The Spatial Dimension of COVID-19: The Potential of Earth Observation Data in Support of Slum Communities with Evidence from Brazil

 ,
,  ,
,  , ,
, ,
Abstract
:
1. Introduction
- (a)
- Lack of basic services (e.g., clean water, sanitation and soap) which do not allow adherence to WHO guidelines for basic hygiene [18];
- (b)
- High density in both population and built environment that eliminate social distancing [19];
- (c)
- Access to work, livelihood, and food supply obligating dwellers to break social isolation recommendations (the informal economic section has been under particular threat by the lockdowns) [20];
- (d)
- The concentration of pre-existing health conditions such as chronic diseases (e.g., diabetes, hypertension [21], and respiratory diseases [22,23]) and infectious ones (e.g., malaria or leptospirosis [24]) because of poverty. Such vulnerabilities lead to a disease severity that requires an intensive care unit (ICU), and ultimately to mortality;
- (e)
- (f)
- (g)
- Limited access to information, public health facilities, and social or financial aid [29];
- (h)
- Community organizations and empowerment through local leadership and available infrastructure for humanitarian aid actions, such as schools, community centers, and religious buildings [4].

2. Materials and Methods
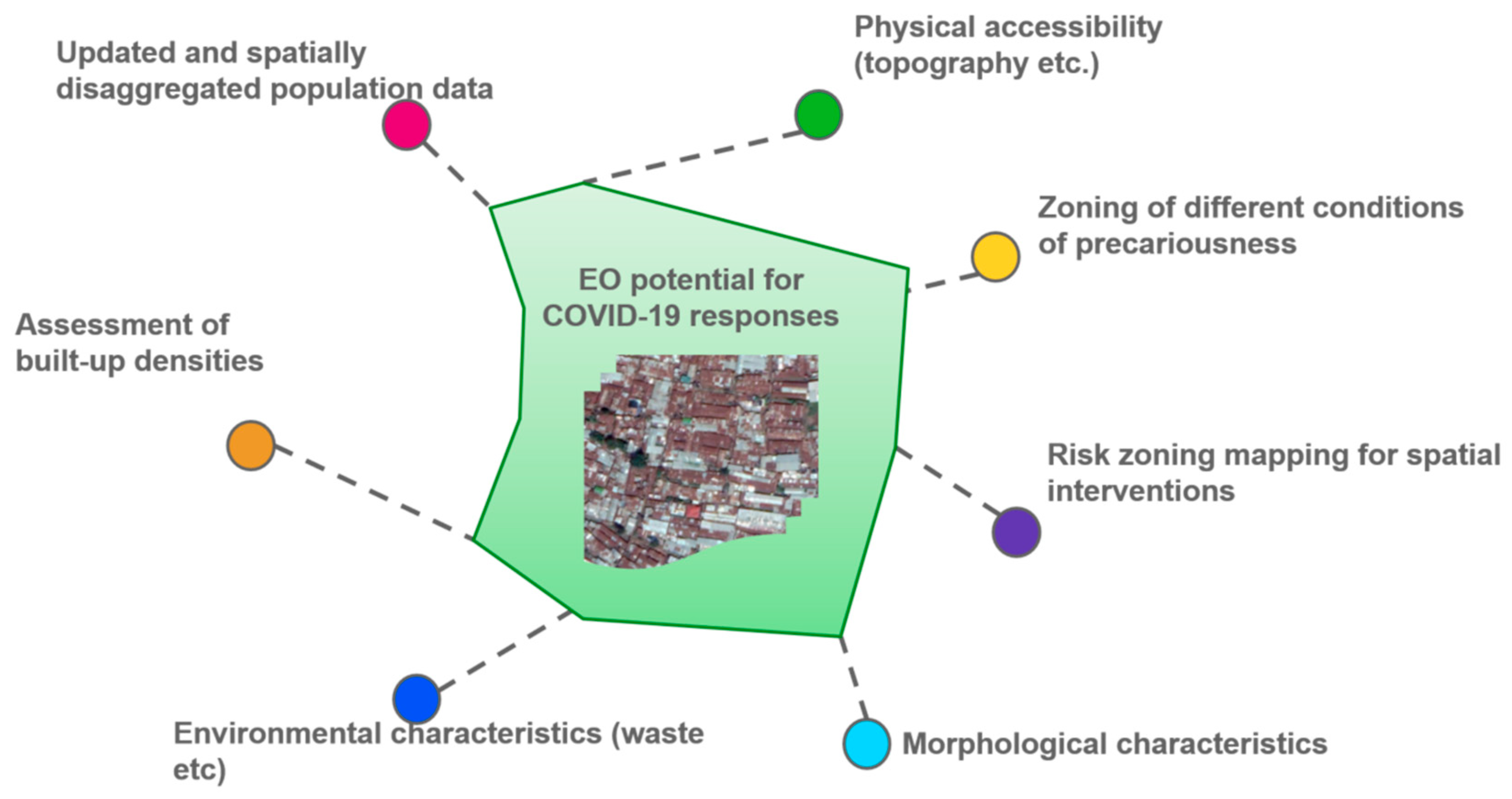
2.1. The Conceptual Frame of Information Needs and Spatial Data to Support COVID-19 Responses
- Static: distribution of spaces, such as dense buildings, narrow footpaths, and houses in flooding areas (water sinks). These are physical and environmental conditions (variables) potentially associated with a higher risk of COVID-19 transmission or morbidity.
- Dynamic: distribution of potential movements, e.g., the spatial relation between residents and work/money/water/food supply, which leads to possible exposure to COVID-19.
