A Noninvasive Test for MicroRNA Expression in Oral Squamous Cell Carcinoma

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Material and Methods
4.1. Ethics Statement
4.2. Sample Collection
4.3. Oral Brushing Method
4.4. RNA Isolation and cDNA Synthesis
4.5. miRNA Expression
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Braakhuis, B.J.; Tabor, M.P.; Leemans, C.R.; van der Waal, I.; Snow, G.B.; Brakenhoff, R.H. Second primary tumors and field cancerization in oral and oropharyngeal cancer: Molecular techniques provide new insights and definitions. Head Neck 2002, 24, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.H.; Ozsahin, M.; Zhang, G.N.; Touboul, E.; De Vataire, F.; Andolenko, P.; Lacau-Saint-Guily, J.; Laugier, A.; Schlienger, M. Synchronous and metachronous head and neck carcinomas. Cancer 1994, 74, 1933–1938. [Google Scholar] [CrossRef] [Green Version]
- Hunter, T. Cooperation between oncogenes. Cell 1991, 64, 249–270. [Google Scholar] [CrossRef]
- Bishop, J.M. Molecular themes in oncogenesis. Cell 1991, 64, 235–248. [Google Scholar] [CrossRef]
- Min, A.; Zhu, C.; Peng, S.; Rajthala, S.; Costea, D.E.; Sapkota, D. MicroRNAs as Important Players and Biomarkers in Oral Carcinogenesis. BioMed Res. Int. 2015, 2015, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blenkiron, C.; Miska, E.A. miRNAs in cancer: Approaches, aetiology, diagnostics and therapy. Hum. Mol. Genet. 2007, 16, R106–R113. [Google Scholar] [CrossRef] [PubMed]
- Cowland, J.B.; Hother, C.; Gronbaek, K. MicroRNAs and cancer. APMIS 2007, 115, 1090–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambros, V. The functions of animal microRNAs. Nature 2004, 431, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Harfe, B.D. MicroRNAs in vertebrate development. Curr. Opin. Genet. Dev. 2005, 15, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Maaskola, J.; Siegal, M.L.; Rajewsky, N. Reexamining microRNA site accessibility in Drosophila: A population genomics study. PLoS ONE 2009, 4, e5681. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Z. MicroRNAs as oncogenes and tumor suppressors. N. Engl. J. Med. 2005, 353, 1768–1771. [Google Scholar] [CrossRef] [PubMed]
- Calin, G.A.; Sevignani, C.; Dumitru, C.D.; Hyslop, T.; Noch, E.; Yendamuri, S.; Shimizu, M.; Rattan, S.; Bullrich, F.; Negrini, M.; et al. Human microRNA genes are frequently located at fragile sites and genomic regions involved in cancers. Proc. Natl. Acad. Sci. USA 2004, 101, 2999–3004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calin, G.A.; Croce, C.M. MicroRNA signatures in human cancers. Nat. Rev. Cancer 2006, 6, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Cervigne, N.K.; Reis, P.P.; Machado, J.; Sadikovic, B.; Bradley, G.; Galloni, N.N.; Pintilie, M.; Jurisica, I.; Perez-Ordonez, B.; Gilbert, R.; et al. Identification of a microRNA signature associated with progression of leukoplakia to oral carcinoma. Hum. Mol. Genet. 