Unproductive Effects of ALK Gene Amplification and Copy Number Gain in Non-Small-Cell Lung Cancer. ALK Gene Amplification and Copy Gain in NSCLC

 , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Results
2.1. Clinical and Pathological Characteristics of Patients
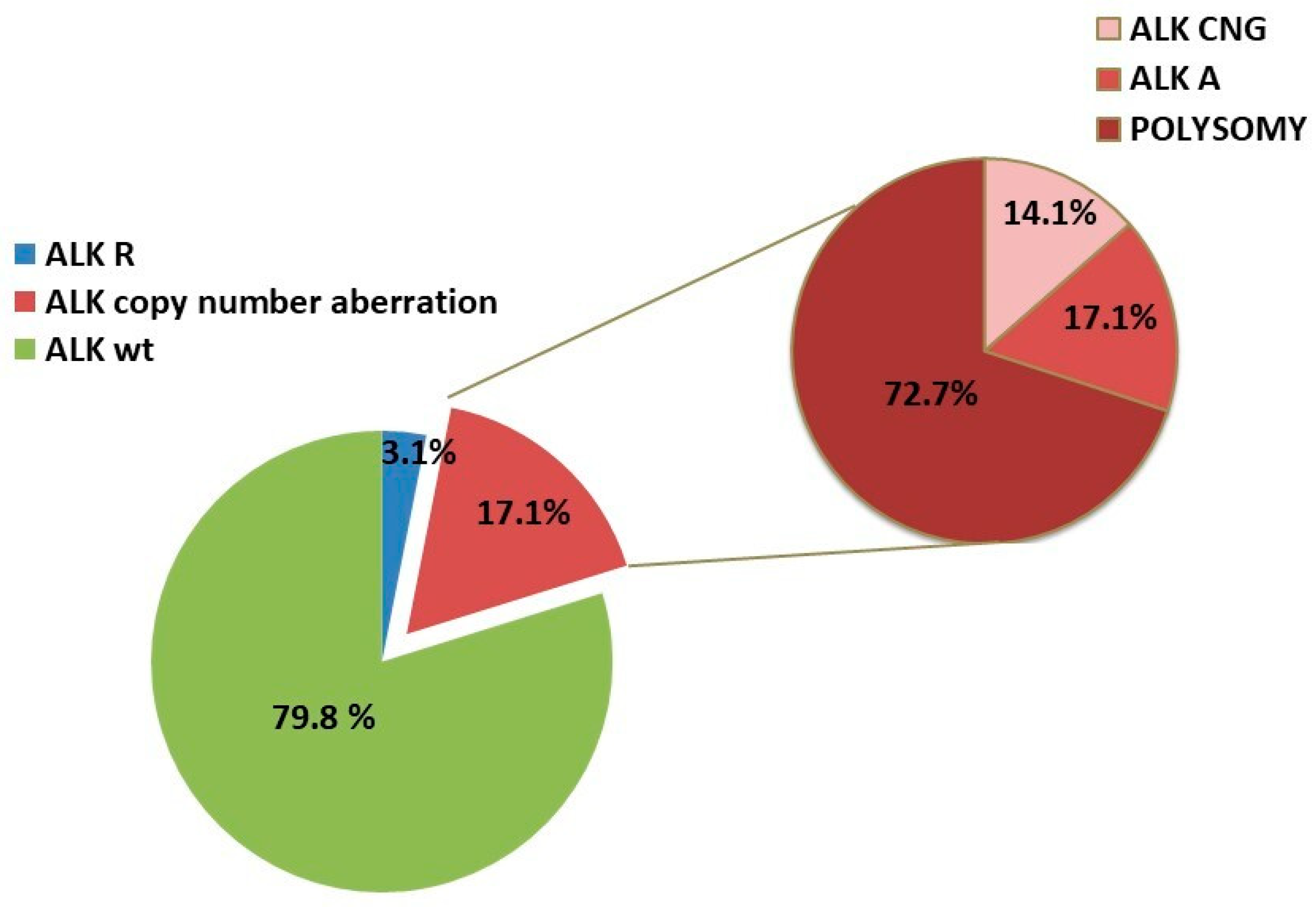
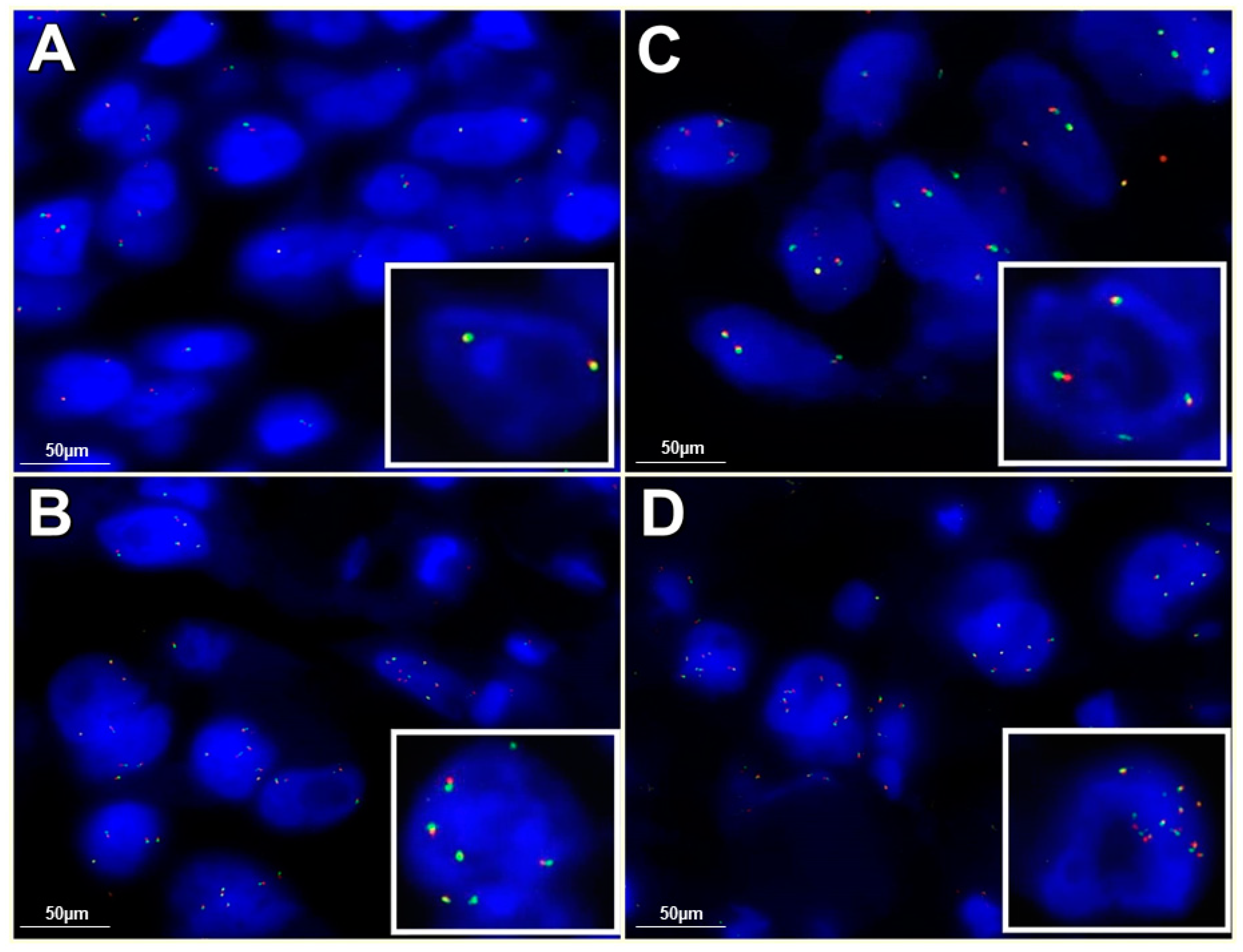
2.2. Fluorescence In Situ Hybridization
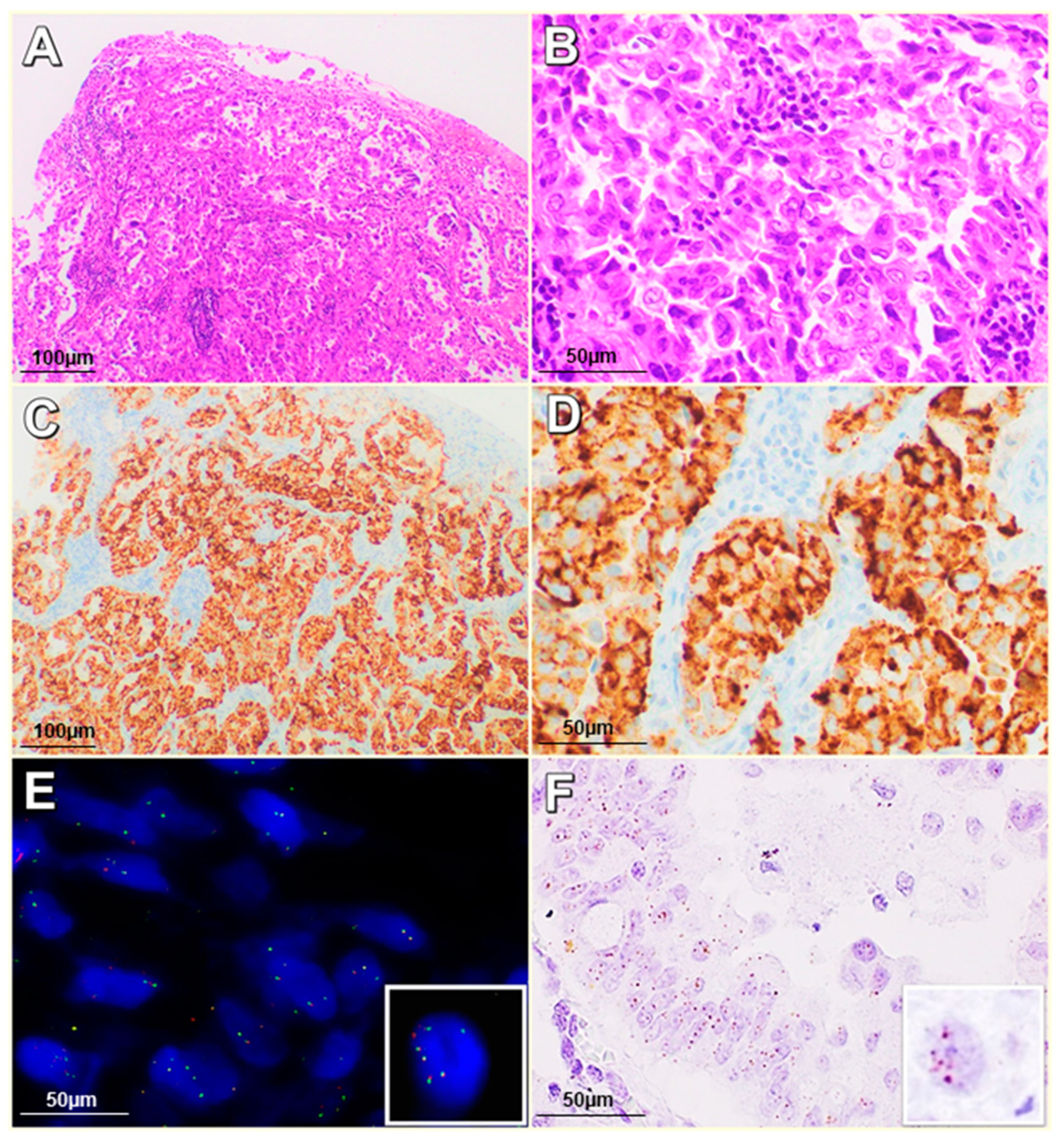
2.3. Immunohistochemistry Analysis of ALK Protein Expression
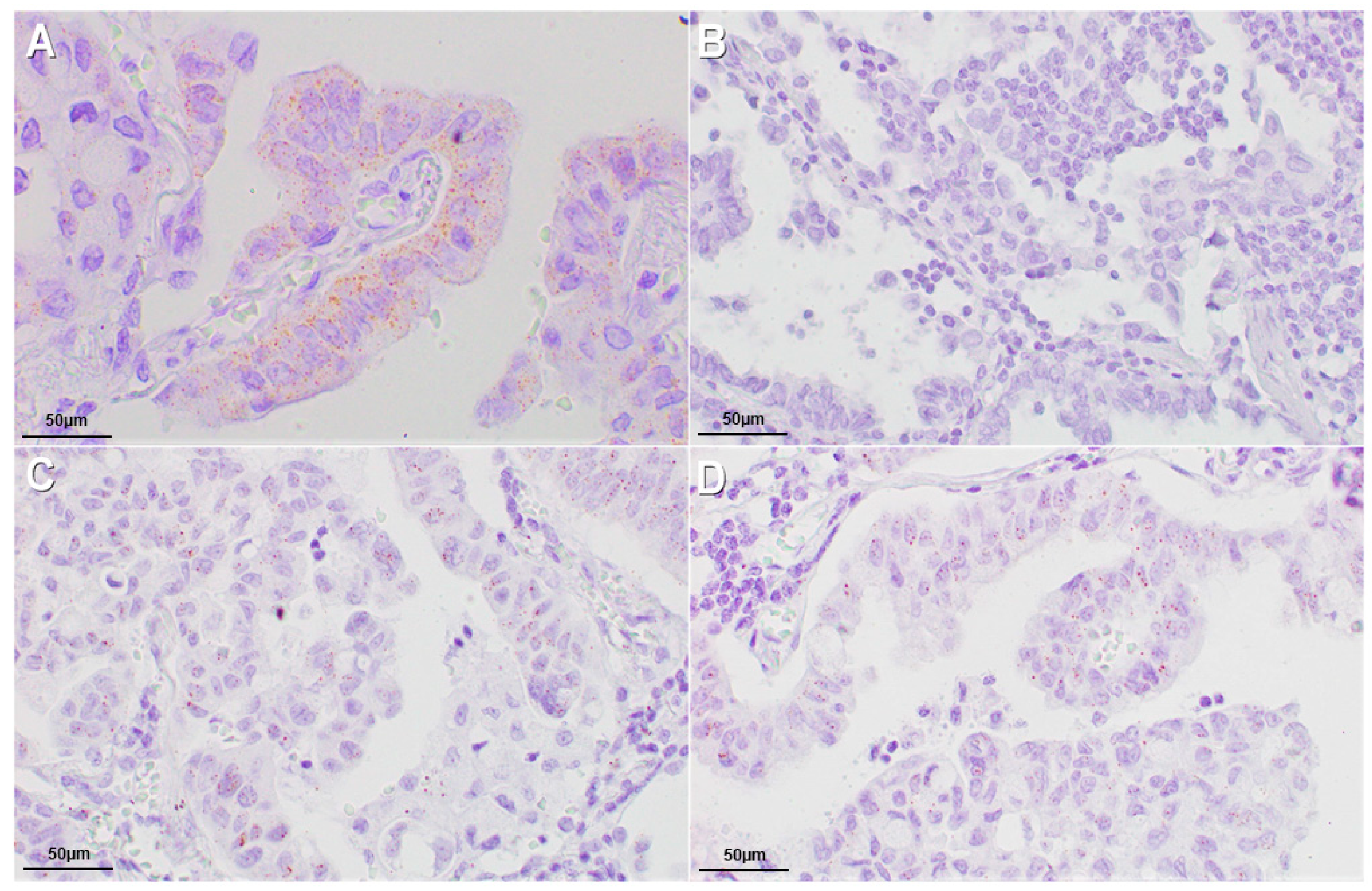
2.4. In Situ Hybridization (ISH) Assay for ALK RNA Detection
3. Discussion
4. Materials and Methods
4.1. Patients and Specimens
4.2. Tissue Microarray Construction
4.3. Fluorescence In Situ Hybridization
4.4. ALK Gene Rearrangement Interpretation
4.5. ALK Copy Number Gain/Amplification Interpretation
4.6. Centromeric Alpha-Satellite Specific for Chromosome 2 Interpretation
4.7. Immunohistochemistry Analysis of ALK Protein Expression
4.8. In Situ Hybridization (ISH) Assay for ALK RNA Detection
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ALK | anaplastic lymphoma kinase |
| NSCLC | non-small cell lung cancer |
| ALK-CNG | ALK gene copy number gain |
| ALK-R | ALK gene rearrangement |
| ALK-A | ALK gene amplification |
| FISH | fluorescence in situ hybridization |
| ALCL | anaplastic large-cell lymphoma |
| JAK/STAT | Janus-activated kinase/signal transducer and activator of transcription |
| EGFR | epidermal growth factor receptor |
| ADC | adenocarcinoma |
| SQ | squamous carcinoma |
| AdSqLC | adenosquamous lung carcinomas |
| TMA | tissue microarrays |