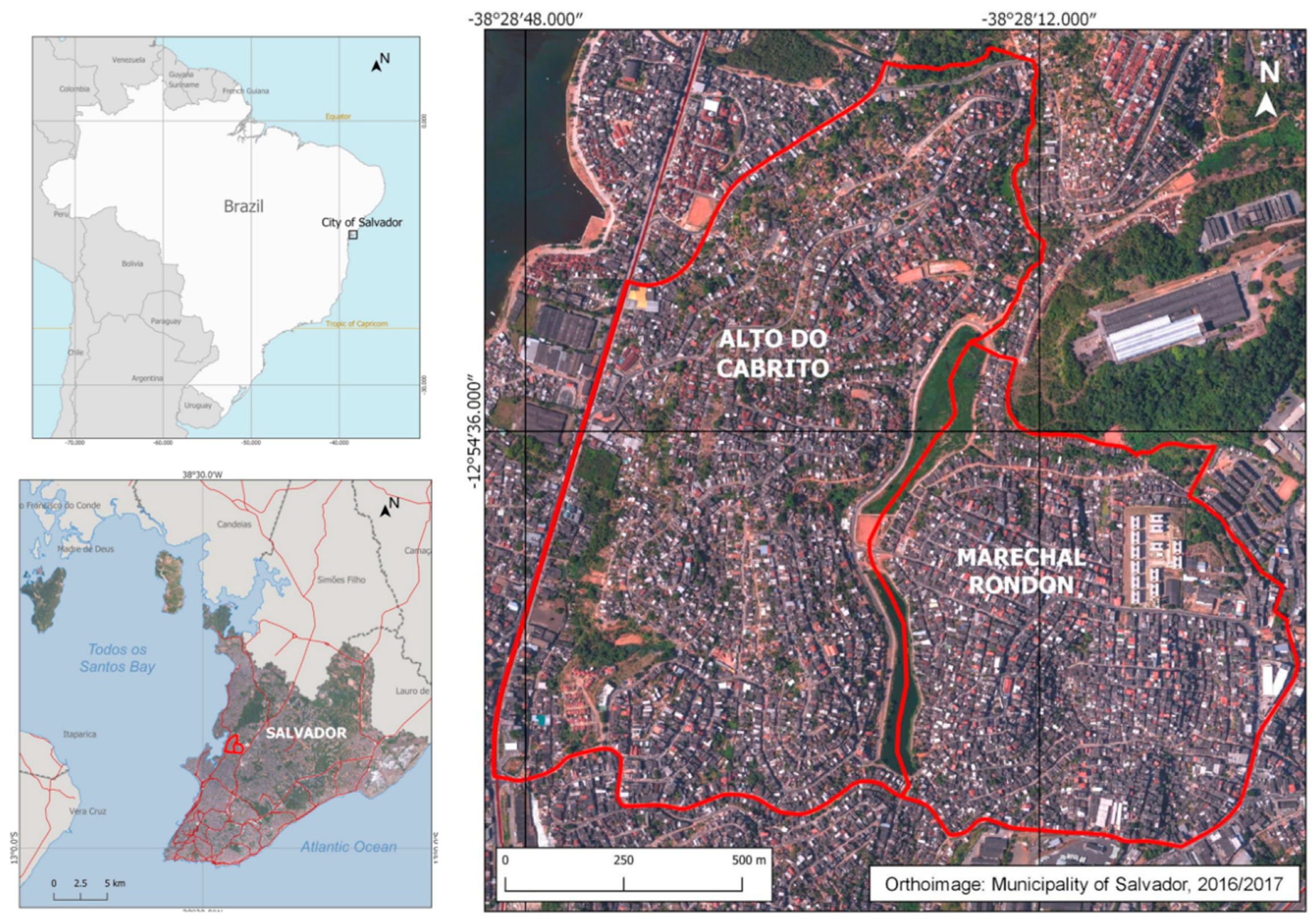
2.2. The Use Case of Spatial Data to Support COVID-19 Responses in Salvador, Brazil
- What are the key spatial (EO) data needed to understand physical variations (spatial patterns) of COVID-19 infections?
- What are the key spatial (EO) data needed to support local (municipal but also community-based) responses to prevent and respond to COVID-19 cases?
- What are the specific spatial (EO) data needed to support slum communities (e.g., to support community-based organizations)?
3. The Case of Salvador in Brazil
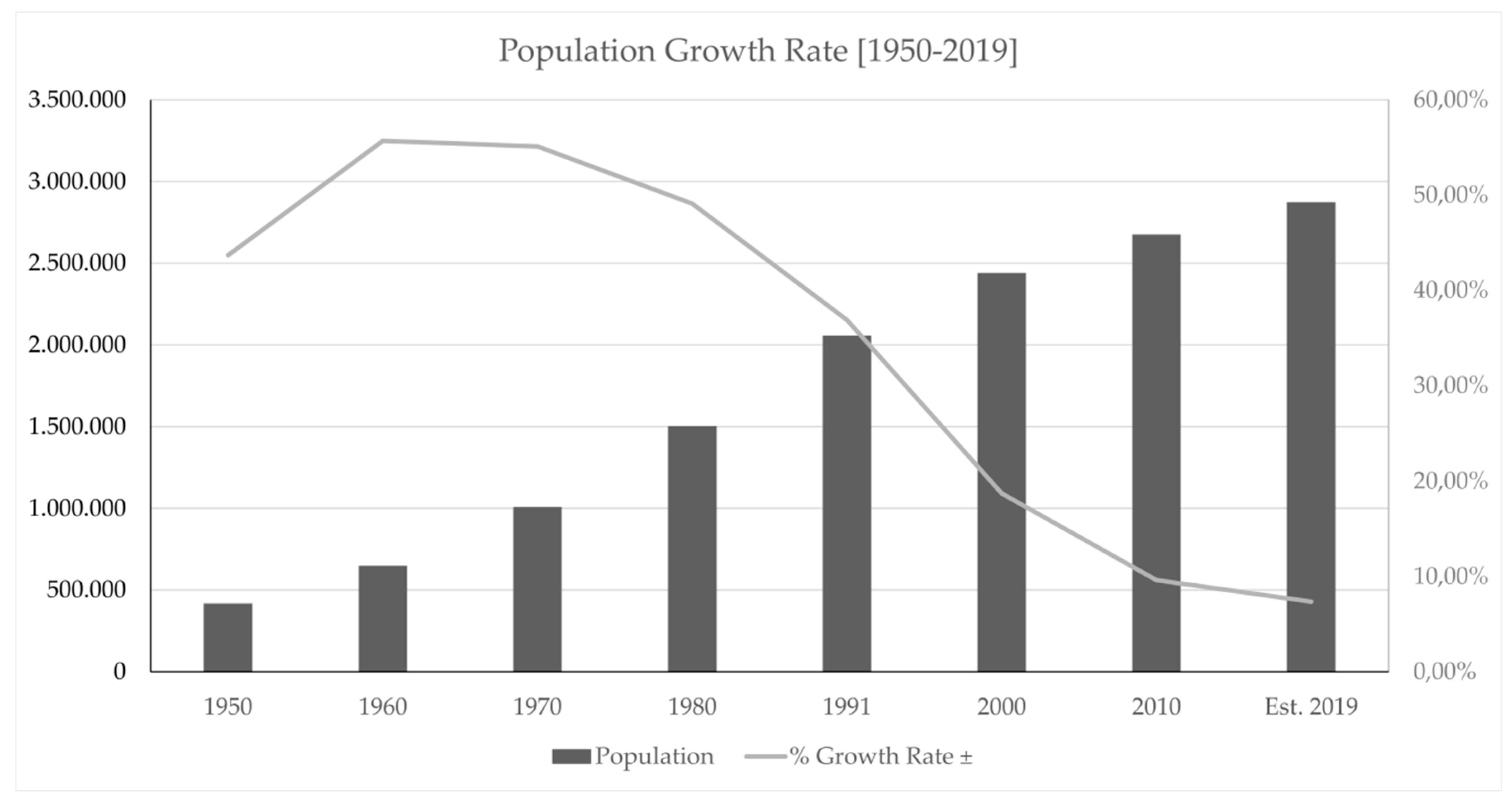
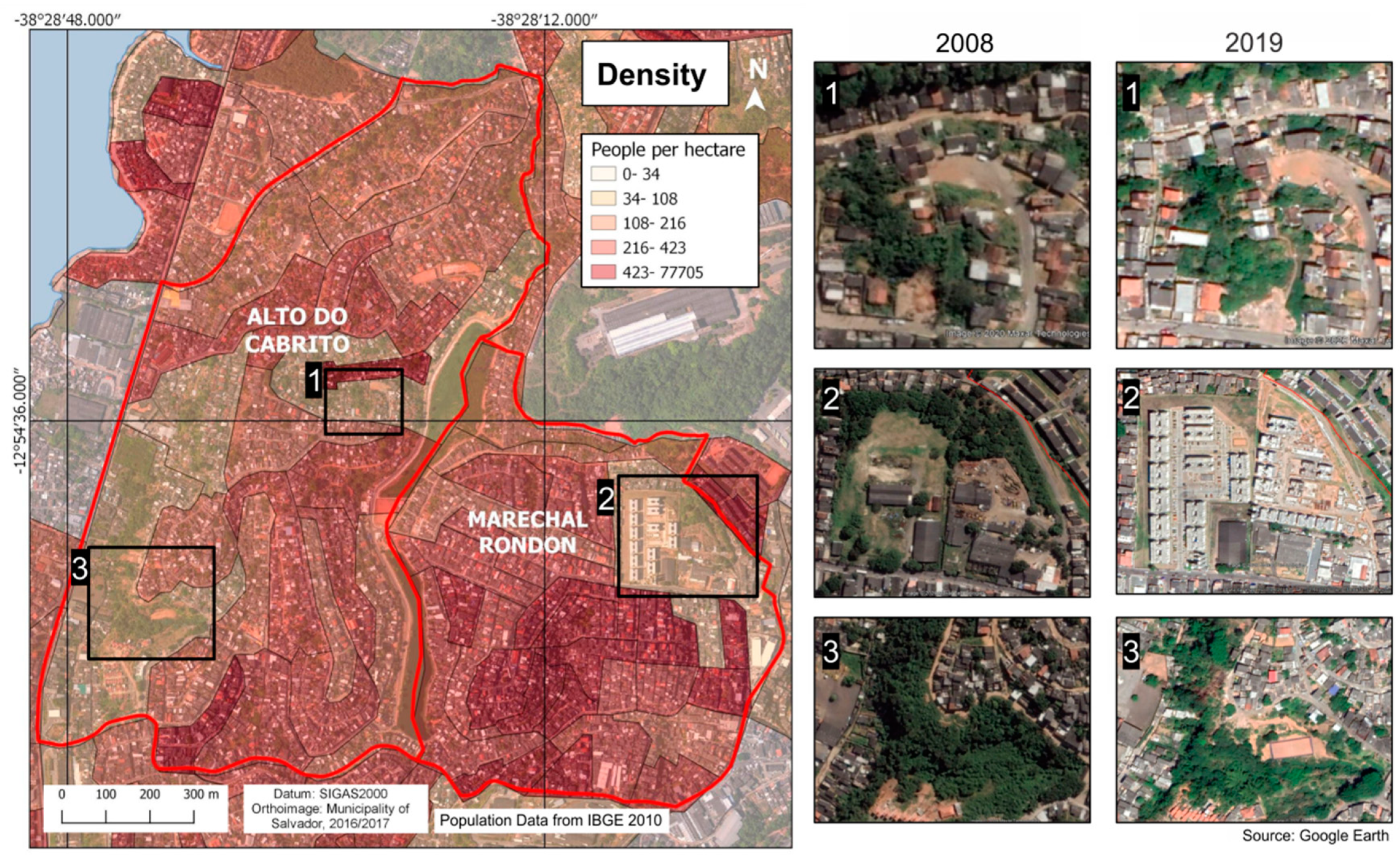
3.1. The General Context of Salvador
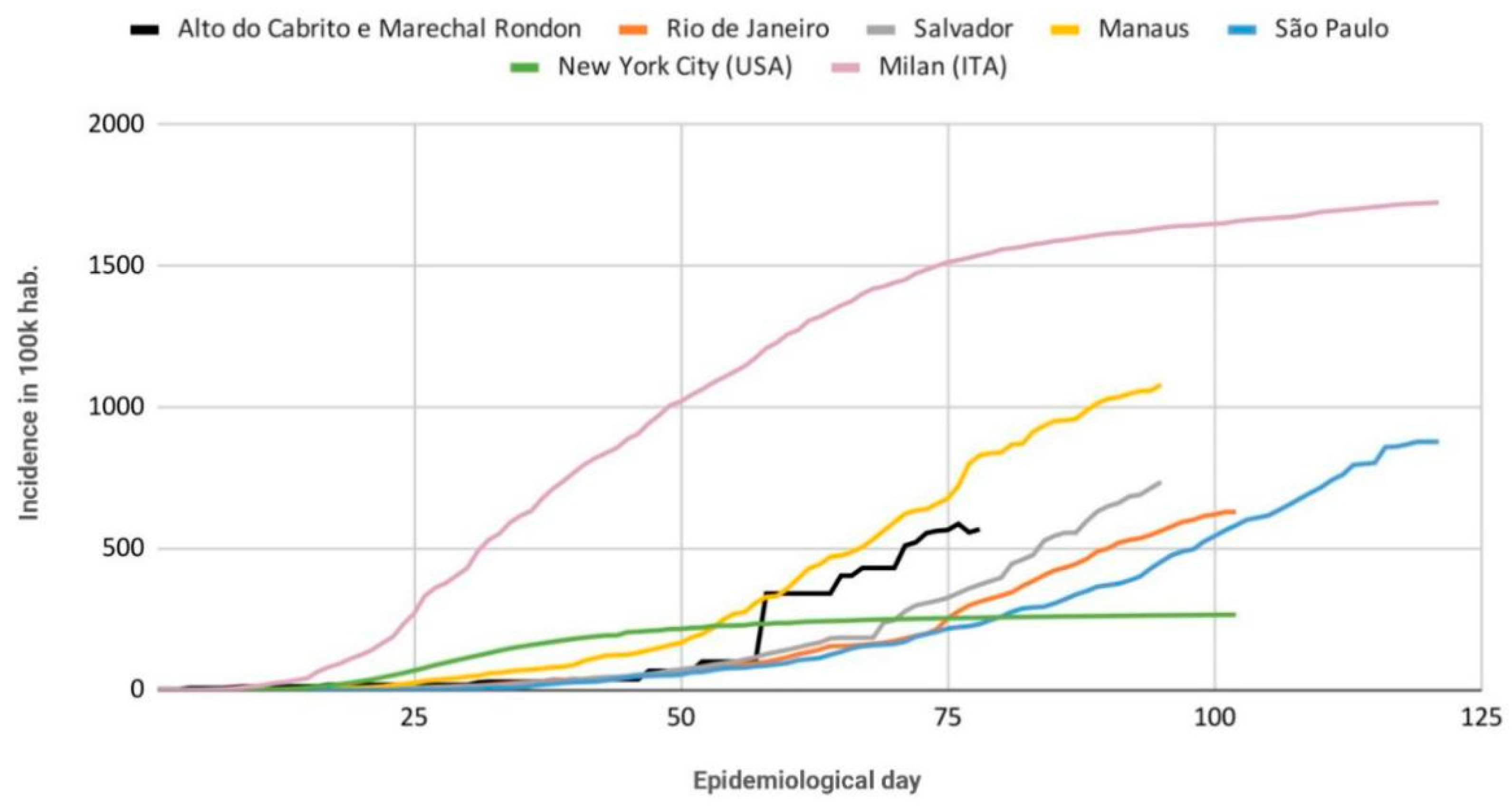
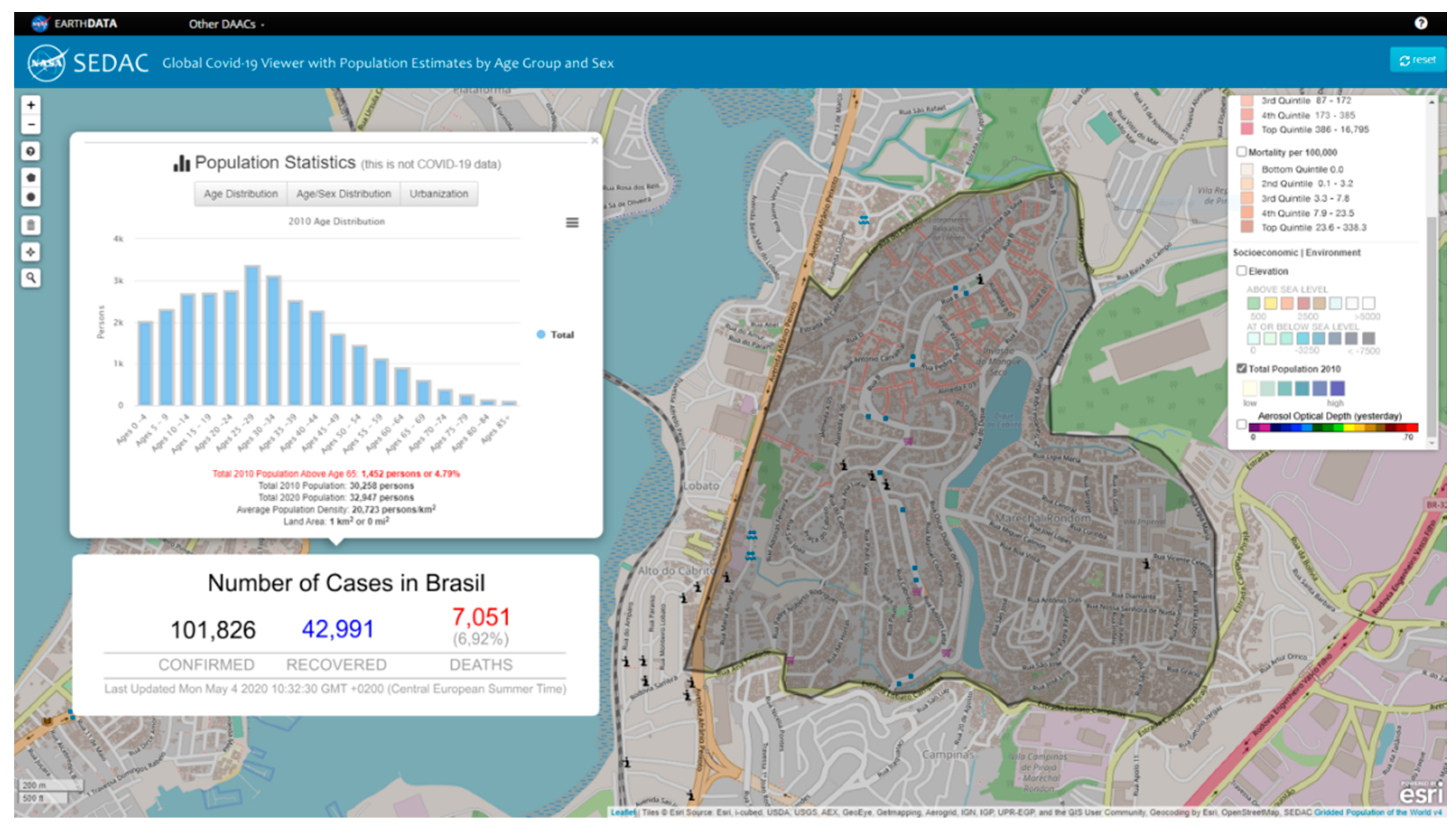
3.2. COVID-19 Crisis in Salvador
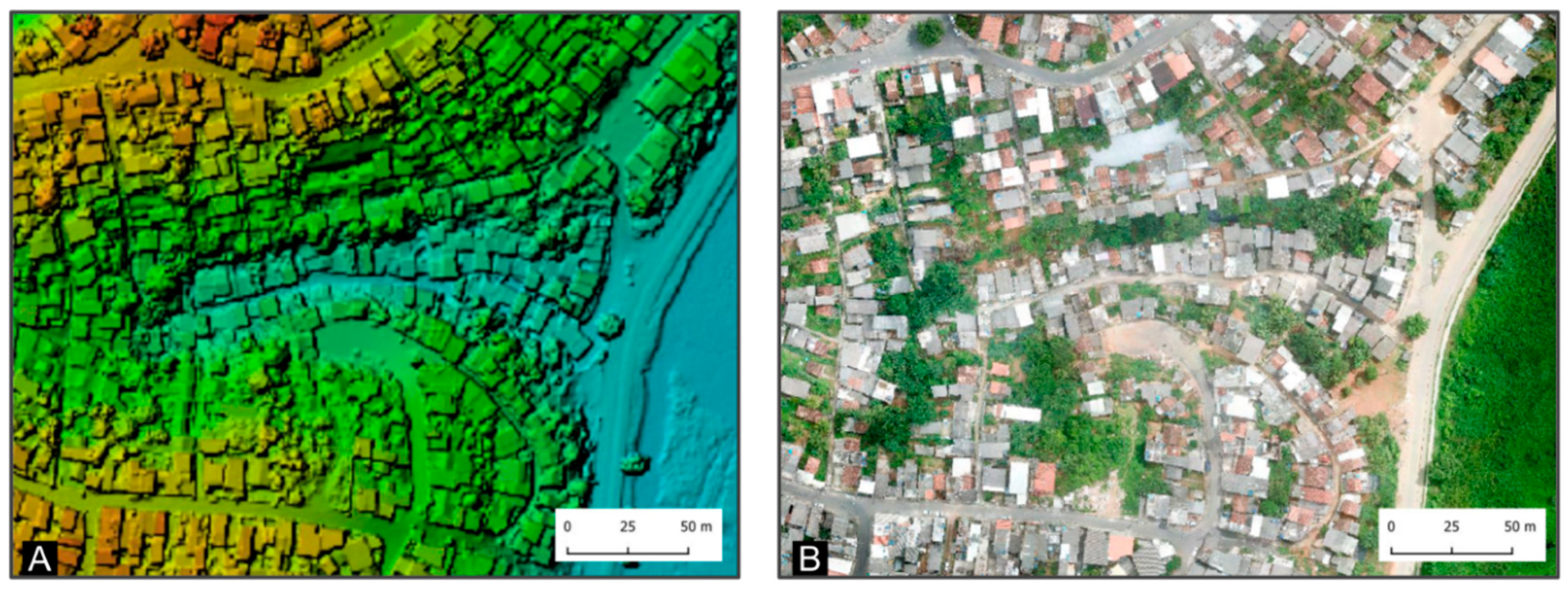
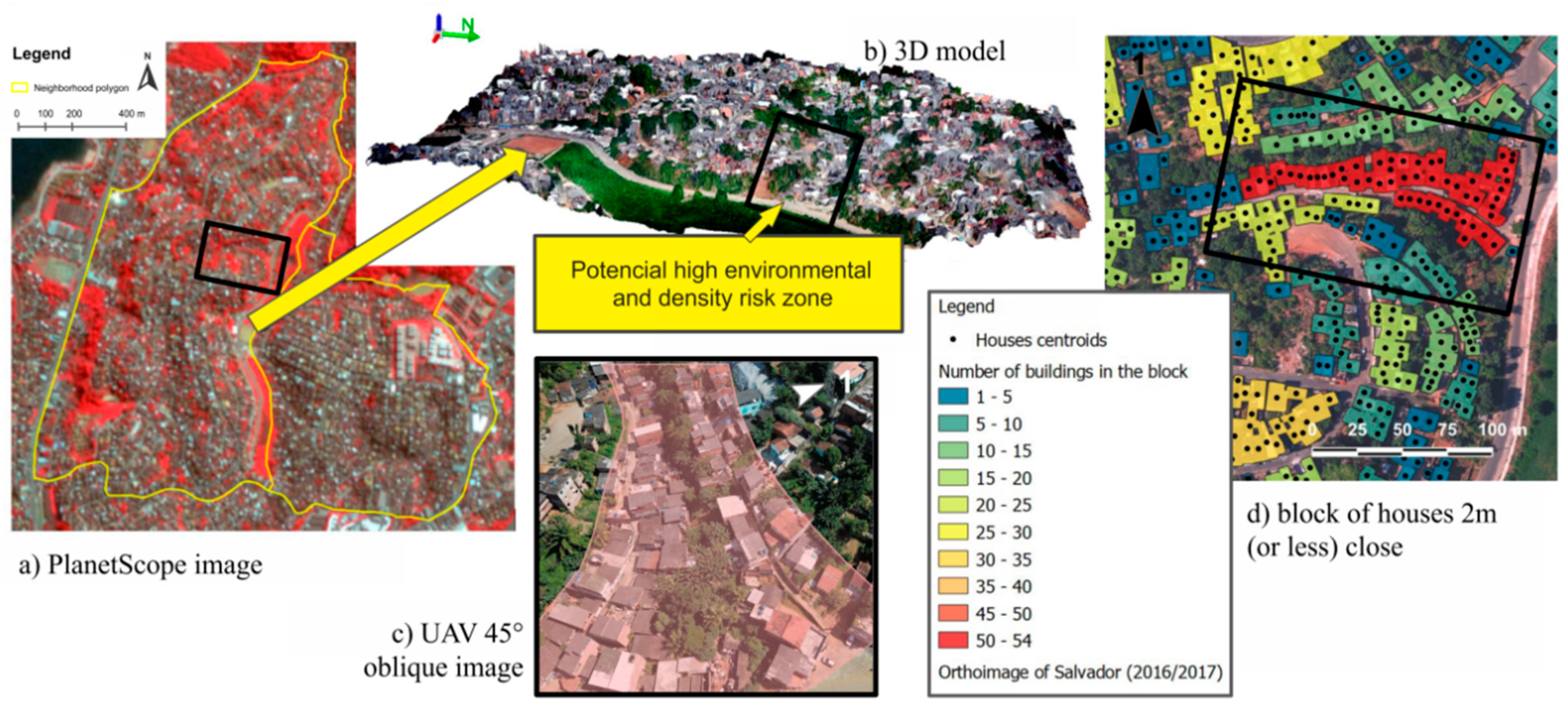
3.3. Examples of Spatial Data to Support COVID-19 Responses
4. Discussion
- (1)
- Rapid problem-oriented data acquirement;
- (2)
- Rapid and timely access to information encoding spatiotemporal dynamics of disease exposure in a household or area;
- (3)
- Assessment of the vulnerability level of an area or household in terms of information regarding density, facility accessibility, and environmental context;
- (4)
