
Comparison of the Therapeutic Effects of [211At]NaAt and [131I]NaI in an NIS-Expressing Thyroid Cancer Mouse Model

 , , , , , ,
, , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
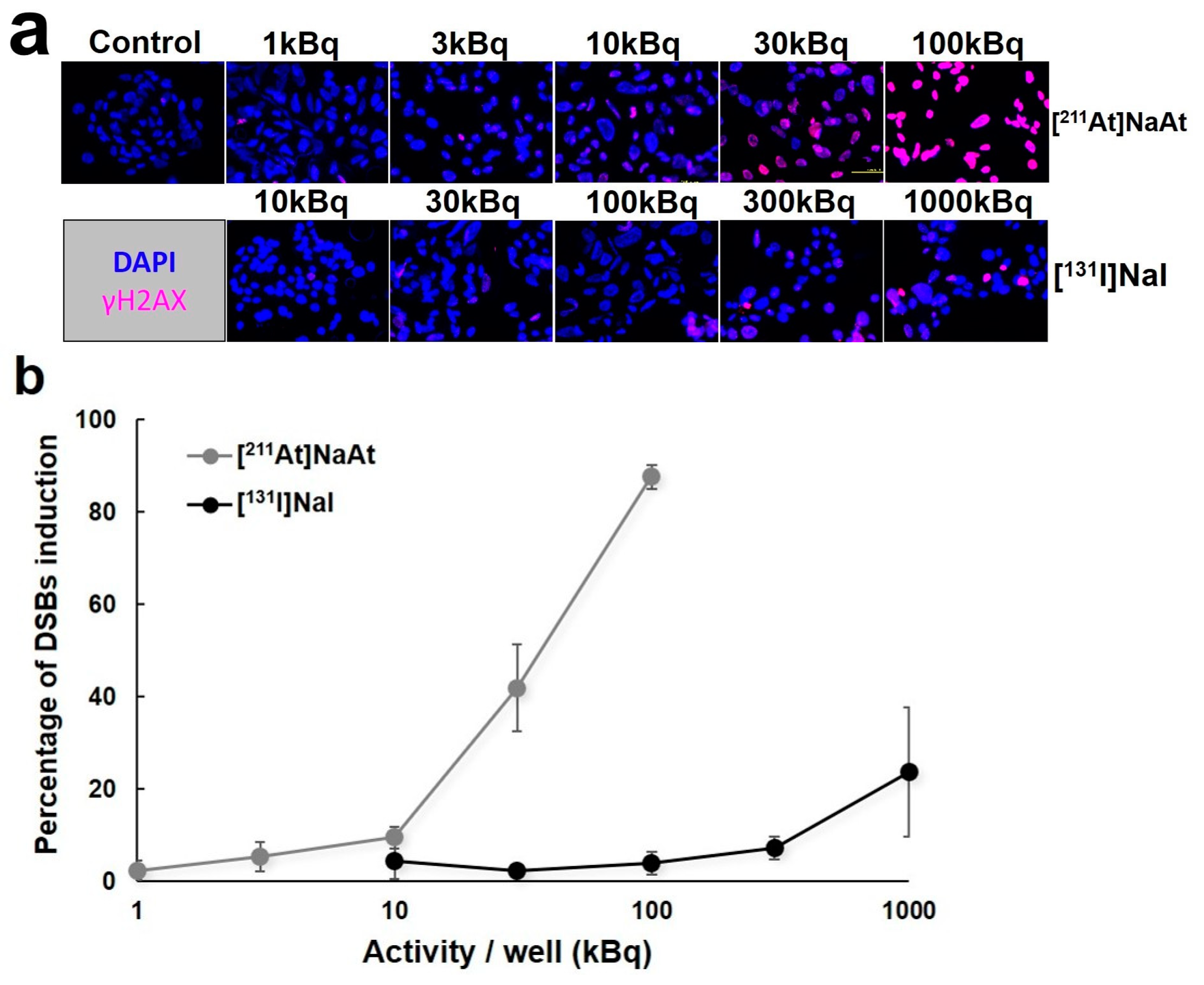
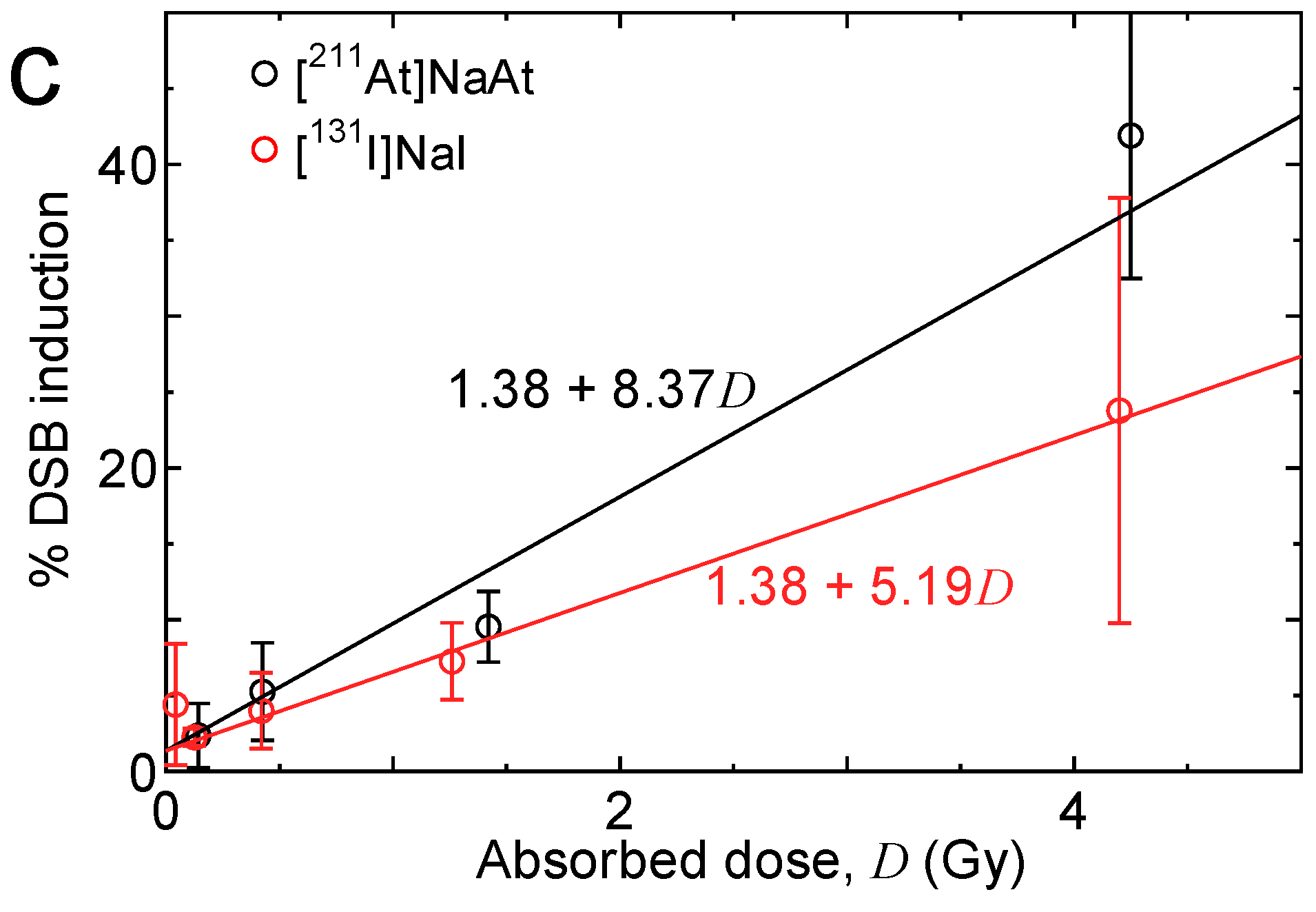
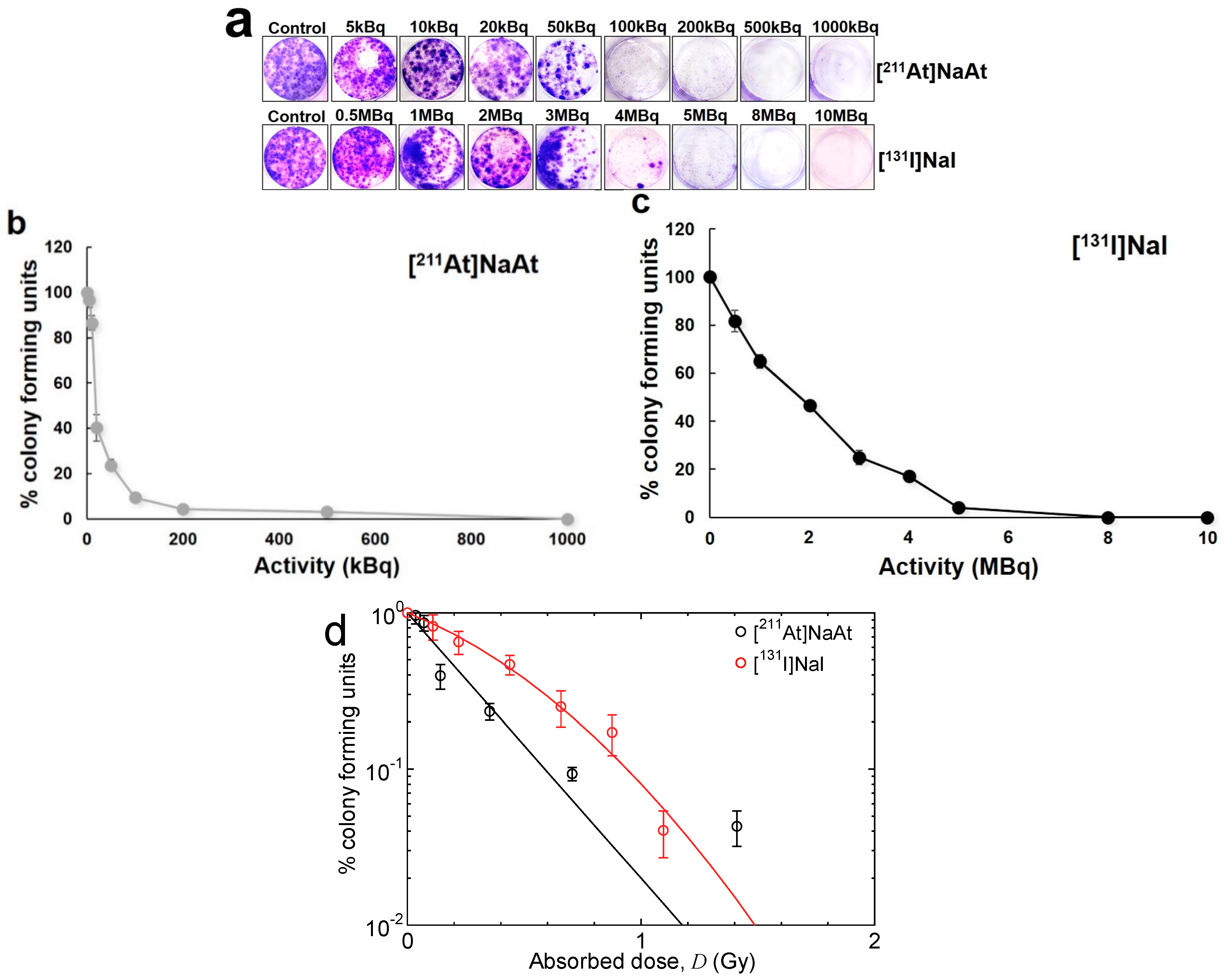
2.1. Observation of DSBs of DNA and Colony Formation in K1-NIS cells
2.2. Biodistribution of [131I]NaI and [211At]NaAt in K1-NIS Xenograft Mice
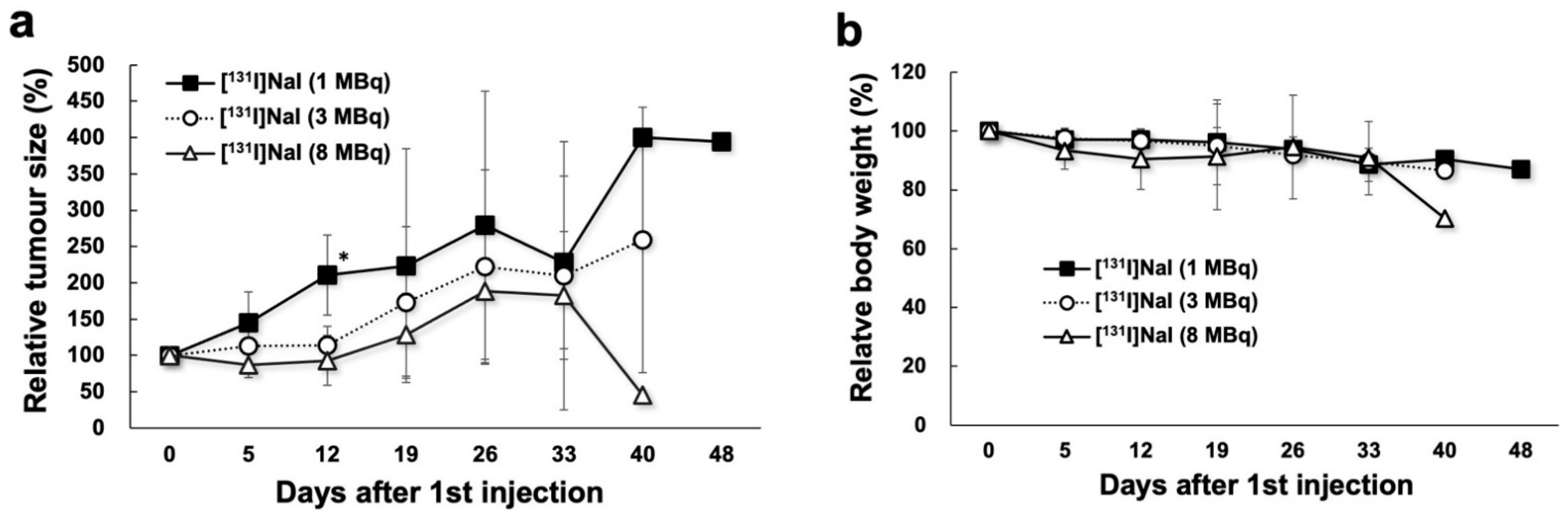
2.3. Changes in Tumour Size and Body Weight in 131I Groups
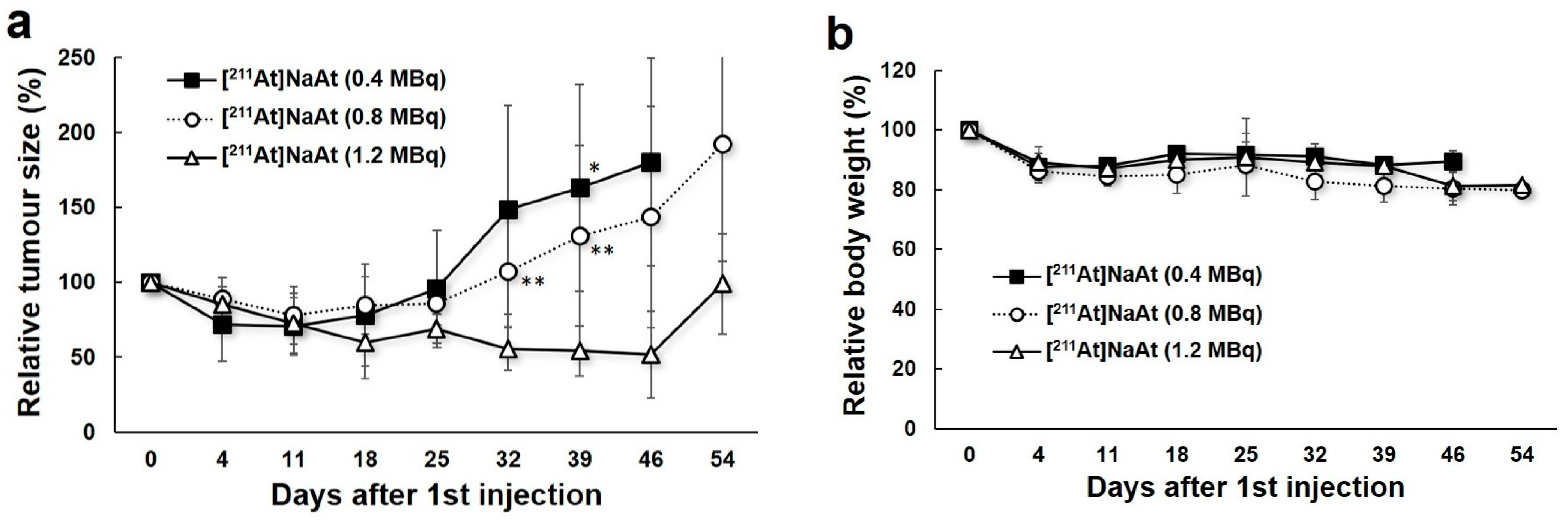
2.4. Changes in Tumour Size and Body Weight in 211At Groups
3. Discussion
4. Materials and Methods
4.1. Preparation of [211At]NaAt Solution
4.2. In Vitro Observation of DSBs of DNA and Colony Formation Assay
4.3. Dosimetry of In Vitro Observation
4.4. Preparation of Animals
4.5. Biodistribution of [131I]NaI and [211At]NaAt in Mice
4.6. Therapy with [131I]NaI and [211At]NaAt Solutions
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maheshwari, Y.K.; Hill, S., Jr.; Haynie, T.P., 3rd; Hickey, R.C.; Samaan, N.A. 131I therapy in differentiated thyroid carcinoma: M. D. Anderson Hospital experience. Cancer 1981, 47, 664–671. [Google Scholar] [CrossRef]
- Maxon, H.R., 3rd; Englaro, E.E.; Thomas, S.R.; Hertzberg, V.S.; Hinnefeld, J.D.; Chen, L.S.; Smith, H.; Cummings, D.; Aden, M.D. Radioiodine-131 therapy for well-differentiated thyroid cancer—A quantitative radiation dosimetric approach: Outcome and validation in 85 patients. J. Nucl. Med. 1992, 33, 1132–1136. [Google Scholar] [PubMed]
