expected for asthma treatment [240].
4.13. Silencing Mast Cells
Mast cells display several inhibitory receptors (i.e., Siglec-8, Siglec-6, CD200R, CD300a, and FcγRIIb) which inhibit mast cell activation [71]. An anti-Siglec-8 antibody inhibited anaphylaxis in humanized mice and IgE-dependent and IgE-independent activation of human mast cells in lung tissues [241,242,243]. Lirentelimab (AK002), a humanized anti-Siglec-8 mAb, showed promising activity in eosinophilic gastritis and duodenitis [244]. RCTs in eosinophilic esophagitis (NCT04322708), allergic conjunctivitis (NCT03379311), chronic urticaria (NCT03436797), and indolent systemic mastocytosis (NCT02808793) are ongoing. Lirentelimab reduced circulating eosinophil and tissue mast cells in eosinophilic gastrointestinal disease patients [245]. Lirentelimab depletes sputum eosinophils from asthmatic subjects and inhibits FcεRI-mediated HLMC activation [242]. Lirentelimab is presently under investigation in patients with atopic dermatitis (NCT05155085), CSU (NCT05528861), and eosinophilic duodenitis (NCT04856891).
AK006, a humanized IgG1 agonistic Siglec-6 mAb, inhibits mast cell activation in vitro. Interestingly, co-culturing human mast cells with macrophages in the presence of AK006 induces antibody-dependent phagocytosis of mast cells [215]. These findings represent a novel strategy to selectively reduce mast cells via Siglec-6 targeting.
LY3454738, a CD200R agonist, is under development for atopic dermatitis and CSU. Bispecific antibodies that cross-link either IgE [246] or KIT [247] and CD300a, and co-aggregate FcεRI with FcγRIIb, inhibited FcεRI-induced or KIT-induced signaling. An engineered protein inhibitor, designed ankyrin repeat protein (DARPin) E2-79 blocks IgE- FcεRI interactions and favors the dissociation of preformed ligand (IgE)-FcεRI complexes. Anti-IgE DARPin-Fc fusion protein inhibits allergen-induced basophil activation [248,249].
4.14. Depleting Mast Cells
Human mast cells express high levels of KIT throughout their development [16]. Activation of KIT by SCF influences several aspects of mast cell responses. Dysregulation of the SCF/KIT pathway markedly alters mast cell homeostasis. For instance, loss-of-function mutations in SCF or KIT result in mast cell deficiency; in contrast, gain-of-function mutations in KIT lead to mast cell hyperplasia and activation, as found in mastocytosis [250,251,252]. The blockage of the SCF/KIT pathway has been investigated in several models of allergic disorders [253,254,255,256,257]. A bispecific antibody cross-linking KIT and CD300a [247] inhibit SCF-induced human mast cell differentiation and survival and skin reactions induced by SCF in mice [247].
Mast cell apoptosis can be achieved via neutralization of the effects of SCF and/or blockage of its receptor KIT (CD117) (Figure 5). CDX-0159 (Celldex Therapeutics, NJ, USA) is a humanized mAb that binds to the extracellular dimerization domain of KIT [258,259]. This mAb is under investigation in CSU (NCT04538794) and chronic inducible urticaria (NCT04548869). In a phase Ia trial, CDX-0159 administration showed a favorable safety profile and caused a marked reduction of peripheral blood tryptase, suggestive of systemic mast cell depletion (NCT04146129). It remains to be evaluated whether this mAb may work in experimental models of asthma [256].
Another approach to block KIT signaling in mast cells is to use specific tyrosine kinase inhibitors (TKIs) (Figure 5). There are several classes of KIT-targeting TKIs, which display distinct pharmacologic characteristics on human mast cells in vitro [260]. KIT-targeting drugs can inhibit mast cell activation and mediator-induced symptoms in allergic disorders [265,266,267,268]. There are very preliminary data on the in vivo efficacy of KIT-specific or multitargeted TKIs in the treatment of patients with severe allergic disorders (e.g., severe asthma). The administration of masitinib to patients with severe glucocorticoid-dependent asthma was associated with steroid-sparing effects [264]. Imatinib did not influence lung function. In another study, imatinib reduced airway hyperresponsiveness in patients with severe asthma compared to controls [262].
In a phase III trial, masitinib reduced asthma exacerbations compared to placebo in severe asthma patients [263]. Avapritinib (BLU-285), a potent inhibitor of mutant KIT and PDGFRA with activation loop mutations, induces mast cell cytoreduction and remission in the majority of advanced systemic mastocytosis patients [269,270]. It should be emphasized that some of these TKIs also inhibit IgE-dependent basophil activation [271,272,273]. This is relevant because basophils play a role in allergic disorders [88,274]. Future studies should evaluate the safety and efficacy of imatinib, masitinib, and possibly newer TKIs in patients with different phenotypes of severe asthma.
5. Discussion and Conclusions
Human mast cells were identified and named over 140 years ago by Paul Ehrlich [1]. IgE was discovered by Kimishige and Teruko Ishizaka [275] and Gunnar Johansson [276]. The approval of omalizumab, the first mAb anti-IgE for the treatment of asthma in 2003, was a breakthrough in the treatment of patients with mast cell-driven diseases, such as asthma and CSU. Since then, several biologics targeting mast cells directly or indirectly have been approved for the treatment of severe asthma. In particular, mAbs targeting IL-5 (mepolizumab [204,205,206,207] and reslizumab [208,209]), IL-5Rα (benralizumab) [175,210,211], IL-4Rα (dupilumab) [169,170,171,212], and TSLP (tezepelumab) [188,189] have been demonstrated to reduce annual exacerbation rates and also certain features (e.g., FEV1) of airway remodeling in severe asthmatic patients. The efficacy and safety of the above mAbs have been recently discussed in detail [142]. Collectively, these clinical findings support the involvement of lung mast cells in central features of severe asthma.
Several promising mast cell-targeted biologics, such as mAbs anti-IL-33 [200] (NTC04570657), anti-ST2 [202], anti-Siglec-8 (NCT03379311; NCT03436797; NCT04322708), and CDX-0159 (NCT04146129) have entered clinical development in asthma or allergic disorders. Moreover, several classes of drugs silencing or depleting mast cells (e.g., TKIs) have shown promising results in patients with severe uncontrolled asthma [262,263,264].
We are going through an exciting and promising era for understanding human mast cell biology. However, we must consider that many aspects of mast cell biology and their complex phenotypic and functional heterogeneity remain largely unknown. Mast cells are exposed to their local environment that, over time, can modify their phenotype and biochemical machinery [277]. More studies using novel techniques (e.g., single-cell mRNA seq, CyTOF) will more accurately reveal mast cell heterogeneity [278,279]. These techniques will contribute to identifying the role of mast cell subtypes in different asthma phenotypes. Another level of complexity derives from the species differences in extrapolating findings from mouse mast cell models to human settings [19,43].
Human mast cells and basophils have some similarities (e.g., FcεRI) but also striking differences [43]. Basophils have been recently identified in the human lung [26,27,280], where they play a prominent role in macrophage differentiation [281]. Macrophages represent the most prominent immune cells in human lung tissue [282,283]. There is also evidence that basophils and their mediators (i.e., IL-4, IL-13) play a role in Th2 and M2 polarization in allergic asthma [43]. Likely, some biologics that primarily target mast cells (e.g., omalizumab, mepolizumab, benralizumab) may also target human basophils [284,285].
Mast cells and their mediators play homeostatic and protective roles in several pathophysiological conditions [19,286]. Moreover, several normal cell types, such as germ cells, hematopoietic stem cells, and melanoblasts, express KIT, and the chronic administration of TKIs and mAbs targeting KIT may be associated with long-term adverse effects. Caution will be necessary in the future when drugs able to markedly reduce tissue mast cells in humans will be available for the treatment of mast cell-driven diseases.
Author Contributions
Conceptualization, R.P. and G.V.; resources, G.M. and G.V.; writing—original draft preparation, R.P., G.M. and G.V.; writing—review and editing, R.P., G.C., G.M., C.E.B. and G.V.; funding acquisition, G.M. and G.V. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported in part by grants from the CISI-Lab Project (University of Naples Federico II), TIMING Project and Campania Bioscience (Regione Campania).
Acknowledgments
The authors apologize to the many researchers who have contributed importantly to this field and whose work was not cited due to space and citation limitations. The authors thank the administrative staff (Roberto Bifulco, Anna Ferraro, and Maria Cristina Fucci) and the medical graphic artist Fabrizio Fiorbianco for the elaboration of figures.
Conflicts of Interest
G.M. has served on the advisory board for AstraZeneca (AZ). C.E.B. declares no direct conflict of interest in relation to this manuscript and indirect conflicts grants and consultancy paid to his institution from AZ, GSK, Sanofi, Regeneron, Roche, Genentech, Novartis, Chiesi, Mologic, 4DPharma. G.V. reports research support from A.Z. None of these affiliations represent a conflict of interest with respect to the design or execution of this review or interpretation of data presented in this manuscript.
Abbreviations
AHR: airway hyperresponsiveness; ANGPT, angiopoietin; BAL, bronchoalveolar lavage; BTK, Bruton’s tyrosine kinase; C5aR, C5a receptor; CADM1, cell adhesion molecule 1; CRH, corticotropin-release hormone; CSU, chronic spontaneous urticaria; CysLTR1, cysteinyl leukotriene receptor 1; CyTOF, Cytometry by time-of-flight; DARPin, designed ankyrin repeat protein; DC, dendritic cell; FDA, Food and Drug Administration; EMA, European Medicines Agency; FeNO, fractional exhaled nitric oxide; FLAP, 5-Lipoxygenase activating protein; HLMC, human lung mast cell; HSMC, human skin mast cell; JAK, Janus kinase; LTC4, cysteinyl leukotriene C4; mAb, monoclonal antibody; HMC, human mast cell; MCT, tryptase+ mast cell; MCTC, tryptase+, chymase+ mast cell; MMP, matrix metalloprotease; MRGPRX2, Mas-related G protein-coupled receptor X2; PAF, platelet-activating factor; PAR2, protease activated receptor 2; PGD2, prostaglandin D2; RCT, randomized control trial; SCF, stem cell factor; SYK, spleen tyrosine kinase; TKI, tyrosine kinase inhibitors; TLR, toll-like receptor; TSLP, thymic stromal lymphopoietin; TSLPR, thymic stromal lymphopoietin receptor; VEGF, vascular endothelial growth factor; VEGFR, vascular endothelial growth factor receptor.
References
- Ehrlich, P. Beitrage sur Theorie und Praxis der Histologischen Farbung. Ph.D. Thesis, University of Leipzig, Leipzig, Germany, 1878. [Google Scholar]
- Bradding, P.; Arthur, G. Mast cells in asthma—State of the art. Clin. Exp. Allergy 2016, 46, 194–263. [Google Scholar] [CrossRef]
- Galli, S.J.; Kalesnikoff, J.; Grimbaldeston, M.A.; Piliponsky, A.M.; Williams, C.M.; Tsai, M. Mast cells as “tunable” effector and immunoregulatory cells: Recent advances. Annu. Rev. Immunol. 2005, 23, 749–786. [Google Scholar] [CrossRef]
- Rivellese, F.; Nerviani, A.; Rossi, F.W.; Marone, G.; Matucci-Cerinic, M.; de Paulis, A.; Pitzalis, C. Mast cells in rheumatoid arthritis: Friends or foes? Autoimmun. Rev. 2017, 16, 557–563. [Google Scholar] [CrossRef]
- Piliponsky, A.M.; Chen, C.C.; Grimbaldeston, M.A.; Burns-Guydish, S.M.; Hardy, J.; Kalesnikoff, J.; Contag, C.H.; Tsai, M.; Galli, S.J. Mast cell-derived TNF can exacerbate mortality during severe bacterial infections in C57BL/6-KitW-sh/W-sh mice. Am. J. Pathol. 2010, 176, 926–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, G.P.; Bot, I.; Kovanen, P.T. Mast cells in human and experimental cardiometabolic diseases. Nat. Rev. Cardiol. 2015, 12, 643–658. [Google Scholar] [CrossRef]
- Varricchi, G.; Marone, G.; Kovanen, P.T. Cardiac Mast Cells: Underappreciated Immune Cells in Cardiovascular Homeostasis and Disease. Trends Immunol. 2020, 41, 734–746. [Google Scholar] [CrossRef]
- Marone, G.; Varricchi, G.; Loffredo, S.; Galdiero, M.R.; Rivellese, F.; de Paulis, A. Are Basophils and Mast Cells Masters in HIV Infection? Int. Arch. Allergy Immunol. 2016, 171, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Varricchi, G.; Galdiero, M.R.; Loffredo, S.; Marone, G.; Iannone, R.; Marone, G.; Granata, F. Are Mast Cells MASTers in Cancer? Front. Immunol. 2017, 8, 424. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.; Li, Z.; Gao, R.; Xing, B.; Gao, Y.; Yang, Y.; Qin, S.; Zhang, L.; Ouyang, H.; Du, P.; et al. A pan-cancer single-cell transcriptional atlas of tumor infiltrating myeloid cells. Cell 2021, 184, 792–809.e23. [Google Scholar] [CrossRef] [PubMed]
- Varricchi, G.; Galdiero, M.R.; Marone, G.; Granata, F.; Borriello, F.; Marone, G. Controversial role of mast cells in skin cancers. Exp. Dermatol. 2017, 26, 11–17. [Google Scholar] [CrossRef]
- Dahlin, J.S.; Ekoff, M.; Grootens, J.; Lof, L.; Amini, R.M.; Hagberg, H.; Ungerstedt, J.S.; Olsson-Stromberg, U.; Nilsson, G. KIT signaling is dispensable for human mast cell progenitor development. Blood 2017, 130, 1785–1794. [Google Scholar] [CrossRef] [Green Version]
- Marone, G.; Borriello, F.; Varricchi, G.; Genovese, A.; Granata, F. Basophils: Historical reflections and perspectives. Chem. Immunol. Allergy 2014, 100, 172–192. [Google Scholar] [PubMed]
