
The Effect of Microcosm Biofilm Decontamination on Surface Topography, Chemistry, and Biocompatibility Dynamics of Implant Titanium Surfaces
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Viable Biofilm Quantification
2.1.1. Machined Ti Surfaces
2.1.2. SLA Ti Surfaces
2.2. Surface Topography, Wettability, Chemistry and Biocompatibility
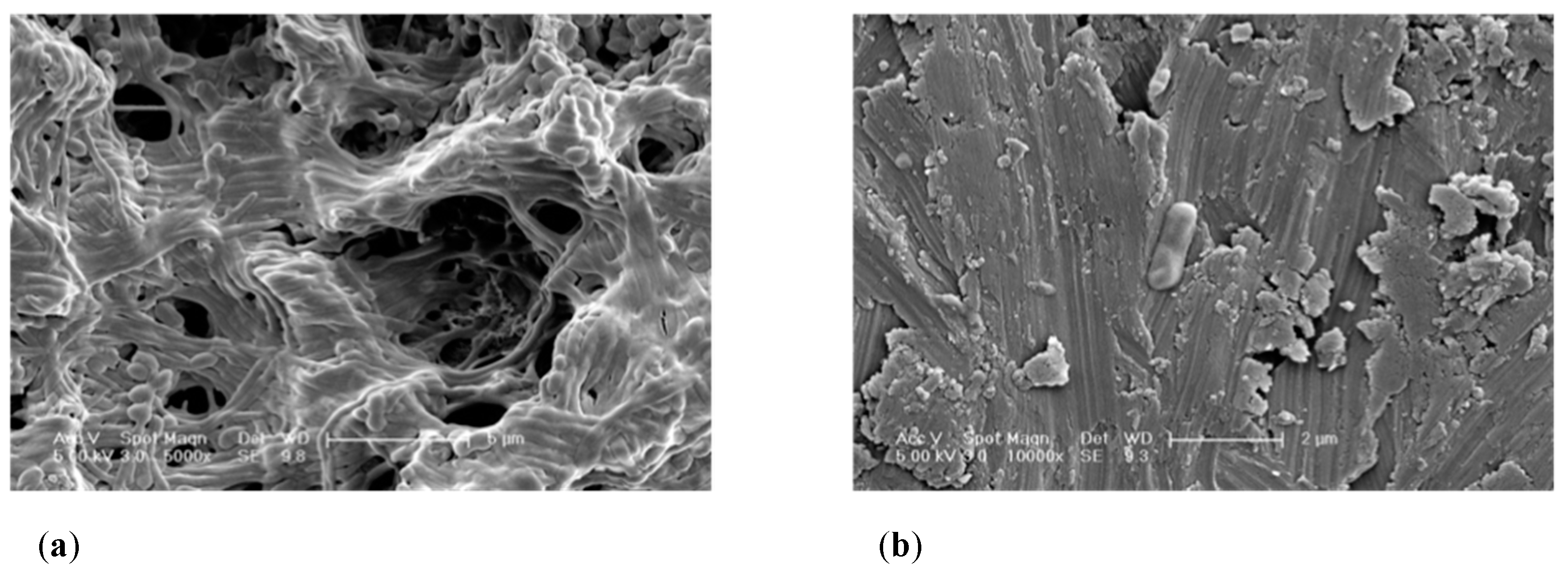
2.2.1. SEM Imaging Ti Surfaces before and after Decontamination
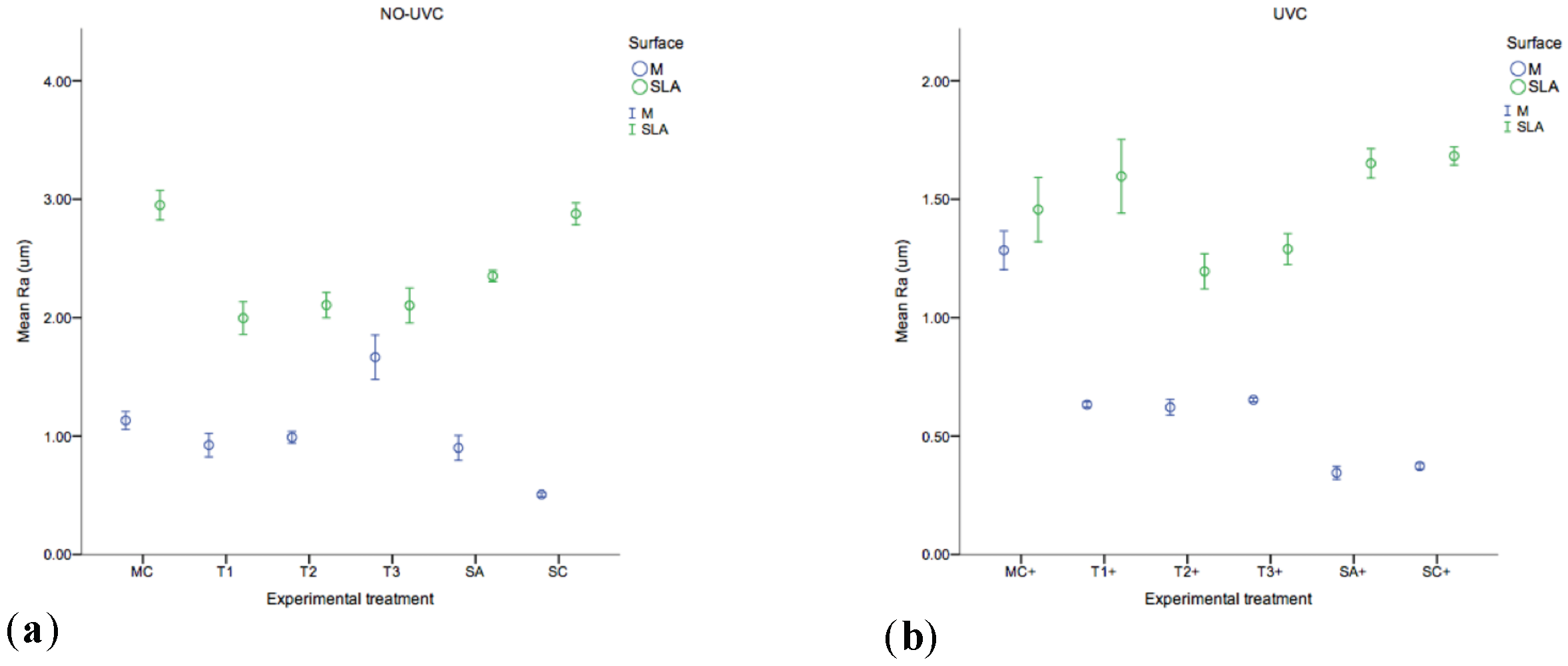
2.2.2. Surface Roughness
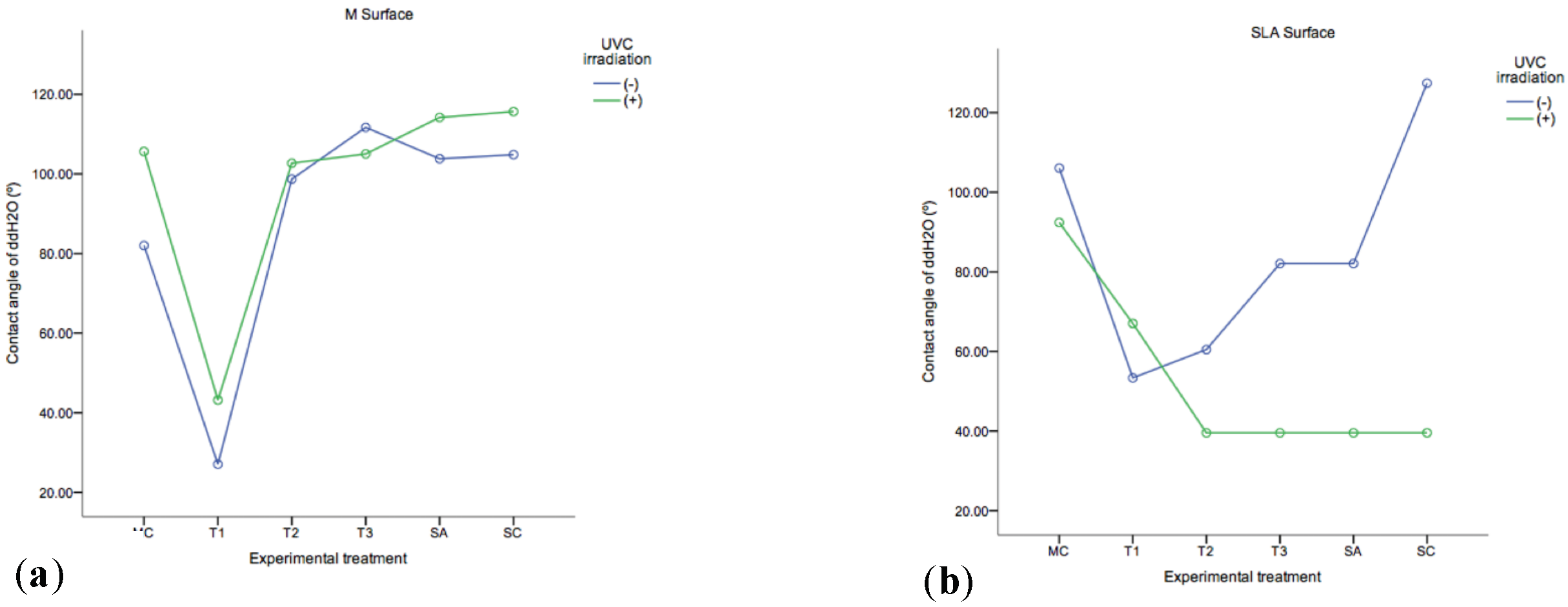
2.2.3. ddH2O Contact Angles
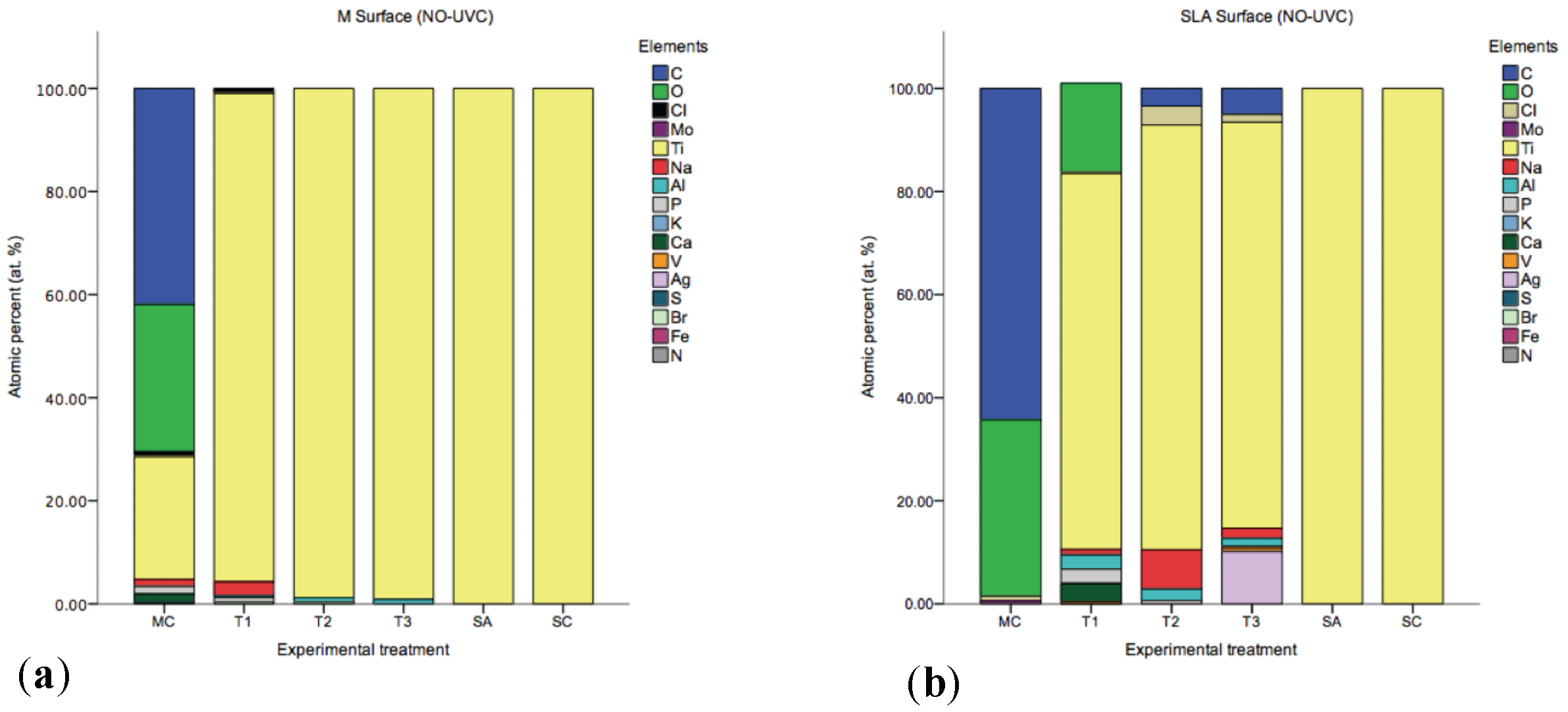
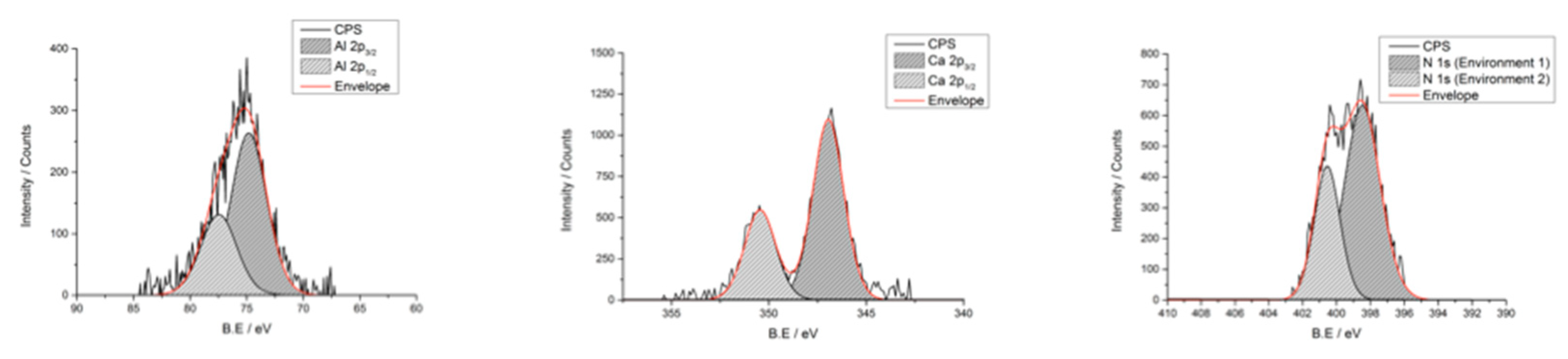
2.2.4. Surface Chemistry
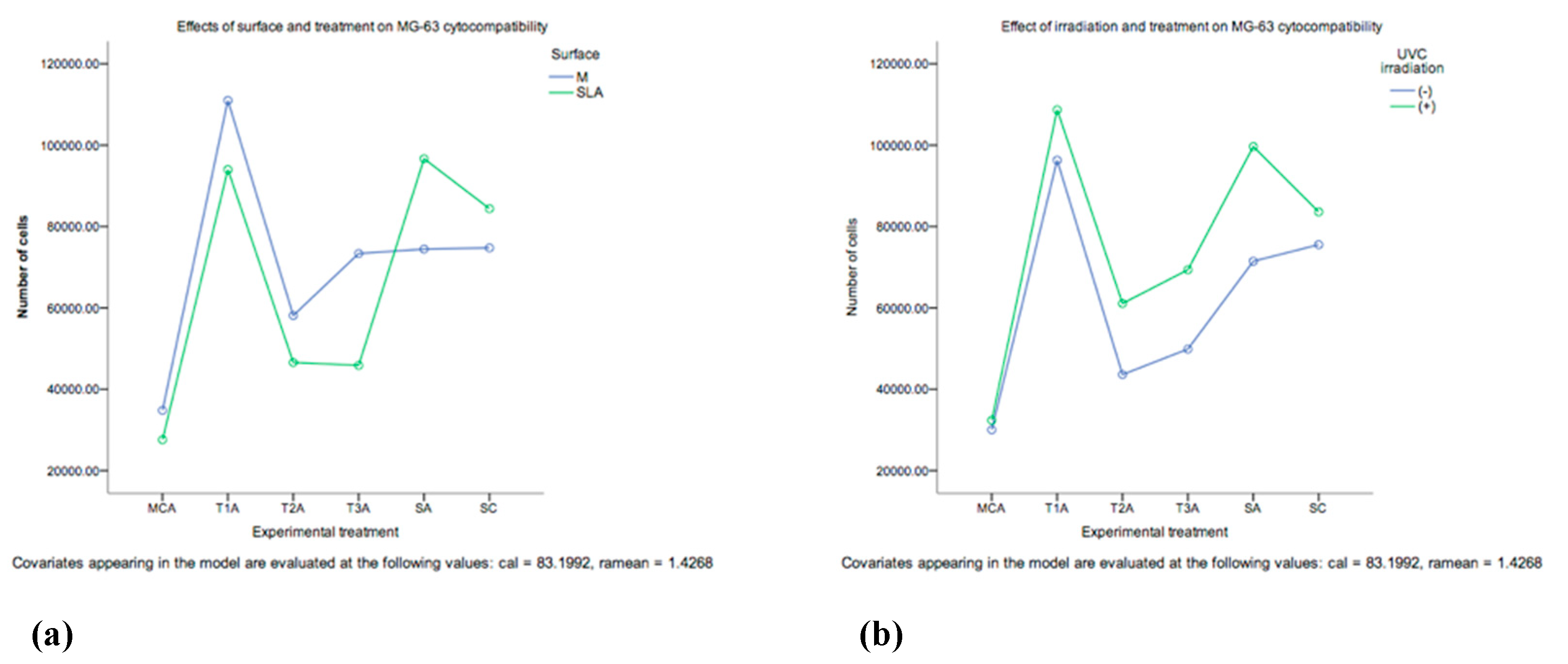
2.2.5. Cytocompatibility of Decontaminated Ti Surfaces
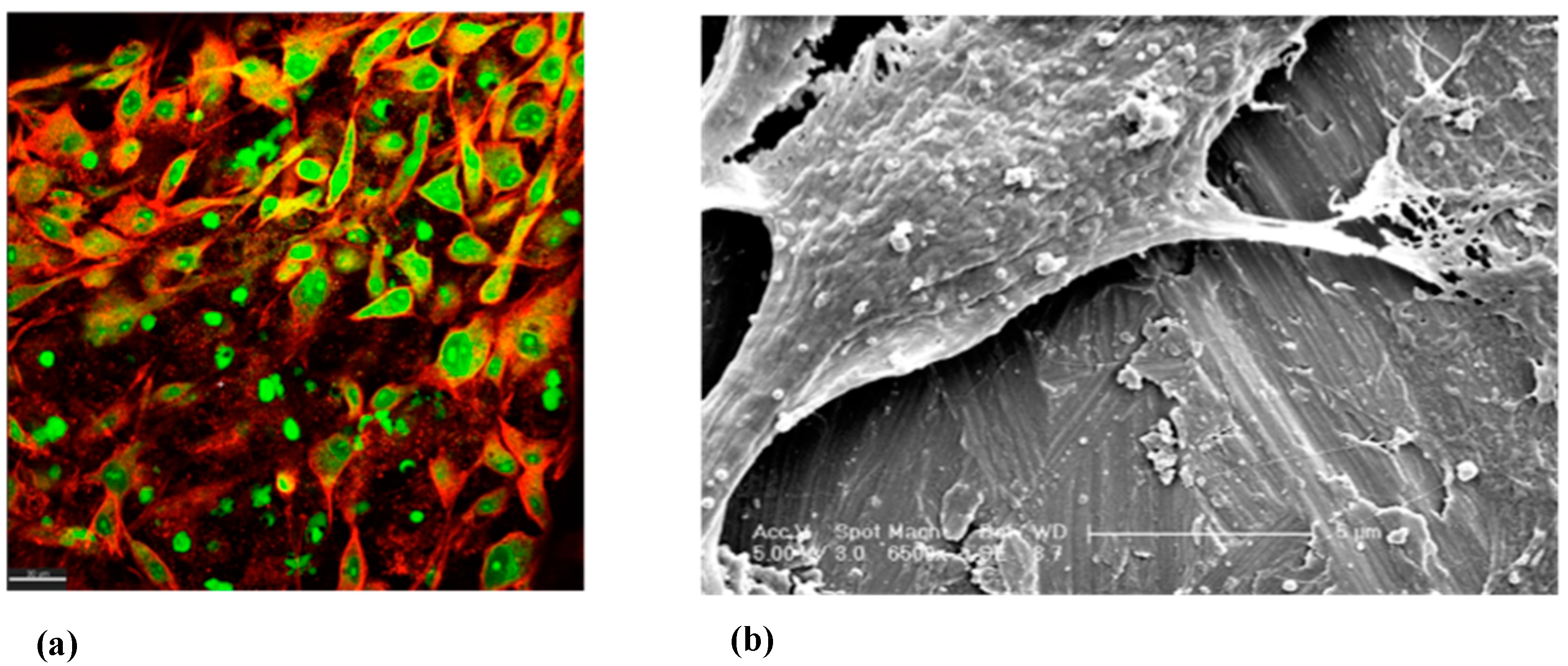
2.2.6. SEM and CLSM Imaging of MG-63
3. Discussion
3.1. Viable Biofilm Quantification
3.2. Surface Topography, Wettability, Chemistry and Biocompatibility
3.2.1. SEM Imaging and Surface Roughness of Ti Surfaces before and after Decontamination
3.2.2. ddH2O Contact Angles
3.2.3. Surface Chemistry
3.2.4. Cytocompatibility of Decontamination Ti Surfaces
3.2.5. SEM and CLSM Imaging of MG-63
4. Materials and Methods
4.1. Microcosm Biofilm Growth
4.2. Microcosm Biofilm Disruption
4.2.1. T1: Mechanical Disruption with Ti Brush
4.2.2. T2: TiB + Photodynamic Therapy
4.2.3. T3: TiB + Chemical Agents
4.2.4. MC+, SC+, SA+, T1+, T2+, T3+: Ultraviolet Irradiation C
4.3. Effect of Therapies on Viable Cell Counts
4.4. Effect of Therapies on Surface Topography, Wettability, Chemistry and Biocompatibility
4.5. Statistical Analyses
5. Conclusions
- Bacterial debris will prevail after mechanical and combination therapy.
- Photofunctionalisation of the Ti surface with Ultraviolet-C (UV-C) radiation appears to have a positive effect in the Ti surface biocompatibility. MG-63 cell proliferation was enhanced by photofunctionalisation of the Ti surface by the use of UV-C irradiation, time, type of treatment and type of surface. The outcomes of this cytocompatibility study favours decontamination of smooth surfaces, and photofunctionalisation of the TiO2 layer.
- All decontamination protocols induced modifications of the Ti oxide layer surface properties. Therefore, it is plausible to focus future research on developing decontamination protocols that facilitate the re-establishment of a biocompatible state of the implant surface chemistry.