- Mayson, S.E.; Chan, M.; Haugen, B.R. Tailoring the approach to radioactive iodine treatment in thyroid cancer. Endocr. Relat. Cancer 2021, 28, T125–T140. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Brose, M.; Elisei, R.; Leboulleux, S.; Luster, M.; Pitoia, F.; Pacini, F. Definition and management of radioactive iodine-refractory differentiated thyroid cancer. Lancet Diabetes Endocrinol. 2014, 2, 356–358. [Google Scholar] [CrossRef]
- Zalutsky, M.R.; Vaidyanathan, G. Astatine-211-labeled radiotherapeutics: An emerging approach to targeted alpha-particle radiotherapy. Curr. Pharm. Des. 2000, 6, 1433–1455. [Google Scholar] [CrossRef] [PubMed]
- Andersson, H.; Palm, S.; Lindegren, S.; Bäck, T.; Jacobsson, L.; Leser, G.; Horvath, G. Comparison of the therapeutic efficacy of 211At- and 131I-labelled monoclonal antibody MOv18 in nude mice with intraperitoneal growth of human ovarian cancer. Anticancer Res. 2001, 21, 409–412. [Google Scholar]
- Dahle, J.; Abbas, N.; Bruland, Ø.S.; Larsen, R.H. Toxicity and relative biological effectiveness of alpha emitting radioimmunoconjugates. Curr. Radiopharm. 2011, 4, 321–328. [Google Scholar] [CrossRef]