| CEP2 | centromeric probe 2 |
References
- Motegi, A.; Fujimoto, J.; Kotani, M.; Sakuraba, H.; Yamamoto, T. ALK receptor tyrosine kinase promotes cell growth and neurite outgrowth. J. Cell Sci. 2004, 117, 3319–3329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, S.W.; Kirstein, M.N.; Valentine, M.B.; Dittmer, K.G.; Shapiro, D.N.; Saltman, D.L.; Look, A.T. Fusion of a kinase gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin’s lymphoma. Science 1994, 263, 1281–1284. [Google Scholar] [CrossRef] [PubMed]
- Chiarle, R.; Voena, C.; Ambrogio, C.; Piva, R.; Inghirami, G. The anaplastic lymphoma kinase in the pathogenesis of cancer. Nat. Rev. Cancer 2008, 8, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Roskoski, R., Jr. Anaplastic lymphoma kinase (ALK): Structure, oncogenic activation, and pharmacological inhibition. Pharmacol. Res. 2013, 68, 68–94. [Google Scholar] [CrossRef]
- Franco, R.; Rocco, G.; Marino, F.Z.; Pirozzi, G.; Normanno, N.; Morabito, A.; Sperlongano, P.; Stiuso, P.; Luce, A.; Botti, G.; et al. Anaplastic lymphoma kinase: A glimmer of hope in lung cancer treatment? Expert Rev. Anticancer Ther. 2013, 13, 407–420. [Google Scholar] [CrossRef]
- Palmer, R.H.; Vernersson, E.; Grabbe, C.; Hallberg, B. Anaplastic lymphoma kinase: Signalling in development and disease. Biochem. J. 2009, 420, 345–361. [Google Scholar] [CrossRef] [Green Version]
- Marino, F.Z.; Rocco, G.; Morabito, A.; Mignogna, C.; Intartaglia, M.; Liguori, G.; Botti, G.; Franco, R. A new look at the ALK gene in cancer: Copy number gain and amplification. Expert Rev. Anticancer Ther. 2016, 16, 493–502. [Google Scholar] [CrossRef]
