Assessment and Mapping of Spatio-Temporal Variations in Human Mortality-Related Parameters at European Scale




Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Methodology
3. Results
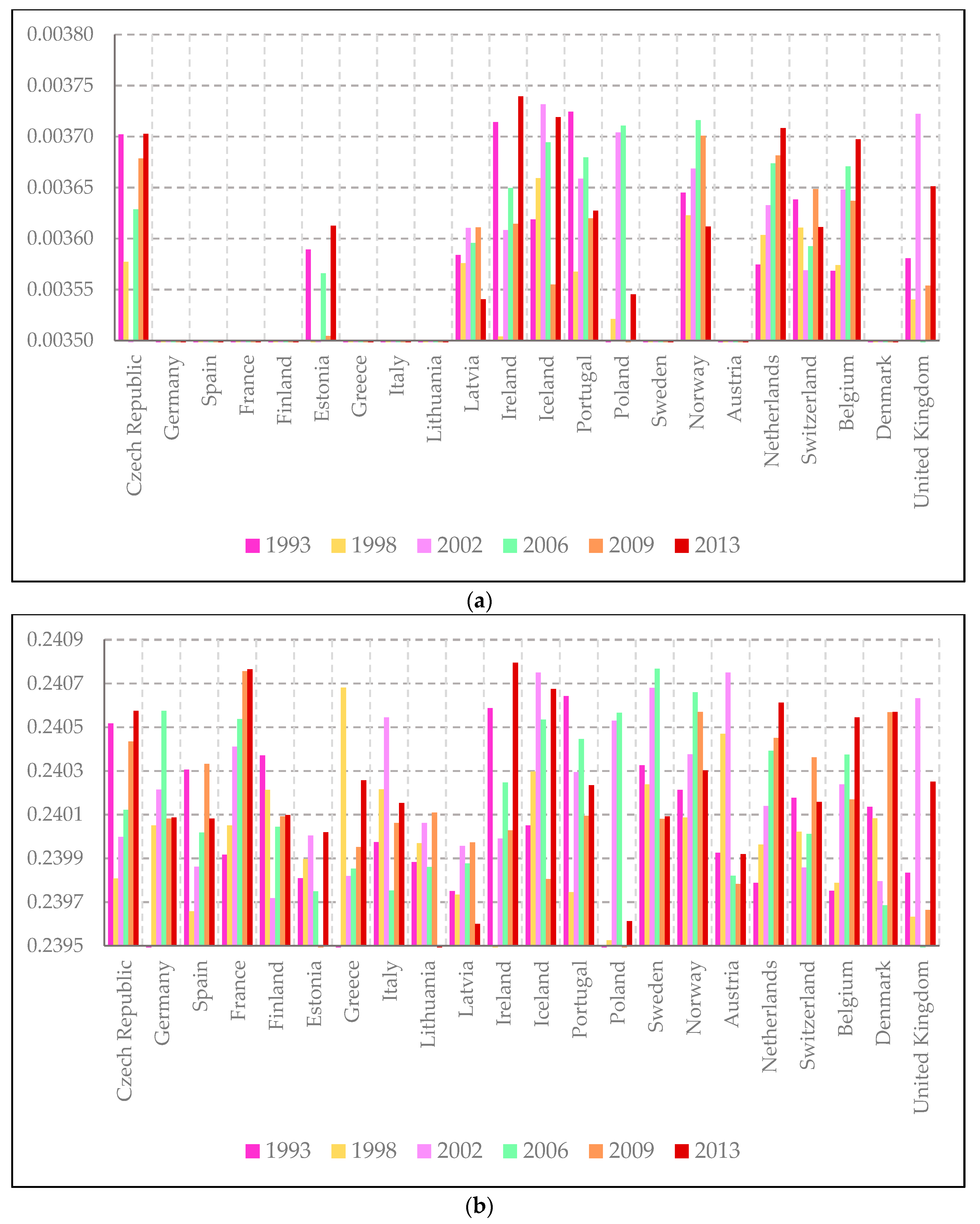
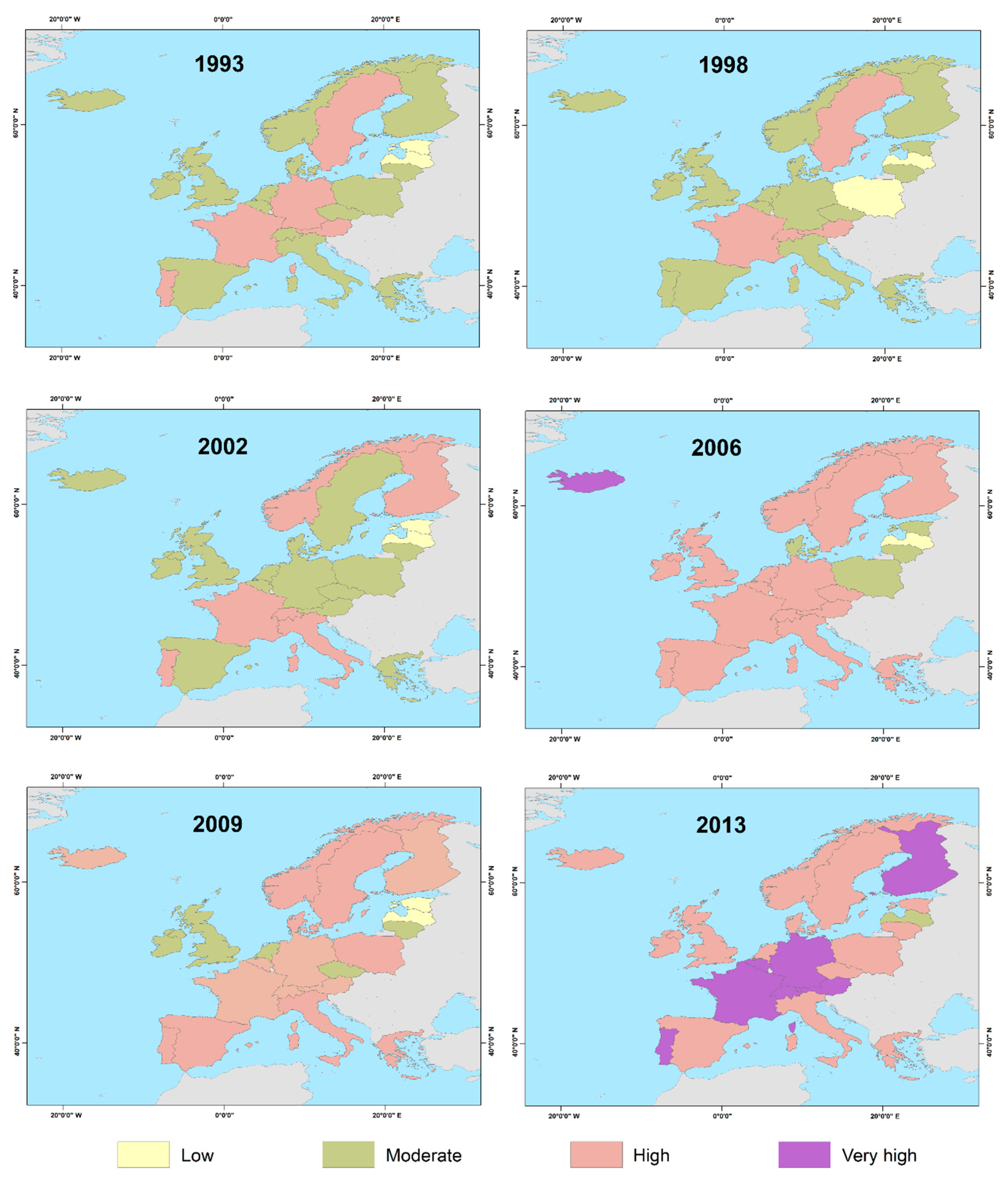
3.1. Infant Mortality (Parameter Θ)
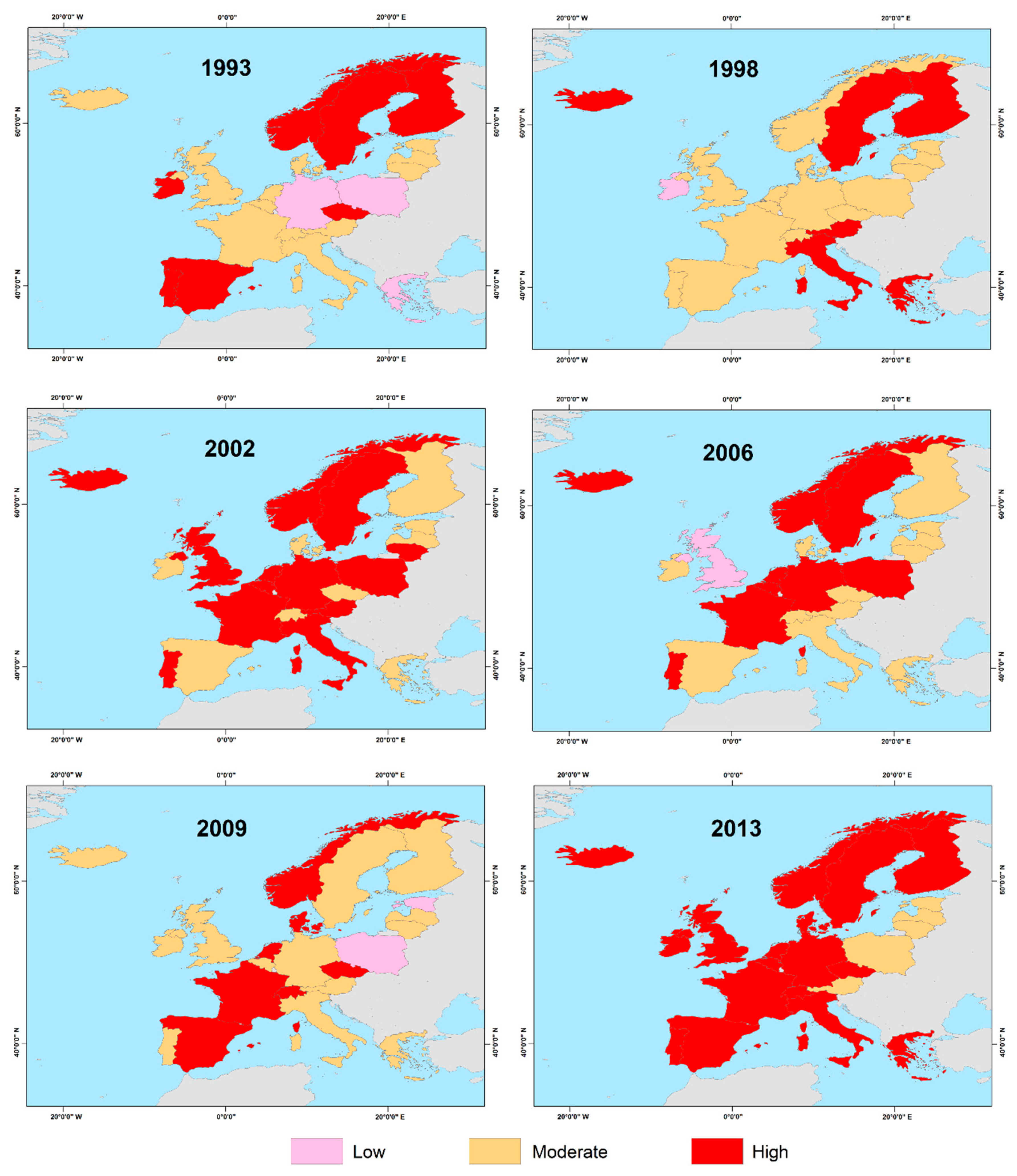
3.2. Population Aging (Parameter Ξ)
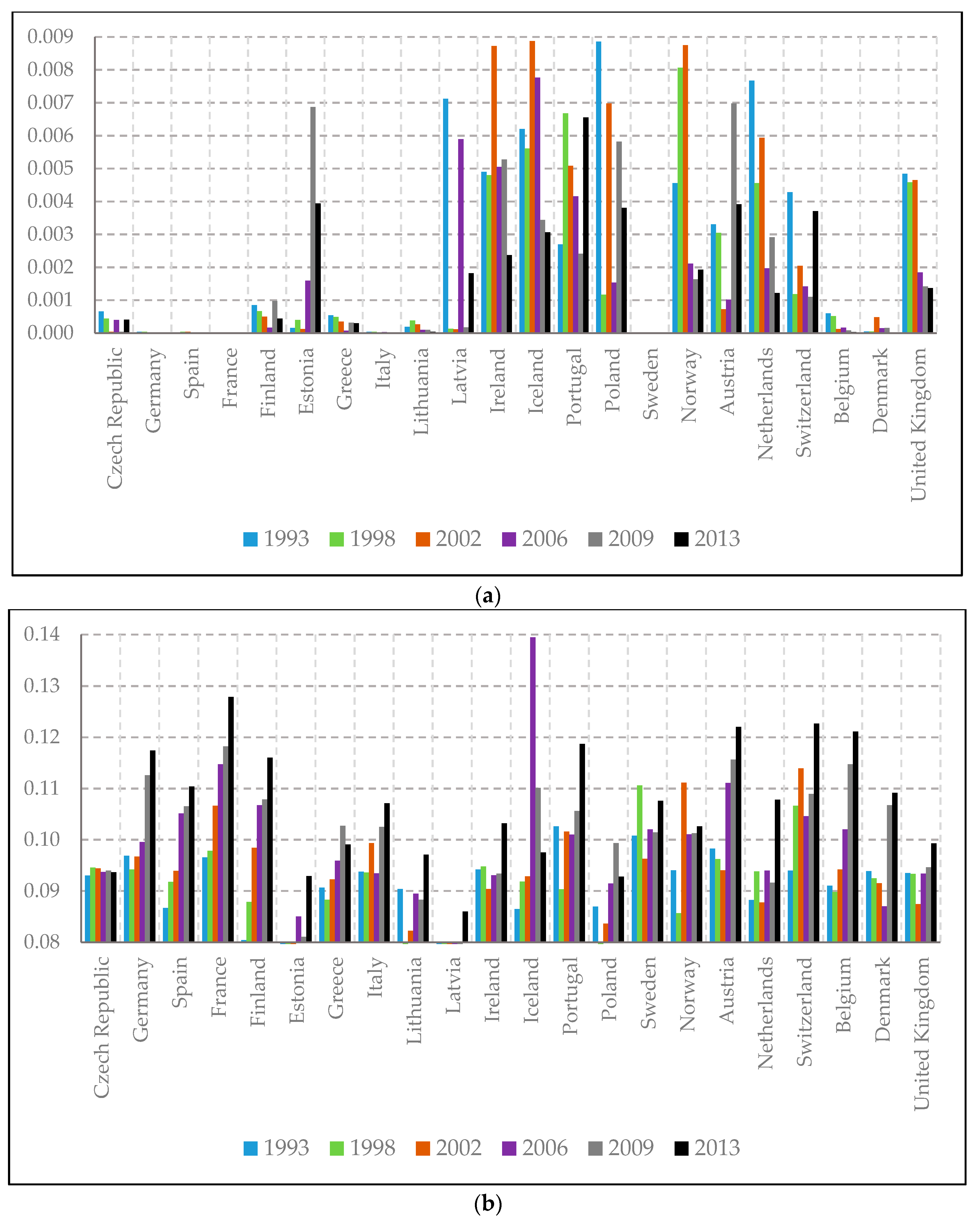
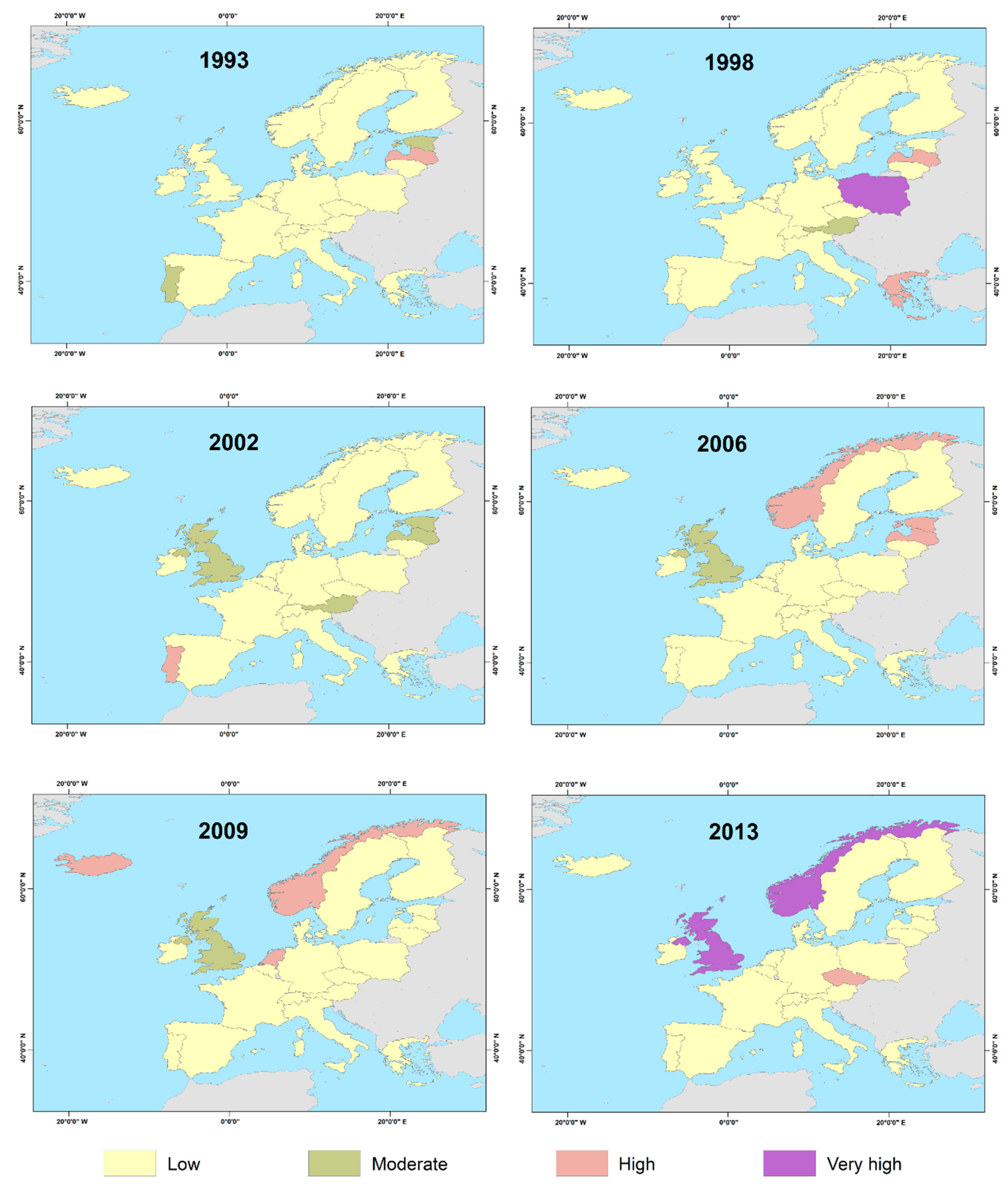
3.3. Individual Unexpected Mortality (Parameter Κ)
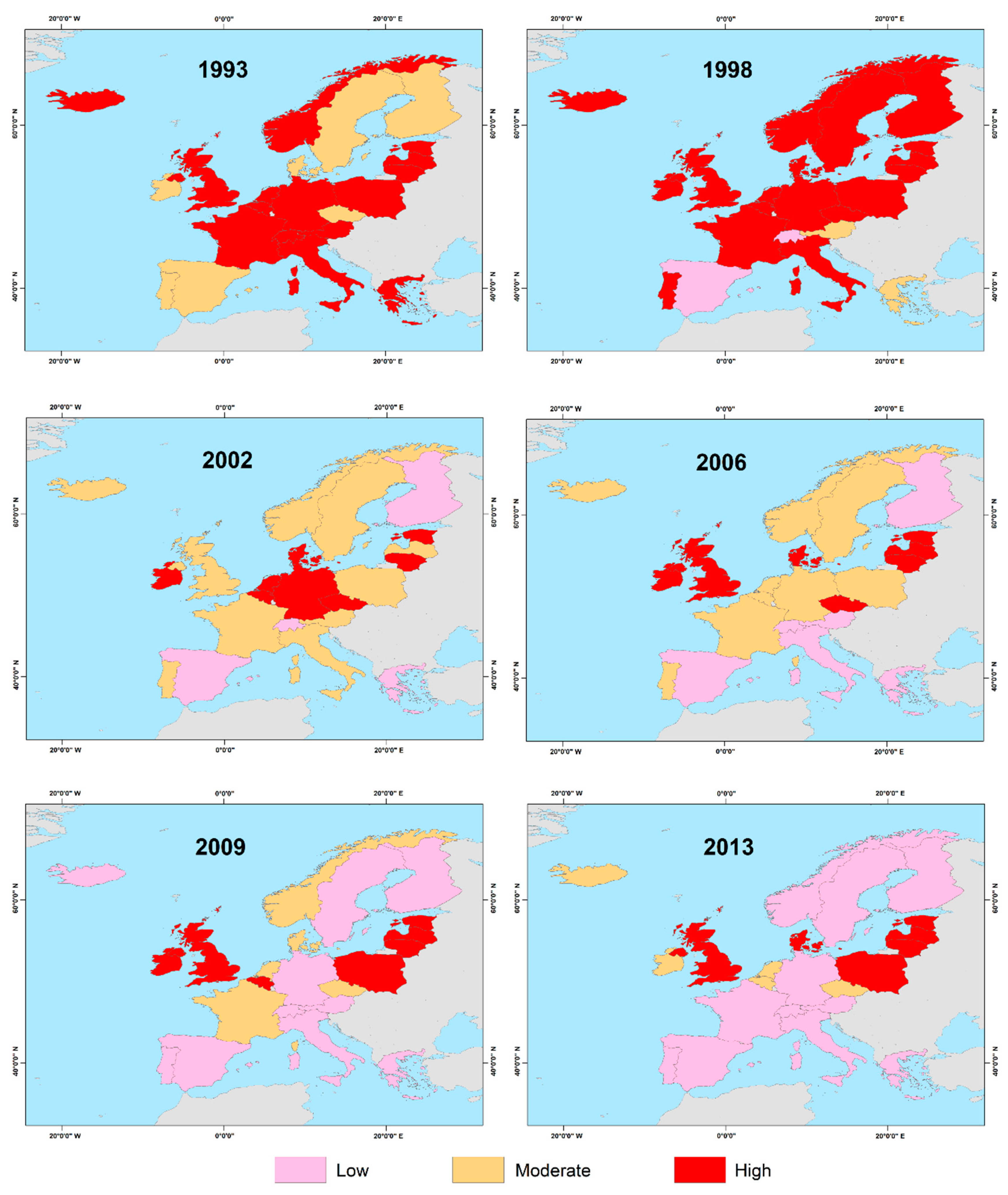
3.4. Population Mortality due to Hazardous Events (Parameter Λ)
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Currie, I.D.; Durban, M.; Eilers, P.H. Smoothing and forecasting mortality rates. Stat. Model. 2004, 4, 279–298. [Google Scholar] [CrossRef]