- Chhiba, K.D.; Hsu, C.L.; Berdnikovs, S.; Bryce, P.J. Transcriptional Heterogeneity of Mast Cells and Basophils upon Activation. J. Immunol. 2017, 198, 4868–4878. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, T.; Katayama, I.; Nishioka, K. Expression of stem cell factor in basal cell carcinoma. Br. J. Dermatol. 1997, 137, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.; Valent, P.; Galli, S.J. KIT as a master regulator of the mast cell lineage. J. Allergy Clin. Immunol. 2022, 149, 1845–1854. [Google Scholar] [CrossRef]
- Welle, M. Development, significance, and heterogeneity of mast cells with particular regard to the mast cell-specific proteases chymase and tryptase. J. Leukoc. Biol. 1997, 61, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Irani, A.M.; Schwartz, L.B. Human mast cell heterogeneity. Allergy Proc. 1994, 15, 303–308. [Google Scholar] [CrossRef]
- Varricchi, G.; de Paulis, A.; Marone, G.; Galli, S.J. Future Needs in Mast Cell Biology. Int. J. Mol. Sci. 2019, 20, 4397. [Google Scholar] [CrossRef] [Green Version]
- Derakhshan, T.; Samuchiwal, S.K.; Hallen, N.; Bankova, L.G.; Boyce, J.A.; Barrett, N.A.; Austen, K.F.; Dwyer, D.F. Lineage-specific regulation of inducible and constitutive mast cells in allergic airway inflammation. J. Exp. Med. 2021, 218, e20200321. [Google Scholar] [CrossRef]
- Dwyer, D.F.; Ordovas-Montanes, J.; Allon, S.J.; Buchheit, K.M.; Vukovic, M.; Derakhshan, T.; Feng, C.; Lai, J.; Hughes, T.K.; Nyquist, S.K.; et al. Human airway mast cells proliferate and acquire distinct inflammation-driven phenotypes during type 2 inflammation. Sci. Immunol. 2021, 6, eabb7221. [Google Scholar] [CrossRef]
- Dwyer, D.F.; Barrett, N.A.; Austen, K.F. Expression profiling of constitutive mast cells reveals a unique identity within the immune system. Nat. Immunol. 2016, 17, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Kurotaki, D.; Osato, N.; Sato, H.; Sasaki, I.; Koizumi, S.; Wang, H.; Kaneda, C.; Nishiyama, A.; Kaisho, T.; et al. Transcription factor IRF8 plays a critical role in the development of murine basophils and mast cells. Blood 2015, 125, 358–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motakis, E.; Guhl, S.; Ishizu, Y.; Itoh, M.; Kawaji, H.; de Hoon, M.; Lassmann, T.; Carninci, P.; Hayashizaki, Y.; Zuberbier, T.; et al. Redefinition of the human mast cell transcriptome by deep-CAGE sequencing. Blood 2014, 123, e58–e67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plum, T.; Wang, X.; Rettel, M.; Krijgsveld, J.; Feyerabend, T.B.; Rodewald, H.R. Human Mast Cell Proteome Reveals Unique Lineage, Putative Functions, and Structural Basis for Cell Ablation. Immunity 2020, 52, 404–416.e5. [Google Scholar] [CrossRef] [PubMed]
- Reyfman, P.A.; Walter, J.M.; Joshi, N.; Anekalla, K.R.; McQuattie-Pimentel, A.C.; Chiu, S.; Fernandez, R.; Akbarpour, M.; Chen, C.I.; Ren, Z.; et al. Single-Cell Transcriptomic Analysis of Human Lung Provides Insights into the Pathobiology of Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2019, 199, 1517–1536. [Google Scholar] [CrossRef]
- Zilionis, R.; Engblom, C.; Pfirschke, C.; Savova, V.; Zemmour, D.; Saatcioglu, H.D.; Krishnan, I.; Maroni, G.; Meyerovitz, C.V.; Kerwin, C.M.; et al. Single-Cell Transcriptomics of Human and Mouse Lung Cancers Reveals Conserved Myeloid Populations across Individuals and Species. Immunity 2019, 50, 1317–1334.e10. [Google Scholar] [CrossRef]
- Cildir, G.; Toubia, J.; Yip, K.H.; Zhou, M.; Pant, H.; Hissaria, P.; Zhang, J.; Hong, W.; Robinson, N.; Grimbaldeston, M.A.; et al. Genome-wide Analyses of Chromatin State in Human Mast Cells Reveal Molecular Drivers and Mediators of Allergic and Inflammatory Diseases. Immunity 2019, 51, 949–965.e6. [Google Scholar] [CrossRef]
- Andersson, C.K.; Mori, M.; Bjermer, L.; Lofdahl, C.G.; Erjefalt, J.S. Novel site-specific mast cell subpopulations in the human lung. Thorax. 2009, 64, 297–305. [Google Scholar] [CrossRef] [Green Version]
- Galdiero, M.R.; Varricchi, G.; Seaf, M.; Marone, G.; Levi-Schaffer, F.; Marone, G. Bidirectional Mast Cell-Eosinophil Interactions in Inflammatory Disorders and Cancer. Front. Med. 2017, 4, 103. [Google Scholar] [CrossRef] [Green Version]
- Poto, R.; Quinti, I.; Marone, G.; Taglialatela, M.; de Paulis, A.; Casolaro, V.; Varricchi, G. IgG Autoantibodies Against IgE from Atopic Dermatitis Can Induce the Release of Cytokines and Proinflammatory Mediators from Basophils and Mast Cells. Front. Immunol. 2022, 13, 880412. [Google Scholar] [CrossRef]
- Genovese, A.; Borgia, G.; Bjorck, L.; Petraroli, A.; de Paulis, A.; Piazza, M.; Marone, G. Immunoglobulin superantigen protein L induces IL-4 and IL-13 secretion from human Fc epsilon RI+ cells through interaction with the kappa light chains of IgE. J. Immunol. 2003, 170, 1854–1861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florio, G.; Petraroli, A.; Patella, V.; Triggiani, M.; Marone, G. The immunoglobulin superantigen-binding site of HIV-1 gp120 activates human basophils. AIDS 2000, 14, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Leist, M.; Sunder, C.A.; Drube, S.; Zimmermann, C.; Geldmacher, A.; Metz, M.; Dudeck, A.; Maurer, M. Membrane-bound stem cell factor is the major but not only driver of fibroblast-induced murine skin mast cell differentiation. Exp. Dermatol. 2017, 26, 255–262. [Google Scholar] [CrossRef]
- Da Silva, C.A.; Reber, L.; Frossard, N. Stem cell factor expression, mast cells and inflammation in asthma. Fundam. Clin. Pharmacol. 2006, 20, 21–39. [Google Scholar] [CrossRef]
- Patella, V.; Marino, I.; Arbustini, E.; Lamparter-Schummert, B.; Verga, L.; Adt, M.; Marone, G. Stem cell factor in mast cells and increased mast cell density in idiopathic and ischemic cardiomyopathy. Circulation 1998, 97, 971–978. [Google Scholar] [CrossRef] [Green Version]
- de Paulis, A.; Minopoli, G.; Arbustini, E.; de Crescenzo, G.; Dal Piaz, F.; Pucci, P.; Russo, T.; Marone, G. Stem cell factor is localized in, released from, and cleaved by human mast cells. J. Immunol. 1999, 163, 2799–2808. [Google Scholar] [PubMed]
- Semlali, A.; Jacques, E.; Koussih, L.; Gounni, A.S.; Chakir, J. Thymic stromal lymphopoietin-induced human asthmatic airway epithelial cell proliferation through an IL-13-dependent pathway. J. Allergy Clin. Immunol. 2010, 125, 844–850. [Google Scholar] [CrossRef]
- Leichner, T.M.; Satake, A.; Harrison, V.S.; Tanaka, Y.; Archambault, A.S.; Kim, B.S.; Siracusa, M.C.; Leonard, W.J.; Naji, A.; Wu, G.F.; et al. Skin-derived TSLP systemically expands regulatory T cells. J. Autoimmun. 2017, 79, 39–52. [Google Scholar] [CrossRef] [Green Version]
- Varricchi, G.; Pecoraro, A.; Marone, G.; Criscuolo, G.; Spadaro, G.; Genovese, A.; Marone, G. Thymic Stromal Lymphopoietin Isoforms, Inflammatory Disorders, and Cancer. Front. Immunol. 2018, 9, 1595. [Google Scholar] [CrossRef] [Green Version]
- Siracusa, M.C.; Saenz, S.A.; Hill, D.A.; Kim, B.S.; Headley, M.B.; Doering, T.A.; Wherry, E.J.; Jessup, H.K.; Siegel, L.A.; Kambayashi, T.; et al. TSLP promotes interleukin-3-independent basophil haematopoiesis and type 2 inflammation. Nature 2011, 477, 229–233. [Google Scholar] [CrossRef]
- Allakhverdi, Z.; Comeau, M.R.; Jessup, H.K.; Yoon, B.R.; Brewer, A.; Chartier, S.; Paquette, N.; Ziegler, S.F.; Sarfati, M.; Delespesse, G. Thymic stromal lymphopoietin is released by human epithelial cells in response to microbes, trauma, or inflammation and potently activates mast cells. J. Exp. Med. 2007, 204, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Gambardella, A.R.; Poto, R.; Tirelli, V.; Schroeder, J.T.; Marone, G.; Mattei, F.; Varricchi, G.; Schiavoni, G. Differential Effects of Alarmins on Human and Mouse Basophils. Front. Immunol. 2022, 13, 894163. [Google Scholar] [CrossRef] [PubMed]
- Shikotra, A.; Ohri, C.M.; Green, R.H.; Waller, D.A.; Bradding, P. Mast cell phenotype, TNFalpha expression and degranulation status in non-small cell lung cancer. Sci. Rep. 2016, 6, 38352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, D.; Doe, C.; Woodman, L.; Heidi Wan, W.Y.; Sutcliffe, A.; Hollins, F.; Brightling, C. Mast cell-airway smooth muscle crosstalk: The role of thymic stromal lymphopoietin. Chest 2012, 142, 76–85. [Google Scholar] [CrossRef] [Green Version]
- Afferni, C.; Buccione, C.; Andreone, S.; Galdiero, M.R.; Varricchi, G.; Marone, G.; Mattei, F.; Schiavoni, G. The Pleiotropic Immunomodulatory Functions of IL-33 and Its Implications in Tumor Immunity. Front. Immunol. 2018, 9, 2601. [Google Scholar] [CrossRef] [Green Version]
- Cayrol, C.; Girard, J.P. Interleukin-33 (IL-33): A nuclear cytokine from the IL-1 family. Immunol. Rev. 2018, 281, 154–168. [Google Scholar] [CrossRef]
- Hsu, C.L.; Neilsen, C.V.; Bryce, P.J. IL-33 is produced by mast cells and regulates IgE-dependent inflammation. PLoS ONE 2010, 5, e11944. [Google Scholar] [CrossRef] [Green Version]
- Russi, A.E.; Ebel, M.E.; Yang, Y.; Brown, M.A. Male-specific IL-33 expression regulates sex-dimorphic EAE susceptibility. Proc. Natl. Acad. Sci. USA 2018, 115, E1520–E1529. [Google Scholar] [CrossRef] [Green Version]
- Iikura, M.; Suto, H.; Kajiwara, N.; Oboki, K.; Ohno, T.; Okayama, Y.; Saito, H.; Galli, S.J.; Nakae, S. IL-33 can promote survival, adhesion and cytokine production in human mast cells. Lab. Invest. 2007, 87, 971–978. [Google Scholar] [CrossRef] [Green Version]
- Bandara, G.; Beaven, M.A.; Olivera, A.; Gilfillan, A.M.; Metcalfe, D.D. Activated mast cells synthesize and release soluble ST2-a decoy receptor for IL-33. Eur. J. Immunol. 2015, 45, 3034–3044. [Google Scholar] [CrossRef]
- Kaur, D.; Gomez, E.; Doe, C.; Berair, R.; Woodman, L.; Saunders, R.; Hollins, F.; Rose, F.R.; Amrani, Y.; May, R.; et al. IL-33 drives airway hyper-responsiveness through IL-13-mediated mast cell: Airway smooth muscle crosstalk. Allergy 2015, 70, 556–567. [Google Scholar] [CrossRef] [Green Version]
- Silver, M.R.; Margulis, A.; Wood, N.; Goldman, S.J.; Kasaian, M.; Chaudhary, D. IL-33 synergizes with IgE-dependent and IgE-independent agents to promote mast cell and basophil activation. Inflamm. Res. 2010, 59, 207–218. [Google Scholar] [CrossRef]
- Joulia, R.; L’Faqihi, F.E.; Valitutti, S.; Espinosa, E. IL-33 fine tunes mast cell degranulation and chemokine production at the single-cell level. J. Allergy Clin. Immunol. 2017, 140, 497–509.e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taracanova, A.; Alevizos, M.; Karagkouni, A.; Weng, Z.; Norwitz, E.; Conti, P.; Leeman, S.E.; Theoharides, T.C. SP and IL-33 together markedly enhance TNF synthesis and secretion from human mast cells mediated by the interaction of their receptors. Proc. Natl. Acad. Sci. USA 2017, 114, E4002–E4009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theoharides, T.C.; Zhang, B.; Kempuraj, D.; Tagen, M.; Vasiadi, M.; Angelidou, A.; Alysandratos, K.D.; Kalogeromitros, D.; Asadi, S.; Stavrianeas, N.; et al. IL-33 augments substance P-induced VEGF secretion from human mast cells and is increased in psoriatic skin. Proc. Natl. Acad. Sci. USA 2010, 107, 4448–4453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivellese, F.; Suurmond, J.; Habets, K.; Dorjee, A.L.; Ramamoorthi, N.; Townsend, M.J.; de Paulis, A.; Marone, G.; Huizinga, T.W.; Pitzalis, C.; et al. Ability of Interleukin-33- and Immune Complex-Triggered Activation of Human Mast Cells to Down-Regulate Monocyte-Mediated Immune Responses. Arthritis Rheumatol. 2015, 67, 2343–2353. [Google Scholar] [CrossRef]
- Cristinziano, L.; Poto, R.; Criscuolo, G.; Ferrara, A.L.; Galdiero, M.R.; Modestino, L.; Loffredo, S.; de Paulis, A.; Marone, G.; Spadaro, G.; et al. IL-33 and Superantigenic Activation of Human Lung Mast Cells Induce the Release of Angiogenic and Lymphangiogenic Factors. Cells 2021, 10, 145. [Google Scholar] [CrossRef]
- Igawa, S.; Di Nardo, A. Skin microbiome and mast cells. Transl. Res. 2017, 184, 68–76. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Yu, Y.Y.; Zhang, Y.R.; Zhang, W.; Yu, B. The modulatory effect of TLR2 on LL-37-induced human mast cells activation. Biochem. Biophys. Res. Commun. 2016, 470, 368–374. [Google Scholar] [CrossRef]
- Kulka, M.; Alexopoulou, L.; Flavell, R.A.; Metcalfe, D.D. Activation of mast cells by double-stranded RNA: Evidence for activation through Toll-like receptor 3. J. Allergy. Clin. Immunol. 2004, 114, 174–182. [Google Scholar] [CrossRef]
- Suurmond, J.; Rivellese, F.; Dorjee, A.L.; Bakker, A.M.; Rombouts, Y.J.; Rispens, T.; Wolbink, G.; Zaldumbide, A.; Hoeben, R.C.; Huizinga, T.W.; et al. Toll-like receptor triggering augments activation of human mast cells by anti-citrullinated protein antibodies. Ann. Rheum. Dis. 2015, 74, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Suurmond, J.; Dorjee, A.L.; Knol, E.F.; Huizinga, T.W.; Toes, R.E. Differential TLR-induced cytokine production by human mast cells is amplified by FcvarepsilonRI triggering. Clin. Exp. Allergy 2015, 45, 788–796. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, J.T. Basophils: Emerging roles in the pathogenesis of allergic disease. Immunol. Rev. 2011, 242, 144–160. [Google Scholar] [CrossRef] [PubMed]
- Patella, V.; Marino, I.; Lamparter, B.; Arbustini, E.; Adt, M.; Marone, G. Human heart mast cells. Isolation, purification, ultrastructure, and immunologic characterization. J. Immunol. 1995, 154, 2855–2865. [Google Scholar] [PubMed]
- Hofstra, C.L.; Desai, P.J.; Thurmond, R.L.; Fung-Leung, W.P. Histamine H4 receptor mediates chemotaxis and calcium mobilization of mast cells. J. Pharmacol. Exp. Ther. 2003, 305, 1212–1221. [Google Scholar] [CrossRef] [Green Version]
- Triggiani, M.; Gentile, M.; Secondo, A.; Granata, F.; Oriente, A.; Taglialatela, M.; Annunziato, L.; Marone, G. Histamine induces exocytosis and IL-6 production from human lung macrophages through interaction with H1 receptors. J. Immunol. 2001, 166, 4083–4091. [Google Scholar] [CrossRef] [Green Version]
- Levi-Schaffer, F.; Eliashar, R. Mast cell stabilizing properties of antihistamines. J. Invest. Dermatol. 2009, 129, 2549–2551. [Google Scholar] [CrossRef] [Green Version]