- Successful treatment for peri-implantitis should integrate a comprehensive approach, including not only the elimination of live bacteria, but also the bacterial debris, and taking into account the Ti surface biomaterial alterations, re-contamination of implant surfaces, and host interactions. Therefore, decontamination protocols for titanium (Ti) surfaces should be carefully chosen by the clinician.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral. Implant. Res. 2009, 20 (Suppl. 4), 172–184. [Google Scholar] [CrossRef] [PubMed]
- Elani, H.W.; Starr, J.R.; Da Silva, J.D.; Gallucci, G.O. Trends in Dental Implant Use in the U.S., 1999–2016, and Projections to 2026. J. Dent. Res. 2018, 97, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S158–S171. [Google Scholar] [CrossRef] [PubMed]
- Klinge, B.; Meyle, J. Peri-implant tissue destruction. The Third EAO Consensus Conference 2012. Clin. Oral. Implant. Res. 2012, 23 (Suppl. S6), 108–110. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S286–S291. [Google Scholar] [CrossRef]
- Sousa, V.; Mardas, N.; Spratt, D.; Boniface, D.; Dard, M.; Donos, N. Experimental models for contamination of titanium surfaces and disinfection protocols. Clin. Oral. Implants Res. 2016, 27, 1233–1242. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Bertl, K.; Eren, S.; Gotfredsen, K. Mechanical and biological complications after implantoplasty-A systematic review. Clin. Oral. Implants Res. 2019, 30, 833–848. [Google Scholar] [CrossRef]
- Roccuzzo, A.; Stähli, A.; Monje, A.; Sculean, A.; Salvi, G.E. Peri-Implantitis: A Clinical Update on Prevalence and Surgical Treatment Outcomes. J. Clin. Med. 2021, 10, 1107. [Google Scholar] [CrossRef]
- Schwarz, F.; Alcoforado, G.; Guerrero, A.; Jönsson, D.; Klinge, B.; Lang, N.; Mattheos, N.; Mertens, B.; Pitta, J.; Ramanauskaite, A.; et al. Peri-implantitis: Summary and consensus statements of group 3. The 6th EAO Consensus Conference 2021. Clin. Oral. Implants Res. 2021, 32 (Suppl. 21), 245–253. [Google Scholar] [CrossRef]
- Mattheos, N.; Janda, M.; Acharya, A.; Pekarski, S.; Larsson, C. Impact of design elements of the implant supracrestal complex (ISC) on the risk of peri-implant mucositis and peri-implantitis: A critical review. Clin. Oral. Implant Res. 2021, 32 (Suppl. 21), 181–202. [Google Scholar] [CrossRef]