- Zalutsky, M.R.; Reardon, D.A.; Akabani, G.; Coleman, R.E.; Friedman, A.H.; Friedman, H.S.; McLendon, R.E.; Wong, T.Z.; Bigner, D.D. Clinical experience with alpha-particle emitting 211At: Treatment of recurrent brain tumor patients with 211At-labeled chimeric antitenascin monoclonal antibody 81C6. J. Nucl. Med. 2008, 49, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Hallqvist, A.; Bergmark, K.; Bäck, T.; Andersson, H.; Dahm-Kähler, P.; Johansson, M.; Lindegren, S.; Jensen, H.; Jacobsson, L.; Hultborn, R.; et al. Intraperitoneal α-emitting radioimmunotherapy with 211At in relapsed ovarian cancer: Long-term follow-up with individual absorbed dose estimations. J. Nucl. Med. 2019, 60, 1073–1079. [Google Scholar] [CrossRef] [Green Version]
- Petrich, T.; Quintanilla-Martinez, L.; Korkmaz, Z.; Samson, E.; Helmeke, H.J.; Meyer, G.J.; Knapp, W.H.; Pötter, E. Effective cancer therapy with the alpha-particle emitter [211At]astatine in a mouse model of genetically modified sodium/iodide symporter-expressing tumors. Clin. Cancer Res. 2006, 12, 1342–1348. [Google Scholar] [CrossRef] [Green Version]
- Watabe, T.; Kaneda-Nakashima, K.; Liu, Y.; Shirakami, Y.; Ooe, K.; Toyoshima, A.; Shimosegawa, E.; Fukuda, M.; Shinohara, A.; Hatazawa, J. Enhancement of 211At uptake via the sodium iodide symporter by the addition of ascorbic acid in targeted alpha-therapy of thyroid cancer. J. Nucl. Med. 2019, 60, 1301–1307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Watabe, T.; Kaneda-Nakashima, K.; Ooe, K.; Shirakami, Y.; Toyoshima, A.; Shimosegawa, E.; Nakano, T.; Shinohara, A.; Hatazawa, J. Preclinical evaluation of radiation-induced toxicity in targeted alpha therapy using [211At] NaAt in Mice: A Revisit. Transl. Oncol. 2020, 13, 100757. [Google Scholar] [CrossRef] [PubMed]