- Genovese, A.; Patella, V.; De Crescenzo, G.; De Paulis, A.; Spadaro, G.; Marone, G. Loratadine and desethoxylcarbonyl-loratadine inhibit the immunological release of mediators from human Fc epsilon RI+ cells. Clin. Exp. Allergy 1997, 27, 559–567. [Google Scholar] [CrossRef]
- Malbec, O.; Cassard, L.; Albanesi, M.; Jonsson, F.; Mancardi, D.; Chicanne, G.; Payrastre, B.; Dubreuil, P.; Vivier, E.; Daeron, M. Trans-inhibition of activation and proliferation signals by Fc receptors in mast cells and basophils. Sci. Signal 2016, 9, ra126. [Google Scholar] [CrossRef]
- Levi-Schaffer, F.; Gibbs, B.F.; Hallgren, J.; Pucillo, C.; Redegeld, F.; Siebenhaar, F.; Vitte, J.; Mezouar, S.; Michel, M.; Puzzovio, P.G.; et al. Selected recent advances in understanding the role of human mast cells in health and disease. J. Allergy Clin. Immunol. 2022, 149, 1833–1844. [Google Scholar] [CrossRef]
- Gibbs, B.F.; Sabato, V.; Bridts, C.H.; Ebo, D.G.; Ben-Zimra, M.; Levi-Schaffer, F. Expressions and inhibitory functions of CD300a receptors on purified human basophils. Exp. Dermatol. 2012, 21, 884–886. [Google Scholar] [CrossRef]
- Sabato, V.; Verweij, M.M.; Bridts, C.H.; Levi-Schaffer, F.; Gibbs, B.F.; De Clerck, L.S.; Schiavino, D.; Ebo, D.G. CD300a is expressed on human basophils and seems to inhibit IgE/FcepsilonRI-dependent anaphylactic degranulation. Cytom. B Clin. Cytom. 2012, 82, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Bachelet, I.; Munitz, A.; Moretta, A.; Moretta, L.; Levi-Schaffer, F. The inhibitory receptor IRp60 (CD300a) is expressed and functional on human mast cells. J. Immunol. 2005, 175, 7989–7995. [Google Scholar] [CrossRef] [Green Version]
- Bachelet, I.; Munitz, A.; Levi-Schaffer, F. Abrogation of allergic reactions by a bispecific antibody fragment linking IgE to CD300a. J. Allergy Clin. Immunol. 2006, 117, 1314–1320. [Google Scholar] [CrossRef]
- Robida, P.A.; Rische, C.H.; Morgenstern, N.B.; Janarthanam, R.; Cao, Y.; Krier-Burris, R.A.; Korver, W.; Xu, A.; Luu, T.; Schanin, J.; et al. Functional and Phenotypic Characterization of Siglec-6 on Human Mast Cells. Cells 2022, 11, 1138. [Google Scholar] [CrossRef] [PubMed]
- Hudson, S.A.; Herrmann, H.; Du, J.; Cox, P.; Haddadel, B.; Butler, B.; Crocker, P.R.; Ackerman, S.J.; Valent, P.; Bochner, B.S. Developmental, malignancy-related, and cross-species analysis of eosinophil, mast cell, and basophil siglec-8 expression. J. Clin. Immunol. 2011, 31, 1045–1053. [Google Scholar] [CrossRef] [Green Version]
- Mizrahi, S.; Gibbs, B.F.; Karra, L.; Ben-Zimra, M.; Levi-Schaffer, F. Siglec-7 is an inhibitory receptor on human mast cells and basophils. J. Allergy Clin. Immunol. 2014, 134, 230–233. [Google Scholar] [CrossRef]
- Yokoi, H.; Myers, A.; Matsumoto, K.; Crocker, P.R.; Saito, H.; Bochner, B.S. Alteration and acquisition of Siglecs during in vitro maturation of CD34+ progenitors into human mast cells. Allergy 2006, 61, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Korver, W.; Wong, A.; Gebremeskel, S.; Negri, G.L.; Schanin, J.; Chang, K.; Leung, J.; Benet, Z.; Luu, T.; Brock, E.C.; et al. The Inhibitory Receptor Siglec-8 Interacts With FcepsilonRI and Globally Inhibits Intracellular Signaling in Primary Mast Cells Upon Activation. Front. Immunol. 2022, 13, 833728. [Google Scholar] [CrossRef] [PubMed]
- Kikly, K.K.; Bochner, B.S.; Freeman, S.D.; Tan, K.B.; Gallagher, K.T.; D’Alessio, K.J.; Holmes, S.D.; Abrahamson, J.A.; Erickson-Miller, C.L.; Murdock, P.R.; et al. Identification of SAF-2, a novel siglec expressed on eosinophils, mast cells, and basophils. J. Allergy Clin. Immunol. 2000, 105, 1093–1100. [Google Scholar] [CrossRef]
- Kiwamoto, T.; Kawasaki, N.; Paulson, J.C.; Bochner, B.S. Siglec-8 as a drugable target to treat eosinophil and mast cell-associated conditions. Pharmacol. Ther 2012, 135, 327–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okayama, Y.; Kirshenbaum, A.S.; Metcalfe, D.D. Expression of a functional high-affinity IgG receptor, Fc gamma RI, on human mast cells: Up-regulation by IFN-gamma. J. Immunol. 2000, 164, 4332–4339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, D.; Kepley, C.L.; Zhang, M.; Zhang, K.; Saxon, A. A novel human immunoglobulin Fc gamma Fc epsilon bifunctional fusion protein inhibits Fc epsilon RI-mediated degranulation. Nat. Med. 2002, 8, 518–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, D.; Kepley, C.L.; Zhang, K.; Terada, T.; Yamada, T.; Saxon, A. A chimeric human-cat fusion protein blocks cat-induced allergy. Nat. Med. 2005, 11, 446–449. [Google Scholar] [CrossRef]
- Zhang, K.; Kepley, C.L.; Terada, T.; Zhu, D.; Perez, H.; Saxon, A. Inhibition of allergen-specific IgE reactivity by a human Ig Fcgamma-Fcepsilon bifunctional fusion protein. J. Allergy Clin. Immunol. 2004, 114, 321–327. [Google Scholar] [CrossRef]
- Cemerski, S.; Chu, S.Y.; Moore, G.L.; Muchhal, U.S.; Desjarlais, J.R.; Szymkowski, D.E. Suppression of mast cell degranulation through a dual-targeting tandem IgE-IgG Fc domain biologic engineered to bind with high affinity to FcgammaRIIb. Immunol. Lett. 2012, 143, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Varricchi, G.; Raap, U.; Rivellese, F.; Marone, G.; Gibbs, B.F. Human mast cells and basophils-How are they similar how are they different? Immunol. Rev. 2018, 282, 8–34. [Google Scholar] [CrossRef]
- Harvima, I.T.; Nilsson, G. Mast cells as regulators of skin inflammation and immunity. Acta Derm. Venereol. 2011, 91, 644–650. [Google Scholar] [CrossRef] [Green Version]
- Brightling, C.E.; Bradding, P.; Symon, F.A.; Holgate, S.T.; Wardlaw, A.J.; Pavord, I.D. Mast-cell infiltration of airway smooth muscle in asthma. N. Engl. J. Med. 2002, 346, 1699–1705. [Google Scholar] [CrossRef]
- Kaur, D.; Saunders, R.; Hollins, F.; Woodman, L.; Doe, C.; Siddiqui, S.; Bradding, P.; Brightling, C. Mast cell fibroblastoid differentiation mediated by airway smooth muscle in asthma. J. Immunol. 2010, 185, 6105–6114. [Google Scholar] [CrossRef]
- Maun, H.R.; Jackman, J.K.; Choy, D.F.; Loyet, K.M.; Staton, T.L.; Jia, G.; Dressen, A.; Hackney, J.A.; Bremer, M.; Walters, B.T.; et al. An Allosteric Anti-tryptase Antibody for the Treatment of Mast Cell-Mediated Severe Asthma. Cell 2019, 179, 417–431.e19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caughey, G.H. Mast cell proteases as pharmacological targets. Eur. J. Pharmacol. 2016, 778, 44–55. [Google Scholar] [CrossRef] [Green Version]
- Huttunen, M.; Harvima, I.T. Mast cell tryptase and chymase in chronic leg ulcers: Chymase is potentially destructive to epithelium and is controlled by proteinase inhibitors. Br. J. Dermatol. 2005, 152, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Irani, A.M.; Goldstein, S.M.; Wintroub, B.U.; Bradford, T.; Schwartz, L.B. Human mast cell carboxypeptidase. Selective localization to MCTC cells. J. Immunol. 1991, 147, 247–253. [Google Scholar]
- Strik, M.C.; de Koning, P.J.; Kleijmeer, M.J.; Bladergroen, B.A.; Wolbink, A.M.; Griffith, J.M.; Wouters, D.; Fukuoka, Y.; Schwartz, L.B.; Hack, C.E.; et al. Human mast cells produce and release the cytotoxic lymphocyte associated protease granzyme B upon activation. Mol. Immunol. 2007, 44, 3462–3472. [Google Scholar] [CrossRef] [PubMed]
- Di Girolamo, N.; Indoh, I.; Jackson, N.; Wakefield, D.; McNeil, H.P.; Yan, W.; Geczy, C.; Arm, J.P.; Tedla, N. Human mast cell-derived gelatinase B (matrix metalloproteinase-9) is regulated by inflammatory cytokines: Role in cell migration. J. Immunol. 2006, 177, 2638–2650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacGlashan, D.W.; Peters, S.P., Jr.; Warner, J.; Lichtenstein, L.M. Characteristics of human basophil sulfidopeptide leukotriene release: Releasability defined as the ability of the basophil to respond to dimeric cross-links. J. Immunol. 1986, 136, 2231–2239. [Google Scholar]
- Austen, K.F. The cysteinyl leukotrienes: Where do they come from? What are they? Where are they going? Nat. Immunol. 2008, 9, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Dahlen, S.E.; Kumlin, M. Monitoring mast cell activation by prostaglandin D2 in vivo. Thorax 2004, 59, 453–455. [Google Scholar] [CrossRef] [Green Version]
- Schuligoi, R.; Sturm, E.; Luschnig, P.; Konya, V.; Philipose, S.; Sedej, M.; Waldhoer, M.; Peskar, B.A.; Heinemann, A. CRTH2 and D-type prostanoid receptor antagonists as novel therapeutic agents for inflammatory diseases. Pharmacology 2010, 85, 372–382. [Google Scholar] [CrossRef]
- Triggiani, M.; Hubbard, W.C.; Chilton, F.H. Synthesis of 1-acyl-2-acetyl-sn-glycero-3-phosphocholine by an enriched preparation of the human lung mast cell. J. Immunol. 1990, 144, 4773–4780. [Google Scholar] [PubMed]
- Ohkawara, Y.; Yamauchi, K.; Tanno, Y.; Tamura, G.; Ohtani, H.; Nagura, H.; Ohkuda, K.; Takishima, T. Human lung mast cells and pulmonary macrophages produce tumor necrosis factor-alpha in sensitized lung tissue after IgE receptor triggering. Am. J. Respir. Cell Mol. Biol. 1992, 7, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Okayama, Y.; Hagaman, D.D.; Metcalfe, D.D. A comparison of mediators released or generated by IFN-gamma-treated human mast cells following aggregation of Fc gamma RI or Fc epsilon RI. J. Immunol. 2001, 166, 4705–4712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouri-Aria, K.T.; Pilette, C.; Jacobson, M.R.; Watanabe, H.; Durham, S.R. IL-9 and c-Kit+ mast cells in allergic rhinitis during seasonal allergen exposure: Effect of immunotherapy. J. Allergy Clin. Immunol. 2005, 116, 73–79. [Google Scholar] [CrossRef]
- Ishizuka, T.; Okayama, Y.; Kobayashi, H.; Mori, M. Interleukin-3 production by mast cells from human lung. Inflammation 1999, 23, 25–35. [Google Scholar] [CrossRef]
- Okayama, Y.; Petit-Frere, C.; Kassel, O.; Semper, A.; Quint, D.; Tunon-de-Lara, M.J.; Bradding, P.; Holgate, S.T.; Church, M.K. IgE-dependent expression of mRNA for IL-4 and IL-5 in human lung mast cells. J. Immunol. 1995, 155, 1796–1808. [Google Scholar]
- Suttle, M.M.; Nilsson, G.; Snellman, E.; Harvima, I.T. Experimentally induced psoriatic lesion associates with interleukin (IL)-6 in mast cells and appearance of dermal cells expressing IL-33 and IL-6 receptor. Clin. Exp. Immunol. 2012, 169, 311–319. [Google Scholar] [CrossRef]
- Lorentz, A.; Schwengberg, S.; Sellge, G.; Manns, M.P.; Bischoff, S.C. Human intestinal mast cells are capable of producing different cytokine profiles: Role of IgE receptor cross-linking and IL-4. J. Immunol. 2000, 164, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Burd, P.R.; Thompson, W.C.; Max, E.E.; Mills, F.C. Activated mast cells produce interleukin 13. J. Exp. Med. 1995, 181, 1373–1380. [Google Scholar] [CrossRef]
- Rumsaeng, V.; Cruikshank, W.W.; Foster, B.; Prussin, C.; Kirshenbaum, A.S.; Davis, T.A.; Kornfeld, H.; Center, D.M.; Metcalfe, D.D. Human mast cells produce the CD4+ T lymphocyte chemoattractant factor, IL-16. J. Immunol. 1997, 159, 2904–2910. [Google Scholar]
- Mashiko, S.; Bouguermouh, S.; Rubio, M.; Baba, N.; Bissonnette, R.; Sarfati, M. Human mast cells are major IL-22 producers in patients with psoriasis and atopic dermatitis. J. Allergy Clin. Immunol. 2015, 136, 351–359.e1. [Google Scholar] [CrossRef]
- Okayama, Y.; Okumura, S.; Sagara, H.; Yuki, K.; Sasaki, T.; Watanabe, N.; Fueki, M.; Sugiyama, K.; Takeda, K.; Fukuda, T.; et al. FcepsilonRI-mediated thymic stromal lymphopoietin production by interleukin-4-primed human mast cells. Eur. Respir. J. 2009, 34, 425–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ying, S.; O’Connor, B.; Ratoff, J.; Meng, Q.; Mallett, K.; Cousins, D.; Robinson, D.; Zhang, G.; Zhao, J.; Lee, T.H.; et al. Thymic stromal lymphopoietin expression is increased in asthmatic airways and correlates with expression of Th2-attracting chemokines and disease severity. J. Immunol. 2005, 174, 8183–8190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shikotra, A.; Choy, D.F.; Ohri, C.M.; Doran, E.; Butler, C.; Hargadon, B.; Shelley, M.; Abbas, A.R.; Austin, C.D.; Jackman, J.; et al. Increased expression of immunoreactive thymic stromal lymphopoietin in patients with severe asthma. J. Allergy Clin. Immunol. 2012, 129, 104–111.e1-9. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.W.; Kim, D.K.; Park, M.H.; Eun, K.M.; Lee, M.; So, D.; Kong, I.G.; Mo, J.H.; Yang, M.S.; Jin, H.R.; et al. IL-25 as a novel therapeutic target in nasal polyps of patients with chronic rhinosinusitis. J. Allergy Clin. Immunol. 2015, 135, 1476–1485.e7. [Google Scholar] [CrossRef] [Green Version]
- Detoraki, A.; Staiano, R.I.; Granata, F.; Giannattasio, G.; Prevete, N.; de Paulis, A.; Ribatti, D.; Genovese, A.; Triggiani, M.; Marone, G. Vascular endothelial growth factors synthesized by human lung mast cells exert angiogenic effects. J. Allergy Clin. Immunol. 2009, 123, 1142–1149.e1-5. [Google Scholar] [CrossRef]
- Dvorak, A.M.; Morgan, E.S.; Weller, P.F. Ultrastructural immunolocalization of basic fibroblast growth factor to lipid bodies and secretory granules in human mast cells. Histochem. J. 2001, 33, 397–402. [Google Scholar] [CrossRef]
- Nilsson, G.; Forsberg-Nilsson, K.; Xiang, Z.; Hallbook, F.; Nilsson, K.; Metcalfe, D.D. Human mast cells express functional TrkA and are a source of nerve growth factor. Eur. J. Immunol. 1997, 27, 2295–2301. [Google Scholar] [CrossRef]
- Okumura, S.; Sagara, H.; Fukuda, T.; Saito, H.; Okayama, Y. FcepsilonRI-mediated amphiregulin production by human mast cells increases mucin gene expression in epithelial cells. J. Allergy Clin. Immunol. 2005, 115, 272–279. [Google Scholar] [CrossRef]
- Wang, S.W.; Oh, C.K.; Cho, S.H.; Hu, G.; Martin, R.; Demissie-Sanders, S.; Li, K.; Moyle, M.; Yao, Z. Amphiregulin expression in human mast cells and its effect on the primary human lung fibroblasts. J. Allergy Clin. Immunol. 2005, 115, 287–294. [Google Scholar] [CrossRef]
- Yano, K.; Yamaguchi, M.; de Mora, F.; Lantz, C.S.; Butterfield, J.H.; Costa, J.J.; Galli, S.J. Production of macrophage inflammatory protein-1alpha by human mast cells: Increased anti-IgE-dependent secretion after IgE-dependent enhancement of mast cell IgE-binding ability. Lab. Invest. 1997, 77, 185–193. [Google Scholar] [PubMed]