2009, 18, 4818–4829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brito, J.A.; Gomes, C.C.; Guimaraes, A.L.; Campos, K.; Gomez, R.S. Relationship between microRNA expression levels and histopathological features of dysplasia in oral leukoplakia. J. Oral Pathol. Med. 2014, 43, 211–216. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Chen, Z.; Cabay, R.J.; Zhang, L.; Luan, X.; Chen, D.; Yu, T.; Wang, A.; Zhou, X. microRNA-21 and microRNA-375 from oral cytology as biomarkers for oral tongue cancer detection. Oral Oncol. 2016, 57, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, P.S.; Chang, K.W.; Kao, S.Y.; Chu, T.H.; Liu, C.J.; Lin, S.C. Association between the rs2910164 polymorphism in pre-miR-146a and oral carcinoma progression. Oral Oncol. 2012, 48, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Johnson, J.J.; Jiang, R.; Liu, Y.; Stack, M.S. Decrease of miR-146a is associated with the aggressiveness of human oral squamous cell carcinoma. Arch. Oral Biol. 2015, 60, 1416–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, L.; Huang, Y.; Zheng, Y.; Lyu, M.; Zhang, C.; Meng, Z.; Gan, Y.; Yu, G. miR-375 inhibits cell growth and correlates with clinical outcomes in tongue squamous cell carcinoma. Oncol. Rep. 2015, 33, 2061–2071. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Yang, J.; Li, S.; Shan, X.; Liu, X.; Hua, H.; Zhao, C.; Feng, Z.; Cai, Z.; Zhang, L.; et al. Potential involvement of miR-375 in the premalignant progression of oral squamous cell carcinoma mediated via transcription factor KLF5. Oncotarget 2015, 6, 40172–40185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.; Jadhav, K.; Shah, V.; Gupta, N.; Dagrus, K. miRNA 21: Diagnostic Prognostic and Therapeutic Marker for Oral Cancer. Microrna 2016, 5, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.C.; Hung, P.S.; Wang, P.W.; Liu, C.J.; Chu, T.H.; Cheng, H.W.; Lin, S.C. miR-181 as a putative biomarker for lymph-node metastasis of oral squamous cell carcinoma. J. Oral Pathol. Med. 2011, 40, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Tsay, J.C.; Li, Z.; Yie, T.A.; Wu, F.; Segal, L.; Greenberg, A.K.; Leibert, E.; Weiden, M.D.; Pass, H.; Munger, J.; et al. Molecular characterization of the peripheral airway field of cancerization in lung adenocarcinoma. PLoS ONE 2015, 10, e0118132. [Google Scholar] [CrossRef] [PubMed]
- Boldrup, L.; Coates, P.J.; Laurell, G.; Wilms, T.; Fahraeus, R.; Nylander, K. Downregulation of miRNA-424: A sign of field cancerisation in clinically normal tongue adjacent to squamous cell carcinoma. Br. J. Cancer 2015, 112, 1760–1765. [Google Scholar] [CrossRef] [PubMed]