- Bosetti, C.; Bertuccio, P.; Chatenoud, L.; Negri, E.; Levi, F.; La Vecchia, C. Childhood cancer mortality in Europe, 1970–2007. Eur. J. Cancer 2010, 46, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Amaro, J.; Severo, M.; Vilela, S.; Fonseca, S.; Fontes, F.; La Vecchia, C.; Lunet, N. Patterns of breast cancer mortality trends in Europe. Breast 2013, 22, 244–253. [Google Scholar] [CrossRef]
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimatesfor 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [Green Version]
- Hartley, A.; Marshall, D.C.; Salciccioli, J.D.; Sikkel, M.B.; Maruthappu, M.; Shalhoub, J. Trends in Mortality From Ischemic Heart Disease and Cerebrovascular Disease in Europe: 1980 to 2009. Circulation 2016, 133, 1916–1926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballester, J.; Robine, J.-M.; Herrmann, F.R.; Xavier Rodó, X. Effect of the Great Recession on regional mortality trends in Europe. Nat. Commun. 2019, 10, 679. [Google Scholar] [CrossRef]
- Rey, G.; Jougla, E.; Fouillet, A.; Hémon, D. Ecological association between a deprivation index and mortality in France over the period 1997–2001: Variations with spatial scale, degree of urbanicity, age, gender and cause of death. BMC Public Health 2009, 9, 33. [Google Scholar] [CrossRef] [Green Version]
- Schuster, C.; Burkart, K.; Lakes, T. Heat mortality in Berlin – Spatial variability at the neighborhood scale. Urban Clim. 2014, 10, 134–147. [Google Scholar] [CrossRef]
- López-Abente, G.; Aragonés, N.; Pérez-Gómez, B.; Pollán, M.; García-Pérez, J.; Ramis, R.; Fernández-Navarro, P. Time trends in municipal distribution patterns ofcancer mortality in Spain. BMC Cancer 2014, 14, 535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almendra, R.; Santana, P.; Vasconcelos, J. Evidence of social