- Watabe, T.; Kaneda-Nakashima, K.; Ooe, K.; Liu, Y.; Kurimoto, K.; Murai, T.; Shidahara, Y.; Okuma, K.; Takeuchi, M.; Nishide, M.; et al. Extended single-dose toxicity study of [211At]NaAt in mice for the first-in-human clinical trial of targeted alpha therapy for differentiated thyroid cancer. Ann. Nucl. Med. 2021, 35, 702–718. [Google Scholar] [CrossRef]
- Jin, Y.; Van Nostrand, D.; Cheng, L.; Liu, M.; Chen, L. Radioiodine refractory differentiated thyroid cancer. Crit. Rev. Oncol. Hematol. 2018, 125, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Watabe, T.; Hosono, M.; Kinuya, S.; Yamada, T.; Yanagida, S.; Namba, M.; Nakamura, Y. Manual on the proper use of sodium astatide ([211At]NaAt) injections in clinical trials for targeted alpha therapy (1st edition). Ann. Nucl. Med. 2021, 35, 753–766. [Google Scholar] [CrossRef]
- Kaneda-Nakashima, K.; Zhang, Z.; Manabe, Y.; Shimoyama, A.; Kabayama, K.; Watabe, T.; Kanai, Y.; Ooe, K.; Toyoshima, A.; Shirakami, Y.; et al. α-Emitting cancer therapy using 211At-AAMT targeting LAT1. Cancer Sci. 2021, 112, 1132–1140. [Google Scholar] [CrossRef]
- Lyckesvärd, M.N.; Delle, U.; Kahu, H.; Lindegren, S.; Jensen, H.; Bäck, T.; Swanpalmer, J.; Elmroth, K. Alpha particle induced DNA damage and repair in normal cultured thyrocytes of different proliferation status. Mutat. Res. 2014, 765, 48–56. [Google Scholar] [CrossRef]