- Subramaniam, M.M.; Piqueras, M.; Navarro, S.; Noguera, R. Aberrant copy numbers of ALK gene is a frequent genetic alteration in neuroblastomas. Hum. Pathol. 2009, 40, 1638–1642. [Google Scholar] [CrossRef]
- McDermott, U.; Iafrate, A.J.; Gray, N.S.; Dowell, L.; Ulkus, L.E.; Kuhlmann, G.; Greninger, P.; Christensen, J.G.; Haber, D.A.; Settleman, J. Alterations of Anaplastic Lymphoma Kinase May Sensitize Tumors to Anaplastic Lymphoma Kinase Inhibitors. Cancer Res. 2008, 68, 3389–3395. [Google Scholar] [CrossRef] [Green Version]
- Robertson, F.M.; Petricoin, E.F., III; Van Laere, S.J.; Bertucci, F.; Chu, K.; Fernandez, S.V.; Mu, Z.; Alpaugh, K.; Pei, J.; Circo, R.; et al. Presence of anaplastic lymphoma kinase in inflammatory breast cancer. Springerplus 2013, 2, 497. [Google Scholar] [CrossRef] [Green Version]
- Tuma, R.S. ALK gene amplified in most inflammatory breast cancers. J. Natl. Cancer Inst. 2012, 104, 87–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoppmann, S.F.; Streubel, B.; Birner, P. Amplification but not translocation of anaplastic lymphoma kinase is a frequent event in oesophageal cancer. Eur. J. Cancer 2013, 49, 1876–1881. [Google Scholar] [CrossRef] [PubMed]
- Salido, M.; Pijuan, L.; Martínez-Avilés, L.; Galván, A.B.; Cañadas, I.; Rovira, A.; Zanui, M.; Martínez, A.; Longarón, R.; Sole, F.; et al. Increased ALK gene copy number and amplification are frequent in non-small cell lung cancer. J. Thorac. Oncol. 