- Melillo, R.M.; Guarino, V.; Avilla, E.; Galdiero, M.R.; Liotti, F.; Prevete, N.; Rossi, F.W.; Basolo, F.; Ugolini, C.; de Paulis, A.; et al. Mast cells have a protumorigenic role in human thyroid cancer. Oncogene 2010, 29, 6203–6215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visciano, C.; Liotti, F.; Prevete, N.; Cali, G.; Franco, R.; Collina, F.; de Paulis, A.; Marone, G.; Santoro, M.; Melillo, R.M. Mast cells induce epithelial-to-mesenchymal transition and stem cell features in human thyroid cancer cells through an IL-8-Akt-Slug pathway. Oncogene 2015, 34, 5175–5186. [Google Scholar] [CrossRef] [PubMed]
- Granata, F.; Frattini, A.; Loffredo, S.; Staiano, R.I.; Petraroli, A.; Ribatti, D.; Oslund, R.; Gelb, M.H.; Lambeau, G.; Marone, G.; et al. Production of vascular endothelial growth factors from human lung macrophages induced by group IIA and group X secreted phospholipases A2. J. Immunol. 2010, 184, 5232–5241. [Google Scholar] [CrossRef]
- de Paulis, A.; Prevete, N.; Fiorentino, I.; Rossi, F.W.; Staibano, S.; Montuori, N.; Ragno, P.; Longobardi, A.; Liccardo, B.; Genovese, A.; et al. Expression and functions of the vascular endothelial growth factors and their receptors in human basophils. J. Immunol. 2006, 177, 7322–7331. [Google Scholar] [CrossRef] [Green Version]
- Loffredo, S.; Borriello, F.; Iannone, R.; Ferrara, A.L.; Galdiero, M.R.; Gigantino, V.; Esposito, P.; Varricchi, G.; Lambeau, G.; Cassatella, M.A.; et al. Group V Secreted Phospholipase A2 Induces the Release of Proangiogenic and Antiangiogenic Factors by Human Neutrophils. Front. Immunol. 2017, 8, 443. [Google Scholar] [CrossRef] [Green Version]
- Poto, R.; Cristinziano, L.; Modestino, L.; de Paulis, A.; Marone, G.; Loffredo, S.; Galdiero, M.R.; Varricchi, G. Neutrophil Extracellular Traps, Angiogenesis and Cancer. Biomedicines 2022, 10, 431. [Google Scholar] [CrossRef]
- Thomas, M.; Augustin, H.G. The role of the Angiopoietins in vascular morphogenesis. Angiogenesis 2009, 12, 125–137. [Google Scholar] [CrossRef]
- Loffredo, S.; Bova, M.; Suffritti, C.; Borriello, F.; Zanichelli, A.; Petraroli, A.; Varricchi, G.; Triggiani, M.; Cicardi, M.; Marone, G. Elevated plasma levels of vascular permeability factors in C1 inhibitor-deficient hereditary angioedema. Allergy 2016, 71, 989–996. [Google Scholar] [CrossRef]
- Varricchi, G.; Loffredo, S.; Bencivenga, L.; Ferrara, A.L.; Gambino, G.; Ferrara, N.; de Paulis, A.; Marone, G.; Rengo, G. Angiopoietins, Vascular Endothelial Growth Factors and Secretory Phospholipase A2 in Ischemic and Non-Ischemic Heart Failure. J. Clin. Med. 2020, 9, 1928. [Google Scholar] [CrossRef]
- Varricchi, G.; Poto, R.; Ferrara, A.L.; Gambino, G.; Marone, G.; Rengo, G.; Loffredo, S.; Bencivenga, L. Angiopoietins, vascular endothelial growth factors and secretory phospholipase A2 in heart failure patients with preserved ejection fraction. Eur. J. Intern. Med. 2022, 22, S0953. [Google Scholar] [CrossRef] [PubMed]
- Duah, E.; Teegala, L.R.; Kondeti, V.; Adapala, R.K.; Keshamouni, V.G.; Kanaoka, Y.; Austen, K.F.; Thodeti, C.K.; Paruchuri, S. Cysteinyl leukotriene 2 receptor promotes endothelial permeability, tumor angiogenesis, and metastasis. Proc. Natl. Acad. Sci. USA 2019, 116, 199–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patella, V.; Florio, G.; Petraroli, A.; Marone, G. HIV-1 gp120 induces IL-4 and IL-13 release from human Fc epsilon RI+ cells through interaction with the VH3 region of IgE. J. Immunol. 2000, 164, 589–595. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Kaur, D.; Okayama, Y.; Ito, A.; Wardlaw, A.J.; Brightling, C.E.; Bradding, P. Human lung mast cells adhere to human airway smooth muscle, in part, via tumor suppressor in lung cancer-1. J. Immunol. 2006, 176, 1238–1243. [Google Scholar] [CrossRef]
- Hollins, F.; Kaur, D.; Yang, W.; Cruse, G.; Saunders, R.; Sutcliffe, A.; Berger, P.; Ito, A.; Brightling, C.E.; Bradding, P. Human airway smooth muscle promotes human lung mast cell survival, proliferation, and constitutive activation: Cooperative roles for CADM1, stem cell factor, and IL-6. J. Immunol. 2008, 181, 2772–2780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salomonsson, M.; Malinovschi, A.; Kalm-Stephens, P.; Dahlin, J.S.; Janson, C.; Alving, K.; Hallgren, J. Circulating mast cell progenitors correlate with reduced lung function in allergic asthma. Clin. Exp. Allergy 2019, 49, 874–882. [Google Scholar] [CrossRef] [Green Version]
- Schleimer, R.P.; MacGlashan, D.W.; Peters, S.P., Jr.; Pinckard, R.N.; Adkinson, N.F.; Lichtenstein, L.M., Jr. Characterization of inflammatory mediator release from purified human lung mast cells. Am. Rev. Respir. Dis. 1986, 133, 614–617. [Google Scholar]
- Murray, J.J.; Tonnel, A.B.; Brash, A.R.; Roberts, L.J.; Gosset, P., 2nd; Workman, R.; Capron, A.; Oates, J.A. Release of prostaglandin D2 into human airways during acute antigen challenge. N. Engl. J. Med. 1986, 315, 800–804. [Google Scholar] [CrossRef]
- Casale, T.B.; Wood, D.; Richerson, H.B.; Zehr, B.; Zavala, D.; Hunninghake, G.W. Direct evidence of a role for mast cells in the pathogenesis of antigen-induced bronchoconstriction. J. Clin. Invest. 1987, 80, 1507–1511. [Google Scholar] [CrossRef]
- Wenzel, S.E.; Fowler, A.A.; Schwartz, L.B., 3rd. Activation of pulmonary mast cells by bronchoalveolar allergen challenge. In vivo release of histamine and tryptase in atopic subjects with and without asthma. Am. Rev. Respir. Dis. 1988, 137, 1002–1008. [Google Scholar]
- Varricchi, G.; Ferri, S.; Pepys, J.; Poto, R.; Spadaro, G.; Nappi, E.; Paoletti, G.; Virchow, J.C.; Heffler, E.; Canonica, W.G. Biologics and airway remodeling in severe asthma. Allergy, 2022; early view. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, M.; Takahashi, M.; Aoike, N. Expression of vascular endothelial growth factor, basic fibroblast growth factor, and angiogenin immunoreactivity in asthmatic airways and its relationship to angiogenesis. J. Allergy. Clin. Immunol. 2001, 107, 295–301. [Google Scholar] [CrossRef]
- Chetta, A.; Zanini, A.; Foresi, A.; Del Donno, M.; Castagnaro, A.; D’Ippolito, R.; Baraldo, S.; Testi, R.; Saetta, M.; Olivieri, D. Vascular component of airway remodeling in asthma is reduced by high dose of fluticasone. Am. J. Respir. Crit. Care Med. 2003, 167, 751–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Detoraki, A.; Granata, F.; Staibano, S.; Rossi, F.W.; Marone, G.; Genovese, A. Angiogenesis and lymphangiogenesis in bronchial asthma. Allergy 2010, 65, 946–958. [Google Scholar] [CrossRef] [PubMed]
- Varricchi, G.; Loffredo, S.; Borriello, F.; Pecoraro, A.; Rivellese, F.; Genovese, A.; Spadaro, G.; Marone, G. Superantigenic Activation of Human Cardiac Mast Cells. Int. J. Mol. Sci. 2019, 20, 1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altman, M.C.; Lai, Y.; Nolin, J.D.; Long, S.; Chen, C.C.; Piliponsky, A.M.; Altemeier, W.A.; Larmore, M.; Frevert, C.W.; Mulligan, M.S.; et al. Airway epithelium-shifted mast cell infiltration regulates asthmatic inflammation via IL-33 signaling. J. Clin. Invest. 2019, 129, 4979–4991. [Google Scholar] [CrossRef]
- Theoharides, T.C.; Spanos, C.; Pang, X.; Alferes, L.; Ligris, K.; Letourneau, R.; Rozniecki, J.J.; Webster, E.; Chrousos, G.P. Stress-induced intracranial mast cell degranulation: A corticotropin-releasing hormone-mediated effect. Endocrinology 1995, 136, 5745–5750. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Cetrulo, C.L.; Theoharides, T.C. Corticotropin-releasing hormone induces vascular endothelial growth factor release from human mast cells via the cAMP/protein kinase A/p38 mitogen-activated protein kinase pathway. Mol. Pharmacol. 2006, 69, 998–1006. [Google Scholar] [CrossRef] [Green Version]
- Theoharides, T.C.; Enakuaa, S.; Sismanopoulos, N.; Asadi, S.; Papadimas, E.C.; Angelidou, A.; Alysandratos, K.D. Contribution of stress to asthma worsening through mast cell activation. Ann. Allergy Asthma Immunol. 2012, 109, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Varricchi, G.; Rossi, F.W.; Galdiero, M.R.; Granata, F.; Criscuolo, G.; Spadaro, G.; de Paulis, A.; Marone, G. Physiological Roles of Mast Cells: Collegium Internationale Allergologicum Update 2019. Int. Arch. Allergy Immunol. 2019, 179, 247–261. [Google Scholar] [CrossRef]
- Zuberbier, T.; Aberer, W.; Asero, R.; Abdul Latiff, A.H.; Baker, D.; Ballmer-Weber, B.; Bernstein, J.A.; Bindslev-Jensen, C.; Brzoza, Z.; Buense Bedrikow, R.; et al. The EAACI/GA(2)LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy 2018, 73, 1393–1414. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Schunemann, H.J.; Togias, A.; Bachert, C.; Erhola, M.; Hellings, P.W.; Klimek, L.; Pfaar, O.; Wallace, D.; Ansotegui, I.; et al. Next-generation Allergic Rhinitis and Its Impact on Asthma (ARIA) guidelines for allergic rhinitis based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and real-world evidence. J. Allergy Clin. Immunol. 2020, 145, 70–80.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kay, L.J.; Suvarna, S.K.; Peachell, P.T. Histamine H4 receptor mediates chemotaxis of human lung mast cells. Eur. J. Pharmacol. 2018, 837, 38–44. [Google Scholar] [CrossRef]
- Murata, Y.; Song, M.; Kikuchi, H.; Hisamichi, K.; Xu, X.L.; Greenspan, A.; Kato, M.; Chiou, C.F.; Kato, T.; Guzzo, C.; et al. Phase 2a, randomized, double-blind, placebo-controlled, multicenter, parallel-group study of a H4 R-antagonist (JNJ-39758979) in Japanese adults with moderate atopic dermatitis. J. Dermatol. 2015, 42, 129–139. [Google Scholar] [CrossRef]
- Kollmeier, A.P.; Barnathan, E.S.; O’Brien, C.; Chen, B.; Xia, Y.K.; Zhou, B.; Loza, M.J.; Silkoff, P.E.; Ge, M.; Thurmond, R.L. A phase 2a study of toreforant, a histamine H4 receptor antagonist, in eosinophilic asthma. Ann. Allergy Asthma. Immunol. 2018, 121, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Werfel, T.; Layton, G.; Yeadon, M.; Whitlock, L.; Osterloh, I.; Jimenez, P.; Liu, W.; Lynch, V.; Asher, A.; Tsianakas, A.; et al. Efficacy and safety of the histamine H4 receptor antagonist ZPL-3893787 in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 143, 1830–1837. [Google Scholar] [CrossRef]
- Maun, H.R.; Vij, R.; Walters, B.T.; Morando, A.; Jackman, J.K.; Wu, P.; Estevez, A.; Chen, X.; Franke, Y.; Lipari, M.T.; et al. Bivalent antibody pliers inhibit beta-tryptase by an allosteric mechanism dependent on the IgG hinge. Nat. Commun. 2020, 11, 6435. [Google Scholar] [CrossRef]
- Marone, G.; Galdiero, M.R.; Pecoraro, A.; Pucino, V.; Criscuolo, G.; Triassi, M.; Varricchi, G. Prostaglandin D2 receptor antagonists in allergic disorders: Safety, efficacy, and future perspectives. Expert. Opin. Investig. Drugs 2019, 28, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Brightling, C.E.; Gaga, M.; Inoue, H.; Li, J.; Maspero, J.; Wenzel, S.; Maitra, S.; Lawrence, D.; Brockhaus, F.; Lehmann, T.; et al. Effectiveness of fevipiprant in reducing exacerbations in patients with severe asthma (LUSTER-1 and LUSTER-2): Two phase 3 randomised controlled trials. Lancet Respir. Med. 2021, 9, 43–56. [Google Scholar] [CrossRef]
- Asano, K.; Sagara, H.; Ichinose, M.; Hirata, M.; Nakajima, A.; Ortega, H.; Tohda, Y. A Phase 2a Study of DP2 Antagonist GB001 for Asthma. J. Allergy Clin. Immunol. Pract. 2020, 8, 1275–1283.e1. [Google Scholar] [CrossRef]
- American Lung Association Asthma Clinical Research, C.; Peters, S.P.; Anthonisen, N.; Castro, M.; Holbrook, J.T.; Irvin, C.G.; Smith, L.J.; Wise, R.A. Randomized comparison of strategies for reducing treatment in mild persistent asthma. N. Engl. J. Med. 2007, 356, 2027–2039. [Google Scholar]
- Wollenberg, A.; Barbarot, S.; Bieber, T.; Christen-Zaech, S.; Deleuran, M.; Fink-Wagner, A.; Gieler, U.; Girolomoni, G.; Lau, S.; Muraro, A.; et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: Part II. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 850–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanania, N.A.; Korenblat, P.; Chapman, K.R.; Bateman, E.D.; Kopecky, P.; Paggiaro, P.; Yokoyama, A.; Olsson, J.; Gray, S.; Holweg, C.T.; et al. Efficacy and safety of lebrikizumab in patients with uncontrolled asthma (LAVOLTA I and LAVOLTA II): Replicate, phase 3, randomised, double-blind, placebo-controlled trials. Lancet Respir. Med. 2016, 4, 781–796. [Google Scholar] [CrossRef]
- Panettieri, R.A.; Sjobring, U., Jr.; Peterffy, A.; Wessman, P.; Bowen, K.; Piper, E.; Colice, G.; Brightling, C.E. Tralokinumab for severe, uncontrolled asthma (STRATOS 1 and STRATOS 2): Two randomised, double-blind, placebo-controlled, phase 3 clinical trials. Lancet Respir. Med. 2018, 6, 511–525. [Google Scholar] [CrossRef] [Green Version]
- Brightling, C.E.; Chanez, P.; Leigh, R.; O’Byrne, P.M.; Korn, S.; She, D.; May, R.D.; Streicher, K.; Ranade, K.; Piper, E. Efficacy and safety of tralokinumab in patients with severe uncontrolled asthma: A randomised, double-blind, placebo-controlled, phase 2b trial. Lancet Respir. Med. 2015, 3, 692–701. [Google Scholar] [CrossRef]
- Corren, J.; Lemanske, R.F.; Hanania, N.A.; Korenblat, P.E.; Parsey, M.V.; Arron, J.R.; Harris, J.M.; Scheerens, H.; Wu, L.C.; Su, Z.; et al. Lebrikizumab treatment in adults with asthma. N. Engl. J. Med. 2011, 365, 1088–1098. [Google Scholar] [CrossRef] [Green Version]
- Marone, G.; Granata, F.; Pucino, V.; Pecoraro, A.; Heffler, E.; Loffredo, S.; Scadding, G.W.; Varricchi, G. The Intriguing Role of Interleukin 13 in the Pathophysiology of Asthma. Front. Pharmacol. 2019, 10, 1387. [Google Scholar] [CrossRef]
- Wenzel, S.; Ford, L.; Pearlman, D.; Spector, S.; Sher, L.; Skobieranda, F.; Wang, L.; Kirkesseli, S.; Rocklin, R.; Bock, B.; et al. Dupilumab in persistent asthma with elevated eosinophil levels. N. Engl. J. Med. 2013, 368, 2455–2466. [Google Scholar] [CrossRef]