- Wali, R.K.; Hensing, T.A.; Ray, D.W.; Dela Cruz, M.; Tiwari, A.K.; Radosevich, A.; Jepeal, L.; Fernando, H.C.; Litle, V.R.; Charlot, M.; et al. Buccal microRNA dysregulation in lung field carcinogenesis: Gender-specific implications. Int. J. Oncol. 2014, 45, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.J.; Zhang, C.Y.; Zhou, Z.T.; Ma, J.Y.; Liu, Y.; Bao, Z.X.; Jiang, W.W. MicroRNA-155 in oral squamous cell carcinoma: Overexpression, localization, and prognostic potential. Head Neck 2015, 37, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Cabay, R.J.; Jin, Y.; Wang, A.; Lu, Y.; Shah-Khan, M.; Zhou, X. MicroRNA Deregulations in Head and Neck Squamous Cell Carcinomas. J. Oral Maxillofac. Res. 2013, 4, e2. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.H.; Xiong, X.P.; Jia, J.; Zhang, W.F. MicroRNAs: New actors in the oral cancer scene. Oral Oncol. 2011, 47, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Boldrup, L.; Ardito, F.; Gu, X.; Lo Muzio, L.; Nylander, K. Circulating miRNAs from blood, plasma or serum as promising clinical biomarkers in oral squamous cell carcinoma: A systematic review of current findings. Oral Oncol. 2016, 63, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Wang, X.; Veno, M.T.; Bakholdt, V.; Sorensen, J.A.; Krogdahl, A.; Sun, Z.; Gao, S.; Kjems, J. Circulating miRNAs as biomarkers for oral squamous cell carcinoma recurrence in operated patients. Oncotarget 2017. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Kolokythas, A.; Schwartz, J.L.; Epstein, J.B.; Adami, G.R. microRNA from brush biopsy to characterize oral squamous cell carcinoma epithelium. Cancer Med. 2016, 6, 67–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinkmann, O.; Wong, D.T. Salivary transcriptome biomarkers in oral squamous cell cancer detection. Adv. Clin. Chem. 2011, 55, 21–34. [Google Scholar] [PubMed]
- Duz, M.B.; Karatas, O.F.; Guzel, E.; Turgut, N.F.; Yilmaz, M.; Creighton, C.J.; Ozen, M. Identification of miR-139-5p as a saliva biomarker for tongue squamous cell carcinoma: A pilot study. Cell. Oncol. 2016, 39, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.; Alevizos, I. Isolation of circulating microRNA in saliva. Methods Mol. Biol. 2013, 1024, 183–190. [Google Scholar] [PubMed]
- Langevin, S.M.; Stone, R.A.; Bunker, C.H.; Grandis, J.R.; Sobol, R.W.; Taioli, E. MicroRNA-137 promoter methylation in oral rinses from patients with squamous cell carcinoma of the head and neck is associated with gender and body mass index. Carcinogenesis 2010, 31, 864–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.J.; Kao, S.Y.; Tu, H.F.; Tsai, M.M.; Chang, K.W.; Lin, S.C. Increase of microRNA miR-31 level in plasma could be a potential marker of oral cancer. Oral Dis. 2010, 16, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.J.; Lin, S.C.; Yang, C.C.; Cheng, H.W.; Chang, K.W. Exploiting salivary miR-31 as a clinical biomarker of oral squamous cell carcinoma. Head Neck 2012, 34, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Momen-Heravi, F.; Trachtenberg, A.J.; Kuo, W.P.; Cheng, Y.S. Genomewide Study of Salivary MicroRNAs for Detection of Oral Cancer. J. Dent. Res. 2014, 93, 86S–93S. [Google Scholar] [CrossRef] [PubMed]