- Measurement of different aspects of vulnerability;
- (5)
- Estimation and prediction of the population at risk.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ghebreyesus, T.A. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 20 July 2020).
- Holden, M. COVID-19 Death Rate in Deprived Areas in England Double That of Better off Places: ONS. Available online: https://www.usnews.com/news/world/articles/2020-05-01/covid-19-death-rate-in-deprived-areas-in-england-double-that-of-better-off-places-ons (accessed on 13 July 2020).
- Iacobucci, G. COVID-19: Deprived areas have the highest death rates in England and Wales. BMJ 2020, 369, m1810. [Google Scholar] [CrossRef] [PubMed]
- Corburn, J.; Vlahov, D.; Mberu, B.; Riley, L.; Caiaffa, W.T.; Rashid, S.F.; Ko, A.I.; Patel, S.; Jukur, S.; Martínez-Herrera, E.; et al. Slum Health: Arresting COVID-19 and Improving Well-Being in Urban Informal Settlements. J. Urban Health 2020, 97, 348–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Codeço, C.T.; Villela, D.; Coelho, F.; Bastos, L.S.; Carvalho, L.M.; Gomes, M.F.C.; Cruz, O.G.; Lana, R.M. Risco de Espalhamento da COVID-19 em Populações Indígenas: Considerações Preliminares Sobre Vulnerabilidade Geográfica e Sociodemográfica. Available online: https://agencia.fiocruz.br/sites/agencia.fiocruz.br/files/u91/relatorios_tecnicos_-_covid-19_procc-emap-ensp-covid-19-report4_20200419-indigenas.pdf (accessed on 26 August 2020).