- Sanz-Martín, I.; Cha, J.-K.; Sanz-Sánchez, I.; Figuero, E.; Herrera, D.; Sanz, M. Changes in peri-implant soft tissue levels following surgical treatment of peri-implantitis: A systematic review and meta-analysis. Clin. Oral. Implants Res. 2021, 32 (Suppl. 21), 230–244. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Chapple, I.L. Clinical research on peri-implant diseases: Consensus report of Working Group 4. J. Clin. Periodontol. 2012, 39 (Suppl. 12), 202–206. [Google Scholar] [CrossRef] [PubMed]
- Pouponneau, P.; Perrey, O.; Brunon, C.; Grossiord, C.; Courtois, N.; Salles, V.; Alves, A. Electrospun Bioresorbable Membrane Eluting Chlorhexidine for Dental Implants. Polymers 2020, 12, 66. [Google Scholar] [CrossRef] [PubMed]
- Belibasakis, G.N.; Charalampakis, G.; Bostanci, N.; Stadlinger, B. Peri-Implant Infections of Oral Biofilm Etiology. In Advances in Experimental Medicine and Biology; Donelli, G., Ed.; Springer: Cham, Switzerland, 2015; Volume 830. [Google Scholar]
- Berglundh, T.; Abrahamsson, I.; Lang, N.P.; Lindhe, J. De novo alveolar bone formation adjacent to endosseous implants. Clin. Oral. Implants Res. 2003, 14, 251–262. [Google Scholar] [CrossRef]
- Sykaras, N.; Iacopino, A.M.; Marker, V.A.; Triplett, R.G.; Woody, R.D. Implant materials, designs, and surface topographies: Their effect on osseointegration. A literature review. Int. J. Oral Maxillofac. Implant. 2000, 15, 675–690. [Google Scholar]
- Berglundh, T.; Gotfredsen, K.; Zitzmann, N.U.; Lang, N.P.; Lindhe, J. Spontaneous progression of ligature induced peri-implantitis at implants with different surface roughness: An experimental study in dogs. Clin. Oral. Implants Res. 2007, 18, 655–661. [Google Scholar] [CrossRef]
- Albouy, J.-P.; Abrahamsson, I.; Persson, L.G.; Berglundh, T. Spontaneous progression of peri-implantitis at different types of implants. An experimental study in dogs. I: Clinical and radiographic observations. Clin. Oral. Implants Res. 2008, 19, 997–1002. [Google Scholar] [CrossRef]
- Renvert, S.; Polyzois, I.; Claffey, N. How do implant surface characteristics influence peri-implant disease? J. Clin. Periodontol. 2011, 38 (Suppl. 11), 214–222. [Google Scholar] [CrossRef]