2011, 6, 21–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelosi, G.; Gasparini, P.; Cavazza, A.; Rossi, G.; Graziano, P.; Barbareschi, M.; Perrone, F.; Barberis, M.; Takagi, M.; Kunimura, T.; et al. Multiparametric molecular characterization of pulmonary sarcomatoid carcinoma reveals a nonrandom amplification of anaplastic lymphoma kinase (ALK) gene. Lung Cancer 2012, 77, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Miyake, I.; Hakomori, Y.; Shinohara, A.; Gamou, T.; Saito, M.; Iwamatsu, A.; Sakai, R. Activation of anaplastic lymphoma kinase is responsible for hyperphosphorylation of ShcC in neuroblastoma cell lines. Oncogene 2002, 21, 5823–5834. [Google Scholar] [CrossRef] [Green Version]
- Camidge, D.R.; Skokan, M.; Kiatsimkul, P.; Helfrich, B.; Lu, X.; Barón, A.E.; Schulte, N.; Maxson, D.; Aisner, D.L.; Franklin, W.A.; et al. Native and rearranged ALK copy number and rearranged cell count in NSCLC: Implications for ALK inhibitor therapy. Cancer 2013, 119, 3968–3975. [Google Scholar] [CrossRef] [Green Version]
- Caliò, A.; Bria, E.; Pilotto, S.; Gilioli, E.; Nottegar, A.; Eccher, A.; Cima, L.; Santo, A.; Pedron, S.; Turri, G.; et al. ALK gene copy number in lung cancer: Unspecific polyploidy versus specific amplification visible as double minutes. Cancer Biomark. 2017, 18, 215–220. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Woodward, W.; Yang, W.; Reuben, J.M.; Tepperberg, J.; Ogura, D.; Niwa, S.; Huo, L.; Gong, Y.; El-Zein, R.; et al. Status of the anaplastic lymphoma kinase (ALK) gene in inflammatory breast carcinoma. Springerplus 2013, 2, 409. [Google Scholar] [CrossRef] [Green Version]
- Testa, J.R.; Siegfried, J.M. Chromosome abnormalities in human non-small cell lung cancer. Cancer Res. 1992, 52, 2702s–2706s. [Google Scholar]