- Ferrante, L.; Fearnside, P.M. Protect Indigenous peoples from COVID-19. Science 2020, 368, 251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terri, H. How COVID-19 Could Destroy Indigenous Communities—BBC Future. Available online: https://www.bbc.com/future/article/20200727-how-covid-19-could-destroy-indigenous-communities (accessed on 26 August 2020).
- Department of Economic and Social Affairs Indigenous Peoples & The COVID-19 Pandemic: Considerations. Available online: https://www.un.org/development/desa/indigenouspeoples/wp-content/uploads/sites/19/2020/04/COVID19_IP_considerations.pdf (accessed on 26 August 2020).
- Lainhart, W.; Dutari, L.C.; Rovira, J.R.; Sucupira, I.M.C.; Povoa, M.M.; Conn, J.; Loaiza, J.R. Epidemic and Non-Epidemic Hot Spots of Malaria Transmission Occur in Indigenous Comarcas of Panama. PLoS Negl. Trop. Dis. 2016, 10, e0004718. [Google Scholar] [CrossRef]
- UN Department of Economic and Social Affairs Population Division. World Urbanization Prospects. The 2018 Revision; United Nations: New York, NY, USA, 2019; Volume ST/ESA/SER.A/420.
- UN-Habitat Slums almanac 2015-16. Tracking Improvement in the Lives of Slum Dwellers; UN-Habitat: Rio de Janeiro, Brazil, 2016. [Google Scholar]
- Gevaert, C.M.; Kohli, D.; Kuffer, M. Slums, Informal Areas, or Invisible Cities? Mapping the “Missing Spaces”—JURSE 2019. Available online: http://jurse2019.org/special-session-slums-informal-areas-or-invisible-cities-mapping-the-missing-spaces/ (accessed on 13 July 2020).
- Mocnik, F.; Raposo, P.; Feringa, W.; Kraak, M.-J.; Köbben, B. Epidemics and pandemics in maps—The case of COVID-19. J. Maps 2020, 16, 144–152. [Google Scholar] [CrossRef]
- Wilkinson, A. Local response in health emergencies: Key considerations for addressing the COVID-19 pandemic in informal urban settlements. Environ. Urban. 2020, 0956247820922843. [Google Scholar] [CrossRef]
- Coltart, C.E.M.; Lindsey, B.B.; Ghinai, I.; Johnson, A.M.; Heymann, D.L. The Ebola outbreak, 2013–2016: Old lessons for new epidemics. Philos. Trans. R. Soc. B Biol. Sci. 2017, 372, 20160297. [Google Scholar] [CrossRef] [PubMed]
- Field, C.B.; Barros, V.R. Climate Change 2014: Impacts, Adaptation, and Vulnerability—IPCC WGII AR5 Summary for Policymakers. Available online: https://www.researchgate.net/publication/272150376_Climate_change_2014_impacts_adaptation_and_vulnerability_-_IPCC_WGII_AR5_summary_for_policymakers (accessed on 13 July 2020).