- Wenzel, S.; Castro, M.; Corren, J.; Maspero, J.; Wang, L.; Zhang, B.; Pirozzi, G.; Sutherland, E.R.; Evans, R.R.; Joish, V.N.; et al. Dupilumab efficacy and safety in adults with uncontrolled persistent asthma despite use of medium-to-high-dose inhaled corticosteroids plus a long-acting beta2 agonist: A randomised double-blind placebo-controlled pivotal phase 2b dose-ranging trial. Lancet 2016, 388, 31–44. [Google Scholar] [CrossRef]
- Castro, M.; Corren, J.; Pavord, I.D.; Maspero, J.; Wenzel, S.; Rabe, K.F.; Busse, W.W.; Ford, L.; Sher, L.; FitzGerald, J.M.; et al. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. N. Engl. J. Med. 2018, 378, 2486–2496. [Google Scholar] [CrossRef]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; FitzGerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N. Engl. J. Med. 2014, 371, 1198–1207. [Google Scholar] [CrossRef] [Green Version]
- Detoraki, A.; Tremante, E.; D’Amato, M.; Calabrese, C.; Casella, C.; Maniscalco, M.; Poto, R.; Brancaccio, R.; Boccia, M.; Martino, M.; et al. Mepolizumab improves sino-nasal symptoms and asthma control in severe eosinophilic asthma patients with chronic rhinosinusitis and nasal polyps: A 12-month real-life study. Ther. Adv. Respir. Dis. 2021, 15, 17534666211009398. [Google Scholar] [CrossRef]
- Castro, M.; Zangrilli, J.; Wechsler, M.E.; Bateman, E.D.; Brusselle, G.G.; Bardin, P.; Murphy, K.; Maspero, J.F.; O’Brien, C.; Korn, S. Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: Results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet Respir. Med. 2015, 3, 355–366. [Google Scholar] [CrossRef]
- Harrison, T.W.; Chanez, P.; Menzella, F.; Canonica, G.W.; Louis, R.; Cosio, B.G.; Lugogo, N.L.; Mohan, A.; Burden, A.; McDermott, L.; et al. Onset of effect and impact on health-related quality of life, exacerbation rate, lung function, and nasal polyposis symptoms for patients with severe eosinophilic asthma treated with benralizumab (ANDHI): A randomised, controlled, phase 3b trial. Lancet Respir. Med. 2021, 9, 260–274. [Google Scholar] [CrossRef]
- GINA. Global Strategy for Asthma Management and Prevention; Global Initiative for Asthma: Fontana, WI, USA, 2021. [Google Scholar]
- Castro, M.; Wenzel, S.E.; Bleecker, E.R.; Pizzichini, E.; Kuna, P.; Busse, W.W.; Gossage, D.L.; Ward, C.K.; Wu, Y.; Wang, B.; et al. Benralizumab, an anti-interleukin 5 receptor alpha monoclonal antibody, versus placebo for uncontrolled eosinophilic asthma: A phase 2b randomised dose-ranging study. Lancet Respir. Med. 2014, 2, 879–890. [Google Scholar] [CrossRef]
- Haldar, P.; Brightling, C.E.; Hargadon, B.; Gupta, S.; Monteiro, W.; Sousa, A.; Marshall, R.P.; Bradding, P.; Green, R.H.; Wardlaw, A.J.; et al. Mepolizumab and exacerbations of refractory eosinophilic asthma. N. Engl. J. Med. 2009, 360, 973–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenzel, S.E.; Barnes, P.J.; Bleecker, E.R.; Bousquet, J.; Busse, W.; Dahlen, S.E.; Holgate, S.T.; Meyers, D.A.; Rabe, K.F.; Antczak, A.; et al. A randomized, double-blind, placebo-controlled study of tumor necrosis factor-alpha blockade in severe persistent asthma. Am. J. Respir. Crit. Care Med. 2009, 179, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.W.; Holgate, S.; Kerwin, E.; Chon, Y.; Feng, J.; Lin, J.; Lin, S.L. Randomized, double-blind, placebo-controlled study of brodalumab, a human anti-IL-17 receptor monoclonal antibody, in moderate to severe asthma. Am. J. Respir. Crit. Care Med. 2013, 188, 1294–1302. [Google Scholar] [CrossRef]
- Hobo, A.; Harada, K.; Maeda, T.; Uchiyama, M.; Irisawa, R.; Yamazaki, M.; Tsuboi, R. IL-17-positive mast cell infiltration in the lesional skin of lichen planopilaris: Possible role of mast cells in inducing inflammation and dermal fibrosis in cicatricial alopecia. Exp. Dermatol. 2020, 29, 273–277. [Google Scholar] [CrossRef]
- Brightling, C.E.; Nair, P.; Cousins, D.J.; Louis, R.; Singh, D. Risankizumab in Severe Asthma—A Phase 2a, Placebo-Controlled Trial. N. Engl. J. Med. 2021, 385, 1669–1679. [Google Scholar] [CrossRef]
- Whetstone, C.E.; Ranjbar, M.; Omer, H.; Cusack, R.P.; Gauvreau, G.M. The Role of Airway Epithelial Cell Alarmins in Asthma. Cells 2022, 11, 1105. [Google Scholar] [CrossRef] [PubMed]
- Ebina-Shibuya, R.; Leonard, W.J. Role of thymic stromal lymphopoietin in allergy and beyond. Nat. Rev. Immunol. 2022, 1, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Marone, G.; Spadaro, G.; Braile, M.; Poto, R.; Criscuolo, G.; Pahima, H.; Loffredo, S.; Levi-Schaffer, F.; Varricchi, G. Tezepelumab: A novel biological therapy for the treatment of severe uncontrolled asthma. Expert. Opin. Investig. Drugs 2019, 28, 931–940. [Google Scholar] [CrossRef]
- Li, Y.; Wang, W.; Lv, Z.; Li, Y.; Chen, Y.; Huang, K.; Corrigan, C.J.; Ying, S. Elevated Expression of IL-33 and TSLP in the Airways of Human Asthmatics In Vivo: A Potential Biomarker of Severe Refractory Disease. J. Immunol. 2018, 200, 2253–2262. [Google Scholar] [CrossRef] [Green Version]
- Ko, H.K.; Cheng, S.L.; Lin, C.H.; Lin, S.H.; Hsiao, Y.H.; Su, K.C.; Yu, C.J.; Wang, H.C.; Sheu, C.C.; Chiu, K.C.; et al. Blood tryptase and thymic stromal lymphopoietin levels predict the risk of exacerbation in severe asthma. Sci. Rep. 2021, 11, 8425. [Google Scholar] [CrossRef] [PubMed]
- Corren, J.; Parnes, J.R.; Wang, L.; Mo, M.; Roseti, S.L.; Griffiths, J.M.; van der Merwe, R. Tezepelumab in Adults with Uncontrolled Asthma. N. Engl. J. Med. 2017, 377, 936–946. [Google Scholar] [CrossRef]
- Menzies-Gow, A.; Corren, J.; Bourdin, A.; Chupp, G.; Israel, E.; Wechsler, M.E.; Brightling, C.E.; Griffiths, J.M.; Hellqvist, A.; Bowen, K.; et al. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. N. Engl. J. Med. 2021, 384, 1800–1809. [Google Scholar] [CrossRef]
- Diver, S.; Khalfaoui, L.; Emson, C.; Wenzel, S.E.; Menzies-Gow, A.; Wechsler, M.E.; Johnston, J.; Molfino, N.; Parnes, J.R.; Megally, A.; et al. Effect of tezepelumab on airway inflammatory cells, remodelling, and hyperresponsiveness in patients with moderate-to-severe uncontrolled asthma (CASCADE): A double-blind, randomised, placebo-controlled, phase 2 trial. Lancet Respir. Med. 2021, 9, 1299–1312. [Google Scholar] [CrossRef]
- Sverrild, A.; Hansen, S.; Hvidtfeldt, M.; Clausson, C.M.; Cozzolino, O.; Cerps, S.; Uller, L.; Backer, V.; Erjefalt, J.; Porsbjerg, C. The effect of tezepelumab on airway hyperresponsiveness to mannitol in asthma (UPSTREAM). Eur. Respir. J. 2022, 59, 2101296. [Google Scholar] [CrossRef]
- Cao, L.; Liu, F.; Liu, Y.; Liu, T.; Wu, J.; Zhao, J.; Wang, J.; Li, S.; Xu, J.; Dong, L. TSLP promotes asthmatic airway remodeling via p38-STAT3 signaling pathway in human lung fibroblast. Exp. Lung. Res. 2018, 44, 288–301. [Google Scholar] [CrossRef]
- Braile, M.; Fiorelli, A.; Sorriento, D.; Di Crescenzo, R.M.; Galdiero, M.R.; Marone, G.; Santini, M.; Varricchi, G.; Loffredo, S. Human Lung-Resident Macrophages Express and Are Targets of Thymic Stromal Lymphopoietin in the Tumor Microenvironment. Cells 2021, 10, 2012. [Google Scholar] [CrossRef] [PubMed]
- BioMed. Harbour BioMed Announces First Subject Dosed in Phase I Study of Next-Gen Anti-TSLP Fully Human Monoclonal Antibody; BioMed: Southfield, MI, USA, 2022. [Google Scholar]
- Gauvreau, G.M.; Hohlfeld, J.; Boulet, L.-P.; Cockcroft, D.; Davis, B.; FitzGerald, J.M.; Korn, S.; Kornmann, O.; Leigh, R.; Mayers, I.; et al. Late Breaking Abstract—Efficacy of CSJ117 on allergen-induced asthmatic responses in mild atopic asthma patients. Eur. Respir. J. 2020, 56, 3690. [Google Scholar]
- Wang, W.; Li, Y.; Lv, Z.; Chen, Y.; Li, Y.; Huang, K.; Corrigan, C.J.; Ying, S. Bronchial Allergen Challenge of Patients with Atopic Asthma Triggers an Alarmin (IL-33, TSLP, and IL-25) Response in the Airways Epithelium and Submucosa. J. Immunol. 2018, 201, 2221–2231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasiuniene, E.; Janulaityte, I.; Zemeckiene, Z.; Barkauskiene, D.; Sitkauskiene, B. Elevated levels of interleukin-33 are associated with allergic and eosinophilic asthma. Scand. J. Immunol. 2019, 89, e12724. [Google Scholar] [CrossRef]
- Corrigan, C.J.; Wang, W.; Meng, Q.; Fang, C.; Eid, G.; Caballero, M.R.; Lv, Z.; An, Y.; Wang, Y.H.; Liu, Y.J.; et al. Allergen-induced expression of IL-25 and IL-25 receptor in atopic asthmatic airways and late-phase cutaneous responses. J. Allergy Clin. Immunol. 2011, 128, 116–124. [Google Scholar] [CrossRef]
- Beale, J.; Jayaraman, A.; Jackson, D.J.; Macintyre, J.D.R.; Edwards, M.R.; Walton, R.P.; Zhu, J.; Man Ching, Y.; Shamji, B.; Edwards, M.; et al. Rhinovirus-induced IL-25 in asthma exacerbation drives type 2 immunity and allergic pulmonary inflammation. Sci. Transl. Med. 2014, 6, 256ra134. [Google Scholar] [CrossRef] [Green Version]
- Wechsler, M.E.; Ruddy, M.K.; Pavord, I.D.; Israel, E.; Rabe, K.F.; Ford, L.B.; Maspero, J.F.; Abdulai, R.M.; Hu, C.C.; Martincova, R.; et al. Efficacy and Safety of Itepekimab in Patients with Moderate-to-Severe Asthma. N. Engl. J. Med. 2021, 385, 1656–1668. [Google Scholar] [CrossRef]
- Chinthrajah, S.; Cao, S.; Liu, C.; Lyu, S.C.; Sindher, S.B.; Long, A.; Sampath, V.; Petroni, D.; Londei, M.; Nadeau, K.C. Phase 2a randomized, placebo-controlled study of anti-IL-33 in peanut allergy. JCI Insight 2019, 4, e131347. [Google Scholar] [CrossRef]
- Kelsen, S.G.; Agache, I.O.; Soong, W.; Israel, E.; Chupp, G.L.; Cheung, D.S.; Theess, W.; Yang, X.; Staton, T.L.; Choy, D.F.; et al. Astegolimab (anti-ST2) efficacy and safety in adults with severe asthma: A randomized clinical trial. J. Allergy Clin. Immunol. 2021, 148, 790–798. [Google Scholar] [CrossRef]
- Bagnasco, D.; Ferrando, M.; Varricchi, G.; Puggioni, F.; Passalacqua, G.; Canonica, G.W. Anti-Interleukin 5 (IL-5) and IL-5Ra Biological Drugs: Efficacy, Safety, and Future Perspectives in Severe Eosinophilic Asthma. Front. Med. 2017, 4, 135. [Google Scholar] [CrossRef]
- Ortega, H.; Liu, M.C.; Pavord, I.D. Mepolizumab treatment in patients with severe eosinophilic asthma. N. Engl. J. Med 2015, 372, 1777. [Google Scholar] [CrossRef] [Green Version]
- Pavord, I.D.; Korn, S.; Howarth, P.; Bleecker, E.R.; Buhl, R.; Keene, O.N.; Ortega, H.; Chanez, P. Mepolizumab for severe eosinophilic asthma (DREAM): A multicentre, double-blind, placebo-controlled trial. Lancet 2012, 380, 651–659. [Google Scholar] [CrossRef]
- Chupp, G.L.; Bradford, E.S.; Albers, F.C.; Bratton, D.J.; Wang-Jairaj, J.; Nelsen, L.M.; Trevor, J.L.; Magnan, A.; Ten Brinke, A. Efficacy of mepolizumab add-on therapy on health-related quality of life and markers of asthma control in severe eosinophilic asthma (MUSCA): A randomised, double-blind, placebo-controlled, parallel-group, multicentre, phase 3b trial. Lancet Respir. Med. 2017, 5, 390–400. [Google Scholar] [CrossRef]
- Bel, E.H.; Wenzel, S.E.; Thompson, P.J.; Prazma, C.M.; Keene, O.N.; Yancey, S.W.; Ortega, H.G.; Pavord, I.D. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N. Engl. J. Med. 2014, 371, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.A.; Virchow, J.C.; Murphy, K.; Maspero, J.F.; Jacobs, J.; Adir, Y.; Humbert, M.; Castro, M.; Marsteller, D.A.; McElhattan, J.; et al. Effect of fixed-dose subcutaneous reslizumab on asthma exacerbations in patients with severe uncontrolled asthma and corticosteroid sparing in patients with oral corticosteroid-dependent asthma: Results from two phase 3, randomised, double-blind, placebo-controlled trials. Lancet Respir. Med. 2020, 8, 461–474. [Google Scholar] [PubMed] [Green Version]
- Varricchi, G.; Senna, G.; Loffredo, S.; Bagnasco, D.; Ferrando, M.; Canonica, G.W. Reslizumab and Eosinophilic Asthma: One Step Closer to Precision Medicine? Front. Immunol. 2017, 8, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bleecker, E.R.; FitzGerald, J.M.; Chanez, P.; Papi, A.; Weinstein, S.F.; Barker, P.; Sproule, S.; Gilmartin, G.; Aurivillius, M.; Werkstrom, V.; et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting beta2-agonists (SIROCCO): A randomised, multicentre, placebo-controlled phase 3 trial. Lancet 2016, 388, 2115–2127. [Google Scholar] [CrossRef]
- Ferguson, G.T.; FitzGerald, J.M.; Bleecker, E.R.; Laviolette, M.; Bernstein, D.; LaForce, C.; Mansfield, L.; Barker, P.; Wu, Y.; Jison, M.; et al. Benralizumab for patients with mild to moderate, persistent asthma (BISE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2017, 5, 568–576. [Google Scholar] [CrossRef]
- Casale, T.B.; Luskin, A.T.; Busse, W.; Zeiger, R.S.; Trzaskoma, B.; Yang, M.; Griffin, N.M.; Chipps, B.E. Omalizumab Effectiveness by Biomarker Status in Patients with Asthma: Evidence from PROSPERO, A Prospective Real-World Study. J. Allergy Clin. Immunol. Pract. 2019, 7, 156–164.e1. [Google Scholar] [CrossRef]
- Gasser, P.; Tarchevskaya, S.S.; Guntern, P.; Brigger, D.; Ruppli, R.; Zbaren, N.; Kleinboelting, S.; Heusser, C.; Jardetzky, T.S.; Eggel, A. The mechanistic and functional profile of the therapeutic anti-IgE antibody ligelizumab differs from omalizumab. Nat. Commun. 2020, 11, 165. [Google Scholar] [CrossRef] [Green Version]
- Braithwaite, I.E.; Cai, F.; Tom, J.A.; Galanter, J.M.; Owen, R.P.; Zhu, R.; Williams, M.; McGregor, A.G.; Eliahu, A.; Durk, M.R.; et al. Inhaled JAK inhibitor GDC-0214 reduces exhaled nitric oxide in patients with mild asthma: A randomized, controlled, proof-of-activity trial. J. Allergy Clin. Immunol. 2021, 148, 783–789. [Google Scholar] [CrossRef]
- Schanin, J.; Luu, T.; Korver, W.; Brock, E.C.; Benet, Z.; Xu, A.; Chang, K.; Wong, A.; Butuci, M.; McEwen, L.M.; et al. An Agonistic Monoclonal Antibody Against Siglec-6 Selectively Inhibits and Reduces Human Tissue Mast Cells; EAACI: Hamburg, Germany, 2022. [Google Scholar]
- Wilkinson, T.; Dixon, R.; Page, C.; Carroll, M.; Griffiths, G.; Ho, L.P.; De Soyza, A.; Felton, T.; Lewis, K.E.; Phekoo, K.; et al. ACCORD: A Multicentre, Seamless, Phase 2 Adaptive Randomisation Platform Study to Assess the Efficacy and Safety of Multiple Candidate Agents for the Treatment of COVID-19 in Hospitalised Patients: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 691. [Google Scholar] [PubMed]
