Unmethylated Insulin as an Adjunctive Marker of Beta Cell Death and Progression to Type 1 Diabetes in Participants at Risk for Diabetes

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of TrialNet Participants
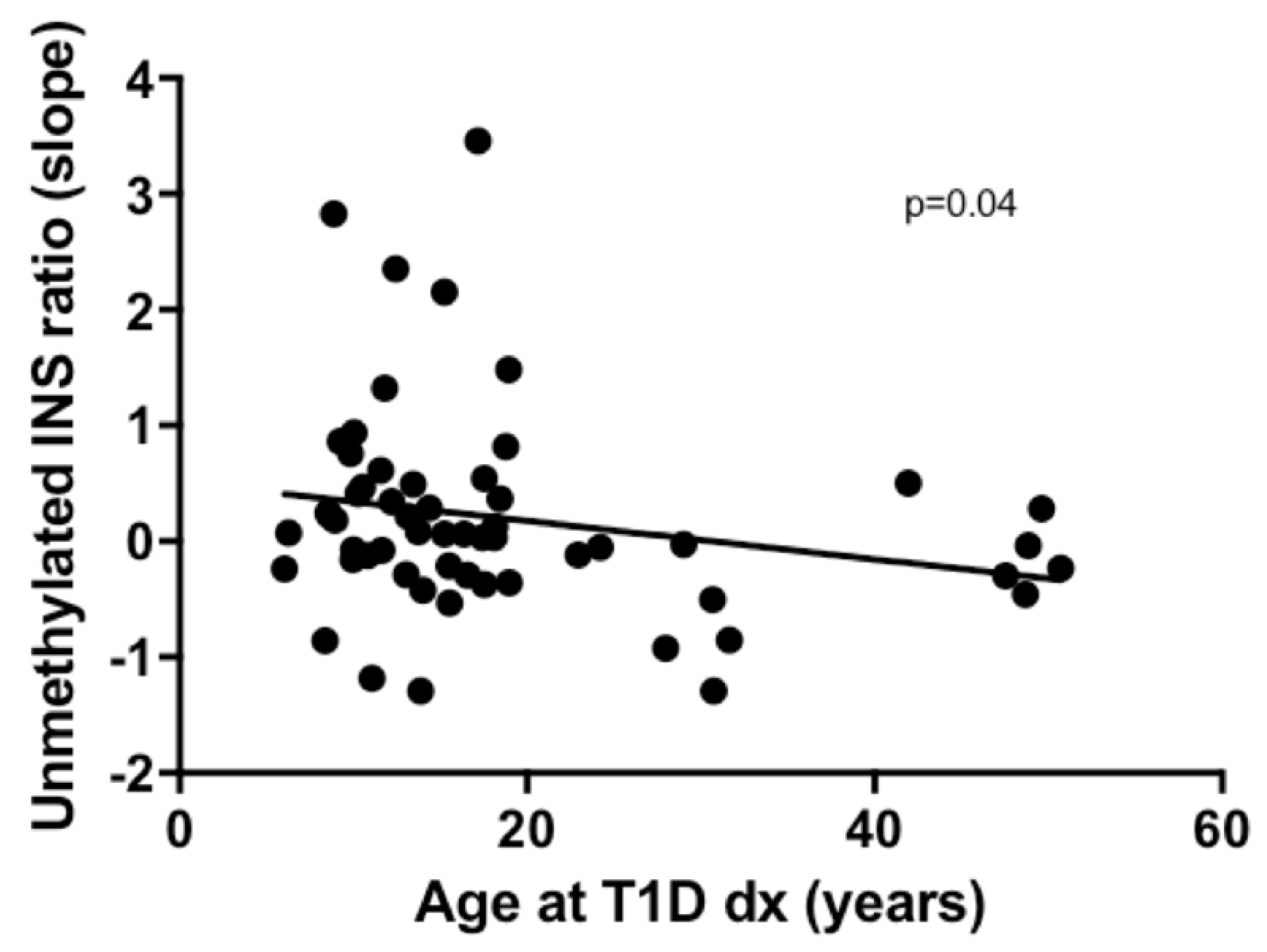
2.2. Association of Unmethylated INS Ratio with Age at T1D Diagnosis
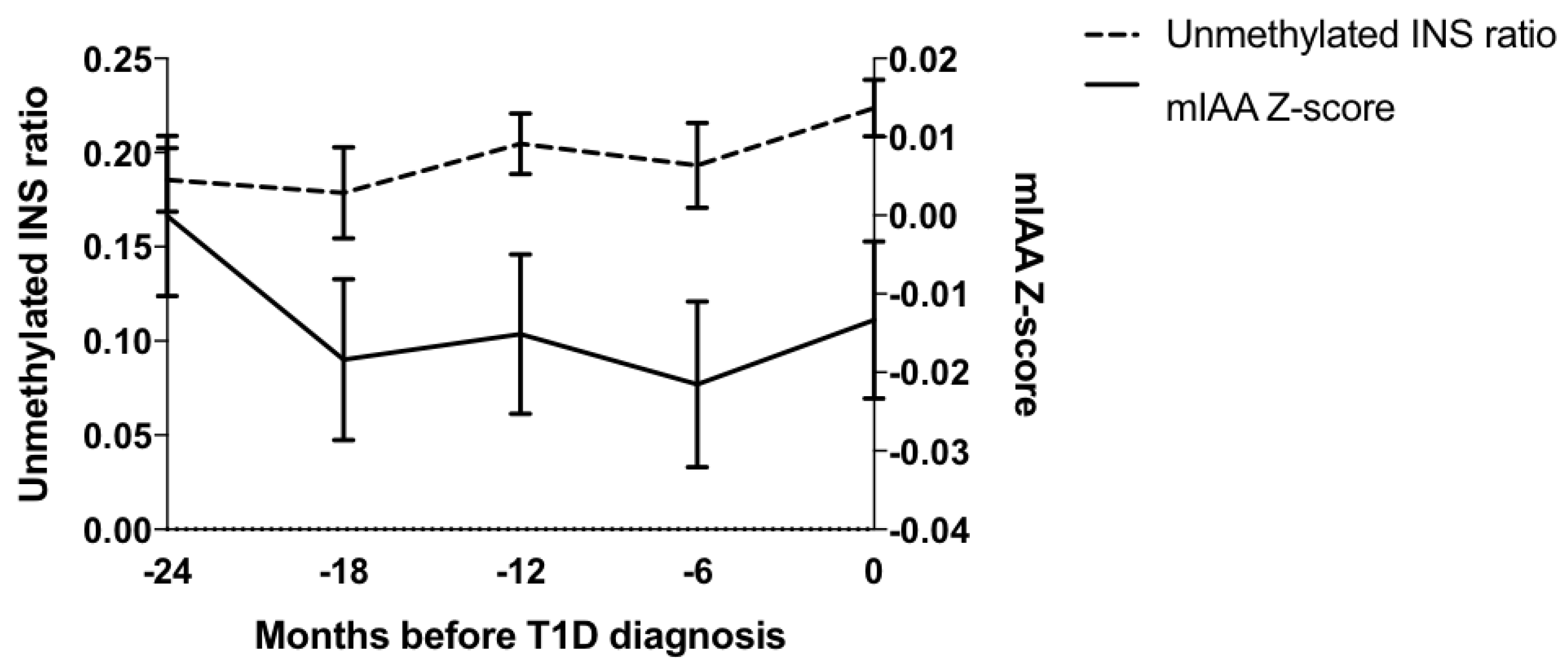
2.3. Association of Unmethylated INS Ratio with iAb Levels
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Laboratory Measurements
4.2.1. Radioassays
4.2.2. ECL Assays
4.3. Statistical Analyses
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| iAb | Islet Autoantibody |
| T1D | Type 1 Diabetes |
| INS | Insulin |
| ECL | Electrochemiluminescence |
| RIA | Radioimmunoassay |
| GAD | glutamic acid decarboxylase |
| IA-2 | insulinoma antigen 2 |
| ZnT8 | zinc transporter 8 |
| mIAA | Insulin autoantibody |
References
- Insel, R.A.; Dunne, J.L.; Atkinson, M.A.; Chiang, J.L.; Dabelea, D.; Gottlieb, P.A.; Greenbaum, C.J.; Herold, K.C.; Krischer, J.P.; Lernmark, A.; et al. Staging Presymptomatic Type 1 Diabetes: A Scientific Statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care 2015, 38, 1964–1974. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, A.G.; Rewers, M.; Simell, O.; Simell, T.; Lempainen, J.; Steck, A.; Winkler, C.; Ilonen, J.; Veijola, R.; Knip, M.; et al. Seroconversion to multiple islet autoantibodies and risk of progression to diabetes in children. JAMA J. Am. Med Assoc. 2013, 309, 2473–2479. [Google Scholar] [CrossRef]
- Steck, A.K.; Johnson, K.; Barriga, K.J.; Miao, D.; Yu, L.; Hutton, J.C.; Eisenbarth, G.S.; Rewers, M.J. Age of islet autoantibody appearance and mean levels of insulin, but not GAD or IA-2 autoantibodies, predict age of diagnosis of type 1 diabetes: Diabetes autoimmunity study in the young. Diabetes Care 2011, 34, 1397–1399. [Google Scholar] [CrossRef]