- Schneiderbauer, S.; Ehrlich, D. Risk, hazard and people’s vulnerability to natural hazards. A Rev. Defin. Concepts Data. Eur. Comm. Jt. Res. Centre. EUR 2004, 21410, 40. [Google Scholar]
- WHO Coronavirus Disease (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 5 May 2020).
- Cheong, L.; Da Silva, E.; Gibson, L.; Rush, D. Novel Coronavirus in Cape Town Informal Settlements: Feasibility of Using Informal Dwelling Outlines to Identify High Risk Areas for COVID-19 Transmission From A Social Distancing Perspective. JMIR Public Health Surveill. 2020, 6, e18844. [Google Scholar] [CrossRef]
- Marino, A.; Klintowitz, D.; Brito, G.; Rolnik, R.; Santoro, P.M.P. Circulação Para Trabalho Explica Concentração de Casos de Covid-19—LabCidade. Available online: http://www.labcidade.fau.usp.br/circulacao-para-trabalho-inclusive-servicos-essenciais-explica-concentracao-de-casos-de-covid-19/ (accessed on 13 July 2020).
- Barber, S.; Roux, A.V.D.; Cardoso, L.; Santos, S.; Toste, V.; James, S.; Barreto, S.M.; Schmidt, M.; Giatti, L.; Chor, D. At the intersection of place, race, and health in Brazil: Residential segregation and cardio-metabolic risk factors in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Soc. Sci. Med. 2018, 199, 67–76. [Google Scholar] [CrossRef]
- Unger, A.; Riley, L.W. Slum Health: From Understanding to Action. PLoS Med. 2007, 4, e295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hood, E. Dwelling Disparities: How Poor Housing Leads to Poor Health. Environ. Health Perspect. 2005, 113, 113. [Google Scholar] [CrossRef]
- Brito, P.L.; Arenas, H.; Lam, N.S.N.; Quintanilha, J.A. Recognition of Urban Patterns Related to Leptospirosis Contamination Risks Using Object Based Classification of Aerial Photography. Test Areas: Informal Settlements of the Railroad Suburb of Salvador, Brazil. In Proceedings of the IEEE International Geoscience and Remote Sensing Symposium (IGARSS 2008), Boston, MA, USA, 7–11 July 2008. [Google Scholar]
- Pasternak, S. Habitação e saúde. Estud. Avançados 2016, 30, 51–66. [Google Scholar] [CrossRef]
- Cecilia, B.; González, S.; Resistência, E.D.E.; Em, M.; Com, A.; Mellitus, D. Condições ambientais como fator de risco para doenças em comunidade carente na zona sul de são Paulo. Rev. Aten. Primária Saúde 2005, 13, 20–28. [Google Scholar]
- Catapreta, C.A.A.; Heller, L. Associação entre coleta de resíduos sólidos domiciliares e saúde, Belo Horizonte (MG), Brasil. Rev. Panam. Salud Pública 1999, 5, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Boadi, K.O.; Kuitunen, M. Environmental and health impacts of household solid waste handling and disposal practices in third world cities: The case of the Accra Metropolitan Area, Ghana. J. Environ. Health 2005, 68, 32–36. [Google Scholar]
- Brito, P.L.; Viana, M.S.; Delgado, J.P.M.; Brandão, A.C.; Pedrassoli, J.C.; Pedreira Júnior, J.U.; Souza, F.A. Nota Técnica 04—Alertas e Propostas de Ações para Península de Itapagipe Baseadas em Análises Geoespaciais de Suporte ao Combate à COVID-19; GeoCombate: Salvador, Brazil, 2020. [Google Scholar]
- Pedreira, J.J.U.; Delgado, J.P.M.; Pedrassoli, J.C.; Souza, F.A.; Brito, P.L.; Viana, M.S.; Galindo, E.; Brata, A.; Cassiano, A.; Freitas, J.C.A.; et al. Nota Técnica 1—Risco dos Bairros de Salvador ao Espalhamento do COVID-19 Decorrente da Circulação de Pessoas e Condições Socioeconômicas; GeoCombate: Salvador, Brazil, 2020. [Google Scholar]
- Kuffer, M.; Thomson, D.R.; Boo, G.; Mahabir, R.; Grippa, T.; VanHuysse, S.; Engstrom, R.; Ndugwa, R.; Makau, J.; Darin, E.; et al. The Role of Earth Observation in an Integrated Deprived Area Mapping “System” for Low-to-Middle Income Countries. Remote Sens. 2020, 12, 982. [Google Scholar] [CrossRef] [Green Version]
- Kuffer, M.; Pfeffer, K.; Sliuzas, R. Slums from Space—15 Years of Slum Mapping Using Remote Sensing. Remote Sens. 2016, 8, 455. [Google Scholar] [CrossRef] [Green Version]
- Digital Globe Open Data Occasion. Available online: https://www.digitalglobe.com/ecosystem/open-data/covid19 (accessed on 26 August 2020).
- Peckham, R.; Sinha, R. Satellites and the New War on Infection: Tracking Ebola in West Africa. Geoforum 2017, 80, 24–38. [Google Scholar] [CrossRef]
- Schootman, M.; Nelson, E.J.; Werner, K.B.; Shacham, E.; Elliott, M.B.; Ratnapradipa, K.L.; Lian, M.; McVay, A. Emerging technologies to measure neighborhood conditions in public health: Implications for interventions and next steps. Int. J. Health Geogr. 2016, 15, 20. [Google Scholar] [CrossRef] [Green Version]
- Grenzdörffer, G.J.; Niemeyer, F. Uav based brdf-measurements of agricultural surfaces with pfiffikus. Int. Arch. Photogramm. Remote Sens. Spat. Inf. Sci. 2012, 229–234. [Google Scholar] [CrossRef] [Green Version]
- Koeva, M.; Muneza, M.; Gevaert, C.M.; Gerke, M.; Nex, F. Using UAVs for map creation and updating. A case study in Rwanda. Surv. Rev. 2016, 50, 312–325. [Google Scholar] [CrossRef] [Green Version]
- Koeva, M.; Stöcker, C.; Crommelinck, S.; Ho, S.; Chipofya, M.; Jan, S.; Bennett, R.; Zevenbergen, J.; Vosselman, G.; Lemmen, C.; et al. Innovative Remote Sensing Methodologies for Kenyan Land Tenure Mapping. Remote Sens. 2020, 12, 273. [Google Scholar] [CrossRef] [Green Version]
- Chiabrando, F.; Nex, F.; Piatti, D.; Rinaudo, F. UAV and RPV systems for photogrammetric surveys in archaelogical areas: Two tests in the Piedmont region (Italy). J. Archaeol. Sci. 2011, 38, 697–710. [Google Scholar] [CrossRef]
- Rinaudo, F.; Chiabrando, F.; Lingua, A.; Spanò, A. Archaeological Site Monitoring: Uav Photogrammetry Can Be An Answer. Int. Arch. Photogramm. Remote Sens. Spat. Inf. Sci. 2012, 39, 583–588. [Google Scholar] [CrossRef] [Green Version]
- Akpan, N. Drones Are Taking Pictures That Could Demystify A Malaria Surge: Goats and Soda: NPR. Available online: https://www.npr.org/sections/goatsandsoda/2014/10/22/357637900/drones-are-taking-pictures-that-could-demystify-a-malaria-surge (accessed on 14 July 2020).