- Park, N.J.; Zhou, H.; Elashoff, D.; Henson, B.S.; Kastratovic, D.A.; Abemayor, E.; Wong, D.T. Salivary microRNA: Discovery, characterization, and clinical utility for oral cancer detection. Clin. Cancer Res. 2009, 15, 5473–5477. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Chen, Z.; Shi, S.; Wang, X.; Wang, W.; Li, N.; Wang, J. Clinical Diagnostic Implications of Body Fluid miRNA in Oral Squamous Cell Carcinoma: A Meta-Analysis. Medicine 2015, 94, e1324. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, Y.X.; Yang, X.; Jiang, L.; Zhou, Z.J.; Zhu, Y.Q. Progress risk assessment of oral premalignant lesions with saliva miRNA analysis. BMC Cancer 2013, 13, 129. [Google Scholar] [CrossRef] [PubMed]
- Zahran, F.; Ghalwash, D.; Shaker, O.; Al-Johani, K.; Scully, C. Salivary microRNAs in oral cancer. Oral Dis. 2015, 21, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Prasad, G.; Seers, C.; Reynolds, E.; McCullough, M.J. The assessment of the robustness of microRNAs from oral cytological scrapings. J. Oral Pathol. Med. 2017, 46, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Bremmer, J.F.; Braakhuis, B.J.; Ruijter-Schippers, H.J.; Brink, A.; Duarte, H.M.; Kuik, D.J.; Bloemena, E.; Leemans, C.R.; van der Waal, I.; Brakenhoff, R.H. A noninvasive genetic screening test to detect oral preneoplastic lesions. Lab. Investig. 2005, 85, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.E.; Fernandes, L.P.; Cantarutti, A.L.; Oyama, C.N.; Figueiredo, P.T.; Guerra, E.N. Assessing oral brushing technique as a source to collect DNA and its use in detecting human papillomavirus. Pathol. Res. Pract. 2013, 209, 291–295. [Google Scholar] [CrossRef] [PubMed]
- De Biase, D.; Visani, M.; Morandi, L.; Marucci, G.; Taccioli, C.; Cerasoli, S.; Baruzzi, A.; Pession, A. miRNAs expression analysis in paired fresh/frozen and dissected formalin fixed and paraffin embedded glioblastoma using real-time pCR. PLoS ONE 2012, 7, e35596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morandi, L.; Gissi, D.; Tarsitano, A.; Asioli, S.; Gabusi, A.; Marchetti, C.; Montebugnoli, L.; Foschini, M.P. CpG location and methylation level are crucial factors for the early detection of oral squamous cell carcinoma in brushing samples using bisulfite sequencing of a 13-gene panel. Clin. Epigenetics 2017, 9, 85. [Google Scholar] [CrossRef] [PubMed]