- Steck, A.K.; Vehik, K.; Bonifacio, E.; Lernmark, A.; Ziegler, A.G.; Hagopian, W.A.; She, J.; Simell, O.; Akolkar, B.; Krischer, J.; et al. Predictors of Progression From the Appearance of Islet Autoantibodies to Early Childhood Diabetes: The Environmental Determinants of Diabetes in the Young (TEDDY). Diabetes Care 2015, 38, 808–813. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Dong, F.; Miao, D.; Fouts, A.R.; Wenzlau, J.M.; Steck, A.K. Proinsulin/Insulin autoantibodies measured with electrochemiluminescent assay are the earliest indicator of prediabetic islet autoimmunity. Diabetes Care 2013, 36, 2266–2270. [Google Scholar] [CrossRef]
- Miao, D.; Guyer, K.M.; Dong, F.; Jiang, L.; Steck, A.K.; Rewers, M.; Eisenbarth, G.S.; Yu, L. GAD65 autoantibodies detected by electrochemiluminescence assay identify high risk for type 1 diabetes. Diabetes 2013, 62, 4174–4178. [Google Scholar] [CrossRef]
- Miao, D.; Steck, A.K.; Zhang, L.; Guyer, K.M.; Jiang, L.; Armstrong, T.; Muller, S.M.; Krischer, J.; Rewers, M.; Yu, L. Electrochemiluminescence assays for insulin and glutamic Acid decarboxylase autoantibodies improve prediction of type 1 diabetes risk. Diabetes Technol. Ther. 2015, 17, 119–127. [Google Scholar] [CrossRef]
- Akirav, E.M.; Lebastchi, J.; Galvan, E.M.; Henegariu, O.; Akirav, M.; Ablamunits, V.; Lizardi, P.M.; Herold, K.C. Detection of beta cell death in diabetes using differentially methylated circulating DNA. Proc. Natl. Acad. Sci. USA 2011, 108, 19018–19023. [Google Scholar] [CrossRef]
- Usmani-Brown, S.; Lebastchi, J.; Steck, A.K.; Beam, C.; Herold, K.C.; Ledizet, M. Analysis of beta-cell death in type 1 diabetes by droplet digital PCR. Endocrinology 2014, 155, 3694–3698. [Google Scholar] [CrossRef]
- Fisher, M.M.; Watkins, R.A.; Blum, J.; Evans-Molina, C.; Chalasani, N.; DiMeglio, L.A.; Mather, K.J.; Tersey, S.A.; Mirmira, R.G. Elevations in Circulating Methylated and Unmethylated Preproinsulin DNA in New-Onset Type 1 Diabetes. Diabetes 2015, 64, 3867–3872. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Lin, G.; Han, Y.; Xie, J.; Li, J. Circulating unmethylated insulin DNA as a potential non-invasive biomarker of beta cell death in type 1 Diabetes: A review and future prospect. Clin. Epigenetics 2017, 9, 44. [Google Scholar] [CrossRef]
- Mirmira, R.G.; Sims, E.K.; Syed, F.; Evans-Molina, C. Biomarkers of beta-Cell Stress and Death in Type 1 Diabetes. Curr. Diabetes Rep. 2016, 16, 95. [Google Scholar] [CrossRef]