- Luk, C.; Tsao, M.S.; Bayani, J.; Shepherd, F.; Squire, J.A. Molecular cytogenetic analysis of non-small cell lung carcinoma by spectral karyotyping and comparative genomic hybridization. Cancer Genet. Cytogenet. 2001, 125, 87–99. [Google Scholar] [CrossRef]
- Shen, H.; Gao, W.; Wu, Y.J.; Qiu, H.R.; Shu, Y.Q. Multicolor fluorescence in situ hybridization and comparative genomic hybridization reveal molecular events in lung adenocarcinomas and squamous cell lung carcinomas. Biomed. Pharmacother. 2009, 63, 396–403. [Google Scholar] [CrossRef]
- Cabillic, F.; Hofman, P.; Ilie, M.; Peled, N.; Hochmair, M.; Dietel, M.; Von Laffert, M.; Gosney, J.R.; Lopez-Rios, F.; Erb, G.; et al. ALK IHC and FISH discordant results in patients with NSCLC and treatment response: For discussion of the question to treat or not to treat? ESMO Open 2018, 3, e000419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uruga, H.; Mino-Kenudson, M. ALK (D5F3) CDx: An immunohistochemistry assay to identify ALK-positive NSCLC patients. Pharmgenom. Pers. Med. 2018, 11, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, W.D. Pathology of lung cancer. Clin. Chest Med. 2011, 32, 669–692. [Google Scholar] [CrossRef] [PubMed]
- Marino, F.Z.; Liguori, G.; Aquino, G.; La Mantia, E.; Bosari, S.; Ferrero, S.; Rosso, L.; Gaudioso, G.; De Rosa, N.; Scrima, M.; et al. Intratumor Heterogeneity of ALK-Rearrangements and Homogeneity of EGFR-Mutations in Mixed Lung Adenocarcinoma. PLoS ONE 2015, 10, e0141521. [Google Scholar] [CrossRef] [Green Version]