- Morandi, L.; Gissi, D.; Tarsitano, A.; Asioli, S.; Monti, V.; Del Corso, G.; Marchetti, C.; Montebugnoli, L.; Foschini, M.P. DNA methylation analysis by bisulfite next-generation sequencing for early detection of oral squamous cell carcinoma and high-grade squamous intraepithelial lesion from oral brushing. J. Craniomaxillofac. Surg. 2015, 43, 1494–1500. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, D.P.; Southwick, H.W.; Smejkal, W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer 1953, 6, 963–968. [Google Scholar] [CrossRef]
- Braakhuis, B.J.; Tabor, M.P.; Kummer, J.A.; Leemans, C.R.; Brakenhoff, R.H. A genetic explanation of Slaughter’s concept of field cancerization: Evidence and clinical implications. Cancer Res. 2003, 63, 1727–1730. [Google Scholar] [PubMed]
- Montebugnoli, L.; Gissi, D.B.; Badiali, G.; Marchetti, C.; Cervellati, F.; Farnedi, A.; Foschini, M.P. Ki-67 from clinically and histologically “normal” distant mucosa as prognostic marker in early-stage (T1-T2N0) oral squamous cell carcinoma: A prospective study. J. Oral Maxillofac. Surg. 2011, 69, 2579–2584. [Google Scholar] [CrossRef] [PubMed]
- Myoung, H.; Kim, M.J.; Lee, J.H.; Ok, Y.J.; Paeng, J.Y.; Yun, P.Y. Correlation of proliferative markers (Ki-67 and PCNA) with survival and lymph node metastasis in oral squamous cell carcinoma: A clinical and histopathological analysis of 113 patients. Int. J. Oral Maxillofac. Surg. 2006, 35, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Gissi, D.B.; Gabusi, A.; Tarsitano, A.; Badiali, G.; Marchetti, C.; Morandi, L.; Foschini, M.P.; Montebugnoli, L. Ki67 Overexpression in mucosa distant from oral carcinoma: A poor prognostic factor in patients with long-term follow-up. J. Craniomaxillofac. Surg. 2016, 44, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Gissi, D.B.; Tarsitano, A.; Leonardi, E.; Gabusi, A.; Neri, F.; Marchetti, C.; Montebugnoli, L.; Foschini, M.P.; Morandi, L. Clonal analysis as a prognostic factor in multiple oral squamous cell carcinoma. Oral Oncol. 2017, 67, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Wu, H.; Wu, F.; Nie, D.; Sheng, S.; Mo, Y.Y. MicroRNA-21 targets tumor suppressor genes in invasion and metastasis. Cell Res. 2008, 18, 350–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, Z.; Liu, M.; Stribinskis, V.; Klinge, C.M.; Ramos, K.S.; Colburn, N.H.; Li, Y. MicroRNA-21 promotes cell transformation by targeting the programmed cell death 4 gene. Oncogene 2008, 27, 4373–4379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.F.; Li, K.K.; Gao, L.; Li, S.Z.; Chen, K.; Zhang, J.B.; Wang, D.; Tu, R.F.; Zhang, J.X.; Tao, K.X.; et al. miR-191 promotes tumorigenesis of human colorectal cancer through targeting C/EBPbeta. Oncotarget 2015, 6, 4144–4158. [Google Scholar] [PubMed]
- Hui, A.B.; Shi, W.; Boutros, P.C.; Miller, N.; Pintilie, M.; Fyles, T.; McCready, D.; Wong, D.; Gerster, K.; Waldron, L.; et al. Robust global micro-RNA profiling with formalin-fixed paraffin-embedded breast cancer tissues. Lab. Investig. 2009, 89, 597–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gombos, K.; Horvath, R.; Szele, E.; Juhasz, K.; Gocze, K.; Somlai, K.; Pajkos, G.; Ember, I.; Olasz, L. miRNA expression profiles of oral squamous cell carcinomas. Anticancer Res. 2013, 33, 1511–1517. [Google Scholar] [PubMed]