- Malaver, A.; Motta, N.; Corke, P.; Gonzalez, F. Development and Integration of a Solar Powered Unmanned Aerial Vehicle and a Wireless Sensor Network to Monitor Greenhouse Gases. Sensors 2015, 15, 4072–4096. [Google Scholar] [CrossRef] [PubMed]
- Eninger, R.M.; Johnson, R.L. Unmanned Aerial Systems in Occupational Hygiene—Learning from Allied Disciplines. Ann. Occup. Hyg. 2015, 59, 949–958. [Google Scholar] [CrossRef] [Green Version]
- Doherty, P.; Rudol, P. A UAV Search and Rescue Scenario with Human Body Detection and Geolocalization; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 2007; Volume 4830, pp. 1–13. [Google Scholar]
- Gevaert, C.M. Unmanned Aerial Vehicle Mapping for Settlement Upgrading; University Library/University of Twente: Enschede, The Netherlands, 2018. [Google Scholar]
- Stöcker, C.; Bennett, R.; Nex, F.; Gerke, M.; Zevenbergen, J. Review of the Current State of UAV Regulations. Remote Sens. 2017, 9, 459. [Google Scholar] [CrossRef] [Green Version]
- LiDAR Uses in Disaster Response. Available online: https://www.harrisgeospatial.com/Support/Self-Help-Tools/Help-Articles/Help-Articles-Detail/ArtMID/10220/ArticleID/16108/LiDAR-Uses-in-Disaster-Response (accessed on 14 July 2020).
- Elden, S. Secure the volume: Vertical geopolitics and the depth of power. Politi Geogr. 2013, 34, 35–51. [Google Scholar] [CrossRef]
- Reavley, N.J.; Pilkington, P.D. Use of Twitter to monitor attitudes toward depression and schizophrenia: An exploratory study. PeerJ 2014, 2, e647. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Agrawal, A.; Choudhary, A. Real-time disease surveillance using Twitter data. In Proceedings of the the 19th ACM SIGKDD International Conference; Association for Computing Machinery (ACM), Chicago, IL, USA, 11–14 August 2013; pp. 1474–1477. [Google Scholar]
- Quercia, D.; Schifanella, R.; Aiello, L.M.; McLean, K. Smelly Maps: The Digital Life of Urban Smellscapes. arXiv 2015, arXiv:1505.06851. [Google Scholar]
- Zastrow, M. Crisis mappers turn to citizen scientists. Nature 2014, 515, 321. [Google Scholar] [CrossRef] [PubMed]
- Wukich, C. Social media use in emergency management. J. Emerg. Manag. 2015, 13, 281–295. [Google Scholar] [CrossRef] [PubMed]
- Boulos, M.N.K.; Resch, B.; Crowley, D.N.; Breslin, J.G.; Sohn, G.; Burtner, R.; Pike, W.A.; Jezierski, E.; Chuang, K.-Y.S. Crowdsourcing, citizen sensing and sensor web technologies for public and environmental health surveillance and crisis management: Trends, OGC standards and application examples. Int. J. Health Geogr. 2011, 10, 67. [Google Scholar] [CrossRef] [Green Version]
- Missing Maps Putting the World’s Vulnerable People on the Map. Available online: https://www.missingmaps.org/ (accessed on 26 August 2020).
- Magalhaes, T.; Chalegre, K.D.M.; Braga, M.C.; Foy, B. The Endless Challenges of Arboviral Diseases in Brazil. Trop. Med. Infect. Dis. 2020, 5, 75. [Google Scholar] [CrossRef]
- IBGE. Aglomerados Subnormais; IBGE: Brasília, Brazil, 2010.
- Silva, J.; Barbosa, J.; Biteti, M.; Fernandes, F. O Que é a Favela, Afinal? Observatório de Favelas: Rio de Janeiro, Brazil, 2009; ISBN 9788598881072. [Google Scholar]
- IdeaMaps Network Responding to COVID-19 in LMIC Cities: Citizens—Documentos Google. Available online: https://docs.google.com/document/d/19fsQAJZp7DpZT4f5qfcYnNylYMDP_EtmC4hoO7jtJro/edit (accessed on 14 July 2020).
- JEI Corona Diaries of the Urban Poor. Available online: https://www.justempower.org/coronadiaries (accessed on 20 July 2020).
- WHO. WHO Housing and Health Guidelines; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Hamidi, S.; Sabouri, S.; Ewing, R. Does Density Aggravate the COVID-19 Pandemic? J. Am. Plan. Assoc. 2020, 1–15. [Google Scholar] [CrossRef]
- IBGE. Estimativas de população para os municípios e para as Unidades da Federação brasileiros, com data de referência em 1° de julho de 2019. Diário União 28 Agosto 2019. Available online: https://agenciadenoticias.ibge.gov.br/en/agencia-press-room/2185-news-agency/releases-en/25283-ibge-divulga-as-estimativas-da-populacao-dos-municipios-para-2020 (accessed on 20 July 2020).
- IBGE. Produto Interno Bruto dos Municípios 2017; IBGE: Brasília, Brazil, 2017; p. 16.
- IBGE. Subnormal Agglomerates—About the Publication—2010—Territorial Information. Available online: https://www.ibge.gov.br/en/geosciences/full-list-geosciences/17553-subnormal-agglomerates.html?edicao=17588&t=sobre (accessed on 16 July 2020).
- Gomes, J.; Pedrassoli, J. Levantamento de Características de Moradias Em Favelas com o Uso de Drone: Um Experimento na Comunidade do Alto das Pombas, Salvador/Ba. In Proceedings of the III Seminário Nacional sobre Urbanização de Favelas—UrbFavelas, Salvador, Brazil, 21–23 November 2018. [Google Scholar]
- Hagan, J.E.; Moraga, P.; Costa, F.; Capian, N.; Ribeiro, G.S.; Wunder, E.A., Jr.; Felzemburgh, R.D.M.; Reis, R.B.; Nery, N.; Santana, F.S.; et al. Spatiotemporal Determinants of Urban Leptospirosis Transmission: Four-Year Prospective Cohort Study of Slum Residents in Brazil. PLoS Negl. Trop. Dis. 2016, 10, e0004275. [Google Scholar] [CrossRef]
- Snyder, R.E.; Rajan, J.V.; Costa, F.; Lima, H.C.A.V.; Calcagno, J.I.; Couto, R.D.; Riley, L.W.; Dos Reis, M.G.; Ko, A.I.; Ribeiro, G.S. Differences in the Prevalence of Non-Communicable Disease between Slum Dwellers and the General Population in a Large Urban Area in Brazil. Trop. Med. Infect. Dis. 2017, 2, 47. [Google Scholar] [CrossRef]
- IPEA Atlas da Vulnerabilidade Social. Available online: http://ivs.ipea.gov.br/index.php/pt/ (accessed on 16 July 2020).
- IBGE Censo Demográfico 2010. Available online: https://portaldemapas.ibge.gov.br/portal.php#homepage (accessed on 20 July 2020).