deprivation on the spatial patterns of excess winter mortality. Int. J. Public Health 2017, 62, 849–856. [Google Scholar] [CrossRef] [Green Version]
- Yashin, A.I.; Iachine, I.A.; Begun, A.S. Mortality modeling: A review. Math. Popul. Stud. 2000, 8, 305–332. [Google Scholar] [CrossRef]
- Vaupel, J.W. Biodemography of human ageing. Nature 2010, 464, 536–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, H.; Tickle, L. Mortality modelling and forecasting: A review of methods. Ann. Actuar. Sci. 2008, 3, 3–43. [Google Scholar] [CrossRef]
- Gompertz, B. On the nature of the function expressive of the law of human mortality, and on a new mode of determining the value of life contingencies. Philos. Trans. R. Soc. Lond. 1825, 115, 513–583. [Google Scholar]
- Makeham, W.M. On the law of mortality and construction of annuity tables. Assur. Mag. J. Inst. Actuar. 1860, 8, 301–310. [Google Scholar] [CrossRef] [Green Version]
- Skiadas, C.H.; Skiadas, C. A modeling approach to life table data sets. Recent Adv. Stoch. Modeling Data Anal. 2007, 350–359. [Google Scholar] [CrossRef] [Green Version]
- Gavrilov, L.A.; Gavrilova, N.S. The Quest for a General Theory of Aging and Longevity. Sci. Aging Knowl. Environ. 2003, 28, 5. [Google Scholar] [CrossRef] [Green Version]
- Vaupel, J.W. Lifesaving, lifetimes and lifetables. Demogr. Res. 2005, 13, 597–614. [Google Scholar] [CrossRef]
- Andreopoulos, P.; Bersimis, G.F.; Tragaki, A.; Rovolis, A. Mortality modeling using probability distributions: Application in greek mortality data. Commun. Stat. Theory Methods 2019, 48, 127–140. [Google Scholar] [CrossRef]
- Human Mortality Database (HMD). Mortality and Population Data. Available online: http://www.mortality.org/ (accessed on 26 November 2019).