- Qin, S.; Zhu, Y.; Ai, F.; Li, Y.; Bai, B.; Yao, W.; Dong, L. MicroRNA-191 correlates with poor prognosis of colorectal carcinoma and plays multiple roles by targeting tissue inhibitor of metalloprotease 3. Neoplasma 2014, 61, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, P.S.; Liu, C.J.; Chou, C.S.; Kao, S.Y.; Yang, C.C.; Chang, K.W.; Chiu, T.H.; Lin, S.C. miR-146a enhances the oncogenicity of oral carcinoma by concomitant targeting of the IRAK1, TRAF6 and NUMB genes. PLoS ONE 2013, 8, e79926. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; He, R.; Ren, F.; Tang, R.; Chen, G. Association of miR-146a rs2910164 polymorphism with squamous cell carcinoma risk: A meta-analysis. J. BUON 2015, 20, 829–841. [Google Scholar] [PubMed]
- Palmieri, A.; Carinci, F.; Martinelli, M.; Pezzetti, F.; Girardi, A.; Cura, F.; Rubini, C.; Scapoli, L. Role of the miR146a polymorphism in the origin and progression of oral squamous cell carcinoma. Eur. J. Oral Sci. 2014, 122, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, L.; Yang, Y.; Xiao, X.; Wang, C.; Zhang, X.; Wang, L.; Li, W.; Zheng, G.; Wang, S.; Dong, Z. Sox2 nuclear expression is closely associated with poor prognosis in patients with histologically node-negative oral tongue squamous cell carcinoma. Oral Oncol. 2011, 47, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Fang, X.; Lou, X.; Hua, D.; Ding, W.; Foltz, G.; Hood, L.; Yuan, Y.; Lin, B. Silencing SOX2 induced mesenchymal-epithelial transition and its expression predicts liver and lymph node metastasis of CRC patients. PLoS ONE 2012, 7, e41335. [Google Scholar] [CrossRef] [PubMed]
- Tao, S.F.; He, H.F.; Chen, Q. Quercetin inhibits proliferation and invasion acts by up-regulating miR-146a in human breast cancer cells. Mol. Cell. Biochem. 2015, 402, 93–100. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO/IARC Classification of Tumours; El-Naggar, A.K.C.J., Grandis, J.R., Takata, T., Slootweg, P.J., Eds.; WHO: Geneva, Switzerland, 2018; Volume 9. [Google Scholar]
- Kademani, D.; Bell, R.B.; Bagheri, S.; Holmgren, E.; Dierks, E.; Potter, B.; Homer, L. Prognostic factors in intraoral squamous cell carcinoma: The influence of histologic grade. J. Oral Maxillofac. Surg. 2005, 63, 1599–1605. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| miRNAs | Smoke | Mean ∆−Ct | SD | Student t | p Value |
|---|---|---|---|---|---|
| miR-191 | yes | 4.9 | 3.5 | 0.5 | 0.6 |
| no | 4.4 | 3.7 | |||
| miR-21 | yes | −0.3 | 3.7 | −0.7 | 0.5 |
| no | 0.4 | 4.2 | |||
| miR-345 | yes | 3.2 | 3.5 | −0.5 | 0.6 |
| no | 3.7 | 3.7 | |||
| miR-146a | yes | 8.6 | 4.6 | 0.2 | 0.9 |