- Cecchinato, D.; Parpaiola, A.; Lindhe, J. Mucosal inflammation and incidence of crestal bone loss among implant patients: A 10-year study. Clin. Oral. Implants Res. 2014, 25, 791–796. [Google Scholar] [CrossRef]
- Derks, J.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Larsson, M.; Berglundh, T. Effectiveness of implant therapy analyzed in a Swedish population: Early and late implant loss. J. Dent. Res. 2015, 94, 44S–51S. [Google Scholar] [CrossRef]
- Carcuac, O.; Derks, J.; Abrahamsson, I.; Wennström, J.L.; Petzold, M.; Berglundh, T. Surgical treatment of peri-implantitis: 3-year results from a randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 1294–1303. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Sculean, A.; Romanos, G.; Herten, M.; Horn, N.; Scherbaum, W.; Becker, J. Influence of different treatment approaches on the removal of early plaque biofilms and the viability of SAOS2 osteoblasts grown on titanium implants. Clin. Oral. Investig. 2005, 9, 111–117. [Google Scholar] [CrossRef]
- John, G.; Becker, J.; Schwarz, F. Rotating titanium brush for plaque removal from rough titanium surfaces--an in vitro study. Clin. Oral. Implants Res. 2014, 25, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A.; Mombelli, A. The therapy of peri-implantitis: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 325–345. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Sahm, N.; Iglhaut, G.; Becker, J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: A randomized controlled clinical study. J. Clin. Periodontol. 2011, 38, 276–284. [Google Scholar] [CrossRef]
- Gittens, R.A.; Olivares-Navarrete, R.; Schwartz, Z.; Boyan, B.D. Implant osseointegration and the role of microroughness and nanostructures: Lessons for spine implants. Acta Biomater. 2014, 10, 3363–3371. [Google Scholar] [CrossRef]
- Gittens, R.A.; Scheideler, L.; Rupp, F.; Hyzy, S.L.; Geis-Gerstorfer, J.; Schwartz, Z.; Boyan, B.D. A review on the wettability of dental implant surfaces II: Biological and clinical aspects. Acta Biomater. 2014, 10, 2907–2918. [Google Scholar] [CrossRef]
- Gittens, R.A.; McLachlan, T.; Olivares-Navarrete, R.; Cai, Y.; Berner, S.; Tannenbaum, R.; Schwartz, Z.; Sandhage, K.H.; Boyan, B.D. The effects of combined micron-/submicron-scale surface roughness and nanoscale features on cell proliferation and differentiation. Biomaterials 2011, 32, 3395–3403. [Google Scholar] [CrossRef]