- Tsao, M.S.; Hirsh, F.R.; Yatabe, Y. IASLC Atlas of ALK and ROS1 Testing in Lung Cancer, 2nd ed.; Fort Meyers Editorial Rx Press: Florida, FL, USA, 2016. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Cases (%) |
|---|---|
| All cases | 578 |
| Age | |
| ≥65 years | 317 (54.8%) |
| <65 years | 261 (45.2%) |
| Gender | |
| Male | 397 (68.7%) |
| Female | 181 (31.3%) |
| Smoking Habit | |
| Yes | 330 (57.1%) |
| No | 83 (14.4%) |
| ex-smokers | 32 (5.5%) |
| NA | 133 (23.0%) |
| Histotype | |
| ADCs | 398 (68.9%) |
| SQs | 139 (24.0%) |
| AdSqLCs | 5 (0.9%) |
| Other | 36 (6.2%) |
| Disease Stage | |
| IA | 132 (22.8%) |
| IB | 120 (20.8%) |
| IIA | 188 (32.6%) |
| IIB | 23 (4.0%) |
| III | 2 (0.3%) |
| IV | 81 (14.0%) |
| NA | 32 (5.5%) |
| Grade | |
| I | 37 (6.4%) |
| II | 262 (45.3%) |
| III | 210 (36.3%) |
| IV | 2 (0.3%) |
| NA | 67 (11.6%) |
| Pz ALK-A | Gender | Age | Histotype | Stage | Grade | Smoker Status | ALK ISH | ALK IHC | ALK-R |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 60 | SQ | IIA | G3 | NA | − | − | WT |
| 2 | M | 74 | ADC | IIA | G2 | Y | − | − | WT |
| 3 | M | 64 | SQ | IIA | G2 | Y | − | − | WT |
| 4 | M | 63 | ADC | IB | NA | Y | − | − | WT |
| 5 | F | 66 | ADC | IIA | G2 | NA | − | − | WT |
| 6 | M | 77 | SQ | IIA | G3 | Y | − | − | WT |
| 7 | M | 55 | SQ | IIA | G2 | EX | − | − | WT |
| 8 | F | 71 | ADC | IIA | G2 | EX | + | + | R |
| 9 | M | 59 | SQ | IIA | G2 | EX | − | − | WT |
| 10 | M | 49 | ADC | IIA | G2 | NA | − | − | WT |
| 11 | M | 63 | ADC | IA | G3 | NA | − | − | WT |
| 12 | F | 64 | ADC | IV | G3 | NA | − | − | WT |
| 13 | M | 63 | ADC | IB | G2 | Y | − | − | WT |