- Kuroda, A.; Rauch, T.A.; Todorov, I.; Ku, H.T.; Al-Abdullah, I.H.; Kandeel, F.; Mullen, Y.; Pfeifer, G.P.; Ferreri, K. Insulin gene expression is regulated by DNA methylation. PloS ONE 2009, 4, e6953. [Google Scholar] [CrossRef]
- Husseiny, M.I.; Kaye, A.; Zebadua, E.; Kandeel, F.; Ferreri, K. Tissue-specific methylation of human insulin gene and PCR assay for monitoring beta cell death. PloS ONE 2014, 9, e94591. [Google Scholar] [CrossRef]
- Herold, K.C.; Usmani-Brown, S.; Ghazi, T.; Lebastchi, J.; Beam, C.A.; Bellin, M.D.; Ledizet, M.; Sosenko, J.M.; Krischer, J.P.; Palmer, J.P.; et al. Beta cell death and dysfunction during type 1 diabetes development in at-risk individuals. J. Clin. Investig. 2015, 125, 1163–1173. [Google Scholar] [CrossRef]
- Mahon, J.L.; Sosenko, J.M.; Rafkin-Mervis, L.; Krause-Steinrauf, H.; Lachin, J.M.; Thompson, C.; Bingley, P.J.; Bonifacio, E.; Palmer, J.P.; Eisenbarth, G.S.; et al. The TrialNet Natural History Study of the Development of Type 1 Diabetes: Objectives, design, and initial results. Pediatric Diabetes 2009, 10, 97–104. [Google Scholar] [CrossRef]
- Skyler, J.S.; Greenbaum, C.J.; Lachin, J.M.; Leschek, E.; Rafkin-Mervis, L.; Savage, P.; Spain, L.; Type 1 Diabetes TrialNet Study Group. Type 1 Diabetes TrialNet—An international collaborative clinical trials network. Ann. N. Y. Acad. Sci. 2008, 1150, 14–24. [Google Scholar] [CrossRef]
- Vehik, K.; Cuthbertson, D.; Ruhlig, H.; Schatz, D.A.; Peakman, M.; Krischer, J.P.; Type 1 Diabetes TrialNet Study Group. Long-term outcome of individuals treated with oral insulin: Diabetes prevention trial-type 1 (DPT-1) oral insulin trial. Diabetes Care 2011, 34, 1585–1590. [Google Scholar] [CrossRef]
- Wilcox, N.S.; Rui, J.; Hebrok, M.; Herold, K.C. Life and death of beta cells in Type 1 diabetes: A comprehensive review. J. Autoimmun. 2016, 71, 51–58. [Google Scholar] [CrossRef]
- Michels, A.W.; Landry, L.G.; McDaniel, K.A.; Yu, L.; Campbell-Thompson, M.; Kwok, W.W.; Jones, K.L.; Gottlieb, P.A.; Kappler, J.W.; Tang, Q.; et al. Islet-Derived CD4 T Cells Targeting Proinsulin in Human Autoimmune Diabetes. Diabetes 2017, 66, 722–734. [Google Scholar] [CrossRef]