| no | 8.1 | 4.1 | |||
| miR-649 | yes | 8.7 | 1.7 | −0.3 | 0.7 |
| no | 9.0 | 2.9 | |||
| miR-518b | yes | 5.5 | 5.2 | −1.2 | 0.2 |
| no | 7.0 | 4.2 |
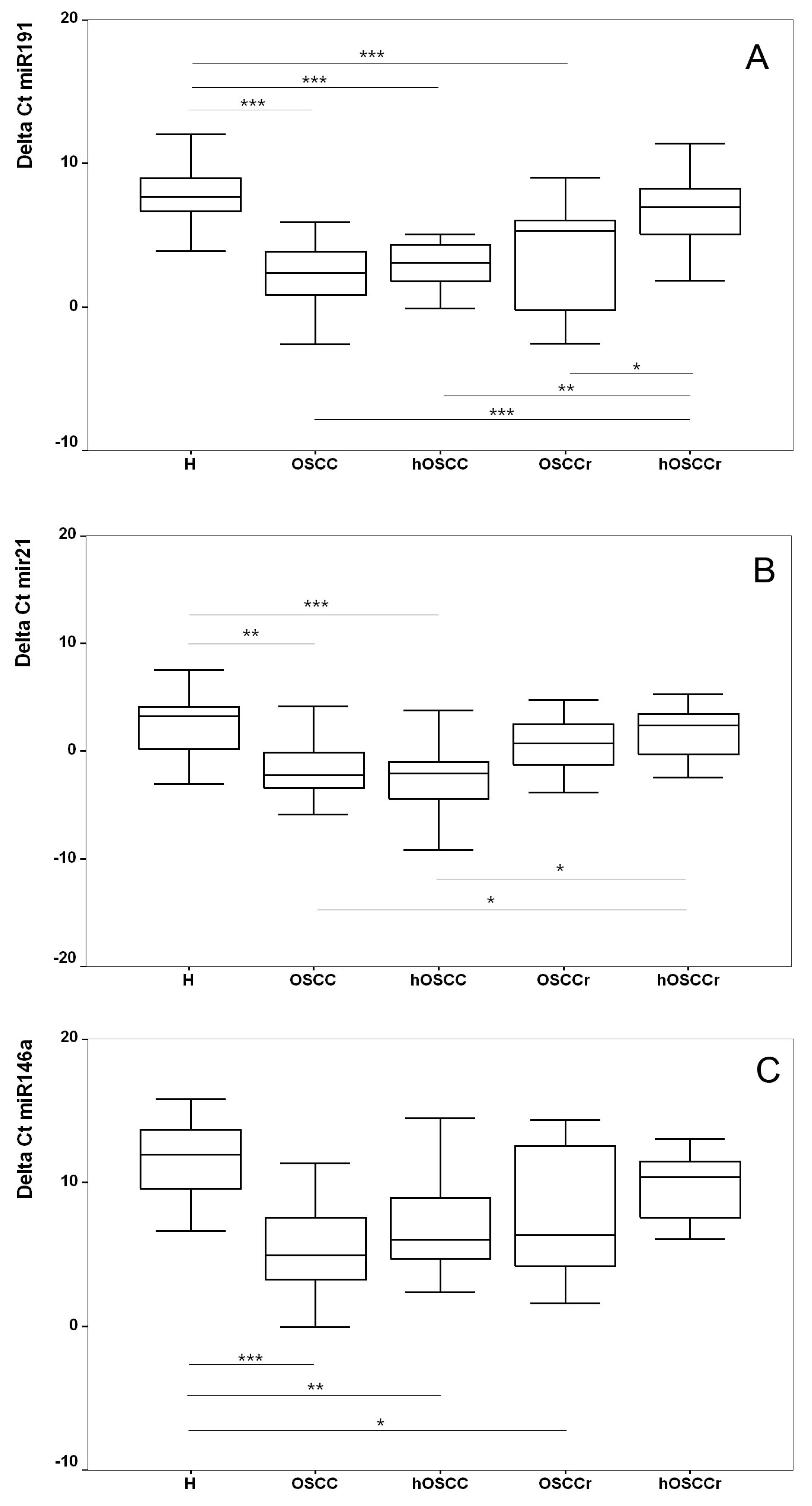
| miRNAs | Reference | Test Group | p Value | ∆∆−Ct | Fold Change |
|---|---|---|---|---|---|
| mir-191 | H | OSCC | < 0.001 * | −5.7 (95% CI −7.7; −3.6) | 50 (95% CI 12; 211) |
| H | hOSCC | < 0.001 * | −4.7 (95% CI −6.8; −2.7) | 27 (95% CI 6; 111) | |
| H | OSCCr | < 0.001 * | −4.2 (95% CI −6.4; −2.1) | 19 (95% CI 4; 82) | |
| H | hOSCCr | 0.632 | −1.0 (95% CI −3.2; 1.2) | 2 (95% CI 0.4; 9) | |
| mir-21 | H | OSCC | 0.002 * | −4.0 (95% CI −6.7; −1.3) | 16 (95% CI 2; 104) |
| H | hOSCC | < 0.001 * | −4.5 (95% CI −7.3; −1.7) | 23 (95% CI 3; 161) | |
| H | OSCCr | 0.770 | −1.1 (95% CI −3.9; 1.7) | 2 (95% CI 0.3; 15) | |
| H | hOSCCr | 0.992 | −0.4 (95% CI −3.3; 2.5) | 1.3 (95% CI 0.2; 10) | |
| mir-146a | H | OSCC | < 0.001 * | −5.7 (95% CI −8.8; −2.6) | 52 (95% CI 6; 452) |
| H | hOSCC | 0.003 * | −4.4 (95% CI −7.6; −1.2) | 22 (95% CI 2; 198) | |
| H | OSCCr | 0.020 * | −3.9 (95% CI −7.3; −0.5) | 15 (95% CI 1.4; 154) | |
| H | hOSCCr | 0.687 | −1.6 (95% CI −53; 2.1) | 3 (95% CI 0.2; 39) |
| Participants | N. | Sex | Mean Age | Smoker | Alcohol Consumption | T Stage | N Stage | Site of Brushing Specimen | |
|---|---|---|---|---|---|---|---|---|---|
| First | Second | ||||||||
| OSCC | 14 | 5 M, 9 F | 68.15 ± 13.09 | 5 Yes 9 No | 2 Yes 12 No | 6 T1 6 T2 2 T4 | 12 N0 2 N2 | 5 Cheek 5 Gingiva 4 Tongue | Opposite cheek |
| OSCCr | 13 | 4 M, 9 F | 58.9 ± 9.38 | 1 Yes 12 No | 1 Yes 11 No | 3 T1 6 T1 1 T3 3 T4 | 9 N0 1 N1 2 N2 1 N3 | 5 Tongue 3 Gingiva 4 Cheek 1 Floor of mouth | Opposite cheek |
| Healthy donors | 24 | 12 M, 12 F | 50.4 ± 18.6 | 8 Yes 16 No | 3 Yes 21 No | 8 Cheek 8 Gingiva 8 Tongue | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gissi, D.B.; Morandi, L.; Gabusi, A.; Tarsitano, A.; Marchetti, C.; Cura, F.; Palmieri, A.; Montebugnoli, L.; Asioli, S.; Foschini, M.P.; et al. A Noninvasive Test for MicroRNA Expression in Oral Squamous Cell Carcinoma. Int. J. Mol. Sci. 2018, 19, 1789. https://doi.org/10.3390/ijms19061789
Gissi DB, Morandi L, Gabusi A, Tarsitano A, Marchetti C, Cura F, Palmieri A, Montebugnoli L, Asioli S, Foschini MP, et al. A Noninvasive Test for MicroRNA Expression in Oral Squamous Cell Carcinoma. International Journal of Molecular Sciences. 2018; 19(6):1789. https://doi.org/10.3390/ijms19061789
Chicago/Turabian StyleGissi, Davide B., Luca Morandi, Andrea Gabusi, Achille Tarsitano, Claudio Marchetti, Francesca Cura, Annalisa Palmieri, Lucio Montebugnoli, Sofia Asioli, Maria P. Foschini, and et al. 2018. "A Noninvasive Test for MicroRNA Expression in Oral Squamous Cell Carcinoma" International Journal of Molecular Sciences 19, no. 6: 1789. https://doi.org/10.3390/ijms19061789