- Ballantyne, S.J.; Barlow, J.L.; Jolin, H.E.; Nath, P.; Williams, A.S.; Chung, K.F.; Sturton, G.; Wong, S.H.; McKenzie, A.N. Blocking IL-25 prevents airway hyperresponsiveness in allergic asthma. J. Allergy Clin. Immunol. 2007, 120, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.W.; Morgan, W.J.; Gergen, P.J.; Mitchell, H.E.; Gern, J.E.; Liu, A.H.; Gruchalla, R.S.; Kattan, M.; Teach, S.J.; Pongracic, J.A.; et al. Randomized trial of omalizumab (anti-IgE) for asthma in inner-city children. N. Engl. J. Med. 2011, 364, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.A.; Marcotte, G.V.; MacGlashan, D.; Togias, A.; Saini, S. Omalizumab-induced reductions in mast cell Fce psilon RI expression and function. J. Allergy Clin. Immunol. 2004, 114, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Hanania, N.A.; Alpan, O.; Hamilos, D.L.; Condemi, J.J.; Reyes-Rivera, I.; Zhu, J.; Rosen, K.E.; Eisner, M.D.; Wong, D.A.; Busse, W. Omalizumab in severe allergic asthma inadequately controlled with standard therapy: A randomized trial. Ann. Intern. Med. 2011, 154, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Normansell, R.; Walker, S.; Milan, S.J.; Walters, E.H.; Nair, P. Omalizumab for asthma in adults and children. Cochrane Database Syst. Rev. 2014, 13, CD003559. [Google Scholar] [CrossRef]
- Hew, M.; Gillman, A.; Sutherland, M.; Wark, P.; Bowden, J.; Guo, M.; Reddel, H.K.; Jenkins, C.; Marks, G.B.; Thien, F.; et al. Real-life effectiveness of omalizumab in severe allergic asthma above the recommended dosing range criteria. Clin. Exp. Allergy 2016, 46, 1407–1415. [Google Scholar] [CrossRef]
- Alhossan, A.; Lee, C.S.; MacDonald, K.; Abraham, I. “Real-life” Effectiveness Studies of Omalizumab in Adult Patients with Severe Allergic Asthma: Meta-analysis. J. Allergy Clin. Immunol. Pract. 2017, 5, 1362–1370.e2. [Google Scholar] [CrossRef]
- Esquivel, A.; Busse, W.W.; Calatroni, A.; Togias, A.G.; Grindle, K.G.; Bochkov, Y.A.; Gruchalla, R.S.; Kattan, M.; Kercsmar, C.M.; Khurana Hershey, G.; et al. Effects of Omalizumab on Rhinovirus Infections, Illnesses, and Exacerbations of Asthma. Am. J. Respir. Crit. Care Med. 2017, 196, 985–992. [Google Scholar] [CrossRef]
- Pelaia, C.; Calabrese, C.; Terracciano, R.; de Blasio, F.; Vatrella, A.; Pelaia, G. Omalizumab, the first available antibody for biological treatment of severe asthma: More than a decade of real-life effectiveness. Ther. Adv. Respir. Dis. 2018, 12, 1753466618810192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennington, L.F.; Tarchevskaya, S.; Brigger, D.; Sathiyamoorthy, K.; Graham, M.T.; Nadeau, K.C.; Eggel, A.; Jardetzky, T.S. Structural basis of omalizumab therapy and omalizumab-mediated IgE exchange. Nat. Commun. 2016, 7, 11610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruse, G.; Yin, Y.; Fukuyama, T.; Desai, A.; Arthur, G.K.; Baumer, W.; Beaven, M.A.; Metcalfe, D.D. Exon skipping of FcepsilonRIbeta eliminates expression of the high-affinity IgE receptor in mast cells with therapeutic potential for allergy. Proc. Natl. Acad. Sci. USA 2016, 113, 14115–14120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kambayashi, T.; Koretzky, G.A. Proximal signaling events in Fc epsilon RI-mediated mast cell activation. J. Allergy Clin. Immunol 2007, 119, 544–552. [Google Scholar] [CrossRef]
- Villoutreix, B.O.; Laconde, G.; Lagorce, D.; Martineau, P.; Miteva, M.A.; Dariavach, P. Tyrosine kinase syk non-enzymatic inhibitors and potential anti-allergic drug-like compounds discovered by virtual and in vitro screening. PLoS ONE 2011, 6, e21117. [Google Scholar] [CrossRef]
- Hayashi, H.; Kaneko, R.; Demizu, S.; Akasaka, D.; Tayama, M.; Harada, T.; Irie, H.; Ogino, Y.; Fujino, N.; Sasaki, E. TAS05567, a Novel Potent and Selective Spleen Tyrosine Kinase Inhibitor, Abrogates Immunoglobulin-Mediated Autoimmune and Allergic Reactions in Rodent Models. J. Pharmacol. Exp. Ther. 2018, 366, 84–95. [Google Scholar] [CrossRef]
- Ramis, I.; Otal, R.; Carreno, C.; Domenech, A.; Eichhorn, P.; Orellana, A.; Maldonado, M.; De Alba, J.; Prats, N.; Fernandez, J.C.; et al. A novel inhaled Syk inhibitor blocks mast cell degranulation and early asthmatic response. Pharmacol. Res. 2015, 99, 116–124. [Google Scholar] [CrossRef]
- Tabeling, C.; Herbert, J.; Hocke, A.C.; Lamb, D.J.; Wollin, S.L.; Erb, K.J.; Boiarina, E.; Movassagh, H.; Scheffel, J.; Doehn, J.M.; et al. Spleen tyrosine kinase inhibition blocks airway constriction and protects from Th2-induced airway inflammation and remodeling. Allergy 2017, 72, 1061–1072. [Google Scholar] [CrossRef]
- Strich, J.R.; Ramos-Benitez, M.J.; Randazzo, D.; Stein, S.R.; Babyak, A.; Davey, R.T.; Suffredini, A.F.; Childs, R.W.; Chertow, D.S. Fostamatinib Inhibits Neutrophils Extracellular Traps Induced by COVID-19 Patient Plasma: A Potential Therapeutic. J. Infect. Dis. 2021, 223, 981–984. [Google Scholar] [CrossRef]
- Koziol-White, C.J.; Jia, Y.; Baltus, G.A.; Cooper, P.R.; Zaller, D.M.; Crackower, M.A.; Sirkowski, E.E.; Smock, S.; Northrup, A.B.; Himes, B.E.; et al. Inhibition of spleen tyrosine kinase attenuates IgE-mediated airway contraction and mediator release in human precision cut lung slices. Br. J. Pharmacol. 2016, 173, 3080–3087. [Google Scholar] [CrossRef] [Green Version]
- Meltzer, E.O.; Berkowitz, R.B.; Grossbard, E.B. An intranasal Syk-kinase inhibitor (R112) improves the symptoms of seasonal allergic rhinitis in a park environment. J. Allergy Clin. Immunol. 2005, 115, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Guyer, B.J.; Shimamoto, S.R.; Bradhurst, A.L.; Grossbard, E.B.; Dreskin, S.C.; Nelson, H.S. Mast cell inhibitor R112 is well tolerated and affects prostaglandin D2 but not other mediators, symptoms, or nasal volumes in a nasal challenge model of allergic rhinitis. Allergy Asthma Proc. 2006, 27, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Awan, F.T.; Addison, D.; Alfraih, F.; Baratta, S.J.; Campos, R.N.; Cugliari, M.S.; Goh, Y.T.; Ionin, V.A.; Mundnich, S.; Sverdlov, A.L.; et al. International consensus statement on the management of cardiovascular risk of Bruton’s tyrosine kinase inhibitors in CLL. Blood Adv. 2022, 6, 5516–5525. [Google Scholar] [CrossRef]
- Dispenza, M.C.; Krier-Burris, R.A.; Chhiba, K.D.; Undem, B.J.; Robida, P.A.; Bochner, B.S. Bruton’s tyrosine kinase inhibition effectively protects against human IgE-mediated anaphylaxis. J. Clin. Invest. 2020, 130, 4759–4770. [Google Scholar] [CrossRef]
- Dispenza, M.C.; Pongracic, J.A.; Singh, A.M.; Bochner, B.S. Short-term ibrutinib therapy suppresses skin test responses and eliminates IgE-mediated basophil activation in adults with peanut or tree nut allergy. J. Allergy Clin. Immunol. 2018, 141, 1914–1916.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, H.; Matsumoto, K.; Saito, H. Biologics for allergic and immunologic diseases. J. Allergy Clin. Immunol. 2022, 150, 766–777. [Google Scholar] [CrossRef] [PubMed]
- Youngblood, B.A.; Brock, E.C.; Leung, J.; Falahati, R.; Bryce, P.J.; Bright, J.; Williams, J.; Shultz, L.D.; Greiner, D.L.; Brehm, M.A.; et al. AK002, a Humanized Sialic Acid-Binding Immunoglobulin-Like Lectin-8 Antibody that Induces Antibody-Dependent Cell-Mediated Cytotoxicity against Human Eosinophils and Inhibits Mast Cell-Mediated Anaphylaxis in Mice. Int. Arch. Allergy Immunol. 2019, 180, 91–102. [Google Scholar] [CrossRef]
- Kerr, S.C.; Gonzalez, J.R.; Schanin, J.; Peters, M.C.; Lambrecht, B.N.; Brock, E.C.; Charbit, A.; Ansel, K.M.; Youngblood, B.A.; Fahy, J.V. An anti-siglec-8 antibody depletes sputum eosinophils from asthmatic subjects and inhibits lung mast cells. Clin. Exp. Allergy 2020, 50, 904–914. [Google Scholar] [CrossRef]
- Schanin, J.; Gebremeskel, S.; Korver, W.; Falahati, R.; Butuci, M.; Haw, T.J.; Nair, P.M.; Liu, G.; Hansbro, N.G.; Hansbro, P.M.; et al. A monoclonal antibody to Siglec-8 suppresses non-allergic airway inflammation and inhibits IgE-independent mast cell activation. Mucosal Immunol. 2021, 14, 366–376. [Google Scholar] [CrossRef]
- Dellon, E.S.; Peterson, K.A.; Murray, J.A.; Falk, G.W.; Gonsalves, N.; Chehade, M.; Genta, R.M.; Leung, J.; Khoury, P.; Klion, A.D.; et al. Anti-Siglec-8 Antibody for Eosinophilic Gastritis and Duodenitis. N. Engl. J. Med. 2020, 383, 1624–1634. [Google Scholar] [CrossRef]
- Bhasin, S.; Gill, T.M.; Reuben, D.B.; Latham, N.K.; Ganz, D.A.; Greene, E.J.; Dziura, J.; Basaria, S.; Gurwitz, J.H.; Dykes, P.C.; et al. A Randomized Trial of a Multifactorial Strategy to Prevent Serious Fall Injuries. N. Engl. J. Med. 2020, 383, 129–140. [Google Scholar] [CrossRef]
- Shehata, Y.; Sheikh, A. Farming, childhood allergy, and unpasteurised milk A review of; “Which aspects of the farming lifestyle explain the inwerse association with childhood allergy.” Perkin MR, Strachan DP. Prim. Care Respir. J. 2007, 16, 59–60. [Google Scholar]
- Bachelet, I.; Munitz, A.; Berent-Maoz, B.; Mankuta, D.; Levi-Schaffer, F. Suppression of normal and malignant kit signaling by a bispecific antibody linking kit with CD300a. J. Immunol. 2008, 180, 6064–6069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggel, A.; Buschor, P.; Baumann, M.J.; Amstutz, P.; Stadler, B.M.; Vogel, M. Inhibition of ongoing allergic reactions using a novel anti-IgE DARPin-Fc fusion protein. Allergy 2011, 66, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Eggel, A.; Tarchevskaya, S.S.; Vogel, M.; Prinz, H.; Jardetzky, T.S. Accelerated disassembly of IgE-receptor complexes by a disruptive macromolecular inhibitor. Nature 2012, 491, 613–617. [Google Scholar] [CrossRef] [Green Version]
- Arock, M.; Hoermann, G.; Sotlar, K.; Hermine, O.; Sperr, W.R.; Hartmann, K.; Brockow, K.; Akin, C.; Triggiani, M.; Broesby-Olsen, S.; et al. Clinical impact and proposed application of molecular markers, genetic variants, and cytogenetic analysis in mast cell neoplasms: Status 2022. J. Allergy Clin. Immunol. 2022, 149, 1855–1865. [Google Scholar] [CrossRef]
- Arock, M.; Sotlar, K.; Akin, C.; Broesby-Olsen, S.; Hoermann, G.; Escribano, L.; Kristensen, T.K.; Kluin-Nelemans, H.C.; Hermine, O.; Dubreuil, P.; et al. KIT mutation analysis in mast cell neoplasms: Recommendations of the European Competence Network on Mastocytosis. Leukemia 2015, 29, 1223–1232. [Google Scholar] [CrossRef] [Green Version]
- Valent, P.; Akin, C.; Bonadonna, P.; Hartmann, K.; Brockow, K.; Niedoszytko, M.; Nedoszytko, B.; Siebenhaar, F.; Sperr, W.R.; Oude Elberink, J.N.G.; et al. Proposed Diagnostic Algorithm for Patients with Suspected Mast Cell Activation Syndrome. J. Allergy Clin. Immunol. Pract. 2019, 7, 1125–1133. [Google Scholar] [CrossRef]
- Fonseca, W.; Rasky, A.J.; Ptaschinski, C.; Morris, S.H.; Best, S.K.K.; Phillips, M.; Malinczak, C.A.; Lukacs, N.W. Group 2 innate lymphoid cells (ILC2) are regulated by stem cell factor during chronic asthmatic disease. Mucosal Immunol. 2019, 12, 445–456. [Google Scholar] [CrossRef]
- Ptaschinski, C.; Rasky, A.J.; Fonseca, W.; Lukacs, N.W. Stem Cell Factor Neutralization Protects From Severe Anaphylaxis in a Murine Model of Food Allergy. Front. Immunol. 2021, 12, 604192. [Google Scholar] [CrossRef]
- Brandt, E.B.; Strait, R.T.; Hershko, D.; Wang, Q.; Muntel, E.E.; Scribner, T.A.; Zimmermann, N.; Finkelman, F.D.; Rothenberg, M.E. Mast cells are required for experimental oral allergen-induced diarrhea. J. Clin. Invest. 2003, 112, 1666–1677. [Google Scholar]
- Terhorst-Molawi, D.; Hawro, T.; Grekowitz, E.; Kiefer, L.; Metz, M.; Alvarado, D.; Hawthorne, T.; Merchant, K.; Crew, L.; Crowley, E.; et al. The Anti-KIT Antibody, CDX-0159, Reduces Mast Cell Numbers and Circulating Tryptase and Improves Disease Control in Patients with Chronic Inducible Urticaria (Cindu). J. Allergy Clin. Immunol. 2022, 149, AB178. [Google Scholar] [CrossRef]
- Rasky, A.; Habiel, D.M.; Morris, S.; Schaller, M.; Moore, B.B.; Phan, S.; Kunkel, S.L.; Phillips, M.; Hogaboam, C.; Lukacs, N.W. Inhibition of the stem cell factor 248 isoform attenuates the development of pulmonary remodeling disease. Am. J. Physiol. Lung. Cell Mol. Physiol. 2020, 318, L200–L211. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.; Khan, D.A.; Elieh Ali Komi, D.; Kaplan, A.P. Biologics for the Use in Chronic Spontaneous Urticaria: When and Which. J. Allergy Clin. Immunol. Pract. 2021, 9, 1067–1078. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, D.; Maurer, M.; Gedrich, R.; Seibel, S.B.; Murphy, M.B.; Crew, L.; Goldstein, J.; Crocker, A.; Vitale, L.A.; Morani, P.A.; et al. Anti-KIT monoclonal antibody CDX-0159 induces profound and durable mast cell suppression in a healthy volunteer study. Allergy 2022, 77, 2393–2403. [Google Scholar] [CrossRef]
- Valent, P.; Akin, C.; Hartmann, K.; Reiter, A.; Gotlib, J.; Sotlar, K.; Sperr, W.R.; Degenfeld-Schonburg, L.; Smiljkovic, D.; Triggiani, M.; et al. Drug-induced mast cell eradication: A novel approach to treat mast cell activation disorders? J. Allergy Clin. Immunol. 2022, 149, 1866–1874. [Google Scholar] [CrossRef] [PubMed]
- Kolkhir, P.; Elieh-Ali-Komi, D.; Metz, M.; Siebenhaar, F.; Maurer, M. Understanding human mast cells: Lesson from therapies for allergic and non-allergic diseases. Nat. Rev. Immunol. 2022, 22, 294–308. [Google Scholar] [CrossRef]
- Cahill, K.N.; Katz, H.R.; Cui, J.; Lai, J.; Kazani, S.; Crosby-Thompson, A.; Garofalo, D.; Castro, M.; Jarjour, N.; DiMango, E.; et al. KIT Inhibition by Imatinib in Patients with Severe Refractory Asthma. N. Engl. J. Med. 2017, 376, 1911–1920. [Google Scholar] [CrossRef] [Green Version]
- Chanez, P.; Israel, E.; Davidescu, L.; Ursol, G.; Korzh, O.; Deshmukh, V.; Kuryk, L.; Nortje, M.-M.; Godlevska, O.; Devouassoux, G.; et al. Abstract: Masitinib significantly decreases the rate of asthma exacerbations in patients with severe asthma uncontrolled by oral corticosteroids: A phase 3 multicenter study. Am. J. Respir. Crit. Care Med. 2020, 201, A4210. [Google Scholar]