| 14 | M | 67 | ADC | IIA | G2 | Y | − | − | WT |
| 15 | F | 70 | SQ | IV | G3 | EX | − | − | WT |
| 16 | M | 63 | ADC | IA | G3 | Y | − | − | WT |
| 17 | M | 70 | ADC | IIA | G2 | NA | − | − | WT |
| ALK FISH Status | ALK ISH+ | ALK IHC+ |
|---|---|---|
| 18 ALK-R | 18/18 | 18/18 |
| 17 ALK-A | 1/17 | 1/17 |
| 14 ALK-CNG | 0/14 | 0/14 |
| 72 ALK-CNG and Polisomy Chr2 | 0/72 | 0/72 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zito Marino, F.; Botti, G.; Aquino, G.; Ferrero, S.; Gaudioso, G.; Palleschi, A.; Rocco, D.; Salvi, R.; Micheli, M.C.; Micheli, P.; et al. Unproductive Effects of ALK Gene Amplification and Copy Number Gain in Non-Small-Cell Lung Cancer. ALK Gene Amplification and Copy Gain in NSCLC. Int. J. Mol. Sci. 2020, 21, 4927. https://doi.org/10.3390/ijms21144927
Zito Marino F, Botti G, Aquino G, Ferrero S, Gaudioso G, Palleschi A, Rocco D, Salvi R, Micheli MC, Micheli P, et al. Unproductive Effects of ALK Gene Amplification and Copy Number Gain in Non-Small-Cell Lung Cancer. ALK Gene Amplification and Copy Gain in NSCLC. International Journal of Molecular Sciences. 2020; 21(14):4927. https://doi.org/10.3390/ijms21144927
Chicago/Turabian StyleZito Marino, Federica, Gerardo Botti, Gabriella Aquino, Stefano Ferrero, Gabriella Gaudioso, Alessandro Palleschi, Danilo Rocco, Rosario Salvi, Maria Carolina Micheli, Pietro Micheli, and et al. 2020. "Unproductive Effects of ALK Gene Amplification and Copy Number Gain in Non-Small-Cell Lung Cancer. ALK Gene Amplification and Copy Gain in NSCLC" International Journal of Molecular Sciences 21, no. 14: 4927. https://doi.org/10.3390/ijms21144927