- Gittens, R.A.; Olivares-Navarrete, R.; Tannenbaum, R.; Boyan, B.D.; Schwartz, Z. Electrical implications of corrosion for osseointegration of titanium implants. J. Dent. Res. 2011, 90, 1389–1397. [Google Scholar] [CrossRef]
- Khoury, F.; Keeve, P.L.; Ramanauskaite, A.; Schwarz, F.; Koo, K.-T.; Sculean, A.; Romanos, G. Surgical treatment of peri-implantitis—Consensus report of working group 4. Int. Dent. J. 2019, 69 (Suppl. 2), 18–22. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Bertl, K.; Winning, L.; Polyzois, I. What is the influence of implant surface characteristics and/or implant material on the incidence and progression of peri-implantitis? A systematic literature review. Clin. Oral. Implants Res. 2021, 32 (Suppl. 21), 203–229. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Derks, J.; Abrahamsson, I.; Wennström, J.L.; Berglundh, T. Risk for recurrence of disease following surgical therapy of peri-implantitis-A prospective longitudinal study. Clin. Oral. Implants Res. 2020, 31, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Widodo, A.; Spratt, D.; Sousa, V.; Petrie, A.; Donos, N. An in vitro study on disinfection of titanium surfaces. Clin. Oral. Implants Res. 2016, 27, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Fürst, M.M.; Lang, N.P.; Persson, G.R. One-year bacterial colonization patterns of Staphylococcus aureus and other bacteria at implants and adjacent teeth. Clin. Oral. Implants Res. 2008, 19, 242–248. [Google Scholar] [CrossRef]
- Persson, G.R.; Renvert, S. Cluster of bacteria associated with peri-implantitis. Clin. Implant. Dent. Relat. Res. 2014, 16, 783–793. [Google Scholar] [CrossRef]
- Charalampakis, G.; Rabe, P.; Leonhardt, Å.; Dahlén, G. A follow-up study of peri-implantitis cases after treatment. J. Clin. Periodontol. 2011, 38, 864–871. [Google Scholar] [CrossRef]
- Schwarz, F.; Papanicolau, P.; Rothamel, D.; Beck, B.; Herten, M.; Becker, J. Influence of plaque biofilm removal on reestablishment of the biocompatibility of contaminated titanium surfaces. J. Biomed. Mater. Res. Part A 2006, 77, 437–444. [Google Scholar] [CrossRef]
- Ghasemi, M.; Etemadi, A.; Nedaei, M.; Chiniforush, N.; Pourhajibagher, M. Antimicrobial Efficacy of Photodynamic Therapy Using Two Different Light Sources on the Titanium-Adherent Biofilms of Aggregatibacter actinomycetemcomitans: An in vitro study. Photodiagnosis Photodyn. Ther. 2019, 26, 85–89. [Google Scholar] [CrossRef]