- European Statistical Authority (Eurostat). Population Data. Available online: https://ec.europa.eu/eurostat/ (accessed on 26 November 2019).
- European Statistical Authority (Eurostat). Vector Layer of European Countries. Available online: https://ec.europa.eu/eurostat/ (accessed on 26 November 2019).
- Forfar, D.O.; McCutcheon, J.J.; Wilkie, A.D. On graduation by mathematical formula. J. Inst. Actuar. 1988, 115, 1–149. [Google Scholar] [CrossRef]
- Jones, M.C. On a class of distributions defined by the relationship between their density and distribution functions. Commun. Stat. Theory Methods 2007, 36, 1835–1843. [Google Scholar] [CrossRef]
- Kim, D.; Saada, A. The Social Determinants of Infant Mortality and Birth Outcomes in Western Developed Nations: A Cross-Country Systematic Review. Int. J. Environ. Res. Public Health 2013, 10, 2296–2335. [Google Scholar] [CrossRef] [Green Version]
- Myung, I.J. Tutorial on maximum likelihood estimation. J. Math. Psychol. 2003, 47, 90–100. [Google Scholar] [CrossRef]
- Amemiya, T. Advanced Econometrics; Harvard University Press: Cambridge, MA, USA, 1985. [Google Scholar]
- Elzhov, T.V.; Mullen, K.M.; Spiess, A.N.; Bolker, B. R Interface to the Levenberg-Marquardt Nonlinear Least-Squares Algorithm Found in MINPACK, Plus Support for Bounds. R Package Version 1.2-1. 2016, p. 14. Available online: https://cran.r-project.org/web/packages/minpack.lm/minpack.lm.pdf (accessed on 18 January 2020).
- Ayalew, L.; Yamagishi, H. The application of GIS-based logistic regression for landslide susceptibility mapping in the Kakuda-Yahiko Mountains Central Japan. Geomorphology 2005, 65, 15–31. [Google Scholar] [CrossRef]
- Kalogirou, S.; Tsimbos, C.; Verropoulou, G.; Kotsifakis, G. Regional mortality differentials in Greece by selected causes of death: 2006–2008. J. Maps 2012, 8, 354–360. [Google Scholar] [CrossRef]