- Humbert, M.; de Blay, F.; Garcia, G.; Prud’homme, A.; Leroyer, C.; Magnan, A.; Tunon-de-Lara, J.M.; Pison, C.; Aubier, M.; Charpin, D.; et al. Masitinib, a c-kit/PDGF receptor tyrosine kinase inhibitor, improves disease control in severe corticosteroid-dependent asthmatics. Allergy 2009, 64, 1194–1201. [Google Scholar] [CrossRef]
- Lee-Fowler, T.M.; Guntur, V.; Dodam, J.; Cohn, L.A.; DeClue, A.E.; Reinero, C.R. The tyrosine kinase inhibitor masitinib blunts airway inflammation and improves associated lung mechanics in a feline model of chronic allergic asthma. Int. Arch. Allergy Immunol. 2012, 158, 369–374. [Google Scholar] [CrossRef]
- Vaali, K.; Lappalainen, J.; Lin, A.H.; Mayranpaa, M.I.; Kovanen, P.T.; Berstad, A.; Eklund, K.K. Imatinib mesylate alleviates diarrhea in a mouse model of intestinal allergy. Neurogastroenterol. Motil. 2012, 24, e325–e335. [Google Scholar] [CrossRef]
- Jung, S.H.; Sun, X.; Ryu, W.S.; Yang, B.S. Topical administration of the pan-Src kinase inhibitors, dasatinib and LCB 03-0110, prevents allergic contact dermatitis in mice. Br. J. Dermatol. 2013, 168, 112–119. [Google Scholar] [CrossRef] [PubMed]
- da Silva, A.L.; Magalhaes, R.F.; Branco, V.C.; Silva, J.D.; Cruz, F.F.; Marques, P.S.; Ferreira, T.P.; Morales, M.M.; Martins, M.A.; Olsen, P.C.; et al. The tyrosine kinase inhibitor dasatinib reduces lung inflammation and remodelling in experimental allergic asthma. Br. J. Pharmacol. 2016, 173, 1236–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotlib, J.; Reiter, A.; Radia, D.H.; Deininger, M.W.; George, T.I.; Panse, J.; Vannucchi, A.M.; Platzbecker, U.; Alvarez-Twose, I.; Mital, A.; et al. Efficacy and safety of avapritinib in advanced systemic mastocytosis: Interim analysis of the phase 2 PATHFINDER trial. Nat. Med. 2021, 27, 2192–2199. [Google Scholar] [CrossRef]
- DeAngelo, D.J.; Radia, D.H.; George, T.I.; Robinson, W.A.; Quiery, A.T.; Drummond, M.W.; Bose, P.; Hexner, E.O.; Winton, E.F.; Horny, H.P.; et al. Safety and efficacy of avapritinib in advanced systemic mastocytosis: The phase 1 EXPLORER trial. Nat. Med. 2021, 27, 2183–2191. [Google Scholar] [CrossRef]
- Kneidinger, M.; Schmidt, U.; Rix, U.; Gleixner, K.V.; Vales, A.; Baumgartner, C.; Lupinek, C.; Weghofer, M.; Bennett, K.L.; Herrmann, H.; et al. The effects of dasatinib on IgE receptor-dependent activation and histamine release in human basophils. Blood 2008, 111, 3097–3107. [Google Scholar] [CrossRef] [Green Version]
- Peter, B.; Winter, G.E.; Blatt, K.; Bennett, K.L.; Stefanzl, G.; Rix, U.; Eisenwort, G.; Hadzijusufovic, E.; Gridling, M.; Dutreix, C.; et al. Target interaction profiling of midostaurin and its metabolites in neoplastic mast cells predicts distinct effects on activation and growth. Leukemia 2016, 30, 464–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krauth, M.T.; Mirkina, I.; Herrmann, H.; Baumgartner, C.; Kneidinger, M.; Valent, P. Midostaurin (PKC412) inhibits immunoglobulin E-dependent activation and mediator release in human blood basophils and mast cells. Clin. Exp. Allergy 2009, 39, 1711–1720. [Google Scholar] [CrossRef]
- Savage, J.H.; Courneya, J.P.; Sterba, P.M.; Macglashan, D.W.; Saini, S.S.; Wood, R.A. Kinetics of mast cell, basophil, and oral food challenge responses in omalizumab-treated adults with peanut allergy. J. Allergy Clin. Immunol. 2012, 130, 1123–1129.e2. [Google Scholar] [CrossRef] [Green Version]
- Ishizaka, K.; Ishizaka, T.; Hornbrook, M.M. Physico-chemical properties of human reaginic antibody. IV. Presence of a unique immunoglobulin as a carrier of reaginic activity. J. Immunol. 1966, 97, 75–85. [Google Scholar] [PubMed]
- Johansson, S.G.; Bennich, H. Immunological studies of an atypical (myeloma) immunoglobulin. Immunology 1967, 13, 381–394. [Google Scholar] [PubMed]
- Varricchi, G.; Pecoraro, A.; Loffredo, S.; Poto, R.; Rivellese, F.; Genovese, A.; Marone, G.; Spadaro, G. Heterogeneity of Human Mast Cells With Respect to MRGPRX2 Receptor Expression and Function. Front. Cell Neurosci. 2019, 13, 299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vivanco Gonzalez, N.; Oliveria, J.P.; Tebaykin, D.; Ivison, G.T.; Mukai, K.; Tsai, M.M.; Borges, L.; Nadeau, K.C.; Galli, S.J.; Tsai, A.G.; et al. Mass Cytometry Phenotyping of Human Granulocytes Reveals Novel Basophil Functional Heterogeneity. iScience 2020, 23, 101724. [Google Scholar] [CrossRef] [PubMed]
- Derakhshan, T.; Boyce, J.A.; Dwyer, D.F. Defining mast cell differentiation and heterogeneity through single-cell transcriptomics analysis. J. Allergy Clin. Immunol. 2022, 150, 739–747. [Google Scholar] [CrossRef]
- Heijink, I.H.; Kuchibhotla, V.N.S.; Roffel, M.P.; Maes, T.; Knight, D.A.; Sayers, I.; Nawijn, M.C. Epithelial cell dysfunction, a major driver of asthma development. Allergy 2020, 75, 1902–1917. [Google Scholar] [CrossRef]
- Cohen, M.; Giladi, A.; Gorki, A.D.; Solodkin, D.G.; Zada, M.; Hladik, A.; Miklosi, A.; Salame, T.M.; Halpern, K.B.; David, E.; et al. Lung Single-Cell Signaling Interaction Map Reveals Basophil Role in Macrophage Imprinting. Cell 2018, 175, 1031–1044.e18. [Google Scholar] [CrossRef] [Green Version]
- Aegerter, H.; Lambrecht, B.N.; Jakubzick, C.V. Biology of lung macrophages in health and disease. Immunity 2022, 55, 1564–1580. [Google Scholar] [CrossRef]
- Balestrieri, B.; Granata, F.; Loffredo, S.; Petraroli, A.; Scalia, G.; Morabito, P.; Cardamone, C.; Varricchi, G.; Triggiani, M. Phenotypic and Functional Heterogeneity of Low-Density and High-Density Human Lung Macrophages. Biomedicines 2021, 9, 505. [Google Scholar] [CrossRef]
- MacGlashan, D.; Saini, S., Jr.; Schroeder, J.T. Response of peripheral blood basophils in subjects with chronic spontaneous urticaria during treatment with omalizumab. J. Allergy Clin. Immunol. 2021, 147, 2295–2304.e12. [Google Scholar] [CrossRef]
- Lommatzsch, M.; Marchewski, H.; Schwefel, G.; Stoll, P.; Virchow, J.C.; Bratke, K. Benralizumab strongly reduces blood basophils in severe eosinophilic asthma. Clin. Exp. Allergy 2020, 50, 1267–1269. [Google Scholar] [CrossRef] [PubMed]
- Galli, S.J.; Gaudenzio, N.; Tsai, M. Mast Cells in Inflammation and Disease: Recent Progress and Ongoing Concerns. Annu. Rev. Immunol. 2020, 38, 49–77. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic representation of activating (in red) and inhibitory (in black) receptors on human lung mast cells. A complete (αβγ2), high-affinity receptor for IgE (FcεRI) is expressed by human mast cells and basophils [31]. Antigens, superantigens, and anti-IgE lead to mast cell activation and mediator release through the aggregation of FcεRI bound to IgE [31,32,33]. Mast cells play a role in allergic disorders by releasing preformed (e.g., histamine, tryptase) and de novo synthesized mediators (e.g., cysteinyl leukotriene C4 (LTC4), prostaglandin D2 (PGD2)) and several cytokines and chemokines [3,19]. SCF, which activates the KIT receptor (CD117), highly expressed by mast cells throughout their development, is the most important factor regulating these cells [34,35]. SCF is released by a plethora of cells, including fibroblasts, endothelial cells, and mast cells themselves [36,37]. Thymic stromal lymphopoietin (TSLP) is expressed by airway epithelial cells [38], keratinocytes [39], immune and structural cells [40] and acts as an alarmin. TSLP activates the heterodimeric receptor comprising IL-7Rα and TSLP receptor (TSLPR) on mast cells and other immune cells [41,42,43]. TSLPR mRNA, but not IL-7Rα mRNA, is expressed by human mast cells [42,44]. TSLP, under certain experimental conditions [42], can induce the release of chemokines and cytokines from mast cells [45]. IL-33 is released by damaged epithelial and endothelial cells [46,47] and activates mast cells [48,49]. IL-33 engages the heterodimeric receptor, ST2-IL-1RAcP, on human mast cells [50,51,52] and induces cytokine [50,53,54,55,56] and chemokine release [57]. IL-33 and superantigenic activation cause the release of angiogenic and lymphangiogenic factors from human lung mast cells (HLMCs) [58]. Different mast cell subsets display distinct toll-like receptors (TLRs) [59]. Activation of TLR2, -3, -4, -6, -7, and -9 induce cytokine release from human mast cells [60,61,62]. FcεRI cross-linking amplifies TLR-induced cytokine released from human mast cells [63]. Histamine is preformed in cytoplasmic granules of human mast cells (≅3 pg/cell) and basophils (≅1 pg/cell) [64,65]. Human mast cells express the histamine H1 and H4 receptors [66]. Histamine induces exocytosis and IL-6 production from human lung macrophages by activating H1 receptors [67]. High concentrations of certain H1-antihistamines can inhibit mediator release from human FcεRI+ cells [68,69]. H4R is expressed by human mast cells, and its activation can modulate the function of these cells [66]. Mast cells display several inhibitory receptors [70,71], such as CD300a and CD200R [72,73]. Coaggregation of CD300a and FcεRI with a bispecific antibody inhibits IgE-mediated tryptase and IL-4 release from human mast cells [74] and IgE-mediated anaphylaxis in preclinical asthma models [75]. Siglecs are inhibitory receptors expressed on immune cells [76]. Siglec-8 is expressed on murine and human mast cells [77,78] and on mast cell lines [76,77,79]. Siglec-8 monoclonal antibody (mAb) diminishes FcεRI-mediated histamine and PGD2 release from mast cells [80]. Siglec-8 is also present on eosinophils and basophils [81,82]. Siglec-6 is selectively expressed by mast cells [76], and a mAb cross-linking this receptor (AK006) potently inhibits IgE-mediated human mast cell activation. Siglec-6 interacts with KIT/CD117 and inhibits SCF-mediated mast cell activation (Korver, Schanin, 10th EMBRN meeting, July 11–12, 2022). Human mast cells express the activating FcγRIIA and FcγRI induced by IFN-γ [83]. A human IgG-IgE Fc fusion protein co-crosslinks FcεRI and FcγRII receptors and inhibits histamine release from human basophils and HLMCs [84,85,86]. A dual-targeting tandem IgE-IgG Fc domain inhibits mast cell degranulation [87].
Figure 1.
Schematic representation of activating (in red) and inhibitory (in black) receptors on human lung mast cells. A complete (αβγ2), high-affinity receptor for IgE (FcεRI) is expressed by human mast cells and basophils [31]. Antigens, superantigens, and anti-IgE lead to mast cell activation and mediator release through the aggregation of FcεRI bound to IgE [31,32,33]. Mast cells play a role in allergic disorders by releasing preformed (e.g., histamine, tryptase) and de novo synthesized mediators (e.g., cysteinyl leukotriene C4 (LTC4), prostaglandin D2 (PGD2)) and several cytokines and chemokines [3,19]. SCF, which activates the KIT receptor (CD117), highly expressed by mast cells throughout their development, is the most important factor regulating these cells [34,35]. SCF is released by a plethora of cells, including fibroblasts, endothelial cells, and mast cells themselves [36,37]. Thymic stromal lymphopoietin (TSLP) is expressed by airway epithelial cells [38], keratinocytes [39], immune and structural cells [40] and acts as an alarmin. TSLP activates the heterodimeric receptor comprising IL-7Rα and TSLP receptor (TSLPR) on mast cells and other immune cells [41,42,43]. TSLPR mRNA, but not IL-7Rα mRNA, is expressed by human mast cells [42,44]. TSLP, under certain experimental conditions [42], can induce the release of chemokines and cytokines from mast cells [45]. IL-33 is released by damaged epithelial and endothelial cells [46,47] and activates mast cells [48,49]. IL-33 engages the heterodimeric receptor, ST2-IL-1RAcP, on human mast cells [50,51,52] and induces cytokine [50,53,54,55,56] and chemokine release [57]. IL-33 and superantigenic activation cause the release of angiogenic and lymphangiogenic factors from human lung mast cells (HLMCs) [58]. Different mast cell subsets display distinct toll-like receptors (TLRs) [59]. Activation of TLR2, -3, -4, -6, -7, and -9 induce cytokine release from human mast cells [60,61,62]. FcεRI cross-linking amplifies TLR-induced cytokine released from human mast cells [63]. Histamine is preformed in cytoplasmic granules of human mast cells (≅3 pg/cell) and basophils (≅1 pg/cell) [64,65]. Human mast cells express the histamine H1 and H4 receptors [66]. Histamine induces exocytosis and IL-6 production from human lung macrophages by activating H1 receptors [67]. High concentrations of certain H1-antihistamines can inhibit mediator release from human FcεRI+ cells [68,69]. H4R is expressed by human mast cells, and its activation can modulate the function of these cells [66]. Mast cells display several inhibitory receptors [70,71], such as CD300a and CD200R [72,73]. Coaggregation of CD300a and FcεRI with a bispecific antibody inhibits IgE-mediated tryptase and IL-4 release from human mast cells [74] and IgE-mediated anaphylaxis in preclinical asthma models [75]. Siglecs are inhibitory receptors expressed on immune cells [76]. Siglec-8 is expressed on murine and human mast cells [77,78] and on mast cell lines [76,77,79]. Siglec-8 monoclonal antibody (mAb) diminishes FcεRI-mediated histamine and PGD2 release from mast cells [80]. Siglec-8 is also present on eosinophils and basophils [81,82]. Siglec-6 is selectively expressed by mast cells [76], and a mAb cross-linking this receptor (AK006) potently inhibits IgE-mediated human mast cell activation. Siglec-6 interacts with KIT/CD117 and inhibits SCF-mediated mast cell activation (Korver, Schanin, 10th EMBRN meeting, July 11–12, 2022). Human mast cells express the activating FcγRIIA and FcγRI induced by IFN-γ [83]. A human IgG-IgE Fc fusion protein co-crosslinks FcεRI and FcγRII receptors and inhibits histamine release from human basophils and HLMCs [84,85,86]. A dual-targeting tandem IgE-IgG Fc domain inhibits mast cell degranulation [87].