- Leelanarathiwat, K.; Katsuta, Y.; Katsuragi, H.; Watanabe, F. Antibacterial activity of blue high-power light-emitting diode-activated flavin mononucleotide against Staphylococcus aureus biofilm on a sandblasted and etched surface. Photodiagnosis Photodyn. Ther. 2020, 31, 101855. [Google Scholar] [CrossRef]
- Wennerberg, A.; Albrektsson, T. Suggested guidelines for the topographic evaluation of implant surfaces. Int. J. Oral Maxillofac. Implant. 2000, 15, 331–344. [Google Scholar]
- Toma, S.; Brecx, M.C.; Lasserre, J.F. Clinical Evaluation of Three Surgical Modalities in the Treatment of Peri-Implantitis: A Randomized Controlled Clinical Trial. J. Clin. Med. 2019, 8, 966. [Google Scholar] [CrossRef] [PubMed]
- Ramel, C.F.; Lüssi, A.; Özcan, M.; Jung, R.E.; Hämmerle, C.H.F.; Thoma, D.S. Surface roughness of dental implants and treatment time using six different implantoplasty procedures. Clin. Oral. Implants Res. 2016, 27, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Teughels, W.; Van Assche, N.; Sliepen, I.; Quirynen, M. Effect of material characteristics and/or surface topography on biofilm development. Clin. Oral. Implants Res. 2006, 17 (Suppl. 2), 68–81. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Bollen, C.M. The influence of surface roughness and surface-free energy on supra- and subgingival plaque formation in man. A review of the literature. J. Clin. Periodontol. 1995, 22, 1–14. [Google Scholar] [CrossRef]
- Meier, R.M.; Pfammatter, C.; Zitzmann, N.U.; Filippi, A.; Kühl, S. Surface quality after implantoplasty. Schweiz. Monatsschr. Zahnmed. 2012, 122, 714–724. [Google Scholar] [PubMed]
- Barrak, F.N.; Li, S.; Muntane, A.M.; Jones, J.R. Particle release from implantoplasty of dental implants and impact on cells. Int. J. Implant. Dent. 2020, 6, 50. [Google Scholar] [CrossRef]
- Aita, H.; Hori, N.; Takeuchi, M.; Suzuki, T.; Yamada, M.; Anpo, M.; Ogawa, T. The effect of ultraviolet functionalization of titanium on integration with bone. Biomaterials 2009, 30, 1015–1025. [Google Scholar] [CrossRef]
- Ueno, T.; Yamada, M.; Suzuki, T.; Minamikawa, H.; Sato, N.; Hori, N.; Takeuchi, K.; Hattori, M.; Ogawa, T. Enhancement of bone-titanium integration profile with UV-photofunctionalized titanium in a gap healing model. Biomaterials 2010, 31, 1546–1557. [Google Scholar] [CrossRef]