- Lorat, Y.; Timm, S.; Jakob, B.; Taucher-Scholz, G.; Rübe, E. Clustered double-strand breaks in heterochromatin perturb DNA repair after high linear energy transfer irradiation. Radiother. Oncol. 2016, 121, 154–161. [Google Scholar] [CrossRef]
- Ritter, M.A.; Cleaver, J.E.; Tobias, A. High-LET radiations induce a large proportion of non-rejoining DNA breaks. Nature 1977, 266, 653–655. [Google Scholar] [CrossRef]
- Goodhead, D.T. Initial events in the cellular effects of ionizing radiations: Clustered damage in DNA. Int. J. Radiat. Biol. 1994, 65, 7–17. [Google Scholar] [CrossRef]
- Pouget, J.P.; Mather, S.J. General aspects of the cellular response to low- and high-LET radiation. Eur. J. Nucl. Med. 2001, 28, 541–561. [Google Scholar] [CrossRef] [PubMed]
- Jenner, T.J.; deLara, M.; O’Neill, P.; Stevens, D.L. Induction and rejoining of DNA double-strand breaks in V79-4 mammalian cells following gamma- and alpha-irradiation. Int. J. Radiat. Biol. 1993, 64, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Sgouros, G.; Roeske, J.C.; McDevitt, M.R.; Palm, S.; Allen, B.J.; Fisher, D.R.; Brill, A.B.; Song, H.; Howell, R.W.; Akabani, G.; et al. MIRD Pamphlet No. 22 (abridged): Radiobiology and dosimetry of alpha-particle emitters for targeted radionuclide therapy. J. Nucl. Med. 2010, 51, 311–328. [Google Scholar] [CrossRef] [Green Version]