- Drevenstedt, G.L.; Crimmins, E.M.; Vasunilashorn, S.; Finch, C.E. The rise and fall of excess male infant mortality. Proc. Natl. Acad. Sci. USA 2008, 105, 5016–5021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Organisation for Economic Co-Operation and Development (OECD). Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Wasserman, D.; Cheng, Q.; Jiang, G.X. Global suicide rates among young people aged 15–19. World Psychiatry 2005, 4, 114–120. [Google Scholar]
- Lenart, P.; Kuruczova, D.; Joshi, P.K.; Bienertová-Vašků, J. Male mortality rates mirror mortality rates of older females. Sci. Rep. 2019, 9, 10589. [Google Scholar] [CrossRef] [Green Version]
- Onambele, L.; San Martin-Rodríguez, L.; Niu, H.; Alvarez-Alvarez, I.; Arnedo-Pena, A.; Guillen-Grima, F.; Aguinaga-Ontoso, I. Infant mortality in the European Union: A time trend analysis of the 1994–2015 period. An. De Pediatría 2019, 91, 219–227. [Google Scholar] [CrossRef]
- Suchecka, J.; Urbaniak, B. Determinants of Healthy Ageing for Older People in European Countries—A Spatio-Temporal Approach. Comp. Econ. Res. 2016, 19, 157–178. [Google Scholar] [CrossRef]
- Oksuzyan, A.; Juel, K.; Vaupel, J.W.; Christensen, K. Men: Good health and high mortality. Sex differences in health and aging. Aging Clin. Exp. Res. 2008, 20, 91–102. [Google Scholar] [CrossRef] [Green Version]
- Nordic Burden of Disease Collaborators. Life expectancy and disease burden in the Nordic countries: Results from the Global Burden of Diseases, Injuries, and Risk Factors Study 2017. Lancet Public Health 2019, 4, e658–e669. [Google Scholar] [CrossRef]
- Hazans, M. Migration Experience of the Baltic Countries in the Context of Economic Crisis. In Labor Migration, EU Enlargement, and the Great Recession; Kahanec, M., Zimmermann, K.F., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 297–344. [Google Scholar]
- Laliotis, I.; Ioannidis, J.P.A.; Stavropoulou, C. Total and cause-specific mortality before and after the onset of the Greek economic crisis: An interrupted time-series analysis. Lancet Public Health 2016, 1, e56–e65. [Google Scholar] [CrossRef] [Green Version]