- Spanier, J.A.; Sahli, N.L.; Wilson, J.C.; Martinov, T.; Dileepan, T.; Burrack, A.L.; Finger, E.B.; Blazar, B.R.; Michels, A.W.; Moran, A.; et al. Increased Effector Memory Insulin-Specific CD4(+) T Cells Correlate With Insulin Autoantibodies in Patients With Recent-Onset Type 1 Diabetes. Diabetes 2017, 66, 3051–3060. [Google Scholar] [CrossRef]
- Xu, P.; Beam, C.A.; Cuthbertson, D.; Sosenko, J.M.; Skyler, J.S.; Krischer, J.P.; Type 1 Diabetes TrialNet Study Group. Prognostic accuracy of immunologic and metabolic markers for type 1 diabetes in a high-risk population: Receiver operating characteristic analysis. Diabetes Care 2012, 35, 1975–1980. [Google Scholar] [CrossRef]
- Hao, W.; Gitelman, S.; DiMeglio, L.A.; Boulware, D.; Greenbaum, C.J.; Type 1 Diabetes TrialNet Study Group. Fall in C-Peptide During First 4 Years From Diagnosis of Type 1 Diabetes: Variable Relation to Age, HbA1c, and Insulin Dose. Diabetes Care 2016, 39, 1664–1670. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Robles, D.T.; Abiru, N.; Kaur, P.; Rewers, M.; Kelemen, K.; Eisenbarth, G.S. Early expression of antiinsulin autoantibodies of humans and the NOD mouse: Evidence for early determination of subsequent diabetes. Proc. Natl. Acad. Sci. USA 2000, 97, 1701–1706. [Google Scholar] [CrossRef] [Green Version]
- Bonifacio, E.; Yu, L.; Williams, A.K.; Eisenbarth, G.S.; Bingley, P.J.; Marcovina, S.M.; Adler, K.; Ziegler, A.G.; Mueller, P.W.; Schatz, D.A.; et al. Harmonization of glutamic acid decarboxylase and islet antigen-2 autoantibody assays for national institute of diabetes and digestive and kidney diseases consortia. J. Clin. Endocrinol. Metab. 2010, 95, 3360–3367. [Google Scholar] [CrossRef]
- Wenzlau, J.M.; Juhl, K.; Yu, L.; Moua, O.; Sarkar, S.A.; Gottlieb, P.; Rewers, M.; Eisenbarth, G.S.; Jensen, J.; Davidson, H.W.; et al. The cation efflux transporter ZnT8 (Slc30A8) is a major autoantigen in human type 1 diabetes. Proc. Natl. Acad. Sci. USA 2007, 104, 17040–17045. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Miao, D.; Scrimgeour, L.; Johnson, K.; Rewers, M.; Eisenbarth, G.S. Distinguishing persistent insulin autoantibodies with differential risk: Nonradioactive bivalent proinsulin/insulin autoantibody assay. Diabetes 2012, 61, 179–186. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Gender, female | 29 (51%) |