- Park, J.H.; Olivares-Navarrete, R.; Baier, R.E.; Meyer, A.E.; Tannenbaum, R.; Boyan, B.D.; Schwartz, Z. Effect of cleaning and sterilization on titanium implant surface properties and cellular response. Acta Biomater. 2012, 8, 1966–1975. [Google Scholar] [CrossRef]
- Park, K.-H.; Koak, J.-Y.; Kim, S.-K.; Han, C.-H.; Heo, S.-J. The effect of ultraviolet-C irradiation via a bactericidal ultraviolet sterilizer on an anodized titanium implant: A study in rabbits. Int. J. Oral Maxillofac. Implant. 2013, 28, 57–66. [Google Scholar] [CrossRef]
- Menetrez, M.Y.; Foarde, K.K.; Dean, T.R.; Betancourt, D.A. The effectiveness of UV irradiation on vegetative bacteria and fungi surface contamination. Chem. Eng. 2010, 157, 443–450. [Google Scholar] [CrossRef]
- Gallardo-Moreno, A.M.; Pacha-Olivenza, M.A.; Fernández-Calderón, M.-C.; Pérez-Giraldo, C.; Bruque, J.M.; González-Martín, M.-L. Bactericidal behaviour of Ti6Al4V surfaces after exposure to UV-C light. Biomaterials 2010, 31, 5159–5168. [Google Scholar] [CrossRef] [PubMed]
- Logan, N.; Cross, A.J.; Traynor, A.; Bozec, L.; Parkin, I.P.; Brett, P. Mesenchymal stem cell response to UV-photofunctionalized TiO2 coated CoCrMo. RSC Adv. 2014, 4, 59847–59857. [Google Scholar] [CrossRef]
- Toma, S.; Lasserre, J.; Brecx, M.C.; Nyssen-Behets, C. In vitro evaluation of peri-implantitis treatment modalities on Saos-2osteoblasts. Clin. Oral. Implants Res. 2016, 27, 1085–1092. [Google Scholar] [CrossRef]
- Steinemann, S.G. Titanium—the material of choice? Periodontol. 2000 1998, 17, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Subramani, K.; Wismeijer, D. Decontamination of titanium implant surface and re-osseointegration to treat peri-implantitis: A literature review. Int. J. Oral Maxillofac. Implant. 2012, 27, 1043–1054. [Google Scholar] [PubMed]
- Brett, P.M.; Harle, J.; Salih, V.; Mihoc, R.; Olsen, I.; Jones, F.H.; Tonetti, M. Roughness response genes in osteoblasts. Bone 2004, 35, 124–133. [Google Scholar] [CrossRef]
- Anselme, K.; Bigerelle, M. Statistical demonstration of the relative effect of surface chemistry and roughness on human osteoblast short-term adhesion. J. Mater. Sci. Mater. Med. 2006, 17, 471–479. [Google Scholar] [CrossRef]
- Schwarz, F.; Sculean, A.; Wieland, M.; Horn, N.; Nuesry, E.; Bube, C.; Becker, J. Effects of hydrophilicity and microtopography of titanium implant surfaces on initial supragingival plaque biofilm formation. A pilot study. Mund Kiefer Gesichtschir. 2007, 11, 333–338. [Google Scholar] [CrossRef]