- Lafaut, D.; Vandenheede, H.; Surkyn, J.; Coene, G. Counting the non-existing: Causes of death of undocumented migrants in Brussels-Capital Region (Belgium), 2005–2010. Arch. Public Health 2019, 77. [Google Scholar] [CrossRef] [Green Version]
- Van Meeteren, M.; van de Pol, S.; Dekker, R.; Engbersen, G.; Snel, E. Destination Netherlands: History of Immigration and Immigration Policy in the Netherlands. In Immigrants: Acculturation, Socioeconomic Challenges and Cultural Psychology; Ho, J., Ed.; Nova Science Publishers: New York, NY, USA, 2013; pp. 113–170. [Google Scholar]
- Domnich, A.; Panatto, D.; Gasparini, R.; Amicizia, D. The “healthy immigrant” effect: Does it exist in Europe today? Ital. J. Public Health 2012, 9, e7532–e7537. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
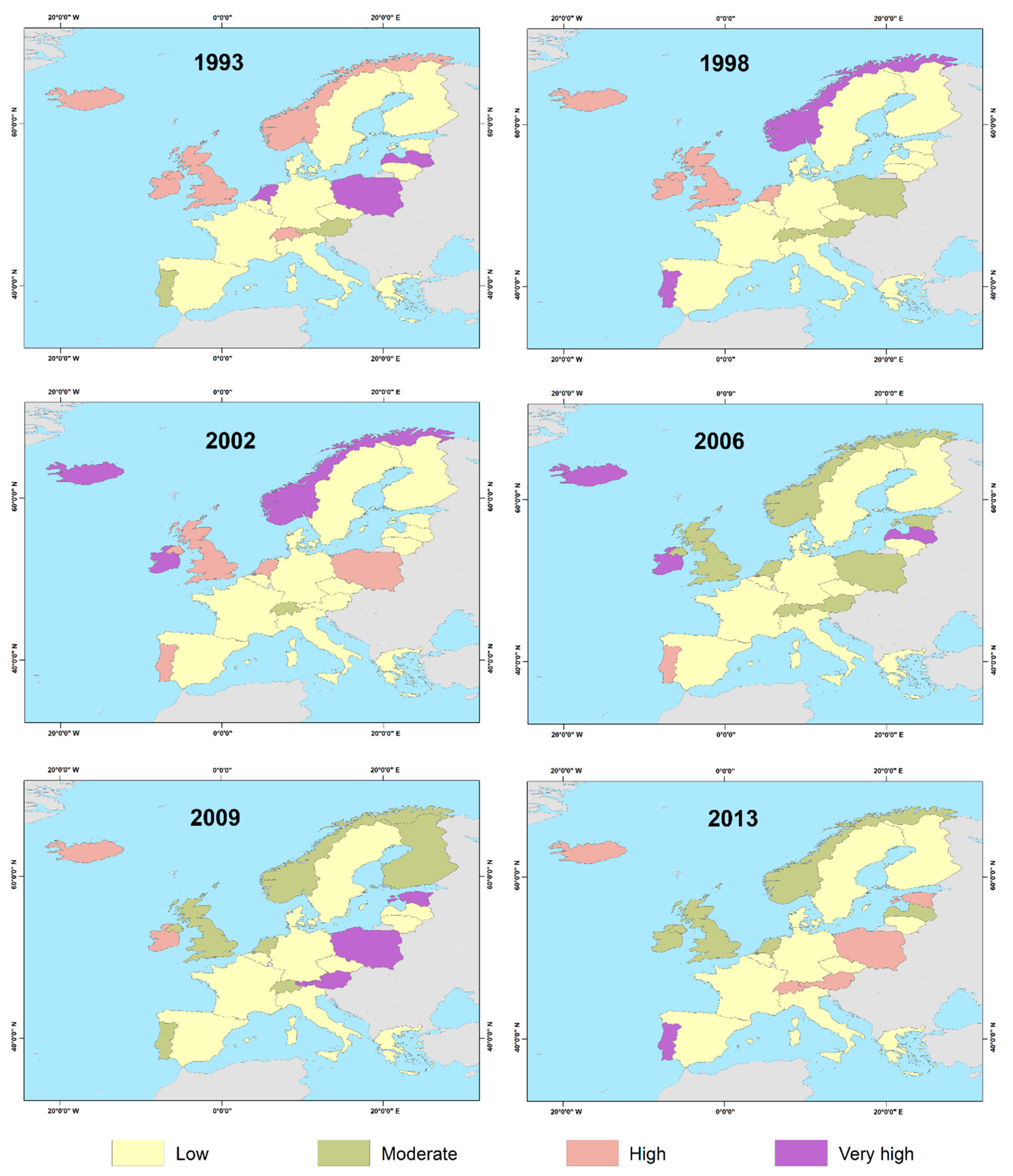
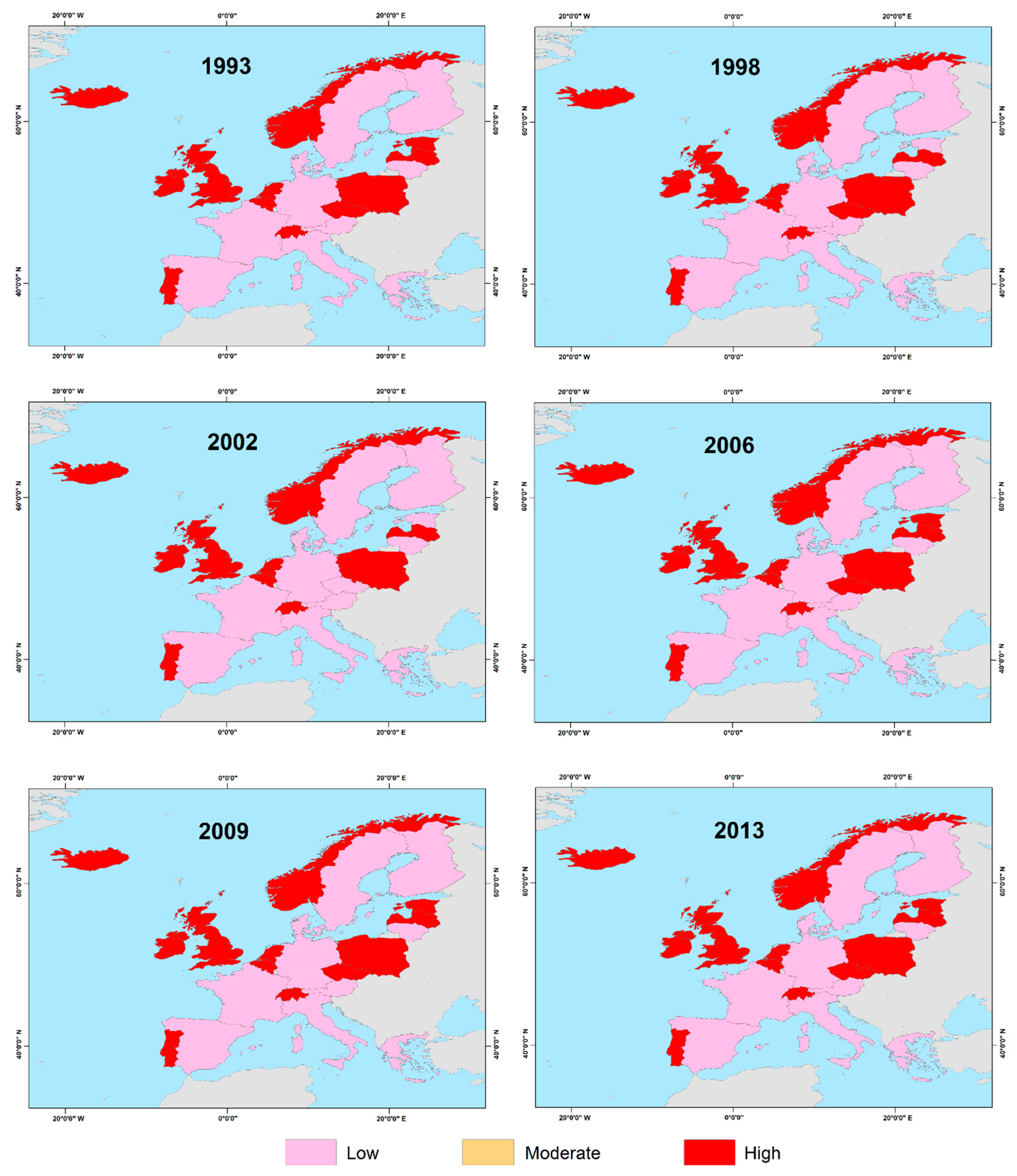
| Classes | Standard Deviations | |
|---|---|---|
| Males | Females | |
| Low | <−0.5 std | <−0.5 std |
| Moderate | −0.5–0.5 std | −0.5–0.5 std |
| High | 0.5–1.5 std | > 0.5 std |
| Very high | >1.5 std | – |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreopoulos, P.; Polykretis, C.; Tragaki, A. Assessment and Mapping of Spatio-Temporal Variations in Human Mortality-Related Parameters at European Scale. ISPRS Int. J. Geo-Inf. 2020, 9, 547. https://doi.org/10.3390/ijgi9090547
Andreopoulos P, Polykretis C, Tragaki A. Assessment and Mapping of Spatio-Temporal Variations in Human Mortality-Related Parameters at European Scale. ISPRS International Journal of Geo-Information. 2020; 9(9):547. https://doi.org/10.3390/ijgi9090547
Chicago/Turabian StyleAndreopoulos, Panagiotis, Christos Polykretis, and Alexandra Tragaki. 2020. "Assessment and Mapping of Spatio-Temporal Variations in Human Mortality-Related Parameters at European Scale" ISPRS International Journal of Geo-Information 9, no. 9: 547. https://doi.org/10.3390/ijgi9090547