- Sato, T.; Masunaga, S.I.; Kumada, H.; Hamada, N. Microdosimetric modeling of biological effectiveness for boron neutron capture therapy considering intra- and intercellular heterogeneity in 10B distribution. Sci. Rep. 2018, 8, 988. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Matsuya, Y.; Hamada, N. Microdosimetric modeling of relative biological effectiveness for skin reactions: Possible linkage between in vitro and in vivo data. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Shimura, H.; Haraguchi, K.; Miyazaki, A.; Endo, T.; Onaya, T. Iodide uptake and experimental 131I therapy in transplanted undifferentiated thyroid cancer cells expressing the Na+/I− symporter gene. Endocrinology 1997, 138, 4493–4496. [Google Scholar] [CrossRef]
- Zuckier, L.S.; Dohan, O.; Li, Y.; Chang, J.; Carrasco, N.; Dadachova, E. Kinetics of perrhenate uptake and comparative biodistribution of perrhenate, pertechnetate, and iodide by NaI symporter-expressing tissues in vivo. J. Nucl. Med. 2004, 45, 500–507. [Google Scholar]
- Godlewska, M.; Banga, P.J. Thyroid peroxidase as a dual active site enzyme: Focus on biosynthesis, hormonogenesis and thyroid disorders of autoimmunity and cancer. Biochimie 2019, 160, 34–45. [Google Scholar] [CrossRef]
- Spetz, J.; Rudqvist, N.; Forssell-Aronsson, E. Biodistribution and dosimetry of free 211At, 125I- and 131I- in rats. Cancer Biother. Radiopharm. 2013, 28, 657–664. [Google Scholar] [CrossRef] [Green Version]