Figure 2.
Schematic representation of the multiple interactions between human lung mast cells and several cells of the innate and adaptive immune system through the release of mediators. Mast cells can interact with monocytes (histamine, LTD4, VEGF-A, and PAF), macrophages (histamine, IL-13, IL-6, PAF, and PGD2), dendritic cells (DCs) (histamine, PGE2, PGD2, VEGF-C, and IL-13), ILCs (IL-1β, IL-9, PGD2, and LTD4), NK cells (histamine and heparin), T cells (histamine, LTC4, LTD4, and TNF-α), TH1 (histamine) and TH2 (histamine, LTC4, LTD4, and PGD2) cells, TFH cells (IL-6), B cells (histamine, PAF, and IL-5), Treg cells (histamine), eosinophils (histamine, IL-5, IL-9, SCF, LTD4, PAF, PGD2, and VEGF-A), neutrophils (histamine, LTB4, PAF, and heparin), basophils (histamine, PAF, and PGD2), and platelets (PAF). Modified with permission from Varricchi 2019 [151].
Figure 2.
Schematic representation of the multiple interactions between human lung mast cells and several cells of the innate and adaptive immune system through the release of mediators. Mast cells can interact with monocytes (histamine, LTD4, VEGF-A, and PAF), macrophages (histamine, IL-13, IL-6, PAF, and PGD2), dendritic cells (DCs) (histamine, PGE2, PGD2, VEGF-C, and IL-13), ILCs (IL-1β, IL-9, PGD2, and LTD4), NK cells (histamine and heparin), T cells (histamine, LTC4, LTD4, and TNF-α), TH1 (histamine) and TH2 (histamine, LTC4, LTD4, and PGD2) cells, TFH cells (IL-6), B cells (histamine, PAF, and IL-5), Treg cells (histamine), eosinophils (histamine, IL-5, IL-9, SCF, LTD4, PAF, PGD2, and VEGF-A), neutrophils (histamine, LTB4, PAF, and heparin), basophils (histamine, PAF, and PGD2), and platelets (PAF). Modified with permission from Varricchi 2019 [151].

Figure 3.
Schematic representation of the multiple interactions between human lung mast cells and various non-immune cells through the release of mediators. Mast cells can interact with bronchial epithelial cells (IL-13, TNF-α, IL-9, TGF-β, and PGD2), brush cells (LTE4), fibroblasts (tryptase, PGD2, TNF-α, TGF-β, IL-13, and IL-1β), smooth-muscle cells (histamine, LTC4, LTD4, PGD2, and tryptase), goblet cells (IL-13 and LTE4), blood endothelial cells (histamine, LTC4, LTD4, PGD2, PAF, VEGF-A, IL-13, and IL-1β), lymphatic endothelial cells (VEGF-C and VEGF-D), and neurons (histamine, NGF, SP, and PGD2). Modified with permission from Varricchi 2019 [151].
Figure 3.
Schematic representation of the multiple interactions between human lung mast cells and various non-immune cells through the release of mediators. Mast cells can interact with bronchial epithelial cells (IL-13, TNF-α, IL-9, TGF-β, and PGD2), brush cells (LTE4), fibroblasts (tryptase, PGD2, TNF-α, TGF-β, IL-13, and IL-1β), smooth-muscle cells (histamine, LTC4, LTD4, PGD2, and tryptase), goblet cells (IL-13 and LTE4), blood endothelial cells (histamine, LTC4, LTD4, PGD2, PAF, VEGF-A, IL-13, and IL-1β), lymphatic endothelial cells (VEGF-C and VEGF-D), and neurons (histamine, NGF, SP, and PGD2). Modified with permission from Varricchi 2019 [151].

Figure 4.
Schematic representation of mast cell-targeted biologics and drugs approved, under development, or potentially useful for asthma treatment. Several immunological stimuli (allergens, super allergens, bacterial, fungal, and viral products, smoke extracts) can damage bronchial epithelial cells to release alarmins, such as thymic stromal lymphopoietin (TSLP) [187,196], IL-33 [196,197], and IL-25 [196,198,199]. Monoclonal antibodies (mAbs) targeting TSLP (tezepelumab) [188,189], IL-33 (etokimab, itepekimab, tozorakimab) [200,201] (NCT04570657), or the IL-33 receptor ST2 (astegolimab) [202], have been approved or are under investigation for asthma treatment. mAbs targeting IL-5, produced by human mast cells [203], such as mepolizumab [204,205,206,207], reslizumab [208,209], or its receptor IL-5Rα (benralizumab) [175,210,211], have been approved for the treatment of eosinophilic asthma. Dupilumab blocks IL-4Rα and is approved for severe asthma [169,170,171]. Omalizumab was the first mAb approved for asthma treatment [212]. Novel mAbs anti-IgE (ligelizumab, UB-221, GI-301, UCB-8600) are under investigation for allergic disorder treatment [213] (NCT05298215; NTC04444466). Other strategies to treat mast cell-driven disease include inhibitors of spleen tyrosine kinase (SYK) (GSK2646264), Bruton’s tyrosine kinase (BTK) (acalabrutinib, fenebrutinib, ibrutinib, remibrutinib), and Janus kinase (JAK) inhibitors (GDC-0214) [214]. Another strategy to inhibit or deplete mast cells is the use of mAb targeting Siglec-8 (lirentelimab, also known as AK002) (NCT03379311; NCT03436797; NCT04322708) or Siglec-6 (OK006) [215].
Figure 4.
Schematic representation of mast cell-targeted biologics and drugs approved, under development, or potentially useful for asthma treatment. Several immunological stimuli (allergens, super allergens, bacterial, fungal, and viral products, smoke extracts) can damage bronchial epithelial cells to release alarmins, such as thymic stromal lymphopoietin (TSLP) [187,196], IL-33 [196,197], and IL-25 [196,198,199]. Monoclonal antibodies (mAbs) targeting TSLP (tezepelumab) [188,189], IL-33 (etokimab, itepekimab, tozorakimab) [200,201] (NCT04570657), or the IL-33 receptor ST2 (astegolimab) [202], have been approved or are under investigation for asthma treatment. mAbs targeting IL-5, produced by human mast cells [203], such as mepolizumab [204,205,206,207], reslizumab [208,209], or its receptor IL-5Rα (benralizumab) [175,210,211], have been approved for the treatment of eosinophilic asthma. Dupilumab blocks IL-4Rα and is approved for severe asthma [169,170,171]. Omalizumab was the first mAb approved for asthma treatment [212]. Novel mAbs anti-IgE (ligelizumab, UB-221, GI-301, UCB-8600) are under investigation for allergic disorder treatment [213] (NCT05298215; NTC04444466). Other strategies to treat mast cell-driven disease include inhibitors of spleen tyrosine kinase (SYK) (GSK2646264), Bruton’s tyrosine kinase (BTK) (acalabrutinib, fenebrutinib, ibrutinib, remibrutinib), and Janus kinase (JAK) inhibitors (GDC-0214) [214]. Another strategy to inhibit or deplete mast cells is the use of mAb targeting Siglec-8 (lirentelimab, also known as AK002) (NCT03379311; NCT03436797; NCT04322708) or Siglec-6 (OK006) [215].

Figure 5.
Schematic representation of two different strategies to deplete mast cells. Several classes of KIT-associated tyrosine kinase inhibitors (TKIs) are now available [16,260,261]. Preliminary evidence indicates that prolonged administration of imatinib [262] and masitinib [263,264] can influence airway hyperresponsiveness or reduce asthma exacerbations in asthma patients. These beneficial effects have been tentatively attributed to the inhibition of mast cell activation and/or depletion of mast cells. Another approach to induce mast cell apoptosis is through blockage of SCF-KIT interaction. CDX-0159 is a mAb that targets the extracellular dimerization domain of KIT [258,259] and causes a marked reduction of peripheral blood tryptase, suggesting systemic mast cell depletion (NCT04146129).
Figure 5.
Schematic representation of two different strategies to deplete mast cells. Several classes of KIT-associated tyrosine kinase inhibitors (TKIs) are now available [16,260,261]. Preliminary evidence indicates that prolonged administration of imatinib [262] and masitinib [263,264] can influence airway hyperresponsiveness or reduce asthma exacerbations in asthma patients. These beneficial effects have been tentatively attributed to the inhibition of mast cell activation and/or depletion of mast cells. Another approach to induce mast cell apoptosis is through blockage of SCF-KIT interaction. CDX-0159 is a mAb that targets the extracellular dimerization domain of KIT [258,259] and causes a marked reduction of peripheral blood tryptase, suggesting systemic mast cell depletion (NCT04146129).


{kind=link}
{kind=link}
{kind=link}
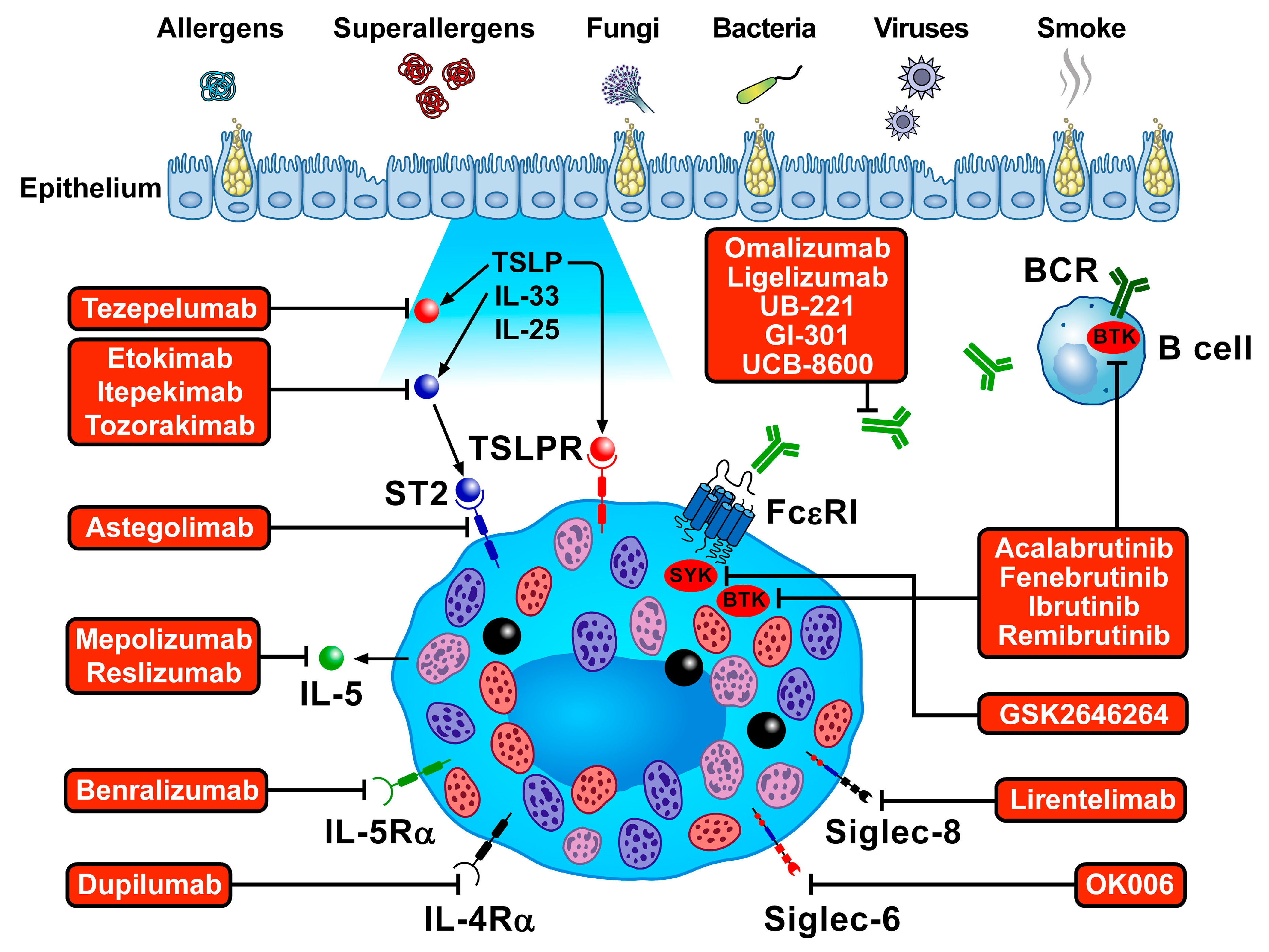{kind=link}
{kind=link}
Table 1.
Preformed and Newly Synthesized Mediators Released by Human Lung Mast Cells.
| Mediator | Properties | References |
|---|---|---|
| Preformed | ||
| Histamine | Preformed in cytoplasmic granules of human mast cells (≅3 pg/cell) and basophils (≅1 pg/cell). | [64,65] |
| β-tryptase | A tetrameric serine protease, abundant in secretory granules of human mast cells. Tryptase+ mast cells are increased in asthmatics bronchial tissue, and their numbers correlate with airway hyperresponsiveness. Tryptase concentrations in bronchoalveolar lavage (BAL) fluid correlates with asthma severity. | [89,90,91,92] |
| Chymase | A chymotrypsin-like serine protease stored in human mast cell secretory granules causes matrix destruction and inflammation. | [93,94] |
| Cathepsin G | A serine protease that controls the functional state of immune cells. | [93] |
| Carboxypeptidase A3 | It cleaves several proteins. | [95] |
| Granzyme B | A protease involved in the induction of target cell death. | [96] |
| Matrix metalloproteinases (MMPs) | A family of extracellular proteinases. | [97] |
| Lipid Mediators | ||
| Cysteinyl leukotriene C4 (LTC4) | Human lung mast cells (HLMCs) synthesize LTC4, a potent bronchoconstrictor acting through the activation of cysteinyl leukotriene receptor 1 (CysLTR1) and CysLTR2. | [98,99] |
| Prostaglandin D2 (PGD2) | It activates the CRTh2 receptor on several immune cells. | [100,101] |
| Platelet-activating factor (PAF) | A phospholipid with proinflammatory and vasoactive effects. | [102] |
| Cytokines | ||
| Stem cell factor (SCF) | They exert several proinflammatory and immunomodulatory effects. | [37] |
| TNF-α | [103] | |
| IL-1β | [104] | |
| IL-3 | [105,106] | |
| IL-5 | [107] | |
| IL-6 | [108] | |
| IL-9 | [109] | |
| IL-10 | [57] | |
| IL-11 | [108] | |
| IL-13 | [109,110] | |
| IL-16 | [111] | |
| IL-22 | [112] | |
| Thymic stromal lymphopoietin (TSLP) | [113,114,115] | |
| IL-25/IL-17E | [116] | |
| Granulocyte-macrophage colony-stimulating factor (GM-CSF) | [107] | |
| Vascular endothelial growth factor (VEGF) | [117] | |
| Fibroblast growth factor 2 (FGF-2) | [118] | |
| Nerve growth factor (NGF) | [119] | |
| Amphiregulin | [120,121] | |
| Chemokines | ||
| CXCL8/IL-8, CCL1/I-309, CCL2/MCP-1, CCL3/MIP-1α, CXCL1/GRO-α, CXCL10/IP-10 | They exert several chemotactic and proinflammatory effects. | [122,123,124] |
| Angiogenic factors | ||
| VEGF-A | The main angiogenic factor released by HLMCs. VEGFs released by macrophages, basophils, and neutrophils contribute to mast cell infiltration in bronchial asthma. | [56,117,125,126,127,128] |
| Angiopoietins (ANGPT1 and ANGPT2) | ANGPTs are involved in blood vessel formation and are released by HLMCs. | [129,130,131,132] |
| LTC4, LTD4 | Non-canonical angiogenic factors. | [133] |
| Lymphangiogenic factors | ||
| VEGF-C, VEGF-D | The main lymphangiogenic factor released by HLMCs. | [58] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Poto, R.; Criscuolo, G.; Marone, G.; Brightling, C.E.; Varricchi, G. Human Lung Mast Cells: Therapeutic Implications in Asthma. Int. J. Mol. Sci. 2022, 23, 14466. https://doi.org/10.3390/ijms232214466
AMA Style
Poto R, Criscuolo G, Marone G, Brightling CE, Varricchi G. Human Lung Mast Cells: Therapeutic Implications in Asthma. International Journal of Molecular Sciences. 2022; 23(22):14466. https://doi.org/10.3390/ijms232214466
Chicago/Turabian StylePoto, Remo, Gjada Criscuolo, Gianni Marone, Chris E. Brightling, and Gilda Varricchi. 2022. "Human Lung Mast Cells: Therapeutic Implications in Asthma" International Journal of Molecular Sciences 23, no. 22: 14466. https://doi.org/10.3390/ijms232214466
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.