| Age at T1D diagnosis, median (25th, 75th percentile) | 15.3 (10.8, 19) |
| Race/Ethnicity | |
| White | 48 (84%) |
| Hispanic | 4 (7%) |
| other | 5 (9%) |
| Unmethylated insulin ratio (mean ± SD) | 0.22 ± 0.13 |
| Antibody status (RIA) | |
| Antibody negative | 8 (15%) |
| Single antibody positive | 17 (32%) |
| ≥2 antibody positive | 29 (53%) |
| GADA positive | 32 (70%) |
| IA-2A positive | 30 (65%) |
| mIAA positive | 13 (24%) |
| ZnT8A positive | 24 (65%) |
| Antibody status (ECL) | |
| ≥single antibody positive | 45 (85%) |
| GADA positive | 22 (42%) |
| IA-2A positive | 18 (34%) |
| mIAA positive | 13 (25%) |
| Variable | Slope | Standard Error | p-Value |
|---|---|---|---|
| GADA | −0.021 | 0.021 | 0.3337 |
| IA-2A | 0.048 | 0.019 | 0.0142 |
| mIAA | 0.059 | 0.019 | 0.003 |
| ZnT8A | 0.012 | 0.024 | 0.6179 |
| ECL-GADA | 0.025 | 0.017 | 0.1425 |
| ECL-IA-2A | 0.027 | 0.022 | 0.2339 |
| ECL-IAA | 0.102 | 0.031 | 0.002 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simmons, K.M.; Fouts, A.; Pyle, L.; Clark, P.; Dong, F.; Yu, L.; Usmani-Brown, S.; Gottlieb, P.; Herold, K.C.; Steck, A.K.; et al. Unmethylated Insulin as an Adjunctive Marker of Beta Cell Death and Progression to Type 1 Diabetes in Participants at Risk for Diabetes. Int. J. Mol. Sci. 2019, 20, 3857. https://doi.org/10.3390/ijms20163857
Simmons KM, Fouts A, Pyle L, Clark P, Dong F, Yu L, Usmani-Brown S, Gottlieb P, Herold KC, Steck AK, et al. Unmethylated Insulin as an Adjunctive Marker of Beta Cell Death and Progression to Type 1 Diabetes in Participants at Risk for Diabetes. International Journal of Molecular Sciences. 2019; 20(16):3857. https://doi.org/10.3390/ijms20163857
Chicago/Turabian StyleSimmons, Kimber M., Alexandra Fouts, Laura Pyle, Pamela Clark, Fran Dong, Liping Yu, Sahar Usmani-Brown, Peter Gottlieb, Kevan C. Herold, Andrea K. Steck, and et al. 2019. "Unmethylated Insulin as an Adjunctive Marker of Beta Cell Death and Progression to Type 1 Diabetes in Participants at Risk for Diabetes" International Journal of Molecular Sciences 20, no. 16: 3857. https://doi.org/10.3390/ijms20163857