- Cobb, L.M.; Harrison, A.; Dudley, N.E.; Carr, T.E.; Humphreys, J.A. Relative concentration of astatine-211 and iodine-125 by human fetal thyroid and carcinoma of the thyroid in nude mice. Radiother. Oncol. 1988, 13, 203–209. [Google Scholar] [CrossRef]
- Kratochwil, C.; Bruchertseifer, F.; Rathke, H.; Bronzel, M.; Apostolidis, C.; Weichert, W.; Haberkorn, U.; Giesel, F.L.; Morgenstern, A. Targeted alpha-therapy of metastatic castration-resistant prostate cancer with 225Ac-PSMA-617: Dosimetry estimate and empiric dose finding. J. Nucl. Med. 2017, 58, 1624–1631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kratochwil, C.; Bruchertseifer, F.; Giesel, F.L.; Weis, M.; Verburg, F.A.; Mottaghy, F.; Kopka, K.; Apostolidis, C.; Haberkorn, U.; Morgenstern, A. 225Ac-PSMA-617 for PSMA-targeted alpha-radiation therapy of metastatic castration-resistant prostate cancer. J. Nucl. Med. 2016, 57, 1941–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khreish, F.; Ebert, N.; Ries, M.; Maus, S.; Rosar, F.; Bohnenberger, H.; Stemler, T.; Saar, M.; Bartholomä, M.; Ezziddin, S. 225Ac-PSMA-617/177Lu-PSMA-617 tandem therapy of metastatic castration-resistant prostate cancer: Pilot experience. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Crowley, L.C.; Christensen, M.E.; Waterhouse, N.J. Measuring survival of adherent cells with the colony-forming assay. Cold Spring Harb. Protoc. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, T.; Iwamoto, Y.; Hashimoto, S.; Ogawa, T.; Furuta, T.; Abe, S.; Kai, T.; Tsai, P.E.; Matsuda, N.; Iwase, H.; et al. Features of Particle and Heavy Ion Transport code System (PHITS) version 3.02. J. Nucl. Sci. Technol. 2018, 55, 684–690. [Google Scholar] [CrossRef] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watabe, T.; Liu, Y.; Kaneda-Nakashima, K.; Sato, T.; Shirakami, Y.; Ooe, K.; Toyoshima, A.; Shimosegawa, E.; Wang, Y.; Haba, H.; et al. Comparison of the Therapeutic Effects of [211At]NaAt and [131I]NaI in an NIS-Expressing Thyroid Cancer Mouse Model. Int. J. Mol. Sci. 2022, 23, 9434. https://doi.org/10.3390/ijms23169434
Watabe T, Liu Y, Kaneda-Nakashima K, Sato T, Shirakami Y, Ooe K, Toyoshima A, Shimosegawa E, Wang Y, Haba H, et al. Comparison of the Therapeutic Effects of [211At]NaAt and [131I]NaI in an NIS-Expressing Thyroid Cancer Mouse Model. International Journal of Molecular Sciences. 2022; 23(16):9434. https://doi.org/10.3390/ijms23169434
Chicago/Turabian StyleWatabe, Tadashi, Yuwei Liu, Kazuko Kaneda-Nakashima, Tatsuhiko Sato, Yoshifumi Shirakami, Kazuhiro Ooe, Atsushi Toyoshima, Eku Shimosegawa, Yang Wang, Hiromitsu Haba, and et al. 2022. "Comparison of the Therapeutic Effects of [211At]NaAt and [131I]NaI in an NIS-Expressing Thyroid Cancer Mouse Model" International Journal of Molecular Sciences 23, no. 16: 9434. https://doi.org/10.3390/ijms23169434