- Mahabir, R.; Croitoru, A.; Crooks, A.; Agouris, P.; Stefanidis, A. A Critical Review of High and Very High-Resolution Remote Sensing Approaches for Detecting and Mapping Slums: Trends, Challenges and Emerging Opportunities. Urban Sci. 2018, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Kuffer, M.; Persello, C.; Pfeffer, K.; Sliuzas, R.; Rao, V.; Itc, K.P. Do we underestimate the global slum population? In Proceedings of the Joint Urban Remote Sensing Event (JURSE 2019), Vannes, France, 22–24 May 2019; IEEE: Vannes, France, 2019; pp. 1–4. [Google Scholar]
- Carr-Hill, R. Missing Millions and Measuring Development Progress. World Dev. 2013, 46, 30–44. [Google Scholar] [CrossRef]
- SEI. Projeções Populacionais Para a Bahia 2010–2030; Governo do Estado da Bahia: Salvador, Brazil, 2013.
- Costa, M.A.; Lui, L.; Santos, R.M.D.; Curi, R.L.C.; Albuquerque, C.G.D.; Tavares, S.R.; Krause, C. Nota Técnica Abril de 2020 Apontamentos Sobre a Dimensão Territorial da Pandemia da COVID-19 e os Fatores que Contribuem Para Aumentar a Vulnerabilidade Socioespacial nas Unidades de Desenvolvimento Humano de Áreas Metropolitanas Brasileiras; IPEA: Brazilia, Brazil, 2020.
- Fornace, K.M.; Drakeley, C.; William, T.; Espino, F.; Cox, J. Mapping infectious disease landscapes: Unmanned aerial vehicles and epidemiology. Trends Parasitol. 2014, 30, 514–519. [Google Scholar] [CrossRef]
- Stevens, F.R.; Gaughan, A.E.; Linard, C.; Tatem, A.J. Disaggregating Census Data for Population Mapping Using Random Forests with Remotely-Sensed and Ancillary Data. PLoS ONE 2015, 10, e0107042. [Google Scholar] [CrossRef] [Green Version]
- Kit, O.; Lüdeke, M.; Reckien, D. Defining the Bull’S Eye: Satellite Imagery-Assisted Slum Population Assessment in Hyderabad, India. Urban Geogr. 2013, 34, 413–424. [Google Scholar] [CrossRef]
- Rolnik, R.; Marino, A.; Klintowitz, D.; Brito, G.; Resende, P.; Nisida, V.; Cavalcante, L. Mapas do Coronavírus Escondem Informações—LabCidade. Available online: http://www.labcidade.fau.usp.br/mapas-do-coronavirus-escondem-informacoes/ (accessed on 16 July 2020).
- Reuters Africa Faces “Hunger Pandemic” as Coronavirus Destroys Jobs and Fuels Poverty. Available online: https://www.reuters.com/article/us-health-coronavirus-africa-hunger-feat/africa-faces-hunger-pandemic-as-coronavirus-destroys-jobs-and-fuels-poverty-idUSKCN22629V (accessed on 16 July 2020).
- Thomson, D.R.; Kuffer, M.; Boo, G.; Hati, B.; Grippa, T.; Elsey, H.; Linard, C.; Mahabir, R.; Kyobutungi, C.; Maviti, J.; et al. Need for an Integrated Deprived Area “Slum” Mapping System (IDEAMAPS) in Low-and Middle-Income Countries (LMICs). Soc. Sci. 2020, 9, 80. [Google Scholar] [CrossRef]
- Hachmann, S.; Arsanjani, J.J.; Vaz, E. Spatial data for slum upgrading: Volunteered Geographic Information and the role of citizen science. Habitat Int. 2018, 72, 18–26. [Google Scholar] [CrossRef]
- Mahabir, R.; Stefanidis, A.; Croitoru, A.; Crooks, A.; Agouris, P. Authoritative and Volunteered Geographical Information in a Developing Country: A Comparative Case Study of Road Datasets in Nairobi, Kenya. ISPRS Int. J. Geo Inf. 2017, 6, 24. [Google Scholar] [CrossRef]
- Mooney, P.; Grinberger, A.Y.; Minghini, M.; Coetzee, S.; Juhasz, L.; Yeboah, G. OpenStreetMap data use cases during the early months of the COVID-19 pandemic 2020. arXiv 2020, arXiv:2008.02653. [Google Scholar]
- de Albuquerque, J.P.; Eckle, M.; Herfort, B.; Zipf, A. Crowdsourcing geographic information for disaster management and improving urban resilience: An overview of recent developments and lessons learned. In European Handbook of Crowdsourced Geographic Information; Ubiquity Press: London, UK, 2016; pp. 309–321. [Google Scholar] [CrossRef] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Spatial Information | EO-Based Data (Potential) | Dimension |
|---|---|---|
| Population | V/HR-imagery + demographic data | Density |
| Buildings | V/HR-imagery | Density |
| Road and pathways types | V/HR-imagery | Density |
| Road width | V/HR-imagery | Density |
| Open spaces within communities | V/HR-imagery | Density |
| Surrounding open spaces | V/HR-imagery | Density/Facilities |
| Local markets | Community-based mapping | Facilities |
| Health facilities | Community-based mapping | Facilities |
| Schools | Community-based mapping | Facilities |
| Community centers | Community-based mapping | Facilities |
| Religious places | Community-based mapping | Facilities |
| Water collection points | Community-based mapping | Facilities |
| Open severs | VHR aerial and UAV imagery | Environmental |
| Slopes | LiDAR point clouds or VHR stereo-images | Environmental |
| Standing water (sinks) | LiDAR point clouds or VHR stereo-images | Environmental |
| Open waters | V/HR-imagery | Environmental |
| Trash piles | VHR and drone imagery | Environmental |
| Heat accumulation | TIR images | Environmental |
| Data Layer | Year | Population Estimate |
|---|---|---|
| Worldpop | 2020 | 40,011 |
| SEDAC * | 2020 * | 32,947 |
| Census | 2010 | 36,521 |
| Census (projected) [74] * | 2020 | 39,271 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brito, P.L.; Kuffer, M.; Koeva, M.; Pedrassoli, J.C.; Wang, J.; Costa, F.; Freitas, A.D.d. The Spatial Dimension of COVID-19: The Potential of Earth Observation Data in Support of Slum Communities with Evidence from Brazil. ISPRS Int. J. Geo-Inf. 2020, 9, 557. https://doi.org/10.3390/ijgi9090557
Brito PL, Kuffer M, Koeva M, Pedrassoli JC, Wang J, Costa F, Freitas ADd. The Spatial Dimension of COVID-19: The Potential of Earth Observation Data in Support of Slum Communities with Evidence from Brazil. ISPRS International Journal of Geo-Information. 2020; 9(9):557. https://doi.org/10.3390/ijgi9090557
Chicago/Turabian StyleBrito, Patricia Lustosa, Monika Kuffer, Mila Koeva, Julio Cesar Pedrassoli, Jiong Wang, Federico Costa, and Anderson Dias de Freitas. 2020. "The Spatial Dimension of COVID-19: The Potential of Earth Observation Data in Support of Slum Communities with Evidence from Brazil" ISPRS International Journal of Geo-Information 9, no. 9: 557. https://doi.org/10.3390/ijgi9090557