- Zhao, G.; Zinger, O.; Schwartz, Z.; Wieland, M.; Landolt, D.; Boyan, B.D. Osteoblast-like cells are sensitive to submicron-scale surface structure. Clin. Oral. Implants Res. 2006, 17, 258–264. [Google Scholar] [CrossRef]
- Machnee, C.H.; Wagner, W.C.; Jaarda, M.J.; Lang, B.R. Identification of oxide layers of commercially pure titanium in response to cleaning procedures. Int. J. Oral Maxillofac. Implant. 1993, 8, 529–533. [Google Scholar] [PubMed]
- Tubby, S.; Wilson, M.; Nair, S.P. Inactivation of staphylococcal virulence factors using a light-activated antimicrobial agent. BMC Microbiol. 2009, 9, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weenk, G.H. Microbiological assessment of culture media: Comparison and statistical evaluation of methods. Int. J. Food Microbiol. 1992, 17, 159–181. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Groups * | Experimental Surface Disinfection Protocols * ^ a | ||
|---|---|---|---|
| Biofilm (MC) a | TiB (T1) | Irradiation c | TiB+ (T1+) |
| Sterile (SC) | TiB+PDT (T2) | TiB+PDT+ (T2+) | |
| Sterile autoclaved (SA) | TiB+CA (T3) | TiB+CA+ (T3+) | |
| Biofilm+ (MC+) | |||
| SA+ (SA+) | |||
| SC+ (SC+) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousa, V.; Mardas, N.; Spratt, D.; Hassan, I.A.; Walters, N.J.; Beltrán, V.; Donos, N. The Effect of Microcosm Biofilm Decontamination on Surface Topography, Chemistry, and Biocompatibility Dynamics of Implant Titanium Surfaces. Int. J. Mol. Sci. 2022, 23, 10033. https://doi.org/10.3390/ijms231710033
Sousa V, Mardas N, Spratt D, Hassan IA, Walters NJ, Beltrán V, Donos N. The Effect of Microcosm Biofilm Decontamination on Surface Topography, Chemistry, and Biocompatibility Dynamics of Implant Titanium Surfaces. International Journal of Molecular Sciences. 2022; 23(17):10033. https://doi.org/10.3390/ijms231710033
Chicago/Turabian StyleSousa, Vanessa, Nikos Mardas, Dave Spratt, Iman A. Hassan, Nick J. Walters, Víctor Beltrán, and Nikolaos Donos. 2022. "The Effect of Microcosm Biofilm Decontamination on Surface Topography, Chemistry, and Biocompatibility Dynamics of Implant Titanium Surfaces" International Journal of Molecular Sciences 23, no. 17: 10033. https://doi.org/10.3390/ijms231710033